A Single Lineage of Hepatitis E Virus Causes Both Outbreaks and Sporadic Hepatitis in Sudan

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Serum Samples
2.3. Analysis for Anti-HEV Antibodies
2.4. HEV RNA Detection by Quantitative Real-Time Polymerase Chain Reaction
2.5. PCR Amplification and Sequencing
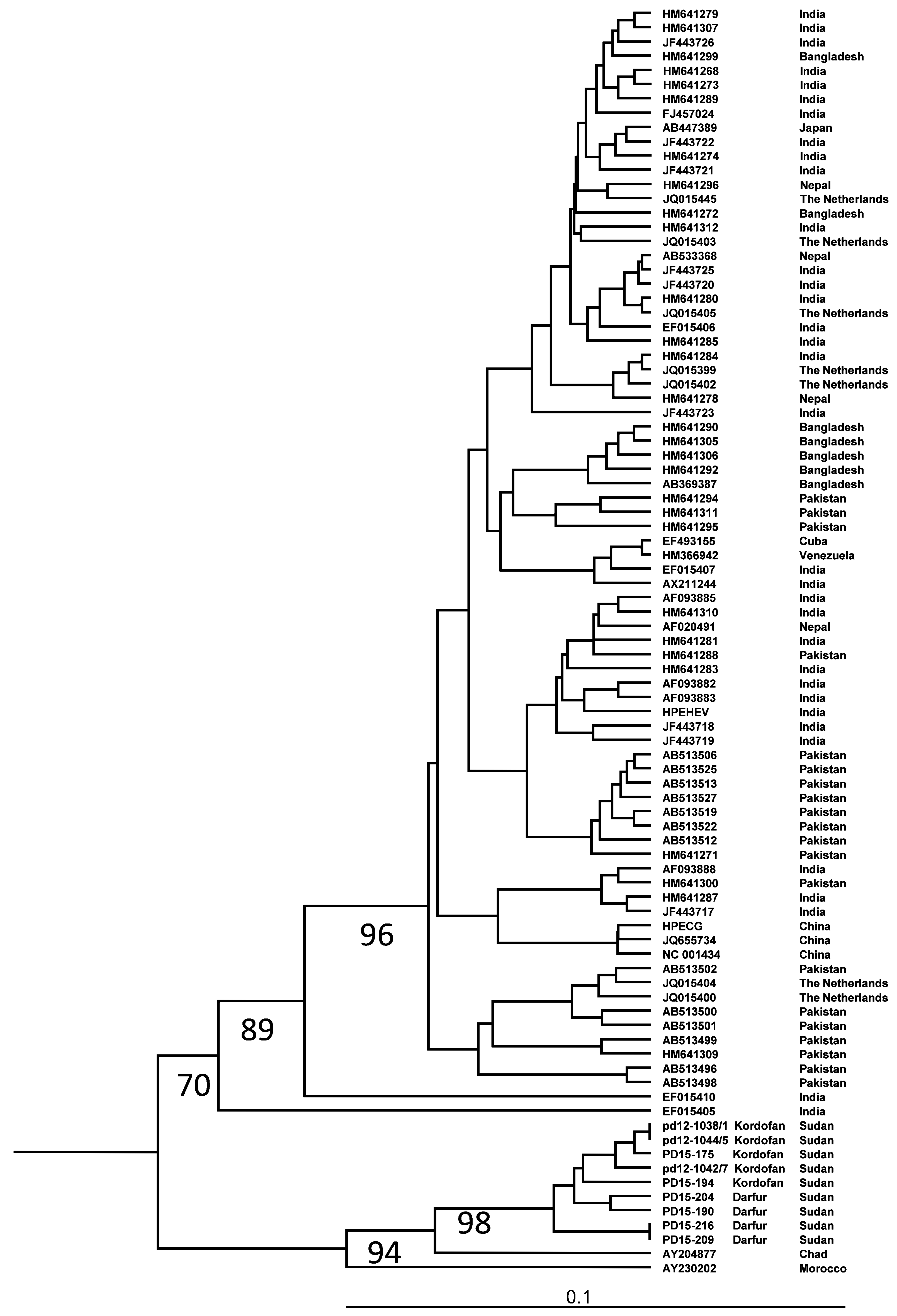
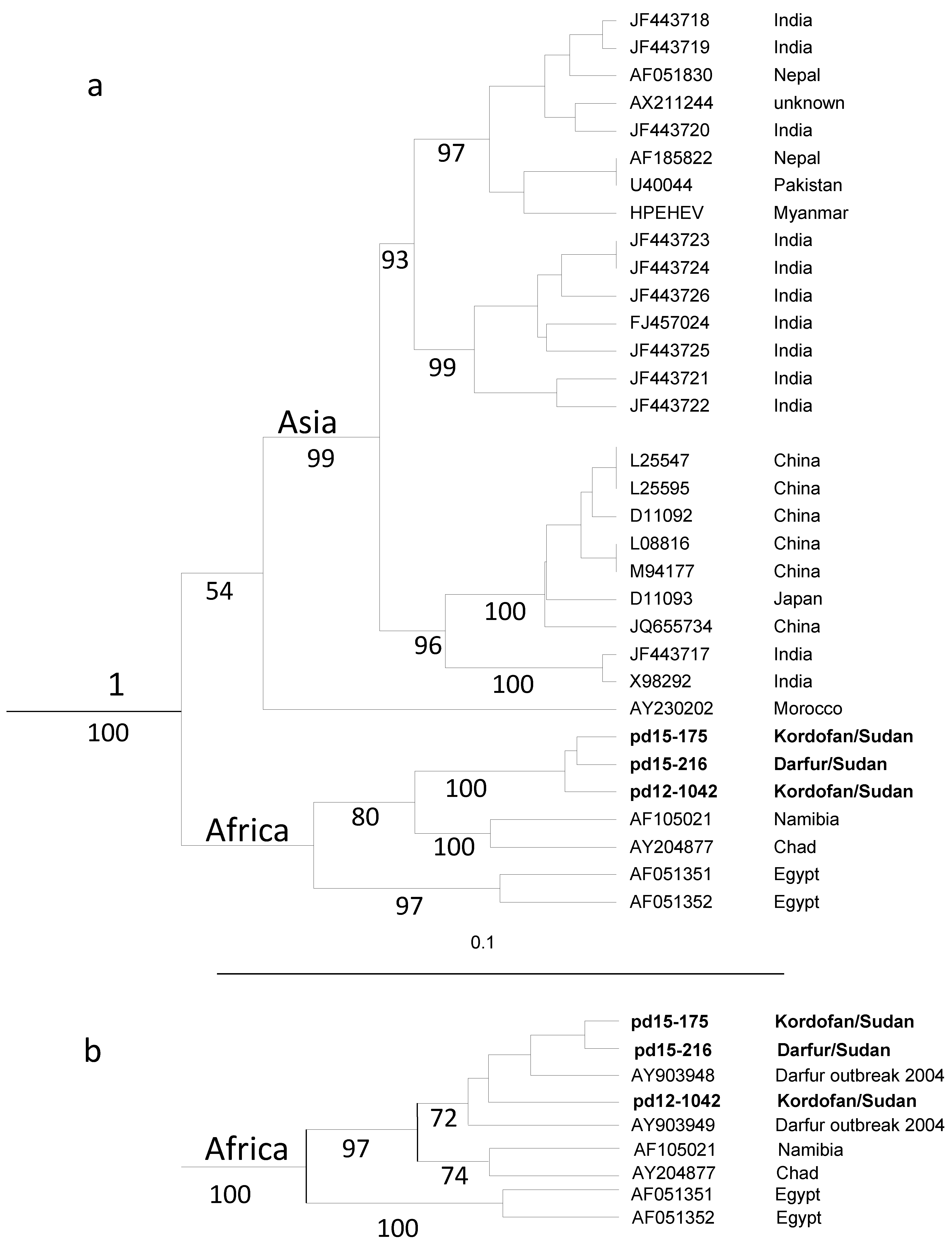
2.6. Phylogenetic Analysis
2.7. Statistical Analysis
3. Results
3.1. Patients
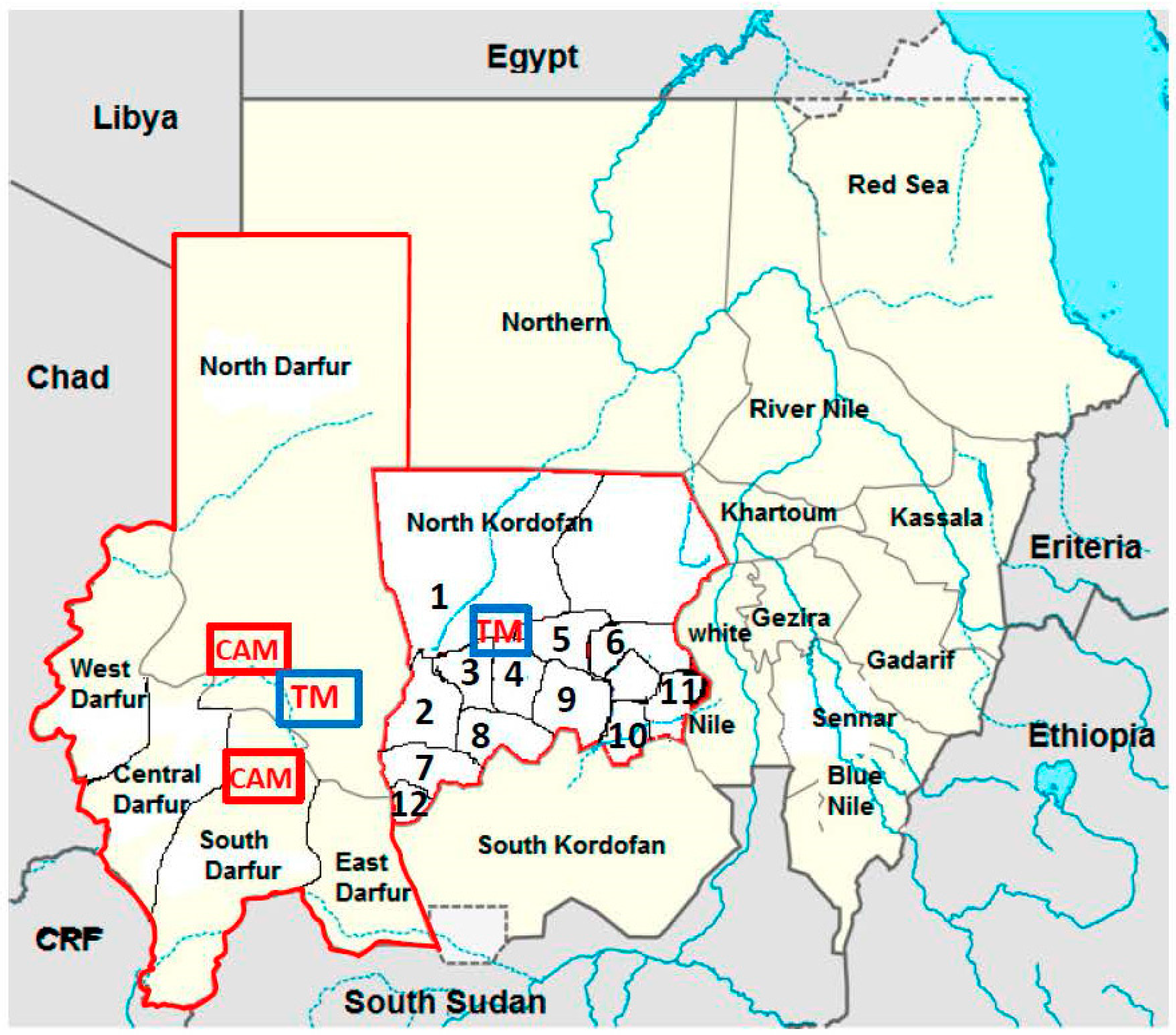
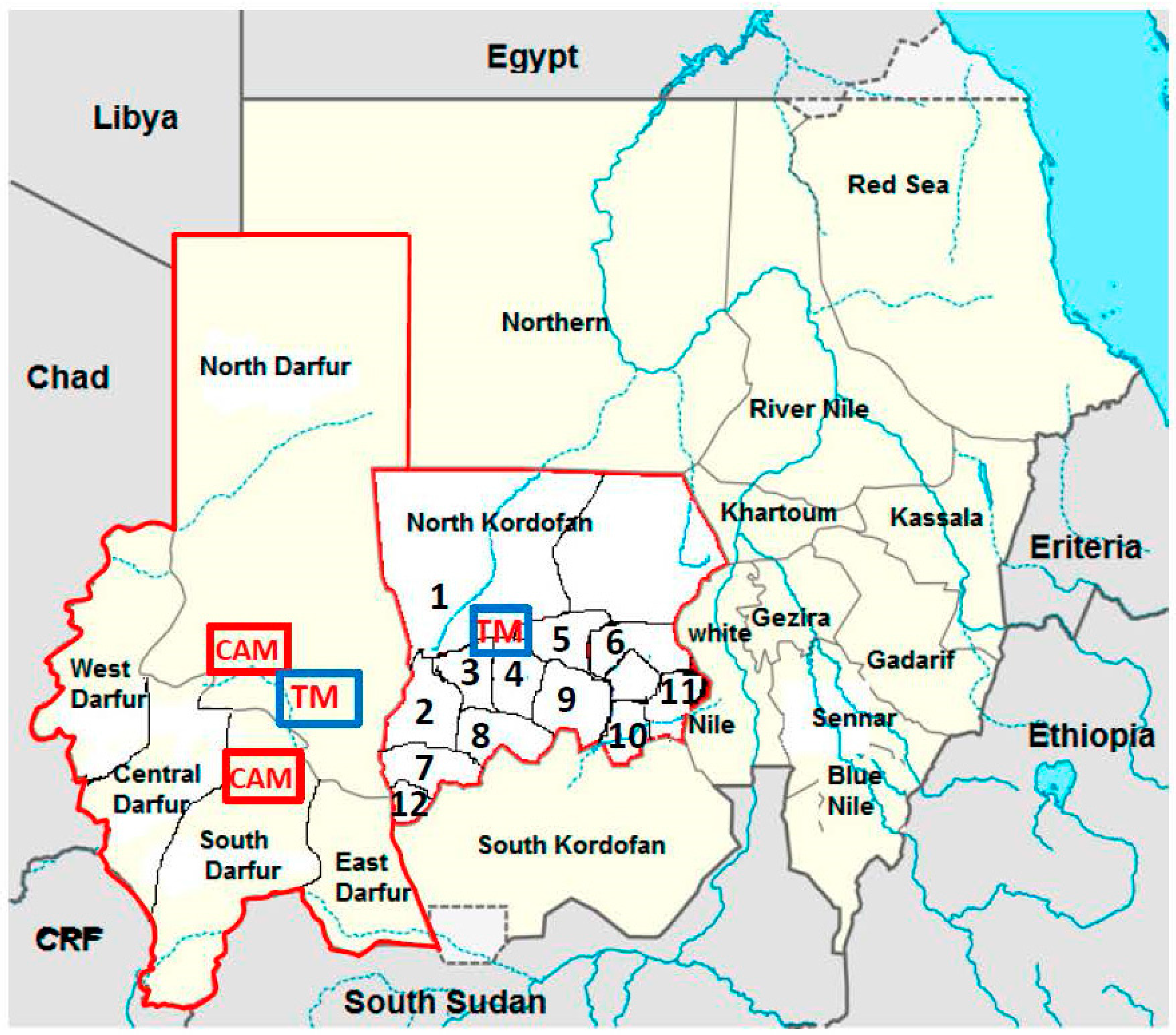
3.2. Sporadic Cases of HEV Infection in North Kordofan from 2011 to 2012
3.3. Outbreaks in Darfur during the Years 2012 and 2014
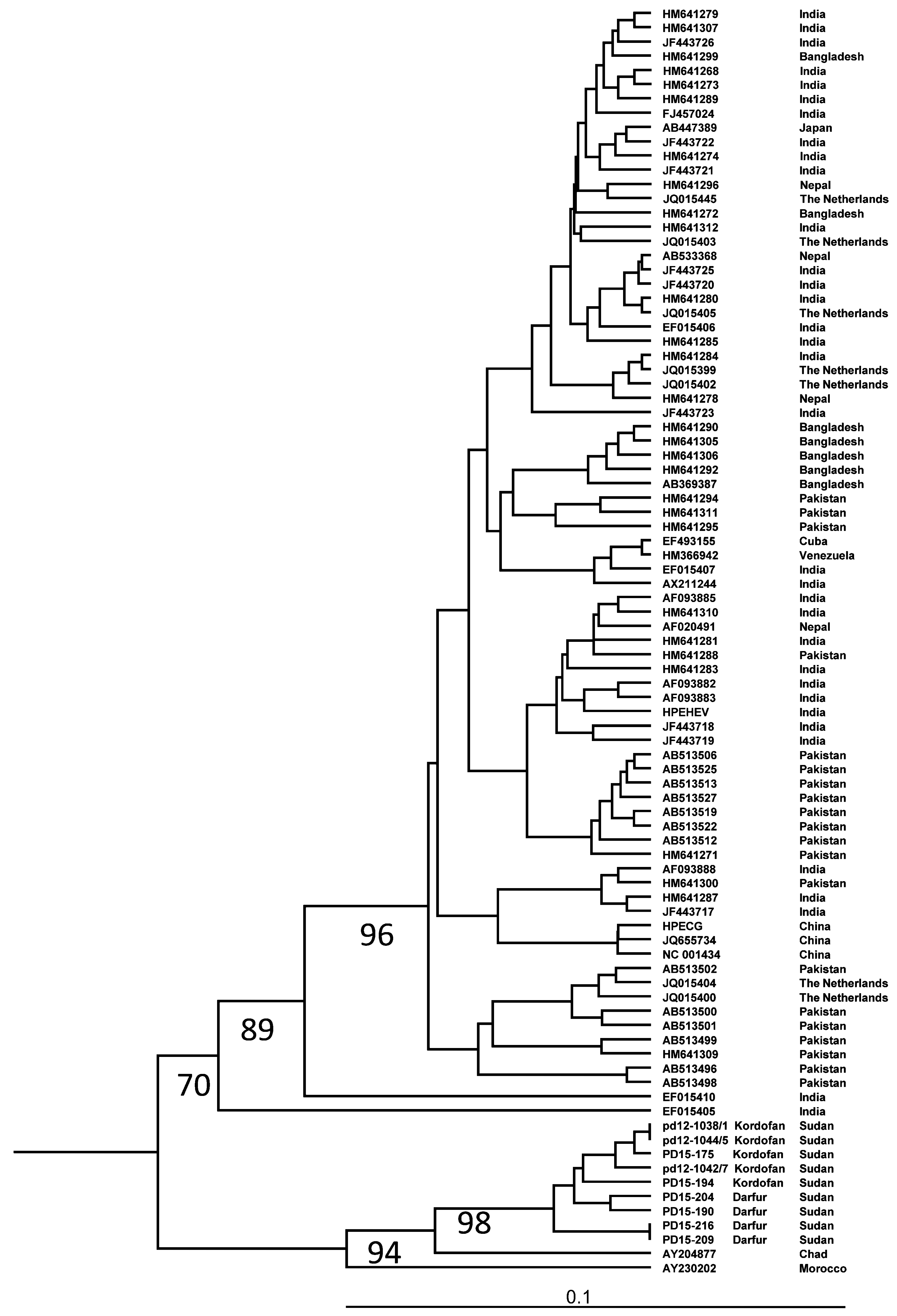
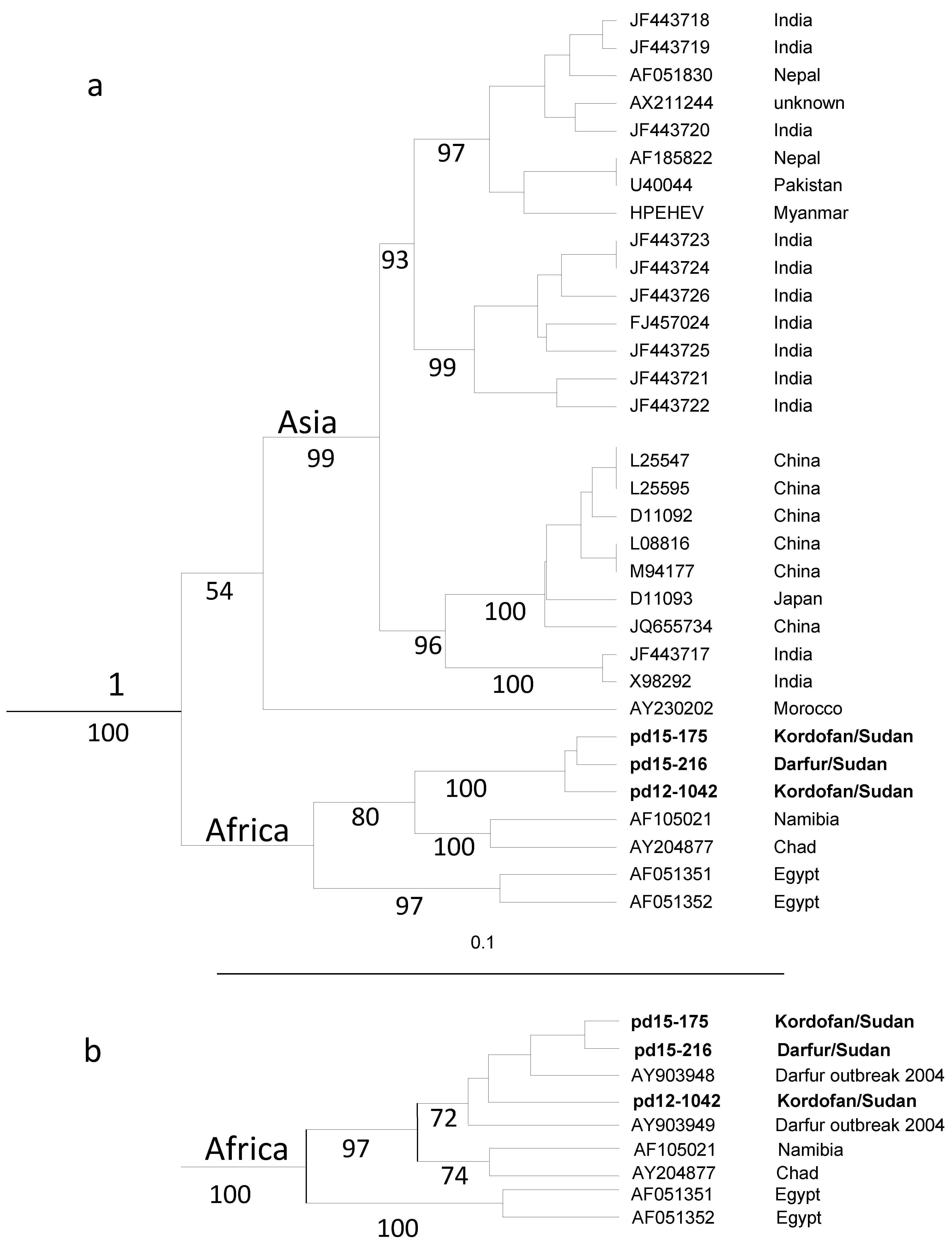
3.4. HEV Genotyping
4. Discussion
5. Conclusions
Acknowledgments
Author Contribution
Conflicts of Interest
References
- Smith, D.B.; Simmonds, P.; Jameel, S.; Emerson, S.U.; Harrison, T.J.; Meng, X.J.; Okamoto, H.; Van der Poel, W.H.; Purdy, M.A. Consensus proposals for classification of the family hepeviridae. J. Gen. Virol. 2015, 96, 1191–1192. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.J. Zoonotic and foodborne transmission of hepatitis E virus. Semin. Liver Dis. 2013, 33, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Abravanel, F.; Lhomme, S.; Dubois, M.; Peron, J.M.; Alric, L.; Kamar, N.; Izopet, J. Hepatitis E virus. Med. Mal. Infect. 2013, 43, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Emerson, S.U.; Purcell, R.H. Hepatitis E. Pediatr. Infect. Dis. J. 2007, 26, 1147–1148. [Google Scholar] [CrossRef] [PubMed]
- Mansuy, J.M.; Bendall, R.; Legrand-Abravanel, F.; Saune, K.; Miedouge, M.; Ellis, V.; Rech, H.; Destruel, F.; Kamar, N.; Dalton, H.R.; et al. Hepatitis E virus antibodies in blood donors, France. Emerg. Infect. Dis. 2011, 17, 2309–2312. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Dalton, H.R.; Abravanel, F.; Izopet, J. Hepatitis E virus infection. Clin. Microbiol. Rev. 2014, 27, 116–138. [Google Scholar] [CrossRef] [PubMed]
