Design and Reproducibility of a Mini-Survey to Evaluate the Quality of Food Intake (Mini-ECCA) in a Mexican Population

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Study Design
2.2. Design of the Mini-ECCA Questionnaire
2.3. Data Collection Procedures and Strategies
2.4. Statistical Analysis
3. Results
3.1. Description of the Population
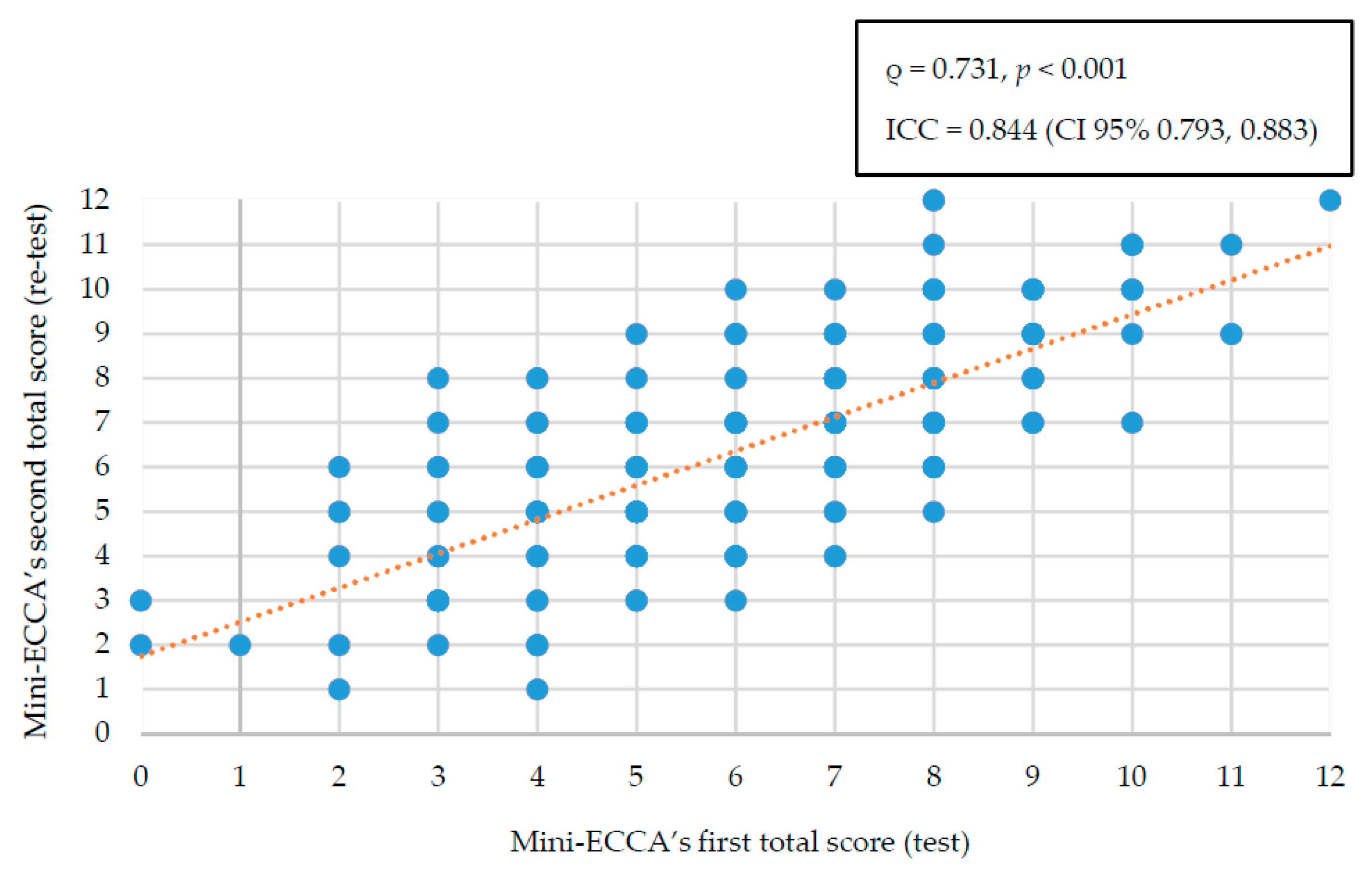
3.2. Reproducibility and Concordance of the Mini-ECCA
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Alkerwi, A. Diet quality concept. Nutrition 2014, 30, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Gil, A.; de Victoria, E.M.; Olza, J. Indicators for the evaluation of diet quality. Nutr. Hosp. 2015, 31 (Suppl. S3), 128–144. [Google Scholar] [CrossRef] [PubMed]
- Macedo-Ojeda, G.; Márquez-Sandoval, F.; Fernández-Ballart, J.; Vizmanos, B. The Reproducibility and relative valdity of a Mexican Diet Index (ICDMx) for the Assessment of the Habitual Diet of Adults. Nutrients 2016, 8, 516. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K. The Healthy Eating Index: Design and applications. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Patterson, R.E.; Haines, P.S.; Popkin, B.M. Diet quality index: Capturing a multidimensional behavior. J. Am. Diet. Assoc. 1994, 94, 57–64. [Google Scholar] [CrossRef]
- Huijbregts, P.; Feskens, E.; Räsänen, L.; Fidanza, F.; Nissinen, A.; Menotti, A.; Kromhout, D. Dietary pattern and 20 year mortality in elderly men in Finland, Italy, and The Netherlands: Longitudinal cohort study. BMJ 1997, 315, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Ponce, X.; Rodriguez-Ramirez, S.; Mundo-Rosas, V.; Shamah, T.; Barquera, S.; de Cossio, T.G. Dietary quality indices vary with sociodemographic variables and anthropometric status among Mexican adults: A cross-sectional study. Results from the 2006 National Health and Nutrition Survey. Public Health Nutr. 2013, 17, 1717–1728. [Google Scholar] [CrossRef] [PubMed]
- Gerber, M. Qualitative methods to evaluate Mediterranean diet in adults. Public Health Nutr. 2006, 9, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Rumawas, M.E.; Dwyer, J.; Mckeown, N.M.; Meigs, J.B.; Rogers, G.; Jacques, P.F. The Development of the Mediterranean-Style Dietary Pattern Score and Its Application to the American Diet in the Framingham Offspring Cohort. J. Nutr. 2009, 139, 1150–1156. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.; Kalogeropoulos, N.; Pitsavos, C.; Rousinou, G.; Palliou, K.; Chrysohoou, C.; Stefanadis, C. Validation of the Med Diet Score via the determination of plasma fatty acids. Int. J. Food Sci. Nutr. 2009, 60, 168–180. