Validation of a Rapid Method to Assess Habitual Beverage Intake Patterns

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Subjects and Design
2.2. The Healthy Beverage Index (HBI)
2.3. The HBI-Q
2.4. HBI via Dietary Recalls
2.5. Statistical Analysis
3. Results
3.1. Demographics
3.2. Comparison of Estimated Energy vs. Reported Energy HBI-Q Methods
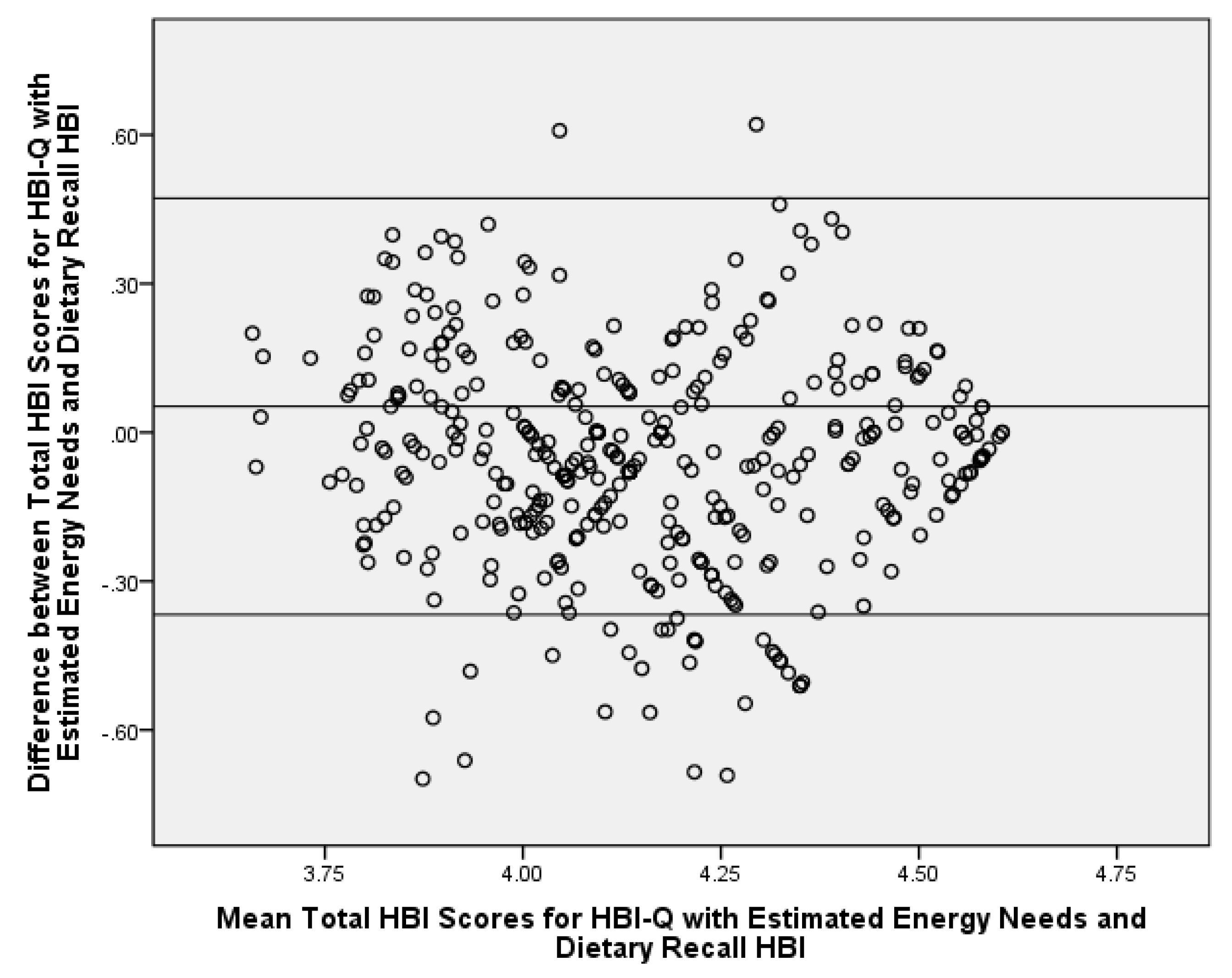
3.3. Comparison of HBI Scores via the HBI-Q and Dietary Recalls
4. Discussion
5. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among adults in the United States: Cross-sectional study using data from NHANES 2005–2010. BMC Public Health 2013, 13, 1068. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; D’Anci, K.E.; Rosenberg, I.H. Water, hydration, and health. Nutr. Rev. 2010, 68, 439–458. [Google Scholar] [CrossRef] [PubMed]
- Daniels, M.C.; Popkin, B.M. Impact of water intake on energy intake and weight status: A systematic review. Nutr. Rev. 2010, 68, 505–521. [Google Scholar] [CrossRef] [PubMed]
- Muckelbauer, R.; Sarganas, G.; Gruneis, A.; Muller-Nordhorn, J. Association between water consumption and body weight outcomes: A systematic review. Am. J. Clin. Nutr. 2013, 98, 282–299. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Schulze, M.B.; Hu, F.B. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am. J. Clin. Nutr. 2006, 84, 274–288. [Google Scholar] [PubMed]
- Vartanian, L.; Schwartz, M.; Brownell, K. Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. Am. J. Public Health 2007, 97, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Brown, I.J.; Stamler, J.; Van Horn, L.; Robertson, C.E.; Chan, Q.; Dyer, A.R.; Huang, C.C.; Rodriguez, B.L.; Zhao, L.; Daviglus, M.L.; et al. Sugar-sweetened beverage, sugar intake of individuals, and their blood pressure: International study of macro/micronutrients and blood pressure. Hypertension 2011, 57, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Caballero, B.; Mitchell, D.C.; Loria, C.; Lin, P.H.; Champagne, C.M.; Elmer, P.J.; Ard, J.D.; Batch, B.C.; Anderson, C.A.; et al. Reducing consumption of sugar-sweetened beverages is associated with reduced blood pressure: A prospective study among United States adults. Circulation 2010, 121, 2398–2406. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Resolved: There is sufficient scientific evidence that decreasing sugar-sweetened beverage consumption will reduce the prevalence of obesity and obesity-related diseases. Obes. Rev. 2013, 14, 606–619. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.K.; Appel, L.J.; Brands, M.; Howard, B.V.; Lefevre, M.; Lustig, R.H.; Sacks, F.; Steffen, L.M.; Wylie-Rosett, J. Dietary sugars intake and cardiovascular health: A scientific statement from the American Heart Association. Circulation 2009, 120, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Dennis, E.A.; Dengo, A.L.; Comber, D.L.; Flack, K.D.; Savla, J.; Davy, K.P.; Davy, B.M. Water consumption increases weight loss during a hypocaloric diet intervention in middle-aged and older adults. Obesity 2009, 18, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Armstrong, L.E.; Bray, G.M.; Caballero, B.; Frei, B.; Willett, W.C. A new proposed guidance system for beverage consumption in the United States. Am. J. Clin. Nutr. 2006, 83, 529–542. [Google Scholar] [PubMed]
- Kosova, E.C.; Auinger, P.; Bremer, A.A. The relationships between sugar-sweetened beverage intake and cardiometabolic markers in young children. J. Acad. Nutr. Diet. 2013, 113, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Rangan, A.; Olsen, N.J.; Bo Andersen, L.; Wedderkopp, N.; Kristensen, P.; Grontved, A.; Ried-Larsen, M.; Lempert, S.M.; Allman-Farinelli, M.; et al. Sugar-sweetened beverages consumption in relation to changes in body fatness over 6 and 12 years among 9-year-old children: The European Youth Heart Study. Eur. J. Clin. Nutr. 2014, 68, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, K.A.; Shikany, J.M.; Keating, K.D.; Allison, D.B. Will reducing sugar-sweetened beverage consumption reduce obesity? Evidence supporting conjecture is strong, but evidence when testing effect is weak. Obes. Rev. 2013, 14, 620–633. [Google Scholar] [CrossRef] [PubMed]
- Sanigorski, A.M.; Bell, A.C.; Swinburn, B.A. Association of key foods and beverages with obesity in Australian schoolchildren. Public Health Nutr. 2007, 10, 152–157. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th Edition. 2015. Available online: http://health.gov/dietaryguidelines/2015/guidelines (accessed on 29 November 2017).
