
Mother-to-Child Transmission of HTLV-1 Epidemiological Aspects, Mechanisms and Determinants of Mother-to-Child Transmission

Abstract
:
{kind=link}
{kind=link}
1. Introduction
2. Evidence of HTLV-1 MTCT during Breastfeeding
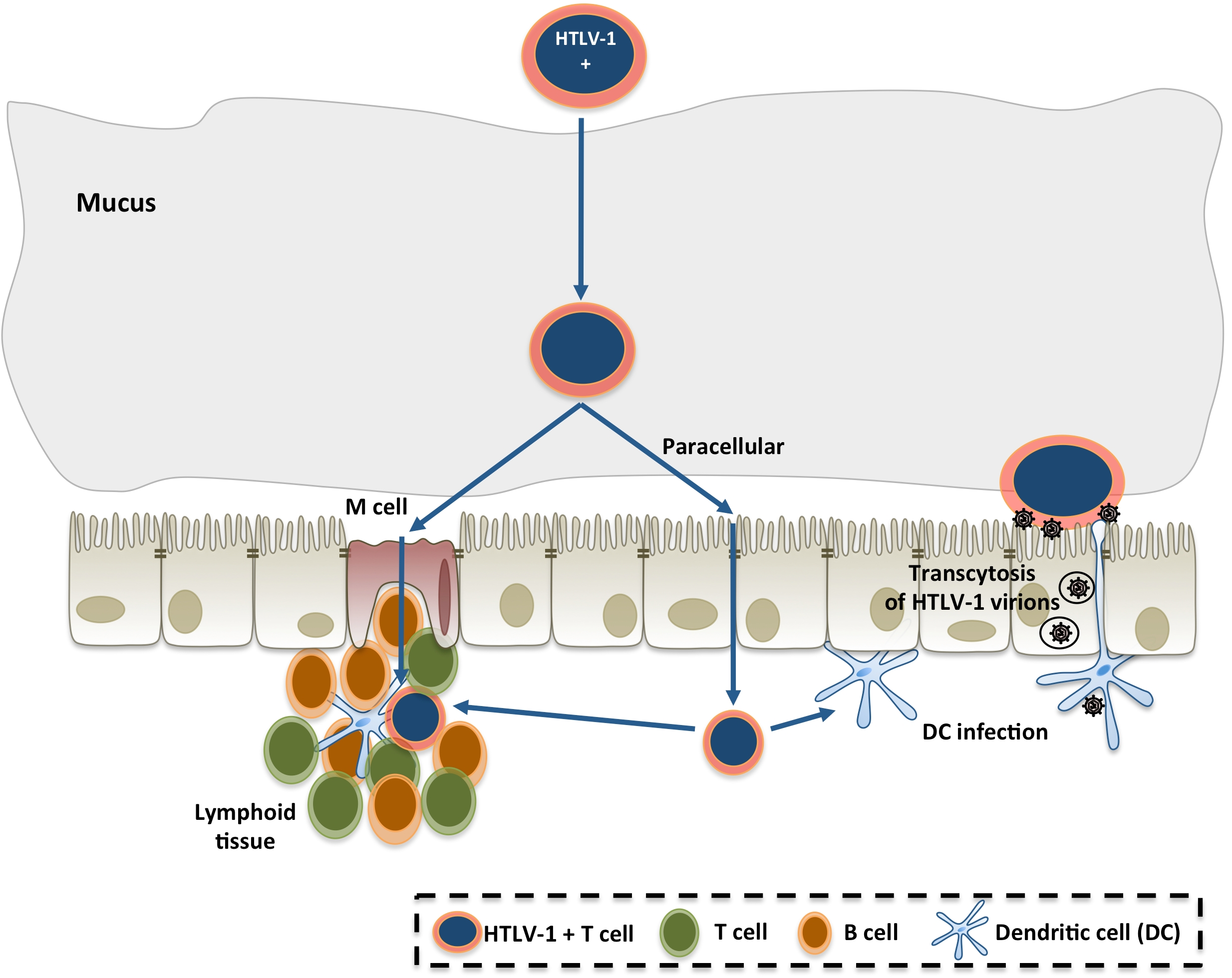
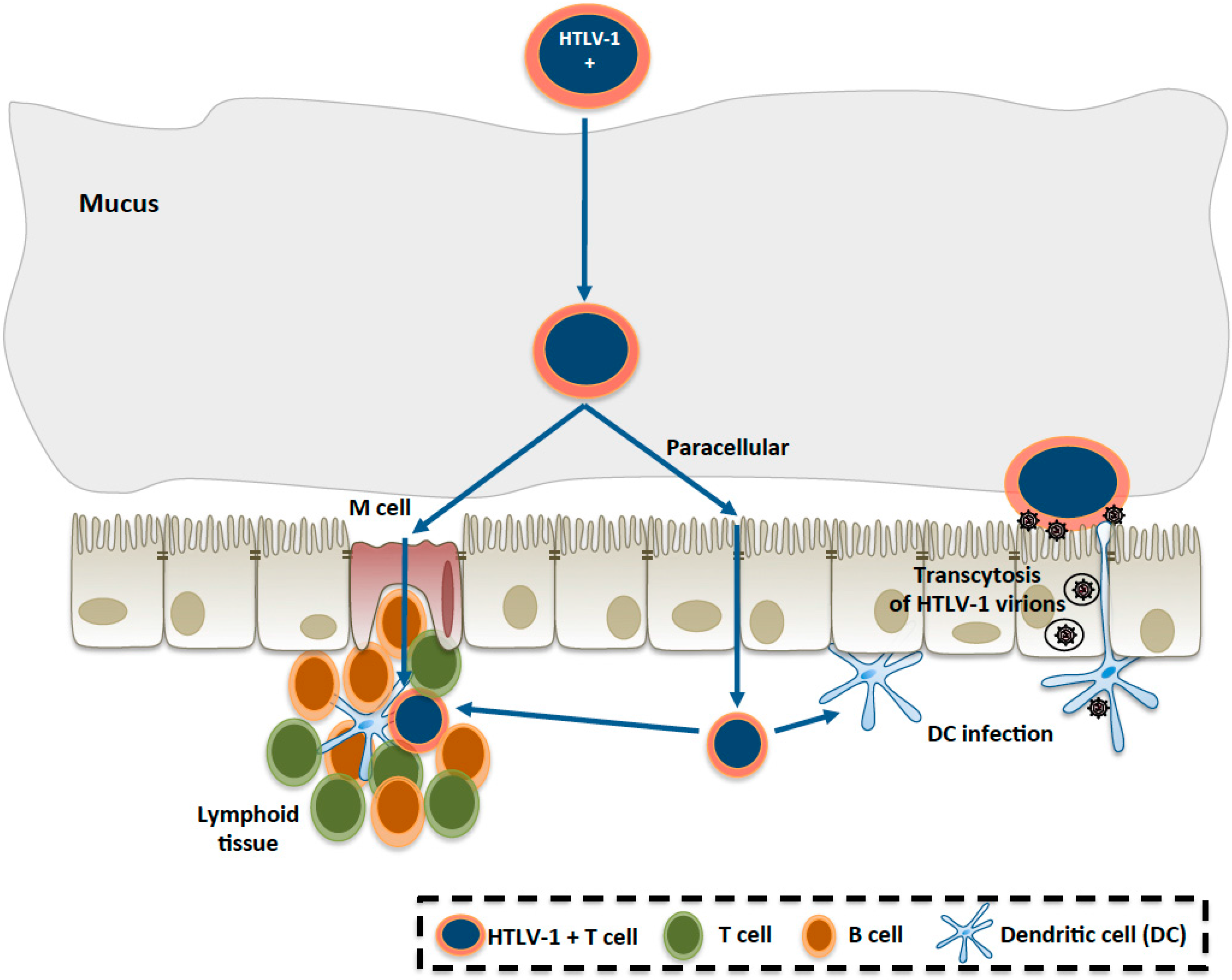
3. The Mechanisms of HTLV-1 MTCT
4. Determinants of HTLV-1 MTCT
5. Ongoing Research on HTLV-1 MTCT and Perspectives
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Gessain, A.; Cassar, O. Epidemiological aspects and world distribution of HTLV-1 Infection. Front. Microbiol. 2012, 3, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.H.; Edwards, A.J.; Cruickshank, J.K.; Rudge, P.; Dalgleish, A.G. In vivo cellular tropism of human T-cell leukemia virus type 1. J. Virol. 1990, 64, 5682–5687. [Google Scholar] [PubMed]
- Nagai, M.; Brennan, M.B.; Sakai, J.A.; Mora, C.A.; Jacobson, S. CD8+ T cells are an in vivo reservoir for human T-cell lymphotropic virus type I. Blood 2001, 98, 1858–1861. [Google Scholar] [CrossRef] [PubMed]
- Koyanagi, Y.; Yoshida, T.; Suzuki, M.; Uma, A.; Ananthasubramaniam, L.; Ramajayam, S.; Yamamoto, N. Dual infection of HIV-1 and HTLV-I in south India: A study on a patient with AIDS-related complex. Microbiol. Immunol. 1993, 37, 983–986. [Google Scholar] [CrossRef] [PubMed]
- Afonso, P.V.; Ozden, S.; Cumont, M.C.; Seilhean, D.; Cartier, L.; Rezaie, P.; Mason, S.; Lambert, S.; Huerre, M.; Gessain, A.; et al. Alteration of blood-brain barrier integrity by retroviral infection. PLoS Pathog. 2008, 4, e1000205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carneiro-Proietti, A.B.; Amaranto-Damasio, M.S.; Leal-Horiguchi, C.F.; Bastos, R.H.; Seabra-Freitas, G.; Borowiak, D.R.; Ribeiro, M.A.; Proietti, F.A.; Ferreira, A.S.; Martins, M.L. Mother-to-Child transmission of human T-Cell lymphotropic viruses-1/2: What we know, and what are the gaps in understanding and preventing this route of infection. J. Pediatr. Infect. Dis. Soc. 2014, 3 (Suppl. 1), S24–S29. [Google Scholar] [CrossRef] [PubMed]
- Murphy, E.L.; Hanchard, B.; Figueroa, J.P.; Gibbs, W.N.; Lofters, W.S.; Campbell, M.; Goedert, J.J.; Blattner, W.A. Modelling the risk of adult T-cell leukemia/lymphoma in persons infected with human T-lymphotropic virus type I. Int. J. Cancer 1989, 43, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Nakano, S.; Saito, K.; Shimamoto, I.; Ichijo, M.; Toyama, T.; Hinuma, Y. Transmission of adult T-cell leukemia retrovirus (HTLV-I) from mother to child: Comparison of bottle- with breast-fed babies. Jpn. J. Cancer Res. 1987, 78, 322–324. [Google Scholar] [PubMed]