- Hino, K.; Kondo, T.; Niwa, H.; Uchida, T.; Shikata, T.; Rikahisa, T.; Mizuno, K. A small epidemic of enterically transmitted non-A, non-B acute hepatitis. Gastroenterol. Jpn. 1991, 26 (Suppl. S3), 139–141. [Google Scholar] [PubMed]
- Balayan, M.S.; Andjaparidze, A.G.; Savinskaya, S.S.; Ketiladze, E.S.; Braginsky, D.M.; Savinov, A.P.; Poleschuk, V.F. Evidence for a virus in non-A, non-B hepatitis transmitted via the fecal-oral route. Intervirology 1983, 20, 23–31. [Google Scholar] [PubMed]
- Worm, H.C.; van der Poel, W.H.; Brandstatter, G. Hepatitis E: An overview. Microbes Infect. 2002, 4, 657–666. [Google Scholar] [CrossRef]
- Kumar, S.; Ratho, R.K.; Chawla, Y.K.; Chakraborti, A. The incidence of sporadic viral hepatitis in North India: A preliminary study. Hepatobiliary Pancreat. Dis. Int. 2007, 6, 596–599. [Google Scholar] [PubMed]
- Aubry, P.; Niel, L.; Niyongabo, T.; Kerguelen, S.; Larouze, B. Seroprevalence of hepatitis E virus in an adult urban population from Burundi. Am. J. Trop. Med. Hyg. 1997, 57, 272–273. [Google Scholar] [PubMed]
- Bile, K.; Isse, A.; Mohamud, O.; Allebeck, P.; Nilsson, L.; Norder, H.; Mushahwar, I.K.; Magnius, L.O. Contrasting roles of rivers and wells as sources of drinking water on attack and fatality rates in a hepatitis E epidemic in Somalia. Am. J. Trop. Med. Hyg. 1994, 51, 466–474. [Google Scholar] [PubMed]
- Howard, C.M.; Handzel, T.; Hill, V.R.; Grytdal, S.P.; Blanton, C.; Kamili, S.; Drobeniuc, J.; Hu, D.; Teshale, E. Novel risk factors associated with hepatitis E virus infection in a large outbreak in Northern Uganda: Results from a case-control study and environmental analysis. Am. J. Trop. Med. Hyg. 2010, 83, 1170–1173. [Google Scholar] [CrossRef] [PubMed]
- Krawczynski, K.; Kamili, S.; Aggarwal, R. Global epidemiology and medical aspects of hepatitis E. Forum (Genova) 2001, 11, 166–179. [Google Scholar] [PubMed]