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Benítez-Arciniega, A.; Soler, C.; Covas, M.I.; Baena-Díez, J.M.; Marrugat, J. Validity of two short screeners for diet quality in time-limited settings. Public Health Nutr. 2011, 15, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Estruch, R. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monteagudo, C.; Mariscal-Arcas, M.; Rivas, A.; Lorenzo-Tovar, M.L.; Tur, J.A.; Olea-Serrano, F. Proposal of a Mediterranean Diet Serving Score. PLoS ONE 2015, 10, e0128594. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Dinu, M.; Pagliali, G.; Marcucci, R.; Casini, A. Validation of literature-based adherence score to Mediterranean diet: The MEDI-LITE score. Int. J. Food. Sci. Nutr. 2017, 68, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Štefan, L.; Prosoli, R.; Juranko, D.; Čule, M.; Milinović, I.; Novak, D.; Sporiš, G. The Reliability of the Mediterranean Diet Quality Index (KIDMED) Questionnaire. Nutrients 2017, 9, 419. [Google Scholar] [CrossRef] [PubMed]
- Balkau, B.; Deanfield, J.E.; Després, J.P.; Bassand, J.P.; Fox, K.A.; Smith, S.C., Jr.; Barter, P.; Tan, C.E.; Van-Gaal, L.; Wittchen, H.U.; et al. International Day for the Evaluation of Abdominal Obesity (IDEA): A study of waist circumference, cardiovascular disease, and diabetes mellitus in 168,000 primary care patients in 63 countries. Circulation 2007, 116, 1942–1951. [Google Scholar] [CrossRef] [PubMed]
- Lacoppidan, S.A.; Kyro, C.; Loft, S.; Helnaes, A.; Christensen, J.; Hansen, C.P.; Olsen, A. Adherence to a healthy Nordic food index is associated with a lower risk of type-2 diabetes—The Danish diet, cancer and health cohort study. Nutrients 2015, 7, 8633–8644. [Google Scholar] [CrossRef] [PubMed]
- Levi, F.; Lucchini, F.; Negri, E.; La Vecchia, C. Trends in mortality from cardiovascular and cerebrovascular diseases in Europe and other areas of the world. Heart 2002, 88, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Patterson, R.; Pietinen, P. Evaluación del estado nutricional en individuos y poblaciones. In Nutrición y Salud Pública, 1st ed.; Gibney, G., Margetts, B., Kearney, J., Arab, L., Eds.; Acribia: Zaragoza, Spain, 2006; pp. 73–91. ISBN 8420010782. [Google Scholar]
- Mann, J. Elección de alimentos. In Nutrición y Salud Pública, 1st ed.; Gibney, G., Margetts, B., Kearney, J., Arab, L., Eds.; Acribia: Zaragoza, Spain, 2006; pp. 363–373. ISBN 8420010782. [Google Scholar]
- Costello, A.B.; Osborne, J.W. Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. PARE 2005, 10, 1–9. [Google Scholar]
- Declaration of Helsinki. Medical Research Involving Human Subjects. Available online: https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/ (accessed on 21 June 2017).