- Hino, S.; Sugiyama, H.; Doi, H.; Ishimaru, T.; Yamabe, T.; Tsuji, Y.; Miyamoto, T. Breaking the cycle of HTLV-I transmission via carrier mothers’ milk. Lancet 1987, 2, 158–159. [Google Scholar] [CrossRef]
- Hino, S.; Katamine, S.; Miyata, H.; Tsuji, Y.; Yamabe, T.; Miyamoto, T. Primary prevention of HTLV-I in Japan. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1996, 13 (Suppl. 1), S199–S203. [Google Scholar] [CrossRef] [PubMed]
- Wiktor, S.Z.; Pate, E.J.; Rosenberg, P.S.; Barnett, M.; Palmer, P.; Medeiros, D.; Maloney, E.M.; Blattner, W.A. Mother-to-child transmission of human T-cell lymphotropic virus type I associated with prolonged breast-feeding. J. Hum. Virol. 1997, 1, 37–44. [Google Scholar] [PubMed]
- Takahashi, K.; Takezaki, T.; Oki, T.; Kawakami, K.; Yashiki, S.; Fujiyoshi, T.; Usuku, K.; Mueller, N.; Osame, M.; Miyata, K.; et al. Inhibitory effect of maternal antibody on mother-to-child transmission of human T-lymphotropic virus type I. The Mother-to-Child Transmission Study Group. Int. J. Cancer 1991, 49, 673–677. [Google Scholar] [CrossRef] [PubMed]
- Hino, S. Establishment of the milk-borne transmission as a key factor for the peculiar endemicity of human T-lymphotropic virus type 1 (HTLV-1): The ATL Prevention Program Nagasaki. Proc. Jpn. Acad. Ser. B Phys. Biol. Sci. 2011, 87, 152–166. [Google Scholar] [CrossRef] [PubMed]
- Hino, S.; Katamine, S.; Miyata, H.; Tsuji, Y.; Yamabe, T.; Miyamoto, T. Primary prevention of HTLV-1 in Japan. Leukemia 1997, 11 (Suppl. 3), 57–59. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.A.; Martins, M.L.; Teixeira, C.; Ladeira, R.; Oliveira Mde, F.; Januario, J.N.; Proietti, F.A.; Carneiro-Proietti, A.B. Blocking vertical transmission of human T cell lymphotropic virus type 1 and 2 through breastfeeding interruption. Pediatr. Infect. Dis. J. 2012, 31, 1139–1143. [Google Scholar] [CrossRef] [PubMed]
- Hino, S.; Yamaguchi, K.; Katamine, S.; Sugiyama, H.; Amagasaki, T.; Kinoshita, K.; Yoshida, Y.; Doi, H.; Tsuji, Y.; Miyamoto, T. Mother-to-child transmission of human T-cell leukemia virus type-I. Jpn. J. Cancer Res. 1985, 76, 474–480. [Google Scholar] [PubMed]
- Komuro, A.; Hayami, M.; Fujii, H.; Miyahara, S.; Hirayama, M. Vertical transmission of adult T-cell leukaemia virus. Lancet 1983, 1, 240. [Google Scholar] [CrossRef]
