

Hepatitis E Virus Infection in Voluntary Blood Donors in the Russian Federation

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Donor Samples
2.2. HEV Testing
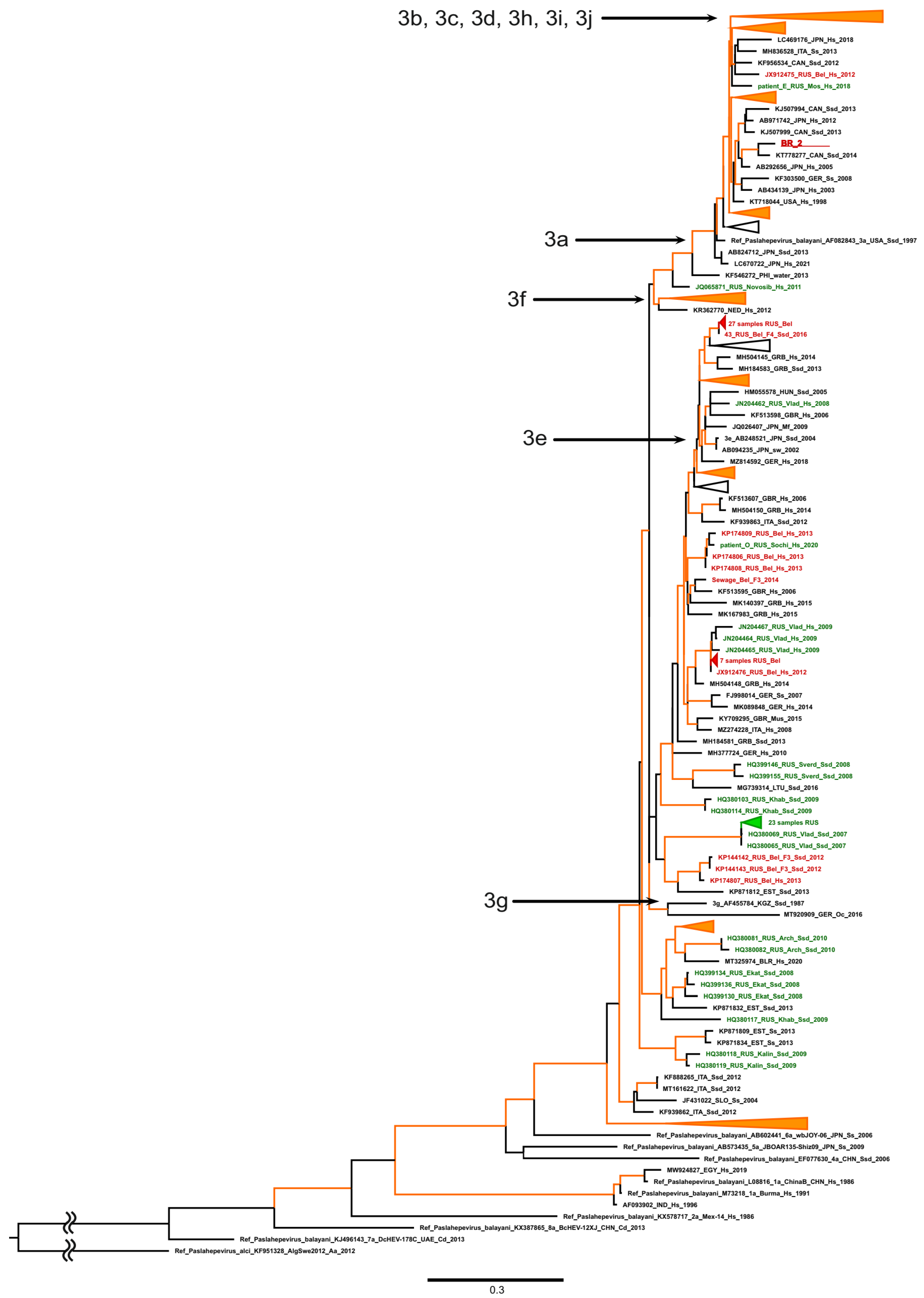
2.3. HEV Sequencing and Phylogenetic Analyses
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Purdy, M.A.; Drexler, J.F.; Meng, X.-J.; Norder, H.; Okamoto, H.; Van der Poel, W.H.M.; Reuter, G.; de Souza, W.M.; Ulrich, R.G.; Smith, D.B. ICTV Virus Taxonomy Profile: Hepeviridae 2022. J. Gen. Virol. 2022, 103, 001778. [Google Scholar] [CrossRef] [PubMed]
- Nelson, K.E.; Labrique, A.B.; Kmush, B.L. Epidemiology of Genotype 1 and 2 Hepatitis E Virus Infections. Cold Spring Harb. Perspect. Med. 2019, 9, a031732. [Google Scholar] [CrossRef] [PubMed]
- Denner, J. Hepatitis E Virus (HEV)—The Future. Viruses 2019, 11, 251. [Google Scholar] [CrossRef] [PubMed]
- Songtanin, B.; Molehin, A.J.; Brittan, K.; Manatsathit, W.; Nugent, K. Hepatitis E Virus Infections: Epidemiology, Genetic Diversity, and Clinical Considerations. Viruses 2023, 15, 1389. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Nishizawa, T.; Sato, H.; Sato, Y.; Jirintai, null; Nagashima, S.; Okamoto, H. Analysis of the Full-Length Genome of a Hepatitis E Virus Isolate Obtained from a Wild Boar in Japan That Is Classifiable into a Novel Genotype. J. Gen. Virol. 2011, 92, 902–908. [Google Scholar] [CrossRef]
- Lee, G.-H.; Tan, B.-H.; Teo, E.C.-Y.; Lim, S.-G.; Dan, Y.-Y.; Wee, A.; Aw, P.P.K.; Zhu, Y.; Hibberd, M.L.; Tan, C.-K.; et al. Chronic Infection with Camelid Hepatitis E Virus in a Liver Transplant Recipient Who Regularly Consumes Camel Meat and Milk. Gastroenterology 2016, 150, 355–357.e3. [Google Scholar] [CrossRef]
- Benavent, S.; Carlos, S.; Reina, G. Rocahepevirus Ratti as an Emerging Cause of Acute Hepatitis Worldwide. Microorganisms 2023, 11, 2996. [Google Scholar] [CrossRef]
- Bi, H.; Yang, R.; Wu, C.; Xia, J. Hepatitis E Virus and Blood Transfusion Safety. Epidemiol. Infect. 2020, 148, e158. [Google Scholar] [CrossRef]
- Cruz, S.; Campos, C.; Timóteo, M.; Tavares, A.; José Nascimento, M.S.; Medeiros, R.; Sousa, H. Hepatitis E Virus in Hematopoietic Stem Cell Transplant Recipients: A Systematic Review. J. Clin. Virol. 2019, 119, 31–36. [Google Scholar] [CrossRef]
- Thakur, V.; Ratho, R.K.; Kumar, S.; Saxena, S.K.; Bora, I.; Thakur, P. Viral Hepatitis E and Chronicity: A Growing Public Health Concern. Front. Microbiol. 2020, 11, 577339. [Google Scholar] [CrossRef]
- Ma, Z.; de Man, R.A.; Kamar, N.; Pan, Q. Chronic Hepatitis E: Advancing Research and Patient Care. J. Hepatol. 2022, 77, 1109–1123. [Google Scholar] [CrossRef]