- Charney, P. Agua, electrolitos y equilibrio ácido-base. In Krause Dietoterapia, 13th ed.; Kathleen-Mahan, L., Escott-Stump, S., Raymond, L.J., Eds.; Elsevier: Barcelona, Spain, 2013; pp. 178–190. ISBN 978-84-8086-963-8. [Google Scholar]
- World Health Organization; Food and Agriculture Organization of the United Nations. Diet, Nutrition and the Prevention of Chronic Diseases; Report of a Joint WHO/FAO Expert Consultation; World Health Organization: Geneva, Switzerland, 2003; p. 54. ISBN 924120916. [Google Scholar]
- Global per Capita Fish Consumption Rises above 20 Kilograms a Year. Available online: http://www.fao.org/news/story/en/item/421871/icode/ (accessed on 14 January 2017).
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; De Jesus, J.M.; Houston-Miller, N.; Hubbard, V.S.; Lee, I.M.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E.; et al. 2013 AHA/ACC Guideline on Lifestyle Management to Reduce Cardiovascular Risk: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2960–2984. [Google Scholar] [CrossRef] [PubMed]
- Q&A on the Carcinogenicity of the Consumption of Red Meat and Processed Meat. Available online: http://www.who.int/features/qa/cancer-red-meat/en/ (accessed on 9 February 2017).
- United States Department of Health and Human Services; United States Department of Agriculture. Dietary Guidelines for Americans, 8th ed.; U.S. Department of Health and Human Services, U.S. Department of Agriculture: Whashington, DC, USA, 2015; pp. 13–36. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 8 March 2018).
- Bourges, H.; Casanueva, E.; Rosado, J. Apéndice 4. Distribución de sustratos energéticos. In Recomendaciones de Ingestión de Nutrimentos para la Población Mexicana. Bases Fisiológicas. Energía, Proteínas, Lípidos, Hidratos de Carbono y Fibra, 1st ed.; Bourges, H., Casanueva, E., Rosado, J., Eds.; Editorial Médica Panamericana: Mexico City, Mexico, 2008; Volume II, p. 191. ISBN 9789687988597. [Google Scholar]
- Jellinger, P.; Handelsman, Y.; Rosenblit, P.; Bloomgarden, Z.; Fonseca, V.A.; Garber, A.J.; Grunberger, G.; Guerin, C.K.; Bell, D.; Mechanick, J.I.; et al. American association of clinical endocrinologists and American college of endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocr. Pract. 2017, 23 (Suppl. S2), 1–87. [Google Scholar] [CrossRef] [PubMed]
- El Consumo de Azúcar en México y la Nueva Directriz de la OMS para su Reducción Global. Available online: https://www.insp.mx/epppo/blog/3609-consumo-azucar-mexico-nueva-directriz-oms.html (accessed on 27 December 2017).
- Sugars Intake for Adults and Children. Available online: http://apps.who.int/iris/bitstream/10665/149782/1/9789241549028_eng.pdf?ua=1 (accessed on 27 December 2017).
- World Health Organization. Recommendations and remarks. In Sodium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012; p. 18. ISBN 978-92-4-150483-6. [Google Scholar]
- Marfell-Jones, M.; Olds, T.; Stewart, A.; Carter, L. Estándares Internacionales para la Evaluación Antropométrica, Revisión 2008; Sociedad Internacional para el Avance de la Cineantropometría: Potchefstroom, South Africa, 2008. [Google Scholar]
- BMI Classification. Available online: http://apps.who.int/bmi/index.jsp?introPage=intro_3.html (accessed on 28 December 2017).
