Intakes of Total, Free, and Naturally Occurring Sugars in the French-Speaking Adult Population of the Province of Québec, Canada: The PREDISE Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. R24W Database
2.3. Sugar Differentiation
2.4. Plausibility of Self-Reported Energy Intakes
2.5. Statistical Analyses
3. Results
3.1. Mean Intakes of Total, Free, and Naturally Occurring Sugars
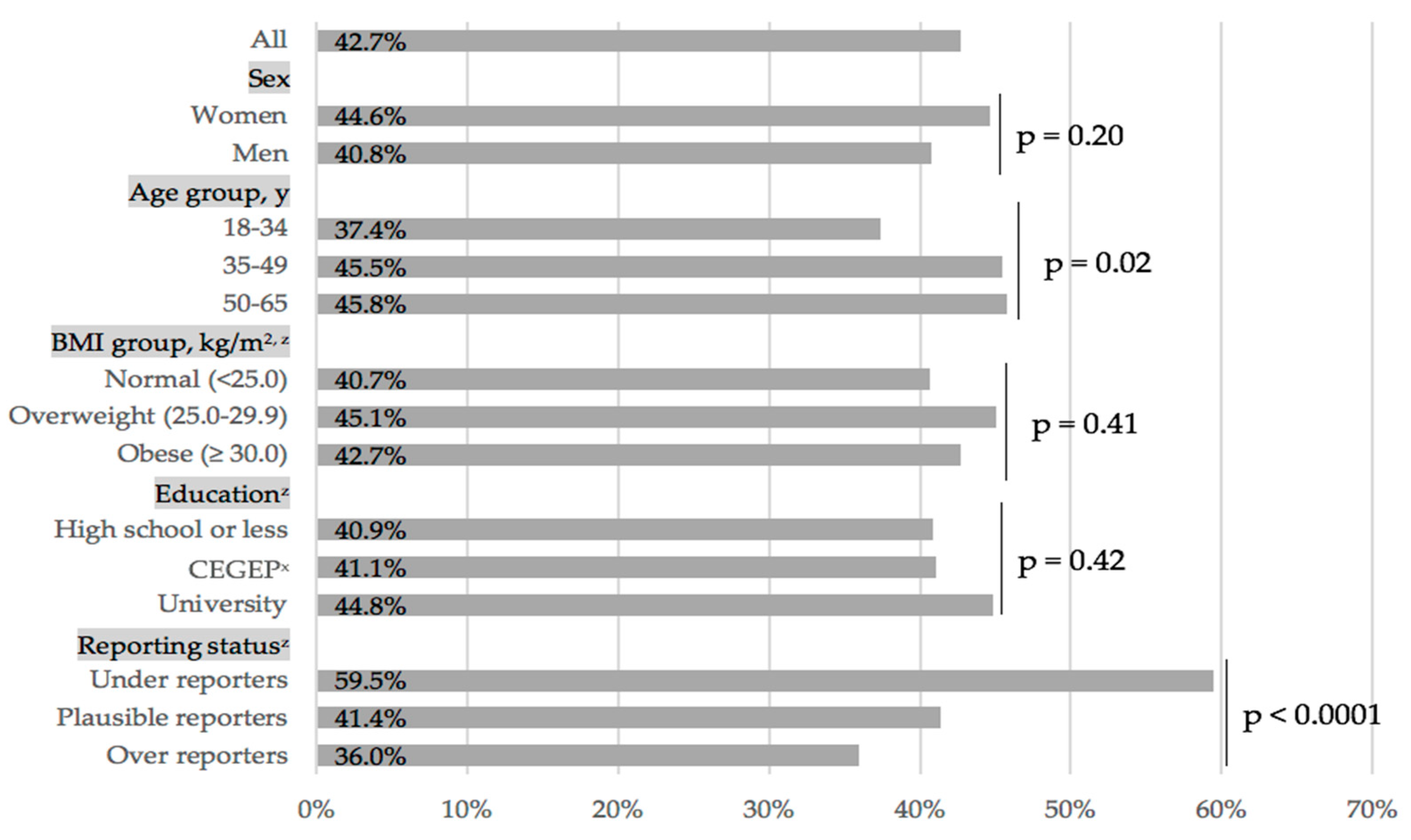
3.2. Proportion of Individuals Meeting WHO’s Recommendation
3.3. Correlations among Types of Sugars
4. Discussion
Strengths and Limits
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Te Morenga, L.A.; Howatson, A.J.; Jones, R.M.; Mann, J. Dietary sugars and cardiometabolic risk: Systematic review and meta-analyses of randomized controlled trials of the effects on blood pressure and lipids. Am. J. Clin. Nutr. 2014, 100, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G.; Iqbal, K.; Schwedhelm, C.; Boeing, H. Food groups and intermediate disease markers: A systematic review and network meta-analysis of randomized trials. Am. J. Clin. Nutr. 2018, 108, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Lampousi, A.M.; Knuppel, S.; Iqbal, K.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of all-cause mortality: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 1462–1473. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Hu, F.B. Sugar-Sweetened Beverages and Cardiometabolic Health: An Update of the Evidence. Nutrients 2019, 11, 1840. [Google Scholar] [CrossRef] [PubMed]
- Xi, B.; Huang, Y.; Reilly, K.H.; Li, S.; Zheng, R.; Barrio-Lopez, M.T.; Martinez-Gonzalez, M.A.; Zhou, D. Sugar-sweetened beverages and risk of hypertension and CVD: A dose-response meta-analysis. Br. J. Nutr. 2015, 113, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Mela, D.J.; Woolner, E.M. Perspective: Total, Added, or Free? What Kind of Sugars Should We Be Talking about? Adv. Nutr. 2018, 9, 63–69. [Google Scholar] [CrossRef]
- Clemens, R.A.; Jones, J.M.; Kern, M.; Lee, S.-Y.; Mayhew, E.J.; Slavin, J.L.; Zivanovic, S. Functionality of Sugars in Foods and Health. Compr. Rev. Food Sci. Food Saf. 2016, 15, 433–470. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Guideline: Sugars Intake for Adults and Children; 9241549025; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Health Canada. Canada’s Dietary Guidelines for for Health Professionals and Policy Makers. Available online: https://food-guide.canada.ca/en/guidelines/ (accessed on 9 September 2019).
