Does Secondhand Smoke Affect the Development of Dental Caries in Children? A Systematic Review


Abstract
:1. Introduction
2. Methods
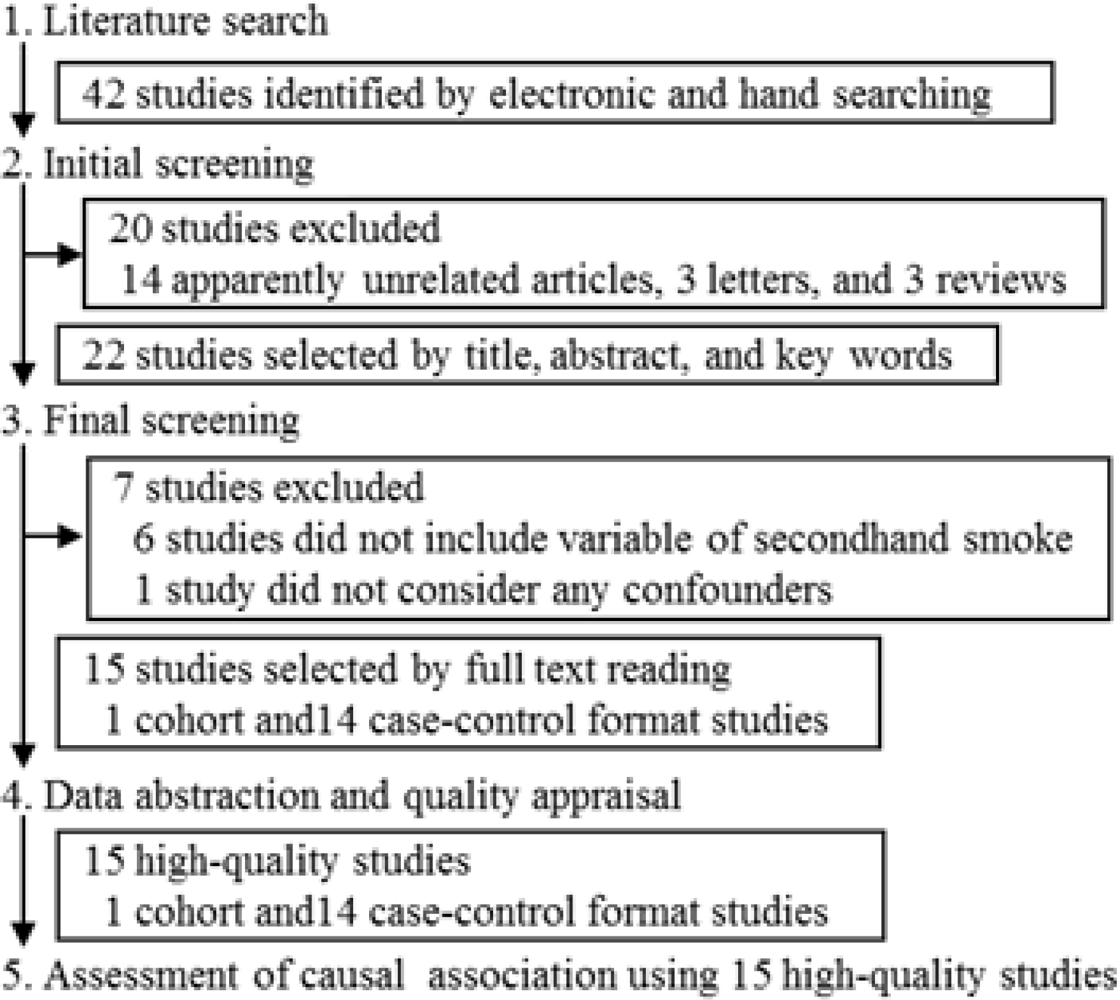
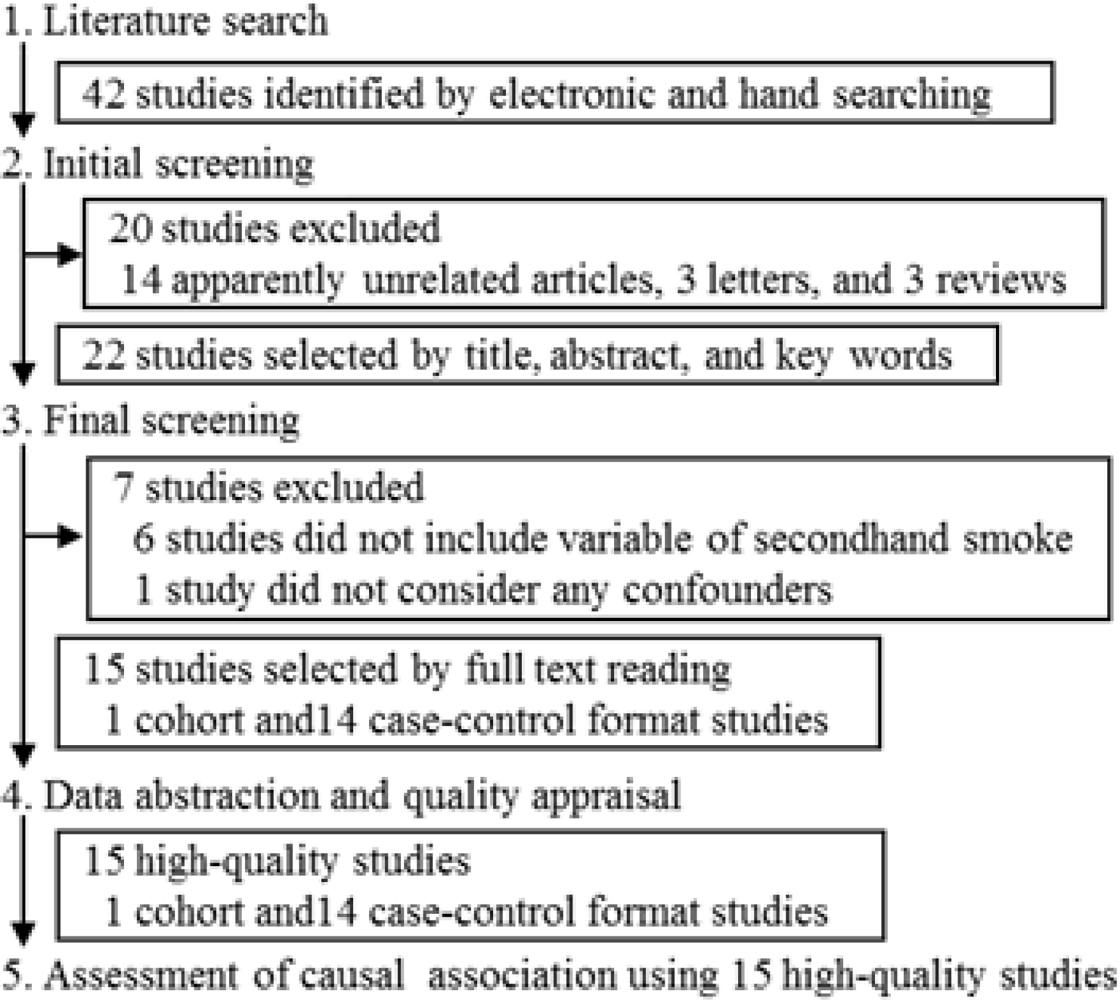
2.1. Literature Search
2.2. Outcome and Exposure
2.3. Eligibility Criteria and Searching Process
2.4. Methodological Quality Assessment
2.5. Data Abstraction
2.6. Evaluation of Causal Association
2.7. Evidence Synthesis of Consistency according to Study Quality
2.8. Evidence Synthesis of Association according to Study Design
- Convincing: Evidence is based on epidemiological studies showing consistent associations between exposure and disease, with little or no evidence to the contrary. The available evidence is based on a substantial number of studies including prospective observational studies, and where relevant, natural experiments of sufficient size, duration, and quality showing consistent effects.