- Wong, J.E.; Parnell, W.R.; Howe, A.S.; Black, K.E.; Skidmore, P.M. Development and validation of a food-based diet quality index for New Zealand adolescents. BMC Public Health 2013, 13, 562. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.G.; Menezes, A.; Horovitz, L.; Jones, E.C.; Warren, R.F. A comparison of two time intervals for test-retest reliability of health status instruments. J. Clin. Epidemiol. 2003, 56, 730–735. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. Measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Echeverría, G.; Urquiaga, I.; Concha, M.J.; Dussaillant, C.; Villarroel, L.; Velasco, N.; Leighton, F.; Rigotti, A. Validación de cuestionario autoaplicable para un índice de alimentación mediterránea en Chile. Rev. Med. Chile 2016, 144, 1531–1543. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Martin, C.; Alonso-Domínguez, R.; Patino-Alonso, M.C.; Gómez-Marcos, M.A.; Maderuelo-Fernández, J.A.; Martin-Cantera, C.; García-Ortiz, L.; Recio-Rodríguez, J.I.; EVIDENT Group. The EVIDENT diet quality index is associated with cardiovascular risk and arterial stiffness in adults. BMC Public Health 2017, 1, 305. [Google Scholar] [CrossRef]
- Agnoli, C.; Krogh, V.; Grioni, S.; Sieri, S.; Palli, D.; Masala, G.; Sacerdote, C.; Vineis, P.; Tumino, R.; Frasca, G.; et al. A priori-defined dietary patterns are associated with reduced risk of stroke in a large Italian cohort. J. Nutr. 2011, 141, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; González, C.A.; Agudo, A.; Vilardell, M.; Berenguer, A.; Amiano, P.; Ardanaz, E.; Arriola, L.; Barricarte, A.; Basterretxea, M.; et al. Adherence to the Mediterranean diet and risk of coronary heart disease in the Spanish EPIC Cohort Study. Am. J. Epidemiol. 2009, 170, 1518–1529. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Fernández-Jarne, E.; Serrano-Martínez, M.; Wright, M.; Gómez-Gracia, E. Development of a short dietary intake questionnaire for the quantitative estimation of adherence to a cardioprotective Mediterranean diet. Eur. J. Clin. Nutr. 2004, 58, 1550–1552. [Google Scholar] [CrossRef] [PubMed]
- Kanauchi, M.; Kanauchi, K. Development of a Mediterranean diet score adapted to Japan and its relation to obesity risk. Food Nutr. Res. 2016, 60, 32172. [Google Scholar] [CrossRef] [PubMed]
- Fulkerson, J.A.; Lytle, L.; Story, M.; Moe, S.; Samuelson, A.; Weymiller, A. Development and validation of a screening instrument to assess the types and quality of foods served at home meals. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 10. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.E.; Burrows, T.L.; Rollo, M.E.; Boggess, M.M.; Watson, J.F.; Guest, M.; Duncanson, K.; Pezdirc, K.; Hutchesson, M.J. The Comparative Validity and Reproducibility of a Diet Quality Index for Adults: The Australian Recommended Food Score. Nutrients 2015, 7, 785–798. [Google Scholar] [CrossRef] [PubMed]
- Encuesta Nacional de Salud y Nutrición de Medio Camino 2016 (ENSANUT 2016). Informe Final de Resultados. Available online: http://promocion.salud.gob.mx/dgps/descargas1/doctos_2016/ensanut_mc_2016-310oct.pdf (accessed on 27 December 2017).
- Ramírez-Silva, I.; Rivera, J.A.; Ponce, X.; Hernández-Ávila, M. Fruit and vegetable intake in the Mexican population: Results from the Mexican National Health and Nutrition Survey 2006. Salud Publica Mexico 2009, 51, S574–S585. [Google Scholar]
- Rodríguez-Burelo, M.R.; Avalos-García, M.I.; López-Ramón, C. Consumo de bebidas de alto contenido calórico en México: Un reto para la salud pública. Salud Tabasco 2014, 20, 28–33. [Google Scholar]
- Martínez, H. Fluid intake in Mexican adults; a cross-sectional study. Nutr. Hosp. 2014, 29, 1179–1187. [Google Scholar] [PubMed]
- Espinosa-Montero, J.; Aguilar-Tamayo, M.F.; Monterrubio-Flores, E.A.; Barquera-Cervera, S. Conocimiento sobre el consumo de agua simple en adultos de nivel socioeconómico bajo de México. Salud Publica Mexico 2013, 55, S423–S430. [Google Scholar] [CrossRef]
- Cantoral, A.; Batis, C.; Basu, N. National estimation of seafood consumption in Mexico: Implications for exposure to methylmercury and polyunsaturated fatty acids. Chemosphere 2017, 174, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization; World Health Organization. Regional Status Report on Alcohol and Health in the Americas; Pan American Health Organization, World Health Organization: Washington, DC, USA, 2015; pp. 23–38. ISBN 978-92-75-11855-9. [Google Scholar]
- 40% de los Mexicanos Come Fuera de su Hogar al Menos una Vez a la Semana o Más a Menudo. Available online: http://www.nielsen.com/mx/es/press-room/2016/40-por-ciento-de-los-mexicanos-come-fuera-de-su-hogar-al-menos-una-vez-a-la-semana-o-mas-a-menudo.html (accessed on 4 June 2017).