- Satow, Y.; Hashido, M.; Ishikawa, K.; Honda, H.; Mizuno, M.; Kawana, T.; Hayami, M. Detection of HTLV-I antigen in peripheral and cord blood lymphocytes from carrier mothers. Lancet 1991, 338, 915–916. [Google Scholar] [PubMed]
- Chakraborty, J.; Clark, S.; Okonta, H.; Duggan, J. A small animal model for mother-to-fetus transmission of ts1, a murine retrovirus. Viral Immunol. 2003, 16, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Duggan, J.; Okonta, H.; Chakraborty, J. Transmission of Moloney murine leukemia virus (ts-1) by breast milk. J. Gen. Virol. 2006, 87 Pt 9, 2679–2684. [Google Scholar] [CrossRef] [PubMed]
- Bittner, J.J. Relation of nursing to the extra-chromosomal theory of breast cancer in mice. Am. J. Cancer 1939, 35, 90–97. [Google Scholar] [PubMed]
- Le Jan, C.; Bellaton, C.; Greenland, T.; Mornex, J.F. Mammary transmission of caprine arthritis encephalitis virus: A 3D model for in vitro study. Reprod. Nutr. Dev. 2005, 45, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, K.; Hino, S.; Amagaski, T.; Ikeda, S.; Yamada, Y.; Suzuyama, J.; Momita, S.; Toriya, K.; Kamihira, S.; Ichimaru, M. Demonstration of adult T-cell leukemia virus antigen in milk from three sero-positive mothers. Gann 1984, 75, 103–105. [Google Scholar] [PubMed]
- Matsubara, F.; Haraguchi, K.; Harada, K.; Koizumi, A. Screening for antibodies to human T-cell leukemia virus type I in Japanese breast milk. Biol. Pharm. Bull. 2012, 35, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Li, H.C.; Biggar, R.J.; Miley, W.J.; Maloney, E.M.; Cranston, B.; Hanchard, B.; Hisada, M. Provirus load in breast milk and risk of mother-to-child transmission of human T lymphotropic virus type I. J. Infect. Dis. 2004, 190, 1275–1278. [Google Scholar] [CrossRef] [PubMed]
- Yamanouchi, K.; Kinoshita, K.; Moriuchi, R.; Katamine, S.; Amagasaki, T.; Ikeda, S.; Ichimaru, M.; Miyamoto, T.; Hino, S. Oral transmission of human T-cell leukemia virus type-I into a common marmoset (Callithrix jacchus) as an experimental model for milk-borne transmission. Jpn. J. Cancer Res. 1985, 76, 481–487. [Google Scholar] [PubMed]
- Kinoshita, K.; Yamanouchi, K.; Ikeda, S.; Momita, S.; Amagasaki, T.; Soda, H.; Ichimaru, M.; Moriuchi, R.; Katamine, S.; Miyamoto, T.; et al. Oral infection of a common marmoset with human T-cell leukemia virus type-I (HTLV-I) by inoculating fresh human milk of HTLV-I carrier mothers. Jpn. J. Cancer Res. 1985, 76, 1147–1153. [Google Scholar] [PubMed]