- Myers, E.F.; Khoo, C.S.; Murphy, W.; Steiber, A.; Agarwal, S. A critical assessment of research needs identified by the dietary guidelines committees from 1980 to 2010. J. Acad. Nutr. Diet. 2013, 113, 957–971. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, V.; Davy, B.; Duffey, K. Is beverage consumption related to specific dietary pattern intakes? Curr. Nutr. Rep. 2015, 4, 72–81. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Epidemiology and Genomics Research Program: National Cancer Institute. Developing the Healthy Eating Index. Available online: https://epi.grants.cancer.gov/hei/developing.html (accessed on 29 November 2017).
- Bratusch-Marrain, P.R.; DeFronzo, R.A. Impairment of insulin-mediated glucose metabolism by hyperosmolality in man. Diabetes 1983, 32, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J. Hydration, morbidity, and mortality in vulnerable populations. Nutr. Rev. 2012, 70 (Suppl. 2), S152–S155. [Google Scholar] [CrossRef] [PubMed]
- Duffey, K.J.; Davy, B.M. The Healthy Beverage Index Is Associated with Reduced Cardiometabolic Risk in US Adults: A Preliminary Analysis. J. Acad. Nutr. Diet. 2015, 115, 1682–1689.e1682. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, V.E.; Comber, D.L.; Estabrooks, P.A.; Savla, J.; Davy, B.M. The beverage intake questionnaire: Determining initial validity and reliability. J. Am. Diet. Assoc. 2010, 110, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, V.E.; Comber, D.L.; Ferguson, K.E.; Estabrooks, P.A.; Savla, J.; Dietrich, A.M.; Serrano, E.; Davy, B.M. A rapid beverage intake questionnaire can detect changes in beverage intake. Eat. Behav. 2013, 14, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, V.E.; Savla, J.; Comber, D.L.; Flack, K.D.; Estabrooks, P.A.; Nsiah-Kumi, P.A.; Ortmeier, S.; Davy, B.M. Development of a brief questionnaire to assess habitual beverage intake (BEVQ-15): Sugar-sweetened beverages and total beverage energy intake. J. Acad. Nutr. Diet. 2012, 112, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Zoellner, J.; Chen, Y.; Davy, B.; You, W.; Hedrick, V.; Corsi, T.; Estabrooks, P. Talking Health, a pragmatic randomized-controlled health literacy trial targeting sugar-sweetened beverage consumption among adults: Rationale, design & methods. Contemp. Clin. Trials 2014, 37, 43–57. [Google Scholar] [PubMed]
- Zoellner, J.M.; Hedrick, V.E.; You, W.; Chen, Y.; Davy, B.M.; Porter, K.J.; Bailey, A.; Lane, H.; Alexander, R.; Estabrooks, P.A. Effects of a behavioral and health literacy intervention to reduce sugar-sweetened beverages: A randomized-controlled trial. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Estabrooks, P.; You, W.; Hedrick, V.; Reinholt, M.; Dohm, E.; Zoellner, J. A pragmatic examination of active and passive recruitment methods to improve the reach of community lifestyle programs: The Talking Health Trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 7. [Google Scholar] [CrossRef] [PubMed]
- Godin, G.; Shephard, R. A simple method to assess exercise behavior in the community. Can. J. Appl. Sport Sci. 1985, 10, 141–146. [Google Scholar] [PubMed]
- Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate; The National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- Mifflin, M.D.; St Jeor, S.T.; Hill, L.A.; Scott, B.J.; Daugherty, S.A.; Koh, Y.O. A new predictive equation for resting energy expenditure in healthy individuals. Am. J. Clin. Nutr. 1990, 51, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids; The National Academies Press: Washington, DC, USA, 2002. [Google Scholar]
- Stote, K.S.; Radecki, S.V.; Moshfegh, A.J.; Ingwersen, L.A.; Baer, D.J. The number of 24 h dietary recalls using the US Department of Agriculture’s automated multiple-pass method required to estimate nutrient intake in overweight and obese adults. Public Health Nutr. 2011, 14, 1736–1742. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Subar, A.F. Dietary Assessment Methodology. In Nutrition in the Prevention and Treatment of Disease, 2nd ed.; Coulston, A., Boushey, C., Eds.; Elsevier, Inc.: Oxford, UK, 2008; pp. 3–39. [Google Scholar]
- Kuhnle, G.G. Nutritional biomarkers for objective dietary assessment. J. Sci. Food Agric. 2012, 92, 1145–1149. [Google Scholar] [CrossRef] [PubMed]
- Myles, P.S.; Cui, J.I. Using the Bland–Altman method to measure agreement with repeated measures. BJA Br. J. Anaesth. 2007, 99, 309–311. [Google Scholar] [CrossRef] [PubMed]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Bland, J.M. Measurement in Medicine: The Analysis of Method Comparison Studies. J. R. Stat. Soc. Ser. D (Statistician) 1983, 32, 307–317. [Google Scholar] [CrossRef]
- Willett, W.C. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]


{kind=link}
| Healthy Beverage Index Components | Description | Points |
|---|---|---|
| Water | Water comprises ≥20% of fluid requirements | 15 |
| No water consumption | 0 | |
| Water is >0% but <20% of fluid requirements | Proportional score between 0 and 15 | |
| Coffee and Tea | Unsweetened coffee and tea comprise 0–40% of fluid requirements | 5 |
| Low-fat Milk | ≤1.5% fat milk comprises 0–16% of fluid requirements | 5 |
| Diet Drinks | Artificially sweetened beverages comprise 0–16% of fluid requirements | 5 |
| 100% Fruit Juice | 100% fruit juice comprises 0–8% of fluid requirements | 5 |
| Alcohol | 0–1 drinks for women, 0–2 drinks for men | 5 |
| Full-fat Milk | 0% of fluid requirements come from 2% fat or full-fat milk | 5 |
| Sugar-sweetened Beverages | Sugar-sweetened beverages are 0–8% of fluid requirements | 15 |
| Total Beverage Energy | Energy from beverages ≤10% of total energy | 20 |
| Energy from beverages ≥15% of total energy | 0 | |
| Energy from beverages is >10% but <15% of total energy | Proportional score between 0 and 20 | |
| Met Fluid Requirements b | Amount of beverages (mL) consumed was ≥ fluid requirements | 20 |
| Amount of beverages (mL) consumed was < fluid requirements | Proportional score between 0 and 20 |
| Moderate to Vigorous Physical Activity Category b | Strengthening Exercise Category c | Corresponding Activity Factor d |
|---|---|---|
| Sedentary | ||
| 1 | 1 | 1.0 |
| 1 | 2 | 1.0 |
| 1 | 3 | 1.0 |
| Does not meet recommendations, but not sedentary | ||
| 2 | 1 | 1.1 |