- Probable: Evidence is based on epidemiological studies showing fairly consistent associations between exposure and disease, but there are perceived shortcomings in the available evidence or some evidence to the contrary, precluding a more definite judgment. Shortcomings in the evidence may be any of the following: insufficient duration of natural experiment (or studies), insufficient experiments (or studies) available, inadequate sample sizes, and incomplete follow-up.
- Possible: Evidence is mainly based on the findings of case-control and cohort formats studies. Insufficient numbers of natural experiments or observational studies are available. Additional natural experiments are required to support the tentative associations.
- Insufficient: Evidence is based on the findings of a few studies that are suggestive but insufficient to establish an association between exposure and disease. Limited or no evidence is available from natural experiments. Additional well-designed research is required to support the tentative associations.
3. Results and Discussion
3.1. Number of Studies
3.2. Characteristics of Studies
3.3. Quality of Studies
3.4. Strength of Association
3.5. Natural Experiment
3.6. Dose-Response Relationship
3.7. Evaluation of Evidence in Epidemiological Studies
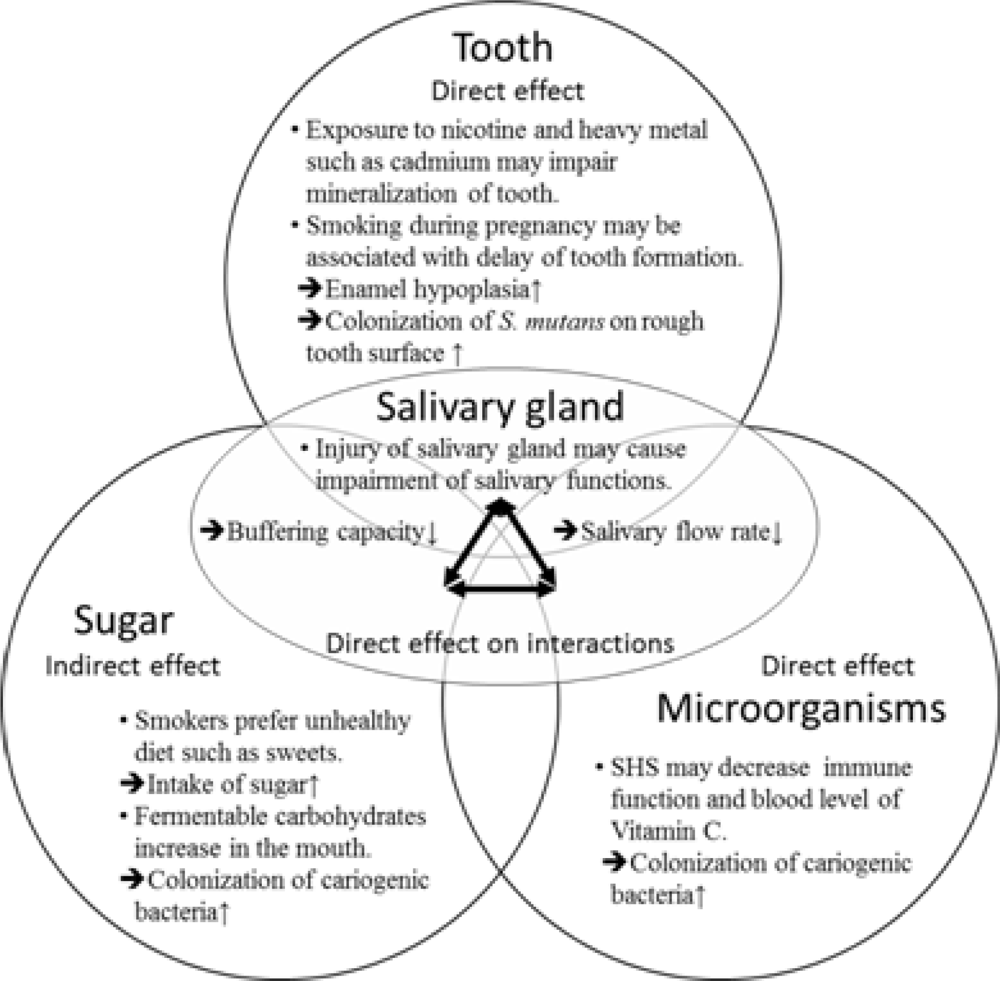
3.8. Biological Plausibility
4. Conclusions
Acknowledgments
- Conflict of Interest StatementNone declared.