- Uemura, Y.; Kotani, S.; Yoshimoto, S.; Fujishita, M.; Yano, S.; Ohtsuki, Y.; Miyoshi, I. Oral transmission of human T-cell leukemia virus type I in the rabbit. Jpn. J. Cancer Res. 1986, 77, 970–973. [Google Scholar] [PubMed]
- Kato, H.; Koya, Y.; Ohashi, T.; Hanabuchi, S.; Takemura, F.; Fujii, M.; Tsujimoto, H.; Hasegawa, A.; Kannagi, M. Oral administration of human T-cell leukemia virus type 1 induces immune unresponsiveness with persistent infection in adult rats. J. Virol. 1998, 72, 7289–7293. [Google Scholar] [PubMed]
- Okochi, K.; Sato, H.; Hinuma, Y. A retrospective study on transmission of adult T cell leukemia virus by blood transfusion: Seroconversion in recipients. Vox Sang. 1984, 46, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, N.; Okada, M.; Koyanagi, Y.; Kannagi, M.; Hinuma, Y. Transformation of human leukocytes by cocultivation with an adult T cell leukemia virus producer cell line. Science 1982, 217, 737–739. [Google Scholar] [CrossRef] [PubMed]
- Popovic, M.; Sarin, P.S.; Robert-Gurroff, M.; Kalyanaraman, V.S.; Mann, D.; Minowada, J.; Gallo, R.C. Isolation and transmission of human retrovirus (human T-cell leukemia virus). Science 1983, 219, 856–859. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.S.; Petrow-Sadowski, C.; Huang, Y.K.; Bertolette, D.C.; Ruscetti, F.W. Cell-free HTLV-1 infects dendritic cells leading to transmission and transformation of CD4+ T cells. Nat. Med. 2008, 14, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Jarvinen, K.M.; Geller, L.; Bencharitiwong, R.; Sampson, H.A. Presence of functional, autoreactive human milk-specific IgE in infants with cow’s milk allergy. Clin. Exp. Allergy 2012, 42, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Ogra, S.S.; Weintraub, D.I.; Ogra, P.L. Immunologic aspects of human colostrum and milk: Interaction with the intestinal immunity of the neonate. Adv. Exp. Med. Biol. 1978, 107, 95–107. [Google Scholar] [PubMed]
- Proietti, F.A.; Carneiro-Proietti, A.B.; Catalan-Soares, B.C.; Murphy, E.L. Global epidemiology of HTLV-I infection and associated diseases. Oncogene 2005, 24, 6058–6068. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, K.; Amagasaki, T.; Hino, S.; Doi, H.; Yamanouchi, K.; Ban, N.; Momita, S.; Ikeda, S.; Kamihira, S.; Ichimaru, M.; et al. Milk-borne transmission of HTLV-I from carrier mothers to their children. Jpn. J. Cancer Res. 1987, 78, 674–680. [Google Scholar] [PubMed]