- Teshale, E.H.; Grytdal, S.P.; Howard, C.; Barry, V.; Kamili, S.; Drobeniuc, J.; Hill, V.R.; Okware, S.; Hu, D.J.; Holmberg, S.D. Evidence of person-to-person transmission of hepatitis E virus during a large outbreak in Northern Uganda. Clin. Infect. Dis. 2010, 50, 1006–1010. [Google Scholar] [CrossRef] [PubMed]
- Teshale, E.H.; Howard, C.M.; Grytdal, S.P.; Handzel, T.R.; Barry, V.; Kamili, S.; Drobeniuc, J.; Okware, S.; Downing, R.; Tappero, J.W.; et al. Hepatitis E epidemic, Uganda. Emerg. Infect. Dis. 2010, 16, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Tsega, E.; Krawczynski, K.; Hansson, B.G.; Nordenfelt, E.; Negusse, Y.; Alemu, W.; Bahru, Y. Outbreak of acute hepatitis E virus infection among military personnel in Northern Ethiopia. J. Med. Virol. 1991, 34, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Hyams, K.C.; Purdy, M.A.; Kaur, M.; McCarthy, M.C.; Hussain, M.A.; El-Tigani, A.; Krawczynski, K.; Bradley, D.W.; Carl, M. Acute sporadic hepatitis E in Sudanese children: Analysis based on a new western blot assay. J. Infect. Dis. 1992, 165, 1001–1005. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.C.; He, J.; Hyams, K.C.; El-Tigani, A.; Khalid, I.O.; Carl, M. Acute hepatitis E infection during the 1988 floods in Khartoum, Sudan. Trans. R. Soc. Trop. Med. Hyg. 1994, 88, 177. [Google Scholar] [CrossRef]
- Ahmed, R.E.; Karsany, M.S.; Adam, I. Brief report: Acute viral hepatitis and poor maternal and perinatal outcomes in pregnant Sudanese women. J. Med. Virol. 2008, 80, 1747–1748. [Google Scholar] [CrossRef] [PubMed]
- Boccia, D.; Guthmann, J.P.; Klovstad, H.; Hamid, N.; Tatay, M.; Ciglenecki, I.; Nizou, J.Y.; Nicand, E.; Guerin, P.J. High mortality associated with an outbreak of hepatitis E among displaced persons in Darfur, Sudan. Clin. Infect. Dis. 2006, 42, 1679–1684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayis, D.A.; Jumaa, A.M.; Gasim, G.I.; Karsany, M.S.; Adam, I. An outbreak of hepatitis E and high maternal mortality at port Sudan, Eastern Sudan. Pathog. Glob. Health 2013, 107, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Hepatitis E: Chad, Sudan. Weekly Epidemiological Record (WER) 2004, 79, 321.