| 2 | 2 | 1.1 |
| 2 | 3 | 1.1 |
| Meets physical activity recommendations but not strengthening exercise recommendations | ||
| 3 | 1 | 1.3 |
| 3 | 2 | 1.3 |
| Meets recommendations for all categories | ||
| 3 | 3 | 1.5 |
| Healthy Beverage Index Components (Possible Score) | Comparison of HBI-Q Scores Using Estimated Energy Needs vs. Reported Energy Intake | ||
|---|---|---|---|
| HBI-Q Scores with Estimated Energy Needs a | HBI-Q Scores with Reported Energy Intake a | Mean Difference b | |
| Water (0–15) | 12.2 (4.7) | 12.1 (4.8) | 0.1 (0.1) |
| Coffee & Tea (0–5) | 4.7 (1.1) | 4.8 (1.0) | −0.1 (0.04) |
| Low Fat Milk (Skim or 1%) (0–5) | 4.5 (1.6) | 4.4 (1.6) | 0.1 (0.05) |
| Diet Drinks (0–5) | 4.2 (1.8) | 4.2 (1.9) | 0.04 (0.05) |
| 100% Fruit Juice (0–5) | 4.3 (1.8) | 4.2 (1.8) | 0.04 (0.1) |
| Alcohol (0–5) | 4.6 (1.4) | 4.6 (1.4) | 0.0 (0.0) |
| Whole Fat Milk (≥2%) (0–5) | 3.3 (2.4) | 3.3 (2.4) | 0.0 (0.0) |
| Sugar-Sweetened Beverages (0–15) | 2.6 (5.7) | 2.8 (5.9) | −0.2 (0.1) |
| Total Beverage Energy (0–20) | 5.2 (8.2) | 5.1 (8.3) | 0.2 (0.2) |
| Met Total Fluid Requirement (0–20) | 18.1 (3.4) | 17.6 (3.8) | 0.5 (0.1) *** |
| Total HBI Score (0–100) | 63.7 (15.8) | 63.2 (16.4) | 0.5 (0.2) |
| Healthy Beverage Index Components (Possible Score) | Comparison of HBI Scores Derived from the HBI-Q vs. Dietary Recalls | ||
|---|---|---|---|
| HBI-Q Scores with Estimated Energy Needs a | Dietary Recall HBI Scores a | Mean Difference b | |
| Water (0–15) | 12.2 (4.7) | 11.9 (5.4) | 0.4 (0.2) |
| Coffee & Tea (0–5) | 4.7 (1.1) | 4.7 (1.2) | 0.04 (0.1) |
| Low Fat Milk (Skim or 1%) (0–5) | 4.5 (1.6) | 4.7 (1.1) | –0.3 (0.1) *** |
| Diet Drinks (0–5) | 4.2 (1.8) | 4.4 (1.6) | –0.2 (0.1) |
| 100% Fruit Juice (0–5) | 4.3 (1.8) | 4.8 (1.1) | −0.5 (0.1) *** |
| Alcohol (0–5) | 4.6 (1.4) | 4.7 (1.2) | −0.1 (0.1) |
| Whole Fat Milk (≥2%) (0–5) | 3.3 (2.4) | 4.5 (1.5) | −1.2 (0.1) *** |
| Sugar-Sweetened Beverages (0–15) | 2.6 (5.7) | 3.2 (6.2) | −0.6 (0.3) |
| Total Beverage Energy (0–20) | 5.2 (8.2) | 7.3 (8.9) | −2.1 (0.4) *** |
| Met Total Fluid Requirement (0–20) | 18.1 (3.4) | 17.1 (4.1) | 0.9 (0.2) *** |
| Total HBI Score (0–100) | 63.7 (15.8) | 67.3 (16.8) | 3.6 (0.7) *** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hedrick, V.E.; Myers, E.A.; Zoellner, J.M.; Duffey, K.J.; Davy, B.M. Validation of a Rapid Method to Assess Habitual Beverage Intake Patterns. Nutrients 2018, 10, 83. https://doi.org/10.3390/nu10010083
Hedrick VE, Myers EA, Zoellner JM, Duffey KJ, Davy BM. Validation of a Rapid Method to Assess Habitual Beverage Intake Patterns. Nutrients. 2018; 10(1):83. https://doi.org/10.3390/nu10010083
Chicago/Turabian StyleHedrick, Valisa E., Emily A. Myers, Jamie M. Zoellner, Kiyah J. Duffey, and Brenda M. Davy. 2018. "Validation of a Rapid Method to Assess Habitual Beverage Intake Patterns" Nutrients 10, no. 1: 83. https://doi.org/10.3390/nu10010083
APA StyleHedrick, V. E., Myers, E. A., Zoellner, J. M., Duffey, K. J., & Davy, B. M. (2018). Validation of a Rapid Method to Assess Habitual Beverage Intake Patterns. Nutrients, 10(1), 83. https://doi.org/10.3390/nu10010083