- Tanaka, A.; Matsubayashi, K.; Odajima, T.; Sakata, H.; Iida, J.; Kai, K.; Goto, N.; Satake, M. Universal Nucleic Acid Donor Screening Revealed Epidemiological Features of Hepatitis E and Prevented Transfusion-Transmitted Infection in Japan. Transfusion 2024, 64, 335–347. [Google Scholar] [CrossRef]
- Boland, F.; Martinez, A.; Pomeroy, L.; O’Flaherty, N. Blood Donor Screening for Hepatitis E Virus in the European Union. Transfus. Med. Hemotherapy Off. Organ Dtsch. Ges. Transfusionsmedizin Immunhamatol. 2019, 46, 95–103. [Google Scholar] [CrossRef]
- Mikhailov, M.I.; Karlsen, A.A.; Potemkin, I.A.; Isaeva, O.V.; Kichatova, V.S.; Malinnikova, E.Y.; Asadi Mobarkhan, F.A.; Mullin, E.V.; Lopatukhina, M.A.; Manuylov, V.A.; et al. Geographic and Temporal Variability of Hepatitis E Virus Circulation in the Russian Federation. Viruses 2022, 15, 37. [Google Scholar] [CrossRef]
- Kyuregyan, K.K.; Polyakov, A.D.; Potemkin, I.A.; Karlsen, A.A.; Isaeva, O.V.; Lopatukhina, M.A.; Mullin, E.V.; Slukinova, O.S.; Malinnikova, E.Y.; Shibrik, E.V.; et al. Belgorod region—The territory endemic for hepatitis E. Vopr. Virusol. 2019, 64, 274–280. [Google Scholar] [CrossRef]
- Potemkin, I.A.; Kyuregyan, K.K.; Isaeva, O.V.; Belyakova, V.V.; Mayorova, O.A.; Shchibrik, E.V.; Polyakov, A.D.; Malinnikova, E.Y.; Mikhailov, M.I. Prevalence of markers of hepatitis E among blood donors in the regions of the Russian Federation. Hematol. Transfusiol. 2013, 58, 26–28. [Google Scholar]
- Tamura, K.; Stecher, G.; Kumar, S. MEGA11: Molecular Evolutionary Genetics Analysis Version 11. Mol. Biol. Evol. 2021, 38, 3022–3027. [Google Scholar] [CrossRef]
- Al-Sadeq, D.W.; Majdalawieh, A.F.; Nasrallah, G.K. Seroprevalence and Incidence of Hepatitis E Virus among Blood Donors: A Review. Rev. Med. Virol. 2017, 27, e1937. [Google Scholar] [CrossRef]
- Izopet, J.; Lhomme, S.; Chapuy-Regaud, S.; Mansuy, J.-M.; Kamar, N.; Abravanel, F. HEV and Transfusion-Recipient Risk. Transfus. Clin. Biol. 2017, 24, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Mättö, J.; Putkuri, N.; Rimhanen-Finne, R.; Laurila, P.; Clancy, J.; Ihalainen, J.; Ekblom-Kullberg, S. Hepatitis E Virus in Finland: Epidemiology and Risk in Blood Donors and in the General Population. Pathogens 2023, 12, 484. [Google Scholar] [CrossRef] [PubMed]
- Gorski, I.; Babić, I.; Bingulac-Popović, J.; Topić-Šestan, P.; Jagnjić, S.; Jemeršić, L.; Prpić, J.; Jukić, I. Prevalence of HEV RNA in Croatian Blood Donors. Transfus. Clin. Biol. 2023, 30, 244–248. [Google Scholar] [CrossRef]