- Hepatitis E, Chad. Weekly Epidemiological Record (WER) 2004, 79, 313.
- Browne, L.B.; Menkir, Z.; Kahi, V.; Maina, G.; Asnakew, S.; Tubman, M.; Elyas, H.Z.; Nigatu, A.; Dak, D.; Maung, U.A.; et al. Notes from the field: Hepatitis E outbreak among refugees from south Sudan—Gambella, Ethiopia, April 2014–January 2015. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 537. [Google Scholar] [PubMed]
- Nicand, E.; Armstrong, G.L.; Enouf, V.; Guthmann, J.P.; Guerin, J.P.; Caron, M.; Nizou, J.Y.; Andraghetti, R. Genetic heterogeneity of hepatitis E virus in Darfur, Sudan, and neighboring Chad. J. Med. Virol. 2005, 77, 519–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norder, H.; Sundqvist, L.; Magnusson, L.; Ostergaard Breum, S.; Lofdahl, M.; Larsen, L.E.; Hjulsager, C.K.; Magnius, L.; Bottiger, B.E.; Widen, F. Endemic hepatitis E in two Nordic countries. Eurosurveillance 2009, 14, 20–28. [Google Scholar]
- Widen, F.; Sundqvist, L.; Matyi-Toth, A.; Metreveli, G.; Belak, S.; Hallgren, G.; Norder, H. Molecular epidemiology of hepatitis E virus in humans, pigs and wild boars in Sweden. Epidemiol. Infect. 2011, 139, 361–371. [Google Scholar] [CrossRef] [PubMed]
- Felsenstein, J. Inferring phylogenies from protein sequences by parsimony, distance and likelyhood methods. Methods Enzymol. 1996, 266, 418–427. [Google Scholar] [PubMed]
- Page, R.D. Visualizing phylogenetic trees using TreeView. Curr. Protoc. Bioinform. 2002, 6. [Google Scholar] [CrossRef]
- Mirazo, S.; Ramos, N.; Mainardi, V.; Gerona, S.; Arbiza, J. Transmission, diagnosis, and management of hepatitis E: An update. Hepat. Med. 2014, 6, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S. Discovery of hepatitis E: The epidemic non-A, non-B hepatitis 30 years down the memory lane. Virus Res. 2011, 161, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Byskov, J.; Wouters, J.S.; Sathekge, T.J.; Swanepoel, R. An outbreak of suspected water-borne epidemic non-A non-B hepatitis in northern Botswana with a high prevalence of hepatitis B carriers and hepatitis delta markers among patients. Trans. R. Soc. Trop. Med. Hyg. 1989, 83, 110–116. [Google Scholar] [CrossRef]
- Isaacson, M.; Frean, J.; He, J.; Seriwatana, J.; Innis, B.L. An outbreak of hepatitis E in Northern Namibia, 1983. Am. J. Trop. Med. Hyg. 2000, 62, 619–625. [Google Scholar] [PubMed]
- Benjelloun, S.; Bahbouhi, B.; Bouchrit, N.; Cherkaoui, L.; Hda, N.; Mahjour, J.; Benslimane, A. Seroepidemiological study of an acute hepatitis E outbreak in Morocco. Res. Virol. 1997, 148, 279–287. [Google Scholar] [CrossRef]
- Escriba, J.M.; Nakoune, E.; Recio, C.; Massamba, P.M.; Matsika-Claquin, M.D.; Goumba, C.; Rose, A.M.; Nicand, E.; Garcia, E.; Leklegban, C.; et al. Hepatitis E, central African Republic. Emerg. Infect. Dis. 2008, 14, 681–683. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, J.A.; Moturi, E.; Spiegel, P.; Schilperoord, M.; Burton, W.; Kassim, N.H.; Mohamed, A.; Ochieng, M.; Nderitu, L.; Navarro-Colorado, C.; et al. Hepatitis E outbreak, dadaab refugee camp, Kenya, 2012. Emerg. Infect. Dis. 2013, 19, 1010–1012. [Google Scholar] [CrossRef] [PubMed]
- Gerbi, G.B.; Williams, R.; Bakamutumaho, B.; Liu, S.; Downing, R.; Drobeniuc, J.; Kamili, S.; Xu, F.; Holmberg, S.D.; Teshale, E.H. Hepatitis E as a cause of acute jaundice syndrome in northern Uganda, 2010–2012. Am. J. Trop. Med. Hyg. 2015, 92, 411–414. [Google Scholar] [CrossRef] [PubMed]
- Teshale, E.H.; Hu, D.J. Hepatitis E: Epidemiology and prevention. World J. Hepatol. 2011, 3, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Subhadra, S.; Singh, B.; Panda, B.K. Hepatitis E virus: The current scenario. Int. J. Infect. Dis. 2013, 17, e228–e233. [Google Scholar] [CrossRef] [PubMed]