- Newby, P.K.; Hu, F.B.; Rimm, E.B.; Smith-Warner, S.A.; Feskanich, D.; Sampson, L.; Willett, W.C. Reproducibility and validity of the Diet Quality Index Revised as assessed by use of a food-frequency questionnaire. Am. J. Clin. Nutr. 2003, 78, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Grafenauer, S.J.; Tapsell, L.C.; Beck, E.J.; Batterham, M.J. Development and validation of a Food Choices Score for use in weight-loss interventions. Br. J. Nutr. 2014, 111, 1862–1870. [Google Scholar] [CrossRef] [PubMed]
- Guenther, P.M.; Reedy, J.; Krebs-Smith, S.M.; Reeve, B.B. Evaluation of the Healthy Eating Index-2005. J. Am. Diet. Assoc. 2008, 108, 1854–1864. [Google Scholar] [CrossRef] [PubMed]
- Benítez-Arciniega, A.A.; Mendez, M.A.; Baena-Díez, J.M.; Rovira-Martori, N.A.; Soler, C.; Marrugat, J.; Covas, M.I.; Sanz, H.; Llopis, A.; Schröder, H. Concurrent and construct validity of Mediterranean diet scores as assessed by a FFQ. Public Health Nutr. 2011, 14, 2015–2021. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-López, M.C.; Muñoz-Hernández, J.A.; De Miera-Juárez, B.S. Impacto del consumo nocivo de alcohol en accidentes y enfermedades crónicas en México. Salud Publica Mexico 2013, 55, S282–S288. [Google Scholar] [CrossRef]


{kind=link}
| Food Group/Food | Evidence | Mini-ECCA Question | Reference |
|---|---|---|---|
| Water | An intake of 1.5 L of water per day is recommended, as it facilitates the proper functioning of various organic processes, such as temperature regulation and the elimination of metabolites. Water also plays a role in the processes of digestion, absorption, and excretion, and it serves as a means of distributing nutrients. | Do you drink at least 1.5 L of water per day? | [3,23] |
| Vegetables | At least 200 g of vegetables per day are recommended. They are a good source of vitamins, minerals, and fiber, and also have low energy density. As the WHO 1 recommends a 400 g combined intake of vegetables and fruits, fruits as a single group were assigned a minimum recommendation of half that amount (200 g). | Do you consume at least 200 g of cooked or raw vegetables per day? | [24] |
| Fish | In general, fish is lower in saturated fat and higher in polyunsaturated fats (Omega-3) than other sources of animal protein. The American Heart Association recommends two servings of fish per week, and that each serving should be 3.5 ounces (100 g). However, because fish intake levels in Mexico are low (6.7% of all proteins consumed) [25], it was decided that this food type should be consumed at least once per week (100 g) as a minimum goal. | Do you eat fresh or frozen fish (100 g) at least one day per week? | [26] |
| Types of meat | A high intake of red meat has been linked to the development of colorectal cancer. In addition, it contains higher levels of saturated fat than other meats. For this reason, the intake of red meat should be minimized in favor of other animal products, such as chicken and fish. | What type of meat do you consume most often? | [27,28] |
| Types of fat | The recommended intake of fatty acids is less than 7% of the total energy expenditure for saturated fat, 6–10% in the case of polyunsaturated fat, and the difference between total fat minus the latter two recommendations, in the case of monounsaturated fat. Adherence to these percentages is considered crucial for the prevention of cardiovascular diseases and their risk factors. | What type of fat do you most frequently consume during the week? | [3,29,30] |
