Calcium Absorption in Infants and Small Children: Methods of Determination and Recent Findings

{kind=link}
{kind=link}
Abstract
:1. Introduction: Assessment of Calcium Absorption in Children
2. Results and Discussion
2.1. Calcium Absorption from Infant Formula Compared to Human Milk
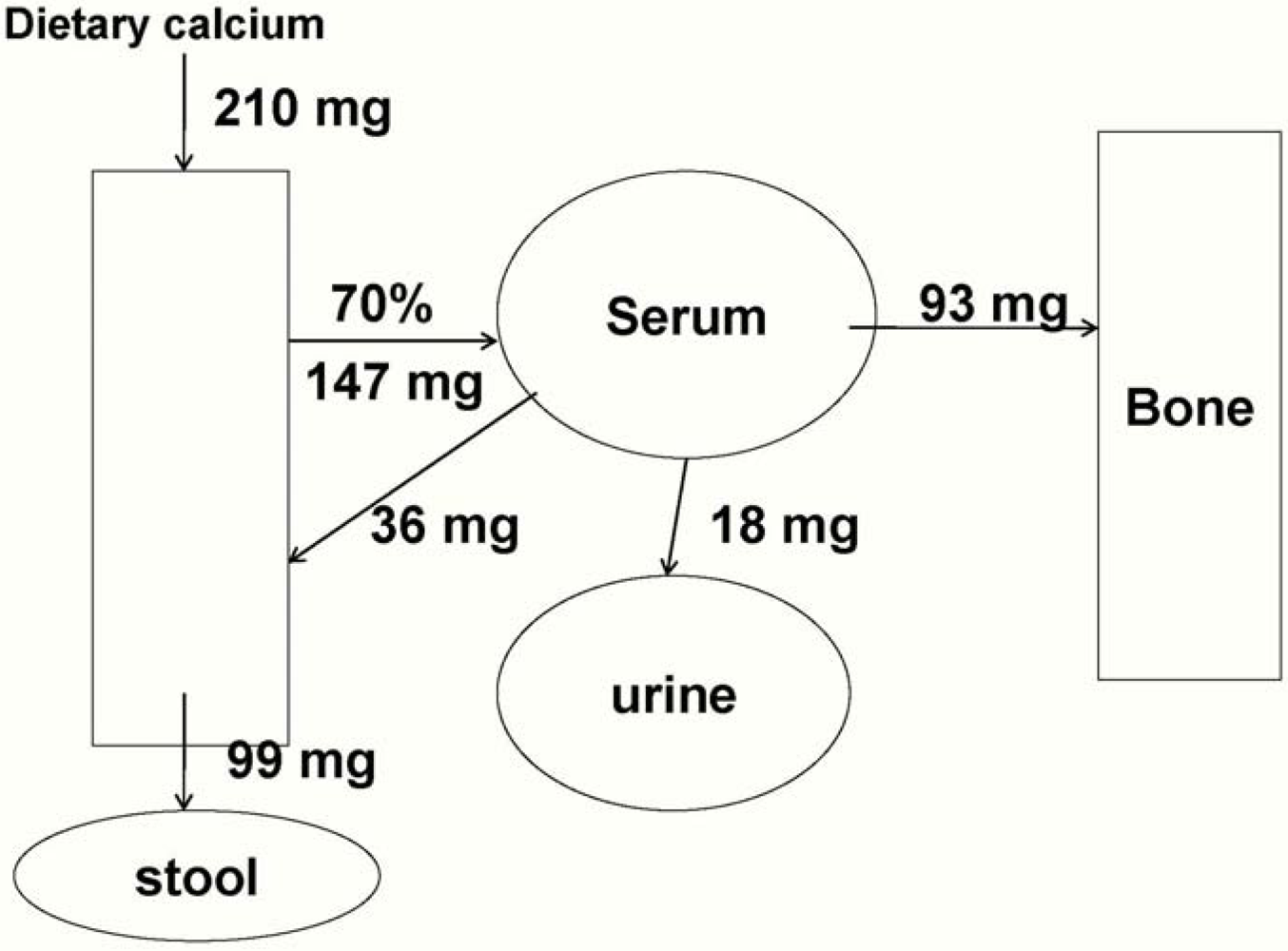
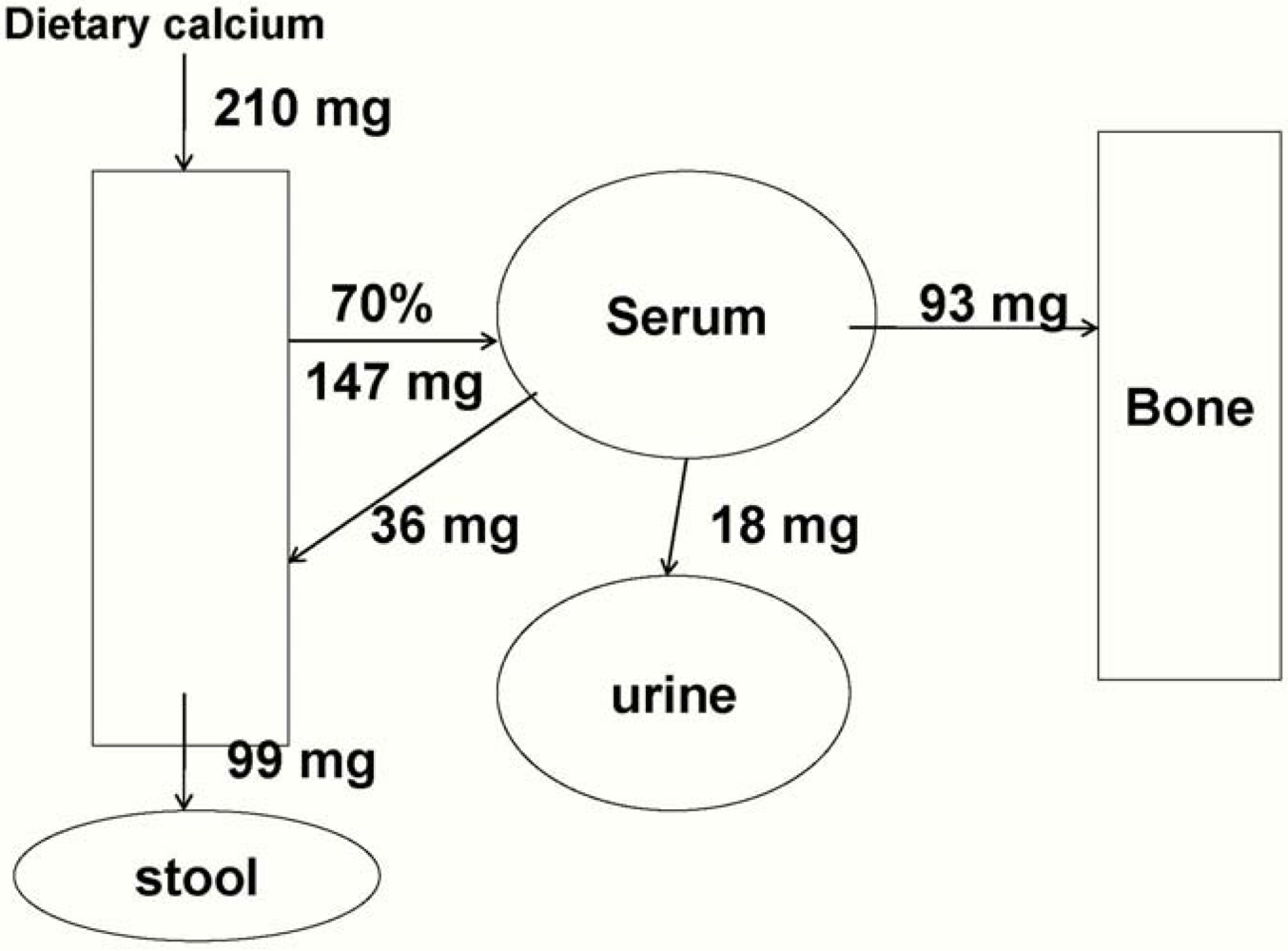
2.2. Post-infancy Calcium Absorption: Ages 1 to 3 Years