- Southern, S.O.; Southern, P.J. Persistent HTLV-I infection of breast luminal epithelial cells: A role in HTLV transmission? Virology 1998, 241, 200–214. [Google Scholar] [CrossRef] [PubMed]
- Satomi, M.; Shimizu, M.; Shinya, E.; Watari, E.; Owaki, A.; Hidaka, C.; Ichikawa, M.; Takeshita, T.; Takahashi, H. Transmission of macrophage-tropic HIV-1 by breast-milk macrophages via DC-SIGN. J. Infect. Dis. 2005, 191, 174–181. [Google Scholar] [CrossRef] [PubMed]
- LeVasseur, R.J.; Southern, S.O.; Southern, P.J. Mammary epithelial cells support and transfer productive human T-cell lymphotropic virus infections. J. Hum. Virol. 1998, 1, 214–223. [Google Scholar] [PubMed]
- Takeuchi, H.; Takahashi, M.; Norose, Y.; Takeshita, T.; Fukunaga, Y.; Takahashi, H. Transformation of breast milk macrophages by HTLV-I: Implications for HTLV-I transmission via breastfeeding. Biomed. Res. 2010, 31, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, P.; Southern, S.O.; Southern, P.J.; Pombo-de-Oliveira, M.S. Clinicopathological studies of a patient with adult T-cell leukemia and pseudogynecomasty. Am. J. Hematol. 2000, 65, 256–259. [Google Scholar] [CrossRef]
- Buehring, G.C.; Kramme, P.M.; Schultz, R.D. Evidence for bovine leukemia virus in mammary epithelial cells of infected cows. Lab. Invest. 1994, 71, 359–365. [Google Scholar] [PubMed]
- Schulz, O.; Pabst, O. Antigen sampling in the small intestine. Trends Immunol. 2013, 34, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Takenouchi, N.; Matsuoka, E.; Moritoyo, T.; Nagai, M.; Katsuta, K.; Hasui, K.; Ueno, K.; Eizuru, Y.; Usuku, K.; Osame, M.; et al. Molecular pathologic analysis of the tonsil in HTLV-I-infected individuals. J. Acquir. Immune Defic. Syndr. 1999, 22, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Kazanji, M. HTLV type 1 infection in squirrel monkeys (Saimiri sciureus): A promising animal model for HTLV type 1 human infection. AIDS Res. Hum. Retrovir. 2000, 16, 1741–1746. [Google Scholar] [CrossRef] [PubMed]
- Haynes, R.A., 2nd; Ware, E.; Premanandan, C.; Zimmerman, B.; Yu, L.; Phipps, A.J.; Lairmore, M.D. Cyclosporine-induced immune suppression alters establishment of HTLV-1 infection in a rabbit model. Blood 2010, 115, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Zacharopoulos, V.R.; Perotti, M.E.; Phillips, D.M. Lymphocyte-facilitated infection of epithelia by human T-cell lymphotropic virus type I. J. Virol. 1992, 66, 4601–4605. [Google Scholar] [PubMed]