References and Notes
- Hanioka, T; Ojima, M; Tanaka, K; Aoyama, H. Relationship between smoking status and tooth loss: Findings from national databases in Japan. J. Epidemiol 2007, 17, 125–132. [Google Scholar]
- Chambrone, L; Chambrone, D; Lima, LA; Chambrone, LA. Predictors of tooth loss during long-term periodontal maintenance: A systematic review of observational studies. J. Clin. Periodontol 2010, 37, 675–684. [Google Scholar]
- US Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2004. [Google Scholar]
- Ojima, M; Hanioka, T; Tanaka, K; Inoshita, E; Aoyama, H. Relationship between smoking status and periodontal conditions: Findings from national databases in Japan. J. Periodontal Res 2006, 41, 573–579. [Google Scholar]
- Labriola, A; Needleman, I; Moles, DR. Systematic review of the effect of smoking on nonsurgical periodontal therapy. Periodontol 2000 2005, 37, 124–137. [Google Scholar]
- Heasman, L; Stacey, F; Preshaw, PM; McCracken, GI; Hepburn, S; Heasman, PA. The effect of smoking on periodontal treatment response: A review of clinical evidence. J. Clin. Periodontol 2006, 33, 241–253. [Google Scholar]
- Straup, DF; Berlin, JA; Morton, SC; Olkin, I; Williamson, GD; Rennie, D; Moher, D; Becker, BJ; Sipe, TA; Thacker, SB; for the Meta-analysis of Observational Studies in Epidemiology (MOOSE) Group. Meta-analysis of observational studies in epidemiology. A proposal for reporting. J. Am. Med. Assoc 2000, 283, 2008–2012. [Google Scholar]
- Wells, G; Shea, B; O’Connell, D; Peterson, J; Welch, V; Losos, M; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed on 10 May 2011).
- Hill, AB. The environment and disease: Association or causation? Proc. Roy. Soc. Med 1965, 58, 295–300. [Google Scholar]
- Rosenthal, JA. Qualitative descriptors of strength of association and effect size. J. Soc. Serv. Res 1996, 21, 37–59. [Google Scholar]
- Van Tulder, M; Furlan, A; Bombardier, C; Bouter, L. Updated method guidelines for systematic reviews in the Cochrane collaboration back review group. Spine 2003, 28, 1290–1299. [Google Scholar]
- Nishida, C; Uauy, R; Kumanyika, S; Shetty, P. The Joint WHO/FAO Expert Consultation on diet, nutrition and the prevention of chronic diseases: Process, product and policy implications. Public Health Nutr 2004, 7, 245–250. [Google Scholar]
- Bolin, AK; Bolin, A; Jansson, L; Calltorp, J. Children’s dental health in Europe. Swed. Dent. J 1997, 21, 25–40. [Google Scholar]
- Williams, SA; Kwan, SY; Parsons, S. Parental smoking practices and caries experience in pre-school children. Caries Res 2000, 34, 117–122. [Google Scholar]
- Aligne, CA; Moss, ME; Auinger, P; Weitzman, M. Association of pediatric dental caries with passive smoking. J. Am. Med. Assoc 2003, 289, 1258–1264. [Google Scholar]
- Shenkin, JD; Broffitt, B; Levy, SM; Warren, JJ. The association between environmental tobacco smoke and primary tooth caries. J. Public Health Dent 2004, 64, 184–186. [Google Scholar]
- Shulman, JD. Is there an association between low birth weight and caries in the primary dentition? Caries Res 2005, 39, 161–167. [Google Scholar]
- Tanaka, K; Hanioka, T; Miyake, Y; Ojima, M; Aoyama, H. Association of smoking in household and dental caries in Japan. J. Public Health Dent 2006, 66, 279–281. [Google Scholar]