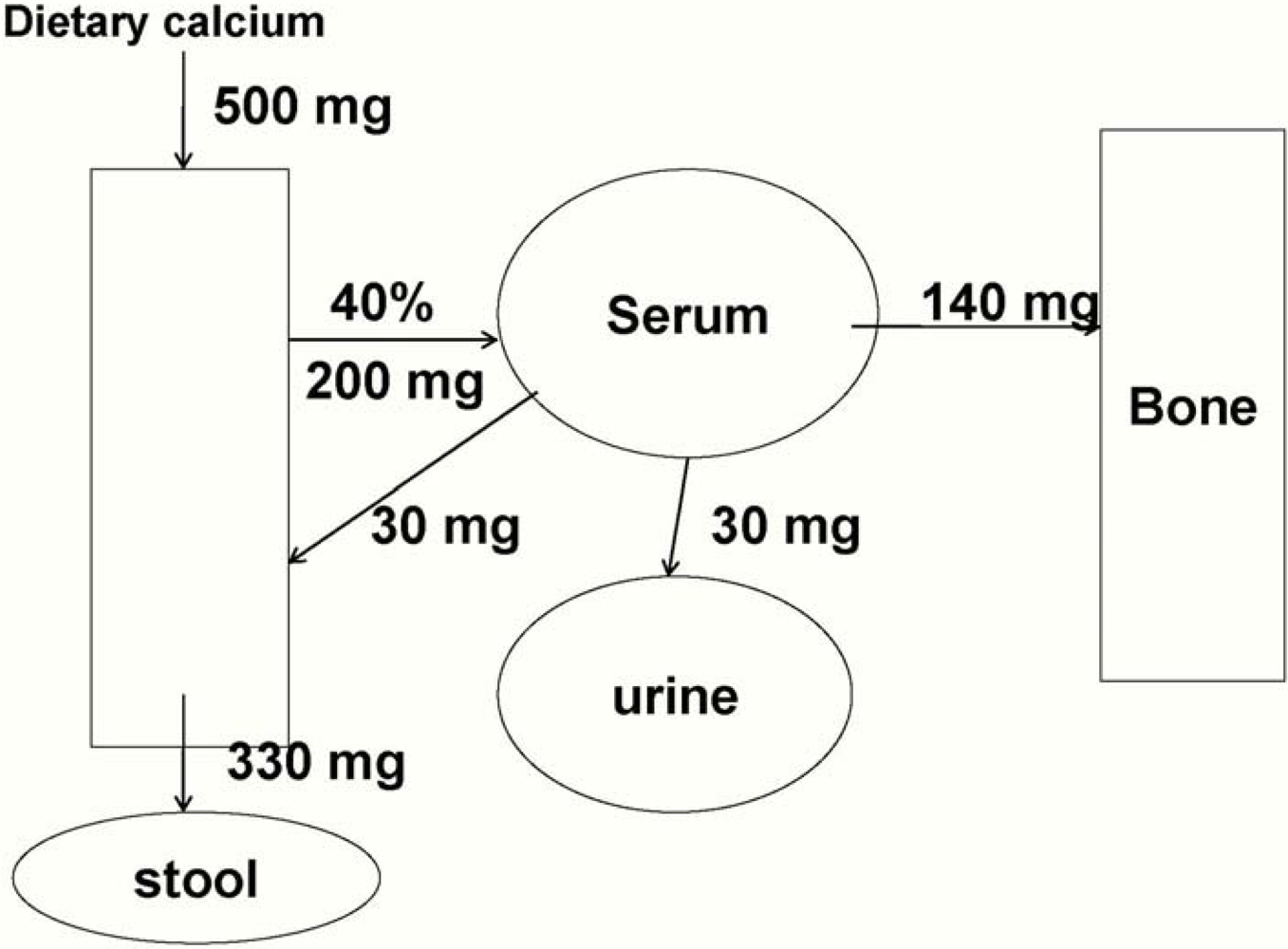
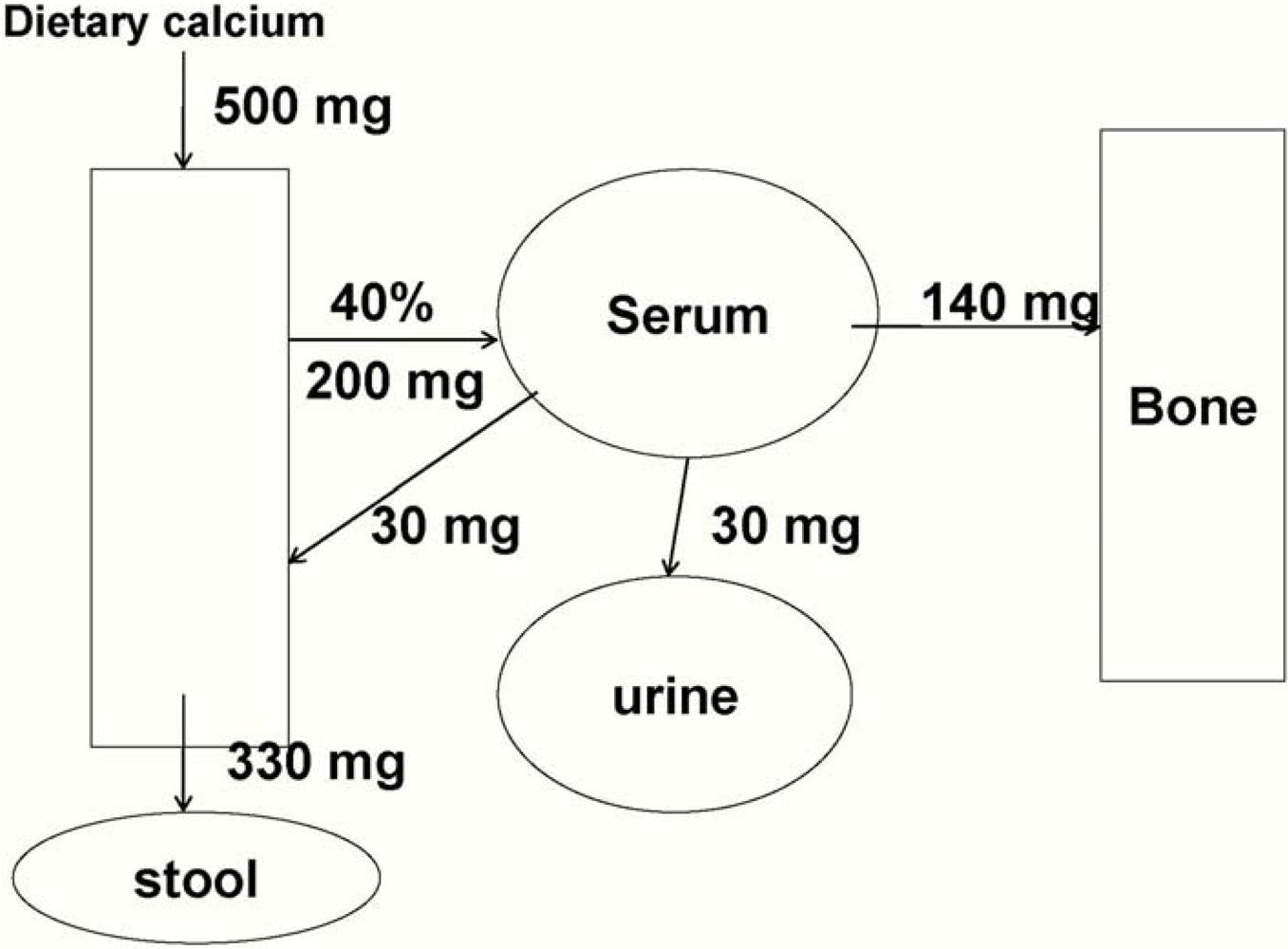
2.3. Calcium Absorption in Older Pre-Pubertal Children (4 to 8 years)
3. Conclusions
Acknowledgements
References and Notes
- Dietary reference intakes for Calcium, Magnesium, Phosphorus, Vitamin D, and Fluoride, Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, Food and Nutrition Board, Institute of Medicine; National Academy: Washington, DC, USA, 1997.