- Martin-Latil, S.; Gnadig, N.F.; Mallet, A.; Desdouits, M.; Guivel-Benhassine, F.; Jeannin, P.; Prevost, M.C.; Schwartz, O.; Gessain, A.; Ozden, S.; et al. Transcytosis of HTLV-1 across a tight human epithelial barrier and infection of subepithelial dendritic cells. Blood 2012, 120, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Afonso, P.V.; Ozden, S.; Prevost, M.C.; Schmitt, C.; Seilhean, D.; Weksler, B.; Couraud, P.O.; Gessain, A.; Romero, I.A.; Ceccaldi, P.E. Human blood-brain barrier disruption by retroviral-infected lymphocytes: Role of myosin light chain kinase in endothelial tight-junction disorganization. J. Immunol. 2007, 179, 2576–2583. [Google Scholar] [CrossRef] [PubMed]
- Hocini, H.; Bomsel, M. Infectious human immunodeficiency virus can rapidly penetrate a tight human epithelial barrier by transcytosis in a process impaired by mucosal immunoglobulins. J. Infect. Dis. 1999, 179 (Suppl. 3), S448–S453. [Google Scholar] [CrossRef] [PubMed]
- Plancoulaine, S.; Buigues, R.P.; Murphy, E.L.; van Beveren, M.; Pouliquen, J.F.; Joubert, M.; Remy, F.; Tuppin, P.; Tortevoye, P.; de The, G.; et al. Demographic and familial characteristics of HTLV-1 infection among an isolated, highly endemic population of African origin in French Guiana. Int. J. Cancer 1998, 76, 331–336. [Google Scholar] [CrossRef]
- Plancoulaine, S.; Gessain, A.; Joubert, M.; Tortevoye, P.; Jeanne, I.; Talarmin, A.; de The, G.; Abel, L. Detection of a major gene predisposing to human T lymphotropic virus type I infection in children among an endemic population of African origin. J. Infect. Dis. 2000, 182, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, K.J.; Usuku, K.; Hall, S.E.; Matsumoto, W.; Taylor, G.P.; Procter, J.; Bunce, M.; Ogg, G.S.; Welsh, K.I.; Weber, J.N.; et al. HLA alleles determine human T-lymphotropic virus-I (HTLV-I) proviral load and the risk of HTLV-I-associated myelopathy. Proc. Natl. Acad. Sci. USA 1999, 96, 3848–3853. [Google Scholar] [CrossRef] [PubMed]
- Plancoulaine, S.; Gessain, A.; Tortevoye, P.; Boland-Auge, A.; Vasilescu, A.; Matsuda, F.; Abel, L. A major susceptibility locus for HTLV-1 infection in childhood maps to chromosome 6q27. Hum. Mol. Genet. 2006, 15, 3306–3312. [Google Scholar] [CrossRef] [PubMed]
- Sawada, T.; Iwahara, Y.; Ishii, K.; Taguchi, H.; Hoshino, H.; Miyoshi, I. Immunoglobulin prophylaxis against milkborne transmission of human T cell leukemia virus type I in rabbits. J. Infect. Dis. 1991, 164, 1193–1196. [Google Scholar] [CrossRef] [PubMed]