- Harvala, H.; Hewitt, P.E.; Reynolds, C.; Pearson, C.; Haywood, B.; Tettmar, K.I.; Ushiro-Lumb, I.; Brailsford, S.R.; Tedder, R.; Ijaz, S. Hepatitis E Virus in Blood Donors in England, 2016 to 2017: From Selective to Universal Screening. Euro Surveill. 2019, 24, 1800386. [Google Scholar] [CrossRef] [PubMed]
- Bes, M.; Costafreda, M.I.; Riveiro-Barciela, M.; Piron, M.; Rico, A.; Quer, J.; Puig, L.; Sauleda, S. Effect of Hepatitis E Virus RNA Universal Blood Donor Screening, Catalonia, Spain, 2017–2020. Emerg. Infect. Dis. 2022, 28, 157–165. [Google Scholar] [CrossRef]
- Wolski, A.; Pischke, S.; Ozga, A.-K.; Addo, M.M.; Horvatits, T. Higher Risk of HEV Transmission and Exposure among Blood Donors in Europe and Asia in Comparison to North America: A Meta-Analysis. Pathogens 2023, 12, 425. [Google Scholar] [CrossRef]
- Mishra, K.K.; Patel, K.; Trivedi, A.; Patel, P.; Ghosh, K.; Bharadva, S. Risk of Hepatitis-E Virus Infections among Blood Donors in a Regional Blood Transfusion Centre in Western India. Transfus. Med. 2021, 31, 193–199. [Google Scholar] [CrossRef]
- Tsoi, W.-C.; Zhu, X.; To, A.P.-C.; Holmberg, J. Hepatitis E Virus Infection in Hong Kong Blood Donors. Vox Sang. 2020, 115, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Kuznetsova, T.; Moor, D.; Khanirzayeva, G.; Geller, J. Evaluation of Prevalence of Hepatitis E Clinical Markers among Donors in Estonia. Viruses 2023, 15, 2118. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.C.; Martin, V.; Linh, L.T.K.; Giang, T.T.; Chau, N.T.M.; Anh, T.N.P.; Nghia, V.X.; The, N.T.; My, T.N.; Sy, B.T.; et al. High Hepatitis E Virus (HEV) Seroprevalence and No Evidence of HEV Viraemia in Vietnamese Blood Donors. Viruses 2023, 15, 2075. [Google Scholar] [CrossRef] [PubMed]
- Savchuk, T.N.; Greenwald, E.N.; Abdrakhmanova, S.A.; Imashpaev, D.M.; Zhangazieva, K.H.; Sausakova, S.B. Study of the prevalence of hepatitis E virus RNA among blood donors in the Republic of Kazakhstan. In Proceedings of the Collection of Proceedings XI International Scientific and Practical Conference “Molecular Diagnostics”, Moscow, Russia, 14–16 November 2023; pp. 12–13. [Google Scholar]
- Laperche, S.; Maugard, C.; Lhomme, S.; Lecam, S.; Ricard, C.; Dupont, I.; Richard, P.; Tiberghien, P.; Abravanel, F.; Morel, P.; et al. Seven Years (2015–2021) of Blood Donor Screening for HEV-RNA in France: Lessons and Perspectives. Blood Transfus. 2023, 21, 110–118. [Google Scholar] [CrossRef]
- Satake, M.; Matsubayashi, K.; Hoshi, Y.; Taira, R.; Furui, Y.; Kokudo, N.; Akamatsu, N.; Yoshizumi, T.; Ohkohchi, N.; Okamoto, H.; et al. Unique Clinical Courses of Transfusion-Transmitted Hepatitis E in Patients with Immunosuppression. Transfusion 2017, 57, 280–288. [Google Scholar] [CrossRef]
