Exploration of the Association between Dietary Fiber Intake and Hypertension among U.S. Adults Using 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines: NHANES 2007–2014


Abstract
:1. Introduction
2. Materials and Methods
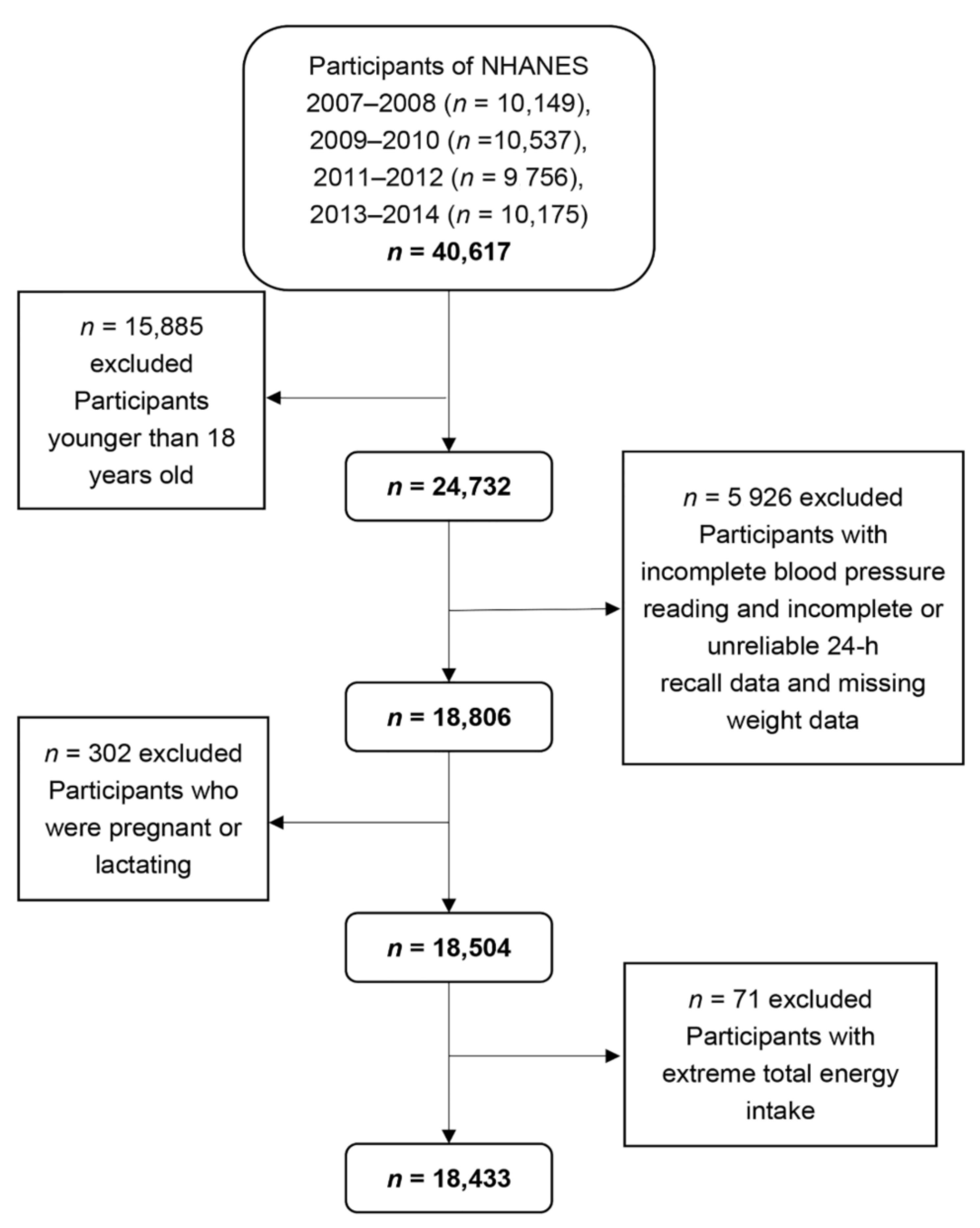