- Chatelan, A.; Gaillard, P.; Kruseman, M.; Keller, A. Total, Added, and Free Sugar Consumption and Adherence to Guidelines in Switzerland: Results from the First National Nutrition Survey menuCH. Nutrients 2019, 11, 1117. [Google Scholar] [CrossRef]
- Mok, A.; Ahmad, R.; Rangan, A.; Louie, J.C.Y. Intake of free sugars and micronutrient dilution in Australian adults. Am. J. Clin. Nutr. 2018, 107, 94–104. [Google Scholar] [CrossRef] [Green Version]
- Kibblewhite, R.; Nettleton, A.; McLean, R.; Haszard, J.; Fleming, E.; Kruimer, D.; Te Morenga, L. Estimating Free and Added Sugar Intakes in New Zealand. Nutrients 2017, 9, 1292. [Google Scholar] [CrossRef] [PubMed]
- Sluik, D.; van Lee, L.; Engelen, A.I.; Feskens, E.J. Total, Free, and Added Sugar Consumption and Adherence to Guidelines: The Dutch National Food Consumption Survey 2007–2010. Nutrients 2016, 8, 70. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Canadian Nutrient File (CNF). Available online: https://food-nutrition.canada.ca/cnf-fce/index-eng.jsp (accessed on 9 September 2019).
- Langlois, K.; Garriguet, D.; Gonzalez, A.; Sinclair, S.; Colapinto, C.K. Change in total sugars consumption among Canadian children and adults. Health Rep. 2019, 30, 10–19. [Google Scholar] [PubMed]
- Hess, J.; Latulippe, M.E.; Ayoob, K.; Slavin, J. The confusing world of dietary sugars: Definitions, intakes, food sources and international dietary recommendations. Food Funct. 2012, 3, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Louie, J.C.; Moshtaghian, H.; Boylan, S.; Flood, V.M.; Rangan, A.M.; Barclay, A.W.; Brand-Miller, J.C.; Gill, T.P. A systematic methodology to estimate added sugar content of foods. Eur. J. Clin. Nutr. 2015, 69, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Brisbois, T.D.; Marsden, S.L.; Anderson, G.H.; Sievenpiper, J.L. Estimated intakes and sources of total and added sugars in the Canadian diet. Nutrients 2014, 6, 1899–1912. [Google Scholar] [CrossRef]
- Health Canada. Eating Well with Canada’s Food Guide. Available online: http://publications.gc.ca/collections/Collection/H164-38-1-2007E.pdf (accessed on 9 September 2019).