- Abrams, S.A. Using stable isotopes to assess mineral absorption and utilization by children. Am. J. Clin. Nutr. 1999, 70, 955–964. [Google Scholar]
- Abrams, S.A. Assessing mineral metabolism in children using stable isotopes. Pediatr. Blood. Cance. 2008, 50, 438–441. [Google Scholar]
- Abrams, S.A.; Sidbury, J.B.; Muenzer, A.; Esteban, N.V.; Vieira, N.E.; Yergey, A.L. Stable isotopic measurement of endogenous fecal calcium excretion in children. J. Pediatr. Gastroenterol. Nutr. 1991, 12, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Ellis, K.J.; Shypailo, R.J.; Hergenroeder, A.; Perez, M.; Abrams, S. Total body calcium and bone mineral content: Comparison of dual-energy X-ray absorptiometry (DXA) with neutron activation analysis (NAA). J. Bone. Miner. Res. 1996, 11, 843–848. [Google Scholar] [PubMed]
- Fomon, S.J.; Nelson, S.E. Calcium, phosphorus, magnesium, and sulfur. In Nutrition of Normal Infants; Fomon, S.J., Ed.; Mosby-Year Book, Inc.: St. Louis, MO, USA, 1993; pp. 192–218. [Google Scholar]
- Butte, N.F.; Wong, W.W.; Hopkinson, J.M.; Smith, E.O.; Ellis, K.J. Infant feeding mode affects early growth and body composition. Pediatrics 2000, 106, 1355–1366. [Google Scholar]
- Specker, B.L.; Beck, A.; Kalkwarf, H.; Ho, M. Randomized trial of varying mineral intake on total body bone mineral accretion during the first year of life. Pediatrics 1997, 99, E12. [Google Scholar]
- Abrams, S.A.; Griffin, I.J.; Davila, P.M. Calcium and zinc absorption from lactose-containing and lactose-free infant formulas. Am. J. Clin. Nutr. 2002, 76, 442–446. [Google Scholar]
- Abrams, S.A.; Wen J, Stuff, J.E. Absorption of calcium, zinc and iron from breast milk by 5- to 7-month-old infants. Pediatr. Res. 1997, 41, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Abrams, S.A. Nutritional rickets: An old disease returns. Nutr. Rev. 2002, 60, 111–115. [Google Scholar]
- Ellis, K.J.; Shypailo, R.J.; Wong, W.W.; Abrams, S.A. The reference child and adolescent models of body composition. A contemporary comparison. Ann. N. Y. Acad. Sci. 2000, 904, 374–382. [Google Scholar] [PubMed]
- Lynch, M.F.; Griffin, I.J.; Hawthorne, K.M.; Chen, Z.; Hamzo, M.; Abrams, S.A. Calcium balance in 1-4-y-old children. Am. J. Clin. Nutr. 2007, 85, 750–754. [Google Scholar]
- Graff, M.; Thacher, T.D.; Fischer, P.R.; Stadler, D.; brams, S. A. Calcium absorption in Nigerian children with rickets. Am. J. Clin. Nutr. 2004, 80, 1415–1421. [Google Scholar] [PubMed]
- Thacher, T.D.; Aliu, O.; Griffin, I.J.; Pam, S.D.; O’Brien, K.O.; Imade, G.E.; Abrams, S.A. Meals and dephytinization affect calcium and zinc absorption in Nigerian children with rickets. J. Nutr. 2009, 139, 926–932. [Google Scholar]
- Oramasionwu, G.E.; Thacher, T.D.; Pam, S.D.; Pettifor, J.M.; Abrams, S.A. Adaptation of calcium absorption during treatment of nutritional rickets in Nigerian children. Br. J. Nutr. 2008, 100, 387–392. [Google Scholar]
- Abrams, S.A.; Copeland, K.C.; Gunn, S.K.; Stuff, J.E.; Clarke, L.L.; Ellis, K.J. Calcium absorption and kinetics are similar in 7- and 8-year-old Mexican-American and Caucasian girls despite hormonal differences. J. Nutr. 1999, 129, 666–671. [Google Scholar] [PubMed]
- Abrams, S.A.; Griffin, I.J.; Davila, P.; Liang, L. Calcium fortification of breakfast cereal enhances calcium absorption in children without affecting iron absorption. J. Pediatr. 2001, 139, 522–526. [Google Scholar]
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Abrams, S.A. Calcium Absorption in Infants and Small Children: Methods of Determination and Recent Findings. Nutrients 2010, 2, 474-480. https://doi.org/10.3390/nu2040474
Abrams SA. Calcium Absorption in Infants and Small Children: Methods of Determination and Recent Findings. Nutrients. 2010; 2(4):474-480. https://doi.org/10.3390/nu2040474
Chicago/Turabian StyleAbrams, Steven A. 2010. "Calcium Absorption in Infants and Small Children: Methods of Determination and Recent Findings" Nutrients 2, no. 4: 474-480. https://doi.org/10.3390/nu2040474