2.1. Study Population
2.2. Blood Pressure Measurements
2.3. Definition of Hypertension
2.4. Dietary Fiber Intake
2.5. Other Potential Factors for Hypertension
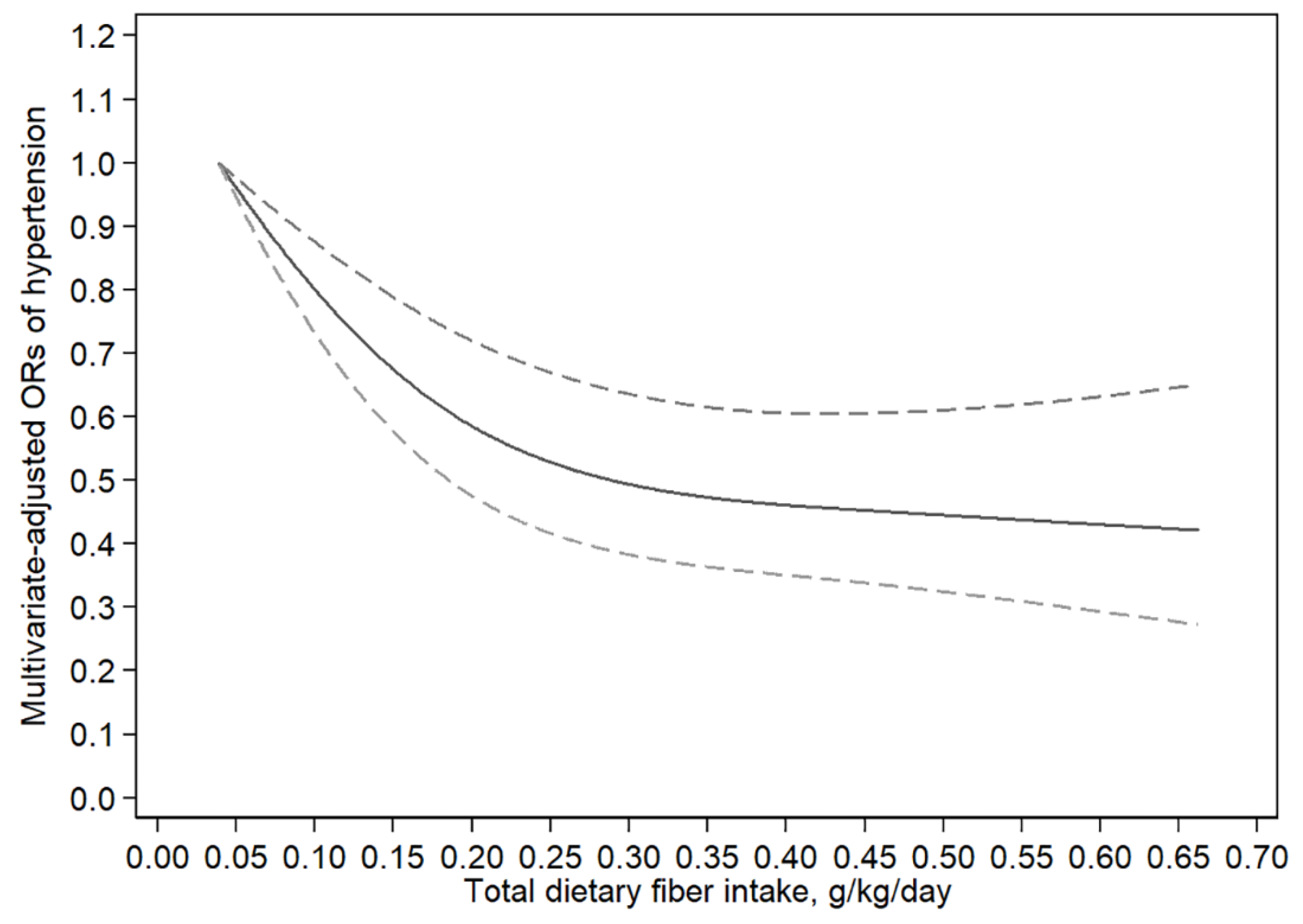
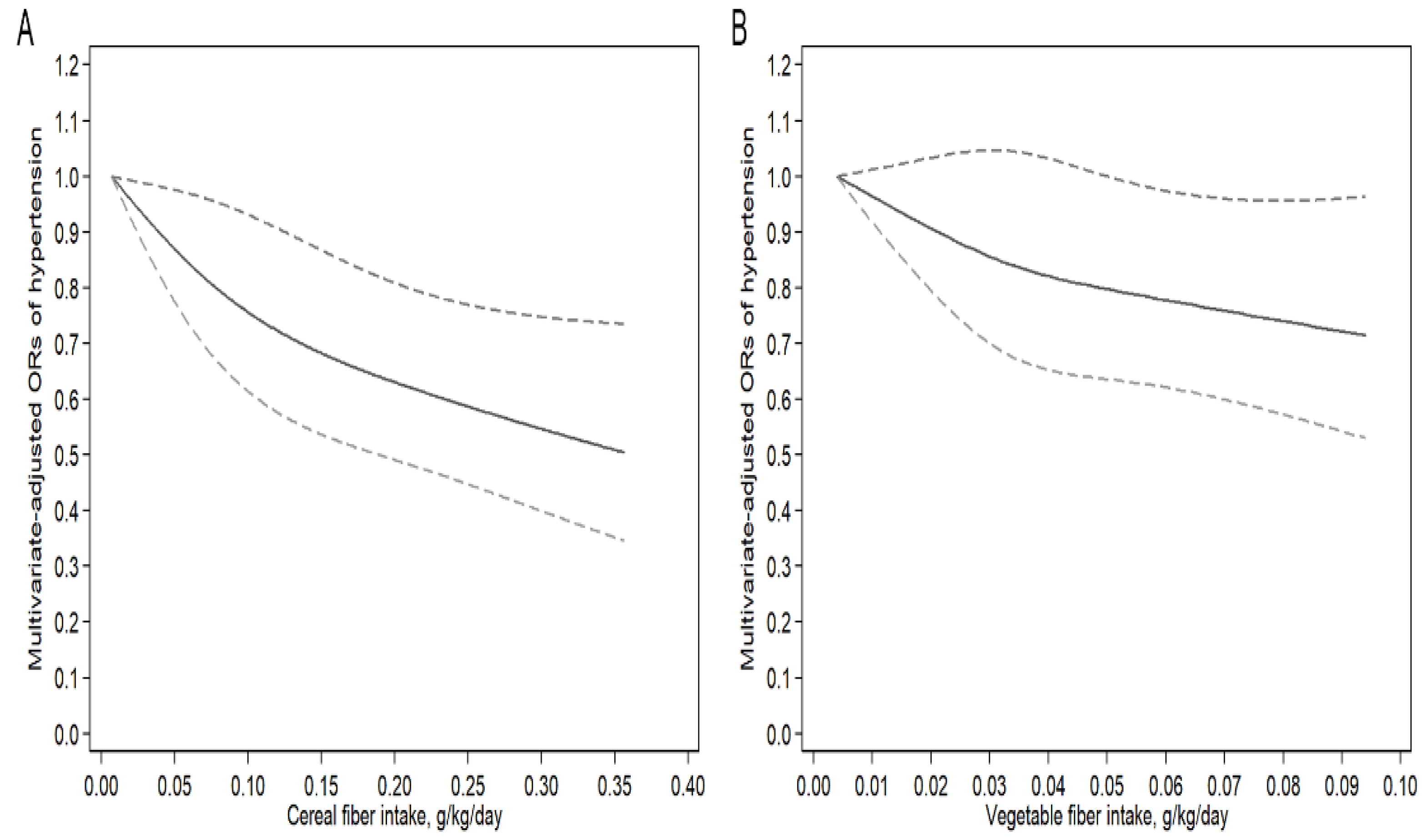
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APHA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [PubMed]
- WHO. A Global Brief on Hypertension. Available online: http://www.who.int/cardiovascular_diseases/publications/global_brief_hypertension/en/ (accessed on 26 July 2018).