- Rein, D.B.; Stevens, G.A.; Theaker, J.; Wittenborn, J.S.; Wiersma, S.T. The global burden of hepatitis E virus genotypes 1 and 2 in 2005. Hepatology 2012, 55, 988–997. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Bendall, R.; Legrand-Abravanel, F.; Xia, N.S.; Ijaz, S.; Izopet, J.; Dalton, H.R. Hepatitis E. Lancet 2012, 379, 2477–2488. [Google Scholar] [CrossRef]
- Guthmann, J.P.; Klovstad, H.; Boccia, D.; Hamid, N.; Pinoges, L.; Nizou, J.Y.; Tatay, M.; Diaz, F.; Moren, A.; Grais, R.F.; et al. A large outbreak of hepatitis E among a displaced population in Darfur, Sudan, 2004: The role of water treatment methods. Clin. Infect. Dis. 2006, 42, 1685–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merens, A.; Guerin, P.J.; Guthmann, J.P.; Nicand, E. Outbreak of hepatitis E virus infection in Darfur, Sudan: Effectiveness of real-time reverse transcription-PCR analysis of dried blood spots. J. Clin. Microbiol. 2009, 47, 1931–1933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cummings, M.J.; Wamala, J.F.; Komakech, I.; Lukwago, L.; Malimbo, M.; Omeke, M.E.; Mayer, D.; Bakamutumaho, B. Hepatitis E in Karamoja, Uganda, 2009–2012: Epidemiology and challenges to control in a setting of semi-nomadic pastoralism. Trans. R. Soc. Trop. Med. Hyg. 2014, 108, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Cummings, M.J.; Wamala, J.F.; Eyura, M.; Malimbo, M.; Omeke, M.E.; Mayer, D.; Lukwago, L. A cholera outbreak among semi-nomadic pastoralists in northeastern Uganda: Epidemiology and interventions. Epidemiol. Infect. 2012, 140, 1376–1385. [Google Scholar] [CrossRef] [PubMed]
- Cummings, M.J.; Wamala, J.F.; Komakech, I.; Malimbo, M.; Lukwago, L. Emerging and reemerging epidemic-prone diseases among settling nomadic pastoralists in Uganda. Acta Trop. 2014, 137, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Mishra, N.; Walimbe, A.M.; Arankalle, V.A. Hepatitis E virus from India exhibits significant amino acid mutations in fulminant hepatic failure patients. Virus Genes 2013, 46, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Inoue, J.; Takahashi, M.; Mizuo, H.; Suzuki, K.; Aikawa, T.; Shimosegawa, T.; Okamoto, H. Nucleotide substitutions of hepatitis E virus genomes associated with fulminant hepatitis and disease severity. Tohoku J. Exp. Med. 2009, 218, 279–284. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Region | Number of Hepatitis E Virus (HEV)- Infected Individuals/Total Number of Individuals investigated | Total | ||
|---|---|---|---|---|
| Men Anti-HEV IgM-positive/Total (%) | Women Anti-HEV IgM-positive/Total (%) | |||
| North Kordofan | Alnohod | 20/82 (24) | 24/79 (30) | 44/161 (27) |
| Gibaish | 1/25 (4) | 3/18 (17) | 4/43 (9) | |
| Wad Banda | 6/41 (15) | 10/54 (19) | 16/105 (15) | |
| Abozabad | 2/8 (25) | 3/9 (33) | 5/17 (29) | |
| Shaikan | 0/23 | 2/16 (12) | 2/39 (5) | |
| Al Khawai | 2/5 (40) | 15/19 (79) | 17/24 (71) | |
| Sudari | 0/2 | 0/3 | 0/5 | |
| Bara | 0/5 | 0/2 | 0/7 | |
| West Bara | 4/8 (50) | 6/17 (35) | 10/25 (40) | |
| Alrahad | 0/1 | 0/1 | 0/2 | |
| Omrawaba | 0/1 | 0 | 0/1 | |
| Alodeia | 0/0 | 0/3 | 0/3 | |
| Subtotal | 35/211 (17) | 63/221 (28) | 98/432 (23) | |
| Darfur | North Darfur | 21/30 (70) | 1/4 (25) | 22/34 (65) |
| Central Darfur | 4/29 (13) | 0/6 | 4/35 (11) | |
| West Darfur | 3/23 (13) | 3/6 (50) | 6/29 (21) | |
| East Darfur | 0/0 | 1/6 (17) | 1/6 (17) | |
| South Darfur | 14/41 (34) | 2/7 (28) | 16/48 (33) | |
| Subtotal | 42/123 (34) | 7/29 (24) | 49/152 (32) | |
| TOTAL | 77/334 (23%) | 70/250 (28%) | 147/584 (25%) | |
| Clinical Symptom | Number of Patients with Hepatitis E and Respective Symptom |
|---|---|
| Jaundice | 97 (99%) |
| Fever | 94 (96%) |
| Abdominal pain | 72 (73.5%) |
| Loss of appetite | 68 (69.4%) |
| Vomiting | 72 (73.5%) |
| Joint pain | 47 (48%) |
| Headache | 32 (32.6%) |
| Region | Age (Years) | Men | Women | Total | HEV RNA Positive/Total Number Investigated |
|---|---|---|---|---|---|
| Number of HEV-Infected Individuals/Total Number Investigated (%) | Number of HEV-Infected Individuals/Total Number Investigated (%) | ||||