| Sweetened beverages | Evidence exists to establish an association between the increase in the prevalence of overweightness, obesity, and diabetes in Mexico in the last 20 years, and the increase in the intake of kilocalories from sweetened beverages in the same period. Based on this evidence and current WHO recommendations regarding the intake of sugars (a maximum of 10% and preferably less than 5% of total energy intake), it is recommended that sweetened beverage intake should not exceed one drink (250 mL) per day. However, due to the high intake of sugar-sweetened beverages in the population, we agreed on an intermediate limit (four sugar-sweetened beverages per week). | Do you consume four or more sweetened beverages per week? | [31,32] |
| Fruits | A minimum intake of 200 g of fruit per day is recommended. Fruits are a good source of vitamins, minerals, antioxidants, and fiber. As the WHO recommends 400 g of vegetables and fruits combined, fruits as a single group were assigned a minimum recommendation of half that amount (200 g). | Do you consume at least 200 g of fruit per day? | [33] |
| Foods consumed outside the home | People who consume food outside the home have a higher risk of being overweight or obese, due to the amount of energy contained in such foods, and because the portions consumed outside the home tend to be larger than those consumed at home. | Do you eat foods not prepared at home three or more days per week? | [28,31,33] |
| Processed foods | Many processed foods contain high amounts of sodium. In this regard, the WHO recommends reducing sodium intake in adults to less than 2 g/day (5 g/day of salt). The WHO has also said that the intake of processed meat should be limited, because it has been linked to cancer. | Do you eat processed foods two or more days per week? | [27,31,32,33] |
| Desserts | Desserts contain high amounts of fats and sugars. In this regard, the WHO recommends reducing the intake of free sugars to less than 5% of the total daily calories, based on evidence for the development of various illnesses, including dental caries. The consensus of experts has determined that these foods should not be completely eliminated. Instead, healthy habits should be encouraged and the recommended intake frequency from this category should be no more than three days per week. | Do you consume sweets or commercial desserts two or more days per week? | [28,31,33] |
| Legumes | Intake from this food group is encouraged, owing to its fiber and protein content. Recommendations call for a minimum intake of three times per week. Due to the variability of the quantities cited in the various information sources (225–450 g), experts recommend a minimum quantity of 300 g per week. | Do you eat legumes at least three days per week (300 g per week)? | [3,11,12,28] |
| Cereals | It is recommended that 50% of cereals consumed be whole grain, due to their higher fiber content. Fiber is known to improve digestion, and to decrease blood glucose and cholesterol levels. | What cereals do you consume most often? | [28] |
| Variable | Frequency | Percentage |
|---|---|---|
| Sex | ||
| Male | 98 | 47.6 |
| Female | 108 | 52.4 |
| Physical activity | ||
| Sedentary lifestyle | 76 | 36.9 |
| Light | 62 | 30.1 |
| Moderate | 68 | 33.0 |
| Education | ||
| Postgraduate | 13 | 6.3 |
| Bachelor’s degree | 78 | 37.9 |
| High school | 69 | 33.5 |
| Middle school | 40 | 19.4 |
| Elementary school | 6 | 2.9 |
| Work area | ||
| Administrative | 118 | 57.3 |
| Operations | 88 | 42.7 |
| Variable | Men (n = 98) | Women (n = 108) | Total (n = 206) |
|---|---|---|---|
| Age | 40.5 ± 8.1 | 41.3 ± 7.1 | 40.9 ± 7.6 |
| Height (cm) | 171.8 ± 6.1 *** | 160.7 ± 5.9 | 166.0 ± 8.2 |
| Weight (kg) | 86.8 ± 14.7 *** | 71.3 ± 13.2 | 78.7 ± 15.9 |
| Body mass index (kg/cm2) | 29.4 ± 4.5 ** | 27.6 ± 5.0 | 28.4 ± 4.8 |