- Centers for Disease, Control, Prevention. Vital Signs: Prevalence, Treatment, and Control of Hypertension--United States, 1999–2002 and 2005–2008. MMWR Morb. Mortal. Wkly. Rep. 2011, 60, 103–108. [Google Scholar]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A Comparative Risk Assessment of Burden of Disease and Injury Attributable to 67 Risk Factors and Risk Factor Clusters in 21 Regions, 1990–2010: A Systematic Analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Li, B.R.; Li, F.; Wang, L.F.; Zhang, D.F. Fruit and Vegetables Consumption and Risk of Hypertension: A Meta-Analysis. J. Clin. Hypertens. 2016, 18, 468–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, J.; Klag, M.J.; Whelton, P.K.; Mo, J.P.; Chen, J.Y.; Qian, M.C.; Mo, P.S.; He, G.Q. Oats and Buckwheat Intakes and Cardiovascular-Disease Risk-Factors in an Ethnic-Minority of China. Am. J. Clin. Nutr. 1995, 61, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Kochar, J.; Gaziano, J.M.; Djousse, L. Breakfast Cereals and Risk of Hypertension in the Physicians’ Health Study I. Clin. Nutr. 2012, 31, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Borgi, L.; Muraki, I.; Satija, A.; Willett, W.C.; Rimm, E.B.; Forman, J.P. Fruit and Vegetable Consumption and the Incidence of Hypertension in Three Prospective Cohort Studies. Hypertension 2016, 67, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.Y.; Davidge, S.T.; Wu, J.P. Bioactive Natural Constituents from Food Sources—Potential Use in Hypertension Prevention and Treatment. Crit. Rev. Food Sci. Nutr. 2013, 53, 615–630. [Google Scholar] [CrossRef] [PubMed]
- Wolk, A.; Manson, J.E.; Stampfer, M.J.; Colditz, G.A.; Hu, F.B.; Speizer, F.E.; Hennekens, C.H.; Willett, W.C. Long-Term Intake of Dietary Fiber and Decreased Risk of Coronary Heart Disease among Women. J. Am. Med. Assoc. 1999, 281, 1998–2004. [Google Scholar] [CrossRef]
- Larsson, S.C.; Mannisto, S.; Virtanen, M.J.; Kontto, J.; Albanes, D.; Virtamo, J. Dietary Fiber and Fiber-Rich Food Intake in Relation to Risk of Stroke in Male Smokers. Eur. J. Clin. Nutr. 2009, 63, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Kumanyika, S.K.; Lemaitre, R.N.; Olson, J.L.; Burke, G.L.; Siscovick, D.S. Cereal, Fruit, and Vegetable Fiber Intake and the Risk of Cardiovascular Disease in Elderly Individuals. J. Am. Med. Assoc. 2003, 289, 1659–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buil-Cosiales, P.; Martinez-Gonzalez, M.A.; Ruiz-Canela, M.; Diez-Espino, J.; Garcia-Arellano, A.; Toledo, E. Consumption of Fruit or Fiber-Fruit Decreases the Risk of Cardiovascular Disease in a Mediterranean Young Cohort. Nutrients 2017, 9, 295. [Google Scholar] [CrossRef] [PubMed]
- Aljuraiban, G.S.; Griep, L.M.; Chan, Q.; Daviglus, M.L.; Stamler, J.; Van Horn, L.; Elliott, P.; Frost, G.S. Total, Insoluble and Soluble Dietary Fibre Intake in Relation to Blood Pressure: The Intermap Study—Corrigendum. Br. J. Nutr. 2015, 114, 1534. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Beunza, J.J.; Bes-Rastrollo, M.; Pajares, R.M.; Martinez-Gonzalez, M.A. Vegetable Protein and Fiber from Cereal Are Inversely Associated with the Risk of Hypertension in a Spanish Cohort. Arch. Med. Res. 2006, 37, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.E.; Greenwood, D.C.; Threapleton, D.E.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.E.; Gale, C.P.; Burley, V.J. Effects of Dietary Fibre Type on Blood Pressure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials of Healthy Individuals. J. Hypertens. 2015, 33, 897–911. [Google Scholar] [CrossRef] [PubMed]