- Brassard, D.; Laramee, C.; Corneau, L.; Begin, C.; Belanger, M.; Bouchard, L.; Couillard, C.; Desroches, S.; Houle, J.; Langlois, M.F.; et al. Poor Adherence to Dietary Guidelines Among French-speaking Adults in the Province of Quebec, Canada: The PREDISE Study. Can. J. Cardiol. 2018, 34, 1665–1673. [Google Scholar] [CrossRef] [PubMed]
- Lafreniere, J.; Laramee, C.; Robitaille, J.; Lamarche, B.; Lemieux, S. Relative validity of a web-based, self-administered, 24-h dietary recall to evaluate adherence to Canadian dietary guidelines. Nutrition 2019, 57, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Lafreniere, J.; Laramee, C.; Robitaille, J.; Lamarche, B.; Lemieux, S. Assessing the relative validity of a new, web-based, self-administered 24 h dietary recall in a French-Canadian population. Public Health Nutr. 2018, 21, 2744–2752. [Google Scholar] [CrossRef] [Green Version]
- Lafrenière, J.; Lamarche, B.; Laramée, C.; Robitaille, J.; Lemieux, S. Validation of a newly automated web-based 24-h dietary recall using fully controlled feeding studies. BMC Nutr. 2017, 3, 34. [Google Scholar] [CrossRef]
- Jacques, S.; Lemieux, S.; Lamarche, B.; Laramee, C.; Corneau, L.; Lapointe, A.; Tessier-Grenier, M.; Robitaille, J. Development of a Web-Based 24-h Dietary Recall for a French-Canadian Population. Nutrients 2016, 8, 724. [Google Scholar] [CrossRef] [PubMed]
- Université Laval. Nutrific. Available online: https://nutrific.fsaa.ulaval.ca (accessed on 9 September 2019).
- United States Department of Agriculture. National Nutrient Database for Standard Reference. Available online: http://ndb.nal.usda.gov/ndb/search (accessed on 9 September 2019).
- Health Canada. Canadian Nutrient File Users’ Guide. Available online: www.healthcanada.gc.ca/cnf (accessed on 9 September 2019).
- Bernstein, J.T.; Schermel, A.; Mills, C.M.; L’Abbe, M.R. Total and Free Sugar Content of Canadian Prepackaged Foods and Beverages. Nutrients 2016, 8, 582. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.T.; Roberts, S.B.; Howarth, N.C.; McCrory, M.A. Effect of screening out implausible energy intake reports on relationships between diet and BMI. Obes. Res. 2005, 13, 1205–1217. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids; National Academy Press: Washington, DC, USA, 2005. [Google Scholar]
- Brassard, D.; Laramée, C.; Provencher, V.; Vohl, M.-C.; Robitaille, J.; Lemieux, S.; Lamarche, B. Consumption of low nutritive value foods and cardiometabolic risk factors among French-speaking adults from Quebec, Canada: The PREDISE study. Nutr. J. 2019, 18, 49. [Google Scholar] [CrossRef] [PubMed]
- Plante, C.; Rochette, L.; Blanchet, C. Les Apports et les Sources Alimentaires de Sucre, de Sodium et de Gras Saturés Chez les Québécois; Institut national de santé publique du Québec: Québec, QC, Canada, 2019; p. 34. [Google Scholar]
- Garriguet, D. Accounting for misreporting when comparing energy intake across time in Canada. Health Rep. 2018, 29, 3–12. [Google Scholar] [PubMed]
- Langlois, K.; Garriguet, D. Sugar consumption among Canadians of all ages. Health Rep. 2011, 22, 23–27. [Google Scholar] [PubMed]
- Ruiz, E.; Rodriguez, P.; Valero, T.; Avila, J.M.; Aranceta-Bartrina, J.; Gil, A.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Dietary Intake of Individual (Free and Intrinsic) Sugars and Food Sources in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 275. [Google Scholar] [CrossRef] [PubMed]
- Lei, L.; Rangan, A.; Flood, V.M.; Louie, J.C. Dietary intake and food sources of added sugar in the Australian population. Br. J. Nutr. 2016, 115, 868–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.; Smithers, L.G.; Braunack-Mayer, A.; Harford, J. How much free sugar do Australians consume? Findings from a national survey. Aust. N. Z. J. Public Health 2018, 42, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, A.; Murakami, K.; Asakura, K.; Uechi, K.; Sugimoto, M.; Wang, H.C.; Masayasu, S.; Sasaki, S. Estimation of Starch and Sugar Intake in a Japanese Population Based on a Newly Developed Food Composition Database. Nutrients 2018, 10, 1474. [Google Scholar] [CrossRef]