| BMI classification (WHO) | |||
| Normal | 11 (11.2) | 36 (33.3) | 47 (22.8) |
| Overweight | 50 (51.0) ** | 41 (38.0) | 91 (44.2) |
| Class I Obesity | 28 (28.6) | 22 (20.4) | 50 (24.3) |
| Class II Obesity | 7 (7.1) | 7 (6.5) | 14 (6.8) |
| Class III Obesity | 2 (2.0) | 2 (1.9) | 4 (1.9) |
| Body fat percentage (%) | 26.5 ± 5.6 | 37.0 ± 6.2 *** | 31.9 ± 7.9 |
| Body water percentage (%) | 52.5 ± 4.1 *** 1 | 46.5 ± 4.2 | 49.3 ± 5.1 2 |
| Percentage of visceral fat (%) | 11.1 ± 4.2 *** | 6.9 ± 2.9 | 8.9 ± 4.2 |
| Bone mass (kg) | 3.2 ± 0.4 *** | 2.3 ± 0.3 3 | 2.7 ± 0.5 4 |
| Muscle mass (kg) | 60.1 ± 7.4 *** 5 | 42.1 ± 5.1 3 | 50.7 ± 11.0 6 |
| Waist circumference (cm) | 97.3 ± 11.6 *** | 84.8 ± 11.2 | 90.7 ± 13.0 |
| Hip circumference (cm) | 102.6 ± 7.4 5 | 104.9 ± 9.9 | 103.8 ± 8.9 4 |
| Classification According to the Scores Obtained | Test | McNemar Test (p-Value) | Weighted *** (95% CI) | |||||
|---|---|---|---|---|---|---|---|---|
| Very Low (1–3 points) | Low (4–6 points) | Good (7–9 points) | Very Good (10–12 points) | Total *** | ||||
| Retest | Very low | 13 (52.0) | 9 (9.8) | 0 (0.0) | 0 (0.0) | 22 (7.2) | 0.091 | 0.545 (0.484, 0.606) |
| Low | 10 (40.0) | 59 (64.1) | 15 (19.5) | 0 (0.0) | 84 (27.6) | |||
| Good | 2 (8.0) | 23 (25.0) | 49 (63.6) | 4 (33.3) | 78 (25.7) | |||
| Very good | 0 (0.0) | 1 (1.1) | 13 (16.9) | 8 (66.7) | 22 (7.2) | |||
| Total | 25 (8.2) | 92 (30.3) | 77 (25.3) | 12 (3.9) | 206 (100.0) | |||
| Variable | Retest | Test | McNemar Test (p-Value) 1 | Kappa *** (95% CI) | Test vs. Retest Score Differences | ||||
|---|---|---|---|---|---|---|---|---|---|
| Yes | No | Total | Decreased | Remained Unchanged | Increased | ||||
| 1. Do you drink at least 1.5 L of water per day? | Yes | 104 (89.7) | 24 (26.7) | 128 (62.1) | 0.065 | 0.639 (0.533, 0.744) | 12 (5.8) | 170 (82.5) | 24 (11.7) |
| No | 12 (10.3) | 66 (73.3) | 78 (37.9) | ||||||
| Total | 116 (53.3) | 90 (43.6) | 206 (100) | ||||||
| 2. Do you consume at least 200 g of cooked or raw vegetables per day? | Yes | 69 (78.4) | 28 (23.7) | 97 (47.1) | 0.243 | 0.540 (0.424, 0.655) | 19 (9.2) | 159 (77.2) | 28 (13.6) |
| No | 19 (21.6) | 90 (76.3) | 109 (52.9) | ||||||
| Total | 88 (42.7) | 118 (57.3) | 206 (100) | ||||||
| 3. Do you eat fresh or frozen fish (100 g) at least one day per week? | Yes | 87 (88.8) | 33 (30.6) | 120 (58.3) | <0.001 | 0.576 (0.468, 0.683) | 11 (5.3) | 162 (78.6) | 33 (16.0) |
| No | 11 (11.2) | 75 (69.4) | 86 (41.7) | ||||||
| Total | 98 (47.6) | 108 (52.4) | 206 (100) | ||||||
| 4. Do you consume four or more sweetened beverages per week? | Yes | 143 (87.7) | 7 (16.3) | 150 (72.8) | 0.019 | 0.643 (0.521, 0.764) | 7 (3.4) | 179 (86.9) | 20 (9.7) |
| No | 20 (12.3) | 36 (83.7) | 56 (27.2) | ||||||
| Total | 163 (79.1) | 43 (20.9) | 206 (100) | ||||||
| 5. Do you consume at least 200 g of fruit per day? | Yes | 107 (79.3) | 19 (26.8) | 126 (61.2) | 0.243 | 0.510 (0.388, 0.631) | 28 (13.6) | 159 (77.2) | 19 (9.2) |
| No | 28 (20.7) | 52 (73.2) | 80 (38.8) | ||||||
| Total | 135 (65.5) | 71 (34.5) | 206 (100) | ||||||
| 7. Do you eat foods not prepared at home three or more days per week? | Yes | 100 (87.0) | 29 (31.9) | 129 (62.6) | 0.049 | 0.560 (0.446, 0.674) | 29 (14.1) | 162 (78.6) | 15 (7.3) |
| No | 15 (13.0) | 62 (68.1) | 77 (37.4) | ||||||
| Total | 115 (55.8) | 91 (44.2) | 206 (100) | ||||||
| 9. Do you eat processed foods two or more days per week? | Yes | 84 (81.6) | 31 (30.1) | 115 (55.8) | 0.119 | 0.515 (0.399, 0.631) | 31 (15.0) | 156 (75.7) | 19 (9.2) |
| No | 19 (18.4) | 72 (69.9) | 91 (44.2) | ||||||
| Total | 103 (50.0) | 103 (50.0) | 206 (100) | ||||||