- Lairon, D.; Arnault, N.; Bertrais, S.; Planells, R.; Clero, E.; Hercberg, S.; Boutron-Ruault, M.C. Dietary Fiber Intake and Risk Factors for Cardiovascular Disease in French Adults. Am. J. Clin. Nutr. 2005, 82, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Streppel, M.T.; Arends, L.R.; van’t Veer, P.; Grobbee, D.E.; Geleijnse, J.M. Dietary Fiber and Blood Pressure—A Meta-Analysis of Randomized Placebo-Controlled Trials. Arch. Intern. Med. 2005, 165, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Masala, G.; Bendinelli, B.; Versari, D.; Saieva, C.; Ceroti, M.; Santagiuliana, F.; Caini, S.; Salvini, S.; Sera, F.; Taddei, S.; et al. Anthropometric and Dietary Determinants of Blood Pressure in over 7000 Mediterranean Women: The European Prospective Investigation into Cancer and Nutrition-Florence Cohort. J. Hypertens. 2008, 26, 2112–2120. [Google Scholar] [CrossRef] [PubMed]
- Davy, B.M.; Melby, C.L.; Beske, S.D.; Ho, R.C.; Davrath, L.R.; Davy, K.P. Oat Consumption Does Not Affect Resting Casual and Ambulatory 24-H Arterial Blood Pressure in Men with High-Normal Blood Pressure to Stage I Hypertension. J. Nutr. 2002, 132, 394–398. [Google Scholar] [CrossRef] [PubMed]
- He, J.A.; Klag, M.J.; Whelton, P.K.; Chen, J.Y.; Qian, M.C.; He, G.Q. Dietary Macronutrients and Blood Pressure in Southwestern China. J. Hypertens. 1995, 13, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- Vernay, M.; Aidara, M.; Salanave, B.; Deschamps, V.; Malon, A.; Oleko, A.; Mallion, J.M.; Hercberg, S.; Castetbon, K. Diet and Blood Pressure in 18–74-Year-Old Adults: The French Nutrition and Health Survey (Enns, 2006–2007). J. Hypertens. 2012, 30, 1920–1927. [Google Scholar] [CrossRef] [PubMed]
- Ascherio, A.; Hennekens, C.; Willett, W.C.; Sacks, F.; Rosner, B.; Manson, J.A.; Witteman, J.; Stampfer, M.J. Prospective Study of Nutritional Factors, Blood Pressure, and Hypertension among Us Women. Hypertension 1996, 27, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease, Control, and Prevention. National Health and Nutrition Examination Survey. Survey Methods and Analytic Guidelines. Available online: https://wwwn.cdc.gov/nchs/nhanes/analyticguidelines.aspx (accessed on 26 July 2018).[Green Version]
- Centers for Disease, Control, and Prevention. National Health and Nutrition Examination Survey. Questionnaires, Datasets, and Related Documentation. Available online: https://wwwn.cdc.gov/nchs/nhanes/Default.aspx (accessed on 26 July 2018).[Green Version]
- Centers for Disease, Control, and Prevention. Physician Examination Procedures Manual. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_05_06/PE.pdf (accessed on 26 July 2018).
- Wang, J.W.; Zhang, L.X.; Wang, F.; Liu, L.S.; Wang, H.Y. Prevalence, Awareness, Treatment, and Control of Hypertension in China: Results from a National Survey. Am. J. Hypertens. 2014, 27, 1355–1361. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture, Agricultural Research Service. Usda Food and Nutrient Database for Dietary Studies. Available online: https://www.cdc.gov/nchs/tutorials/dietary/SurveyOrientation/ResourceDietaryAnalysis/intro.htm (accessed on 26 July 2018).