- Dreier, J.; Knabbe, C.; Vollmer, T. Transfusion-Transmitted Hepatitis E: NAT Screening of Blood Donations and Infectious Dose. Front. Med. 2018, 5, 5. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Region | Number of Tested Donors | Number of HEV RNA-Positive Donors | HEV RNA Detection Rate, % (95% CI) | HEV RNA Positivity Ratio | p * |
|---|---|---|---|---|---|
| Moscow | 14,533 | 3 | 0.021% (0.01–0.06%) | 1:4844 | 0.9518 |
| Belgorod | 5872 | 2 | 0.034% (0.01–0.13%) | 1:2936 | |
| Both regions combined | 20,405 | 5 | 0.024% (0.01–0.05%) | 1:4081 |
| Donor # | Study Region | Donor Gender | Donor Age, Years | Ct in Pool of 6 | Ct in Individual Samples |
|---|---|---|---|---|---|
| MSK_1 | Moscow | female | 39 | 40.4 | 37.5 |
| MSK_2 | Moscow | female | 54 | 39.1 | 41.4 |
| MSK_3 | Moscow | male | 42 | 40.5 | 37.1 |
| BR_1 | Belgorod | male | 41 | 37.6 | 33.5 |
| BR_2 | Belgorod | male | 38 | 25.0 | 20.9 |
| Donor ID | Initial Testing | Follow-Up Testing (6 Months Later, on Average) | ||||
|---|---|---|---|---|---|---|
| HEV RNA | Anti-HEV IgM | Anti-HEV IgG | HEV RNA | Anti-HEV IgM | Anti-HEV IgG | |
| MSK_1 | positive | positive | negative | lost to follow-up | no data | no data |
| MSK_2 | positive | positive | positive | negative | negative | positive |
| MSK_3 | positive | negative | negative | negative | negative | positive |
| BR_1 | positive | positive | positive | negative | negative | positive |
| BR_2 | positive | negative | negative | negative | positive | positive |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Potemkin, I.A.; Kyuregyan, K.K.; Karlsen, A.A.; Isaeva, O.V.; Kichatova, V.S.; Lopatukhina, M.A.; Asadi Mobarkhan, F.A.; Zlobina, A.G.; Zheltobriukh, A.V.; Bocharova, K.A.; et al. Hepatitis E Virus Infection in Voluntary Blood Donors in the Russian Federation. Viruses 2024, 16, 526. https://doi.org/10.3390/v16040526
Potemkin IA, Kyuregyan KK, Karlsen AA, Isaeva OV, Kichatova VS, Lopatukhina MA, Asadi Mobarkhan FA, Zlobina AG, Zheltobriukh AV, Bocharova KA, et al. Hepatitis E Virus Infection in Voluntary Blood Donors in the Russian Federation. Viruses. 2024; 16(4):526. https://doi.org/10.3390/v16040526
Chicago/Turabian StylePotemkin, Ilya A., Karen K. Kyuregyan, Anastasia A. Karlsen, Olga V. Isaeva, Vera S. Kichatova, Maria A. Lopatukhina, Fedor A. Asadi Mobarkhan, Anna G. Zlobina, Andrey V. Zheltobriukh, Ksenia A. Bocharova, and et al. 2024. "Hepatitis E Virus Infection in Voluntary Blood Donors in the Russian Federation" Viruses 16, no. 4: 526. https://doi.org/10.3390/v16040526