| 10. Do you consume sweets or commercial desserts two or more days per week? | Yes | 107 (79.3) | 23 (32.4) | 130 (63.1) | 0.576 | 0.461 (0.335, 0.586) | 23 (11.2) | 155 (75.2) | 28 (13.6) |
| No | 28 (20.7) | 48 (67.6) | 76 (36.9) | ||||||
| Total | 135 (65.5) | 71 (34.5) | 206 (100) | ||||||
| 11. Do you eat legumes at least three days per week (300 g per week)? | Yes | 144 (93.5) | 24 (46.2) | 168 (81.6) | 0.024 | 0.520 (0.381, 0.659) | 10 (4.9) | 172 (83.5) | 24 (1.7) |
| No | 10 (6.5) | 28 (53.8) | 38 (18.4) | ||||||
| Total | 154 (74.8) | 52 (25.2) | 206 (100.0) | ||||||
| Variable | Retest | Test | McNemar Test (p-Value) | Weighted Kappa *** (95% CI) | Test vs. Retest Score Differences | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Whole Grain | Refined | Do Not Know | Total | Decreased | Remained Unchanged | Increased | ||||
| 12. What cereals do you consume most often? | Whole grain | 148 (90.2) | 20 (58.8) | 6 (75.0) | 174 (84.5) | 0.435 | 0.271 (0.218, 0.324) | 16 (7.8) | 164 (789.6) | 26 (12.6) |
| Refined | 12 (7.3) | 12 (35.3) | 1 (12.5) | 25 (12.1) | ||||||
| Do not know | 4 (2.4) | 2 (5.9) | 1 (12.5) | 7 (3.4) | ||||||
| Total | 164 (79.6) | 34 (16.5) | 8 (3.8) | 206 (100.0) | ||||||
| Variable | Retest | Test | McNemar Test (p-Value) 1 | Weighted Kappa *** (95% CI) | Test vs. Retest Score Differences | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| A | B | C | D | Total | Decreased | Remained Unchanged | Increased | ||||
| 6. What type of fat do you most frequently consume during the week? | A (Polyunsaturated) | 69 (76.7) | 14 (14.9) | 6 (42.9) | 3 (37.5) | 92 (44.7) | 0.204 | 0.456 (0.397, 0.515) | 15 (7.3) | 171 (83.0) | 20 (9.7) |
| B (Monounsaturated) | 14 (15.6) | 79 (84.0) | 1 (7.1) | 5 (62.5) | 99 (48.1) | ||||||
| C (Saturated) | 2 (2.2) | 1 (1.1) | 6 (42.9) | 0 (0.0) | 9 (4.4) | ||||||
| D (Do not know) | 5 (5.6) | 0 (0.0) | 1 (7.1) | 0 (0.0) | 6 (2.9) | ||||||
| Total | 90 (43.7) | 94 (45.6) | 14 (6.8) | 8 (3.9) | 206 (100.0) | ||||||
| 8. What type of meat do you consume most often? | A (Chicken) | 75 (81.5) | 22 (24.2) | 2 (25.0) | 6 (40.0) | 105 (51.0) | 0.013 | 0.460 (0.399, 0.521) | 14 (6.8) | 164 (79.6) | 28 (13.6) |
| B (Beef) | 8 (8.7) | 69 (75.8) | 0 (0.0) | 6 (40.0) | 83 (40.3) | ||||||
| C (Fish) | 3 (3.3) | 0 (0.0) | 6 (75.0) | 0 (0.0) | 9 (4.4) | ||||||
| D (Do not know) | 6 (6.5) | 0 (0.0) | 0 (0.0) | 3 (20.0) | 9 (4.4) | ||||||
| Total | 92 (44.7) | 91 (44.2) | 8 (3.9) | 15 (7.2) | 206 (100) | ||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernal-Orozco, M.F.; Badillo-Camacho, N.; Macedo-Ojeda, G.; González-Gómez, M.; Orozco-Gutiérrez, J.F.; Prado-Arriaga, R.J.; Márquez-Sandoval, F.; Altamirano-Martínez, M.B.; Vizmanos, B. Design and Reproducibility of a Mini-Survey to Evaluate the Quality of Food Intake (Mini-ECCA) in a Mexican Population. Nutrients 2018, 10, 524. https://doi.org/10.3390/nu10040524
Bernal-Orozco MF, Badillo-Camacho N, Macedo-Ojeda G, González-Gómez M, Orozco-Gutiérrez JF, Prado-Arriaga RJ, Márquez-Sandoval F, Altamirano-Martínez MB, Vizmanos B. Design and Reproducibility of a Mini-Survey to Evaluate the Quality of Food Intake (Mini-ECCA) in a Mexican Population. Nutrients. 2018; 10(4):524. https://doi.org/10.3390/nu10040524
Chicago/Turabian StyleBernal-Orozco, María Fernanda, Nayeli Badillo-Camacho, Gabriela Macedo-Ojeda, Montserrat González-Gómez, Jaime Fernando Orozco-Gutiérrez, Ruth Jackelyne Prado-Arriaga, Fabiola Márquez-Sandoval, Martha Betzaida Altamirano-Martínez, and Barbara Vizmanos. 2018. "Design and Reproducibility of a Mini-Survey to Evaluate the Quality of Food Intake (Mini-ECCA) in a Mexican Population" Nutrients 10, no. 4: 524. https://doi.org/10.3390/nu10040524