- Ascherio, A.; Rimm, E.B.; Giovannucci, E.L.; Colditz, G.A.; Rosner, B.; Willett, W.C.; Sacks, F.; Stampfer, M.J. A Prospective Study of Nutritional Factors and Hypertension among Us Men. Circulation 1992, 86, 1475–1484. [Google Scholar] [CrossRef] [PubMed]
- Ascherio, A.; Stampfer, M.J.; Colditz, G.A.; Willett, W.C.; McKinlay, J. Nutrient Intakes and Blood Pressure in Normotensive Males. Int. J. Epidemiol. 1991, 20, 886–891. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Non-Hypertension | Hypertension | p Value | |
|---|---|---|---|
| Number of Participants (%) 1 | 9458 (55.07) | 8975 (44.93) | |
| Age group (%) 1 | <0.01 | ||
| 18–39 years | 5212 (80.79) | 1244 (19.21) | |
| 40–59 years | 2956 (51.50) | 3026 (48.50) | |
| ≥60 years | 1290 (24.31) | 4705 (75.69) | |
| Sex (%) 1 | <0.01 | ||
| Male | 4403 (52.89) | 4612 (47.11) | |
| Female | 5055 (57.64) | 4363 (42.36) | |
| Race (%) 1 | <0.01 | ||
| Mexican American | 1670 (68.25) | 1041 (31.75) | |
| Other Hispanic | 1083 (66.74) | 767 (33.26) | |
| Non-Hispanic White | 4108 (53.47) | 4253 (46.53) | |
| Non-Hispanic Black | 1584 (45.59) | 2302 (54.41) | |
| Other race | 1013 (62.27) | 612 (37.73) | |
| Educational level (%) 1 | <0.01 | ||
| Below high school | 2197 (51.06) | 2434 (48.94) | |
| High school | 2040 (51.15) | 2231 (48.85) | |
| Above high school | 5213 (57.68) | 4301 (42.32) | |
| Household income (%) 1 | <0.01 | ||
| <$20,000 | 1770 (50.81) | 2066 (49.19) | |
| $20,000 to <50,000 | 3035 (52.04) | 3033 (47.96) | |
| $50,000 to <75,000 | 1696 (54.77) | 1608 (45.23) | |
| ≥$75,000 | 2562 (59.38) | 1929 (40.62) | |
| Body mass index (%) 1 | <0.01 | ||
| <25 kg/m2 | 3660 (70.65) | 1850 (29.35) | |
| 25 to <30 kg/m2 | 3113 (55.21) | 2917 (44.79) | |
| ≥30 kg/m2 | 2677 (41.57) | 4178 (58.43) | |
| Smoking Status (%) 1 | <0.01 | ||
| Never | 1981 (60.18) | 1578 (39.82) | |
| Currently | 5194 (57.02) | 4623 (42.98) | |
| Former | 1682 (43.11) | 2708 (56.89) | |
| Body weight (kg) 2 | 78.04 (0.36) | 87.37 (0.36) | <0.01 |
| Total energy intake (kcal/day) 2 | 2146.50 (13.10) | 2048.12 (13.42) | <0.01 |
| Total fiber intake (mg/kg/day) 2 | 236.70 (2.94) | 205.88 (2.51) | <0.01 |
| Cereal fiber intake (mg/kg/day) 2 | 107.74 (1.56) | 88.79 (1.32) | <0.01 |
| Vegetable fiber intake (mg/kg/day) 2 | 48.91 (0.84) | 45.18 (0.69) | <0.01 |
| Fruit fiber intake (mg/kg/day) 2 | 43.52 (0.94) | 38.80 (0.85) | <0.01 |
| Cases/Participants 1 | Weighted Prevalence (%) 2 | Crude 3 | Model 1 3 | Model 2 3 | |
|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |||
| Total fiber (g/kg/day) | |||||
| <0.147 | 3343/6144 | 50.94 | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| 0.147 to <0.245 | 3092/6144 | 46.15 | 0.83 (0.73–0.94) ** | 0.67 (0.58–0.78) ** | 0.82 (0.69–0.96) * |
| ≥0.245 | 2540/6145 | 37.4 | 0.58 (0.51–0.64) ** | 0.42 (0.37–0.48) ** | 0.62 (0.52–0.75) ** |
| Cereal fiber (g/kg/day) | |||||
| <0.057 | 3392/6108 | 50.65 | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| 0.057 to <0.108 | 3032/6109 | 46.62 | 0.85 (0.76–0.95) ** | 0.76 (0.67–0.86) ** | 0.90 (0.78–1.03) |
| ≥0.108 | 2503/6110 | 37.22 | 0.58 (0.52–0.65) ** | 0.55 (0.47–0.64) ** | 0.80 (0.67–0.96) * |
| Vegetable fiber (g/kg/day) | |||||
| <0.023 | 2877/5785 | 46.39 | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| 0.023 to <0.050 | 2929/5787 | 46.09 | 0.99 (0.87–1.12) | 0.84 (0.73–0.98) * | 0.91 (0.78–1.07) |