- Bowman, S.; Clemens, J.; Friday, J.; Schroeder, N.; Shimizu, M.; LaComb, R.; Moshfegh, A. Food Patterns Equivalents Intakes by Americans: What We Eat in America, NHANES 2003–2004 and 2015–2016; Dietary Data Brief Technical Report No. 20; Food Surveys Research Group: Beltsville, MD, USA, 2018. [Google Scholar]
- Kaartinen, N.E.; Simila, M.E.; Kanerva, N.; Valsta, L.M.; Harald, K.; Mannisto, S. Naturally occurring and added sugar in relation to macronutrient intake and food consumption: Results from a population-based study in adults. J. Nutr. Sci. 2017, 6, e7. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Thompson, F.E.; McGuire, L.C.; Pan, L.; Galuska, D.A.; Blanck, H.M. Sociodemographic and Behavioral Factors Associated with Added Sugars Intake among US Adults. J. Acad. Nutr. Diet. 2016, 116, 1589–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisberg, M.; Kovalskys, I.; Gomez, G.; Rigotti, A.; Sanabria, L.Y.C.; Garcia, M.C.Y.; Torres, R.G.P.; Herrera-Cuenca, M.; Zimberg, I.Z.; Koletzko, B.; et al. Total and Added Sugar Intake: Assessment in Eight Latin American Countries. Nutrients 2018, 10, 389. [Google Scholar] [CrossRef] [PubMed]
- Azais-Braesco, V.; Sluik, D.; Maillot, M.; Kok, F.; Moreno, L.A. A review of total & added sugar intakes and dietary sources in Europe. Nutr. J. 2017, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada. Food Labelling Changes. Available online: https://www.canada.ca/en/health-canada/services/food-labelling-changes.html (accessed on 9 September 2019).
- Yeung, C.H.; Louie, J.C. Methodology for the assessment of added/free sugar intake in epidemiological studies. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 271–277. [Google Scholar] [CrossRef]
- Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture; US Department of Agriculture, Agricultural Service: Washington, DC, USA, 2015. [Google Scholar]
- Te Morenga, L.; Mallard, S.; Mann, J. Dietary sugars and body weight: Systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ 2012, 346, e7492. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.T.; L’Abbe, M.R. Added sugars on nutrition labels: A way to support population health in Canada. CMAJ 2016, 188, E373–E374. [Google Scholar] [CrossRef]


{kind=link}
Step 1 (as per Step 1 of Bernstein et al. [29]): Foods that contain no total sugar:
| (7.9%) |
Step 2 (as per Step 2 of Bernstein et al. [29]): Foods that contain no free sugar in the ingredient list:
| (17.2%) |
Step 3 (as per Step 3 of Bernstein et al. [29]): Foods that contain no or minimal amounts of naturally occurring sugars:
| (6.5%) |
Step 4 (as per Step 4 of Bernstein et al. [29]): Foods that contain both naturally occurring and free sugars are compared to similar foods without free sugar ingredients (foods from steps 1 and 2):
| (6.3%) |
| (1) | |
| (2) | |
Step 5 (adapted from Step 5 of Bernstein et al. [29]): Foods that contain both naturally occurring sugars and free sugars for which no similar unsweetened food could be used for comparison:
| (16.0%) |
Step 6 (as per Step 6 of Bernstein et al. [29]): Items that could not be compared to similar foods in the FLIP database:
| (0.4%) |
| Step 7 (new step added): This step is used for mixed dishes manually created, based on Canadian Nutrient File (CNF) 2015. The ingredients and their quantity are specified for each recipe. Each ingredient is, itself, subjected to the sugar differentiation method (one of the steps above). | (45.6%) |
Step 8 (new step added): When neither of the steps above could be used to determine free sugar content in foods, an intuitive and logical method is used.