- Ureta-Vidal, A.; Angelin-Duclos, C.; Tortevoye, P.; Murphy, E.; Lepere, J.F.; Buigues, R.P.; Jolly, N.; Joubert, M.; Carles, G.; Pouliquen, J.F.; et al. Mother-to-child transmission of human T-cell-leukemia/lymphoma virus type I: Implication of high antiviral antibody titer and high proviral load in carrier mothers. Int. J. Cancer 1999, 82, 832–836. [Google Scholar] [CrossRef]
- Sawada, T.; Tohmatsu, J.; Obara, T.; Koide, A.; Kamihira, S.; Ichimaru, M.; Kashiwagi, S.; Kajiyama, W.; Matsumura, N.; Kinoshita, K.; et al. High risk of mother-to-child transmission of HTLV-I in p40tax antibody-positive mothers. Jpn. J. Cancer Res. 1989, 80, 506–508. [Google Scholar] [CrossRef] [PubMed]
- Hirata, M.; Hayashi, J.; Noguchi, A.; Nakashima, K.; Kajiyama, W.; Kashiwagi, S.; Sawada, T. The effects of breastfeeding and presence of antibody to p40tax protein of human T cell lymphotropic virus type-I on mother to child transmission. Int. J. Epidemiol. 1992, 21, 989–994. [Google Scholar] [CrossRef] [PubMed]
- Hisada, M.; Maloney, E.M.; Sawada, T.; Miley, W.J.; Palmer, P.; Hanchard, B.; Goedert, J.J.; Manns, A. Virus markers associated with vertical transmission of human T lymphotropic virus type 1 in Jamaica. Clin. Infect. Dis. 2002, 34, 1551–1557. [Google Scholar] [CrossRef] [PubMed]
- Moriuchi, M.; Moriuchi, H. A milk protein lactoferrin enhances human T cell leukemia virus type I and suppresses HIV-1 infection. J. Immunol. 2001, 166, 4231–4236. [Google Scholar] [CrossRef] [PubMed]
- Moriuchi, M.; Moriuchi, H. Induction of lactoferrin gene expression in myeloid or mammary gland cells by human T-cell leukemia virus type 1 (HTLV-1) tax: Implications for milk-borne transmission of HTLV-1. J. Virol. 2006, 80, 7118–7126. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, P.; Tripp, A.; Lairmore, M.D.; Crawford, L.; Sieburg, M.; Ramos, J.C.; Harrington, W., Jr.; Beilke, M.A.; Feuer, G. Adult T-cell leukemia/lymphoma development in HTLV-1-infected humanized SCID mice. Blood 2010, 115, 2640–2648. [Google Scholar] [CrossRef] [PubMed]
- Villaudy, J.; Wencker, M.; Gadot, N.; Gillet, N.A.; Scoazec, J.Y.; Gazzolo, L.; Manz, M.G.; Bangham, C.R.; Dodon, M.D. HTLV-1 propels thymic human T cell development in “human immune system” Rag2−/− λc−/− mice. PLoS Pathog. 2011, 7, e1002231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dodon, M.D.; Villaudy, J.; Gazzolo, L.; Haines, R.; Lairmore, M. What we are learning on HTLV-1 pathogenesis from animal models. Front. Microbiol. 2012, 3, 320. [Google Scholar] [CrossRef] [PubMed]