| North Kordofan | <5 | 4/21 (19%) | 1/11 (9%) | 5/32 (16%) | 4/5 |
| 5–14 | 7/48 (15%) | 18/48 (37%) | 25/96 (26%) | 9/25 | |
| 15–24 | 10/45 (22%) | 20/55 (36%) | 30/100 (30%) | 9/30 | |
| 25–34 | 7/57 12%) | 16/63 (25%) | 23/120 (19%) | 7/23 | |
| 35–44 | 3/15 (20%) | 7/35 (20%) | 10/50 (20%) | 1/10 | |
| 45–54 | 3/13 (23%) | 0/4 | 3/17 (17%) | 1/3 | |
| 55–64 | 1/9 (11%) | 0/2 | 1/11 (9%) | 1/1 | |
| >64 | 0/3 | 1/3 (33%) | 1/6 (17%) | 0/1 | |
| Total | 35/211 (17%) | 63/221 (28%) | 98/432 (23%) | 32/98 | |
| Darfur | <5 | 0/5 | 0/4 | 0/9 | 0 |
| 5–14 | 0/9 | 0/5 | 0/14 | 0 | |
| 15–24 | 16/47 (34%) | 2/5 (40%) | 18/52 (34%) | 5/52 | |
| 25–34 | 21/50 (42%) | 5/19 (50%) | 26/60 (43%) | 12/60 | |
| 35–44 | 4/7 (57%) | 0/3 | 4/10 (40%) | 1/10 | |
| 45–54 | 0/3 | 0/0 | 0/3 | 0 | |
| 55–64 | 1/1 | 0/0 | 1/1 | 0 | |
| >64 | 0/1 | 0/2 | 0/3 | 0 | |
| Total | 42/123 (34%) | 7/29 (24%) | 49/152 (32%) | 18/152 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elduma, A.H.; Zein, M.M.A.; Karlsson, M.; Elkhidir, I.M.E.; Norder, H. A Single Lineage of Hepatitis E Virus Causes Both Outbreaks and Sporadic Hepatitis in Sudan. Viruses 2016, 8, 273. https://doi.org/10.3390/v8100273
Elduma AH, Zein MMA, Karlsson M, Elkhidir IME, Norder H. A Single Lineage of Hepatitis E Virus Causes Both Outbreaks and Sporadic Hepatitis in Sudan. Viruses. 2016; 8(10):273. https://doi.org/10.3390/v8100273
Chicago/Turabian StyleElduma, Adel Hussein, Mai Mohammed Adam Zein, Marie Karlsson, Isam M.E. Elkhidir, and Heléne Norder. 2016. "A Single Lineage of Hepatitis E Virus Causes Both Outbreaks and Sporadic Hepatitis in Sudan" Viruses 8, no. 10: 273. https://doi.org/10.3390/v8100273
APA StyleElduma, A. H., Zein, M. M. A., Karlsson, M., Elkhidir, I. M. E., & Norder, H. (2016). A Single Lineage of Hepatitis E Virus Causes Both Outbreaks and Sporadic Hepatitis in Sudan. Viruses, 8(10), 273. https://doi.org/10.3390/v8100273