| (0.1%) |
| n (Weighted) | Total Sugars, g | Percentage of Total Sugars, % | Energy, kcal | Percentage of Daily Energy (%E) Provided by, %kcal | ||||
|---|---|---|---|---|---|---|---|---|
| Free Sugars | Naturally Occurring Sugars | Total Sugars | Free Sugars | Naturally Occurring Sugars | ||||
| All | 1147 | 116.4 (113.3–119.6) | 59.6 (58.6–60.6) | 40.4 (39.4–41.4) | 2402 (2362–2443) | 19.3 (18.9–19.6) | 11.7 (11.4–12.1) | 7.5 (7.3–7.7) |
| Sex | ||||||||
| Women | 576 | 97.7 (92.8–102.6) a | 57.6 (55.8–59.5) a | 42.4 (40.5–44.2) a | 2001 (1961–2042) a | 19.5 (18.7–20.3) | 11.4 (10.8–12.1) | 8.1 (7.6–8.5) a |
| Men | 571 | 124.9 (119.0–130.7) b | 63.0 (61.1–65.0) b | 37.0 (35.0–38.9) b | 2626 (2575–2678) b | 18.7 (18.0–19.5) | 12.2 (11.5–12.9) | 6.5 (6.1–6.9) b |
| p | <0.0001 | <0.0001 | <0.0001 | <0.0001 | 0.05 | 0.02 | <0.0001 | |
| Age group, years | ||||||||
| 18–34 | 408 | 120.5 (114.1–126.9) a | 63.5 (61.4–65.6) a | 36.5 (34.4–38.6) a | 2458 (2401–2514) a | 19.4 (18.6–20.3) | 12.6 (11.9–13.4) a | 6.8 (6.3–7.3) |
| 35–49 | 338 | 111.1 (104.7–117.5) b | 59.7 (57.4–62.0) b | 40.3 (38.0–42.6) b | 2329 (2278–2381) b | 18.9 (18.0–19.8) | 11.7 (10.8–12.5) a,b | 7.2 (6.7–7.7) |
| 50–65 | 400 | 102.2 (97.0–107.5)c | 57.8 (55.7–59.8) b | 42.2 (40.2–44.3) b | 2154 (2108–2200) c | 19.0 (18.2–19.8) | 11.2 (10.5–11.9) b | 7.8 (7.4–8.3) |
| p | <0.0001 | <0.0001 | <0.0001 | <0.0001 | 0.47 | 0.0006 | 0.001 | |
| Administrative region | ||||||||
| Estrie | 110 | 106.3 (97.6–115.1) | 59.1 (55.7–62.6) | 40.9 (37.4–44.3) | 2321 (2257–2385) | 18.1 (16.9–19.2) | 11.0 (9.9–12.1) | 7.0 (6.4–7.7) |
| Saguenay-Lac-Saint-Jean | 107 | 120.5 (111.0–130.1) | 63.1 (60.1–66.2) | 36.9 (33.8–39.9) | 2341 (2263–2420) | 20.4 (19.2–21.7) | 13.2 (12.1–14.4) | 7.2 (6.6–7.9) |
| Capitale-Nationale/Chaudière-Appalaches | 435 | 111.0 (105.9–116.1) | 59.5 (57.4–61.5) | 40.5 (38.5–42.6) | 2315 (2271–2360) | 19.0 (18.3–19.8) | 11.6 (10.9–12.3) | 7.4 (6.9–7.9) |
| Montréal | 397 | 110.5 (105.6–115.4) | 58.4 (56.5–60.4) | 41.5 (39.6–43.5) | 2321 (2275–2368) | 19.0 (18.3–19.8) | 11.4 (10.7–12.1) | 7.6 (7.2–8.1) |
| Mauricie | 99 | 108.0 (97.1–118.9) | 61.5 (58.2–64.8) | 38.5 (35.2–41.8) | 2269 (2162–2377) | 19.1 (17.6–20.6) | 11.9 (10.7–13.2) | 7.1 (6.3–8.0) |
| p | 108.0 (97.1–118.9) | 0.06 | 0.06 | 0.87 | 0.07 | 0.03 | 0.48 | |
| Body mass index, kg/m2 | ||||||||
| Normal (<25.0) | 453 | 106.1 (100.4–111.8) a | 59.3 (57.3–61.4) | 40.7 (38.6–42.7) | 2146 (2098–2194) a | 19.5 (18.7–20.3) | 11.9 (11.1–12.6) | 7.6 (7.2–8.1) |
| Overweight (25.0–29.9) | 383 | 106.5 (100.4–112.6) a | 59.3 (57.2–61.5) | 40.7 (38.5–42.8) | 2286 (2231.9–2340) a | 18.6 (17.8–19.5) | 11.3 (10.5–12.0) | 7.4 (6.8–7.9) |
| Obese (≥30.0) | 312 | 121.3 (115.2–127.4) b | 62.3 (60.1–64.4) | 37.7 (35.6–39.9) | 2509 (2457.7–2561) b | 19.2 (18.4–20.1) | 12.4 (11.6–13.2) | 6.9 (6.4–7.3) |