- Ouzilou, L.; Caliot, E.; Pelletier, I.; Prevost, M.C.; Pringault, E.; Colbere-Garapin, F. Poliovirus transcytosis through M-like cells. J. Gen. Virol. 2002, 83 Pt 9, 2177–2182. [Google Scholar] [CrossRef] [PubMed]
- Renz, H.; Brandtzaeg, P.; Hornef, M. The impact of perinatal immune development on mucosal homeostasis and chronic inflammation. Nat. Rev. Immunol. 2012, 12, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Van de Pavert, S.A.; Mebius, R.E. New insights into the development of lymphoid tissues. Nat. Rev. Immunol. 2010, 10, 664–674. [Google Scholar] [CrossRef] [PubMed]
- Maranduba, C.M.; De Castro, S.B.; de Souza, G.T.; Rossato, C.; da Guia, F.C.; Valente, M.A.; Rettore, J.V.; Maranduba, C.P.; de Souza, C.M.; do Carmo, A.M.; et al. Intestinal microbiota as modulators of the immune system and neuroimmune system: Impact on the host health and homeostasis. J. Immunol. Res. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Shu, Z.; Ma, J.; Tuerhong, D.; Yang, C.; Upur, H. How intestinal bacteria can promote HIV replication. AIDS Rev. 2013, 15, 32–37. [Google Scholar] [PubMed]
- Kane, M.; Case, L.K.; Kopaskie, K.; Kozlova, A.; MacDearmid, C.; Chervonsky, A.V.; Golovkina, T.V. Successful transmission of a retrovirus depends on the commensal microbiota. Science 2011, 334, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, L.; Langa, S.; Martin, V.; Jimenez, E.; Martin, R.; Rodriguez, J.M. The microbiota of human milk in healthy women. Cell Mol. Biol. 2013, 59, 31–42. [Google Scholar] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Percher, F.; Jeannin, P.; Martin-Latil, S.; Gessain, A.; Afonso, P.V.; Vidy-Roche, A.; Ceccaldi, P.-E. Mother-to-Child Transmission of HTLV-1 Epidemiological Aspects, Mechanisms and Determinants of Mother-to-Child Transmission. Viruses 2016, 8, 40. https://doi.org/10.3390/v8020040
Percher F, Jeannin P, Martin-Latil S, Gessain A, Afonso PV, Vidy-Roche A, Ceccaldi P-E. Mother-to-Child Transmission of HTLV-1 Epidemiological Aspects, Mechanisms and Determinants of Mother-to-Child Transmission. Viruses. 2016; 8(2):40. https://doi.org/10.3390/v8020040
Chicago/Turabian StylePercher, Florent, Patricia Jeannin, Sandra Martin-Latil, Antoine Gessain, Philippe V. Afonso, Aurore Vidy-Roche, and Pierre-Emmanuel Ceccaldi. 2016. "Mother-to-Child Transmission of HTLV-1 Epidemiological Aspects, Mechanisms and Determinants of Mother-to-Child Transmission" Viruses 8, no. 2: 40. https://doi.org/10.3390/v8020040