| ≥0.050 | 2694/5787 | 42.74 | 0.86 (0.76–0.97) * | 0.65 (0.56–0.75) ** | 0.82 (0.69–0.98) * |
| Fruit fiber (g/kg/day) | |||||
| <0.018 | 2320/4563 | 47.12 | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| 0.018 to <0.046 | 2328/4563 | 46.95 | 0.99 (0.88–1.12) | 0.82 (0.71–0.95) * | 0.94 (0.80–1.09) |
| ≥0.046 | 2168/4565 | 42.27 | 0.82 (0.71–0.95) ** | 0.60 (0.50–0.72) ** | 0.86 (0.71–1.04) |
| Total Fiber (g/kg/day) | Cases/Participants 1 | Weighted Prevalence (%) 2 | Crude 3 | Model 1 3 | Model 2 3 |
|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |||
| 18 ≤ age < 45 years | |||||
| <0.147 | 882/2796 | 31.64 | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| 0.147 to <0.245 | 550/2541 | 21.93 | 0.61 (0.51–0.73) ** | 0.55 (0.46–0.67) ** | 0.69 (0.55–0.88) ** |
| ≥0.245 | 398/2637 | 15.52 | 0.40 (0.33–0.48) ** | 0.33 (0.27–0.41) ** | 0.50 (0.38–0.67) ** |
| 45 ≤ age < 65 years | |||||
| <0.147 | 1397/2068 | 65.1 | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| 0.147 to <0.245 | 1258/2055 | 58.67 | 0.76 (0.61–0.95) * | 0.76 (0.60–0.93) * | 0.88 (0.69–1.12) |
| ≥0.245 | 1054/2093 | 47.36 | 0.48 (0.40–0.58) ** | 0.46 (0.38–0.56) ** | 0.69 (0.53–0.90) ** |
| Age ≥ 65 years | |||||
| <0.147 | 1064/1280 | 81.39 | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| 0.147 to <0.245 | 1284/1548 | 80.5 | 0.94 (0.66–1.35) | 0.93 (0.66–1.30) | 1.11 (0.75–1.66) |
| ≥0.245 | 1088/1415 | 73.74 | 0.64 (0.47–0.88) ** | 0.61 (0.45–0.81) * | 0.83 (0.53–1.29) |
| Male | |||||
| <0.147 | 1670/2883 | 54.19 | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| 0.147 to <0.245 | 1560/2962 | 49.14 | 0.82 (0.69–0.96) * | 0.72 (0.60–0.87) * | 0.88 (0.71–1.10) |
| ≥0.245 | 1382/3170 | 39.06 | 0.54 (0.46–0.64) ** | 0.45 (0.38–0.55) ** | 0.66 (0.52–0.84) ** |
| Female | |||||
| <0.147 | 1673/3261 | 48.07 | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| 0.147 to <0.245 | 1532/3182 | 43.32 | 0.83 (0.70–0.98) * | 0.62 (0.52–0.75) ** | 0.74 (0.59–0.94) ** |
| ≥0.245 | 1158/2978 | 35.69 | 0.60 (0.51–0.70) ** | 0.38 (0.32–0.45) ** | 0.58 (0.45–0.75) ** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, B.; Shi, X.; Wang, T.; Zhang, D. Exploration of the Association between Dietary Fiber Intake and Hypertension among U.S. Adults Using 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines: NHANES 2007–2014. Nutrients 2018, 10, 1091. https://doi.org/10.3390/nu10081091
Sun B, Shi X, Wang T, Zhang D. Exploration of the Association between Dietary Fiber Intake and Hypertension among U.S. Adults Using 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines: NHANES 2007–2014. Nutrients. 2018; 10(8):1091. https://doi.org/10.3390/nu10081091
Chicago/Turabian StyleSun, Baoqi, Xiaoyan Shi, Tong Wang, and Dongfeng Zhang. 2018. "Exploration of the Association between Dietary Fiber Intake and Hypertension among U.S. Adults Using 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines: NHANES 2007–2014" Nutrients 10, no. 8: 1091. https://doi.org/10.3390/nu10081091
APA StyleSun, B., Shi, X., Wang, T., & Zhang, D. (2018). Exploration of the Association between Dietary Fiber Intake and Hypertension among U.S. Adults Using 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines: NHANES 2007–2014. Nutrients, 10(8), 1091. https://doi.org/10.3390/nu10081091