| p | <0.0001 | 0.03 | 0.03 | <0.0001 | 0.10 | 0.03 | 0.01 | |
| Education | ||||||||
| High school or less | 284 | 113.2 (106.5–120.0) | 62.7 (60.5–65.0) a | 37.3 (35.0–39.5) a | 2329 (2271–2388) | 19.1 (18.2–20.1) | 12.3 (11.4–13.1) | 6.9 (6.3–7.4) a |
| CEGEPx | 353 | 108.5 (102.9–114.2) | 60.9 (58.8–63.1) a | 39.1 (36.9–41.2) a | 2309 (2258–2361) | 18.8 (18.0–19.6) | 11.8 (11.0–12.5) | 7.0 (6.6–7.5) a |
| University | 510 | 112.0 (106.1–117.9) | 57.3 (55.2–59.4) b | 42.7 (40.6–44.8)b | 2302 (2255–2350) | 19.4 (18.6–20.3) | 11.5 (10.7–12.2) | 7.9 (7.5–8.4) b |
| p | 0.32 | <0.0001 | <0.0001 | 0.70 | 0.27 | 0.22 | 0.0001 | |
| Reporting status | ||||||||
| Under reporters | 185 | 64.0 (58.1–69.8) a | 55.1 (52.1–58.2) a | 44.9 (41.8–47.9) a | 1471 (1414–1528) a | 17.9 (16.8–19.1) | 10.2 (9.2–11.2) a | 7.7 (7.1–8.4) |
| Plausible reporters | 613 | 109.7 (104.9–114.6) b | 61.7 (59.9–63.5) b | 38.3 (36.5–40.1) b | 2264 (2226.0–2302) b | 19.4 (18.7–20.2) | 12.3 (11.6–13.0) b | 7.1 (6.7–7.5) |
| Over reporters | 348 | 160.1 (152.5–167.8) c | 64.1 (62.1–66.1) b | 35.9 (33.9–37.9) b | 35.9 (33.9–37.9) b | 20.0 (19.2–20.8) | 13.0 (12.3–13.7) b | 7.0 (6.5–7.5) |
| p | <0.0001 | <0.0001 | <0.0001 | <0.0001 | 0.005 | <0.0001 | 0.14 | |
| Total Sugars | Free Sugars | Naturally Occurring Sugars | ||
|---|---|---|---|---|
| Overall diet | total sugars | - | 0.79 (p < 0.0001) | 0.45 (p < 0.0001) |
| free sugars | - | - | −0.20 (p < 0.0001) | |
| Foods | total sugars | - | 0.69 (p < 0.0001) | 0.66 (p < 0.0001) |
| free sugars | - | - | −0.09 (p = 0.01) | |
| Drinks | total sugars | - | 0.91 (p < 0.0001) | 0.39 (p < 0.0001) |
| free sugars | - | - | −0.02 (p = 0.61) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bergeron, A.; Labonté, M.-È.; Brassard, D.; Bédard, A.; Laramée, C.; Robitaille, J.; Desroches, S.; Provencher, V.; Couillard, C.; Vohl, M.-C.; et al. Intakes of Total, Free, and Naturally Occurring Sugars in the French-Speaking Adult Population of the Province of Québec, Canada: The PREDISE Study. Nutrients 2019, 11, 2317. https://doi.org/10.3390/nu11102317
Bergeron A, Labonté M-È, Brassard D, Bédard A, Laramée C, Robitaille J, Desroches S, Provencher V, Couillard C, Vohl M-C, et al. Intakes of Total, Free, and Naturally Occurring Sugars in the French-Speaking Adult Population of the Province of Québec, Canada: The PREDISE Study. Nutrients. 2019; 11(10):2317. https://doi.org/10.3390/nu11102317
Chicago/Turabian StyleBergeron, Amélie, Marie-Ève Labonté, Didier Brassard, Alexandra Bédard, Catherine Laramée, Julie Robitaille, Sophie Desroches, Véronique Provencher, Charles Couillard, Marie-Claude Vohl, and et al. 2019. "Intakes of Total, Free, and Naturally Occurring Sugars in the French-Speaking Adult Population of the Province of Québec, Canada: The PREDISE Study" Nutrients 11, no. 10: 2317. https://doi.org/10.3390/nu11102317