- Iida, H; Auinger, P; Billings, RJ; Weitzman, M. Association between infant breastfeeding and early childhood caries in the United States. Pediatrics 2007, 120, e944–e952. [Google Scholar]
- Ayo-Yusuf, OA; Reddy, PS; van Wyk, PJ; van den Borne, BW. Household smoking as a risk indicator for caries in adolescents’ permanent teeth. J. Adolesc. Health 2007, 41, 309–311. [Google Scholar]
- Hanioka, T; Nakamura, E; Ojima, M; Tanaka, K; Aoyama, H. Association of dental caries of 3-year-old children with smoking status of parents. Paediatr. Perinat. Epidemiol 2008, 22, 546–550. [Google Scholar]
- Aida, J; Ando, Y; Oosaka, M; Niimi, K; Morita, M. Contributions of social context to inequality in dental caries: A multilevel analysis of Japanese 3-year-old children. Community Dent. Oral Epidemiol 2008, 36, 149–156. [Google Scholar]
- Leroy, R; Hoppenbrouwers, K; Jara, A; Declerck, D. Parental smoking behavior and caries experience in preschool children. Community Dent. Oral Epidemiol 2008, 36, 249–257. [Google Scholar]
- Tanaka, K; Miyake, Y; Sasaki, S. The effect of maternal smoking during pregnancy and postnatal household smoking on dental caries in young children. J. Pediatr 2009, 155, 410–415. [Google Scholar]
- Julihn, A; Ekbom, A; Modéer, T. Maternal overweight and smoking: Prenatal risk factors for caries development in offspring during the teenage period. Eur. J. Epidemiol 2009, 24, 753–762. [Google Scholar]
- Tanaka, K; Miyake, Y; Arakawa, M; Sasaki, S; Ohya, Y. Household smoking and dental caries in schoolchildren: The Ryukyus Child Health Study. BMC Publ. Health 2010, 10, 335. [Google Scholar]
- Ditmyer, M; Dounis, G; Mobley, C; Schwarz, E. Case-control study of determinants for high and low dental caries prevalence in Nevada youth. BMC Oral Health 2010, 10, 24. [Google Scholar]
- Oliveira, AF; Chaves, AM; Rosenblatt, A. The influence of enamel defects on the development of early childhood caries in a population with low socioeconomic status: A longitudinal study. Caries Res 2006, 40, 296–302. [Google Scholar]
- Sisson, KL. Theoretical explanations for social inequalities in oral health. Community Dent. Oral Epidemiol 2007, 35, 81–88. [Google Scholar]
- Saad, AY. Postnatal effects of nicotine on incisor development of albino mouse. J. Oral. Pathol. Med 1990, 19, 426–429. [Google Scholar]
- Heikkeninen, T; Alvesalo, L; Osborne, RH; Pittiniemi, P. Maternal smoking and tooth formation in the foetus III. Thin mandibular incisors and delayed motor development at 1 year of age. Early Hum. Dev 1997, 47, 327–340. [Google Scholar]
- Chowdhury, IG; Bromage, TG. Effects of fetal exposure to nicotine on dental development of the laboratory rat. Anat. Rec 2000, 258, 397–405. [Google Scholar]
- Billings, RJ; Berkowitz, RJ; Watson, G. Teeth. Pediatrics 2004, 113, 1120–1127. [Google Scholar]
- Arora, M; Weuve, J; Schwartz, J; Wright, RO. Association of environmental cadmium exposure with pediatric dental caries. Environ. Health Perspect 2008, 116, 821–825. [Google Scholar]
- Kum-Nji, P; Meloy, L; Herrod, HG. Environmental tobacco smoke exposure: Prevalence and mechanisms of causation of infections in children. Pediatrics 2006, 117, 1745–1754. [Google Scholar]
- Crawley, HF; While, D. Parental smoking and the nutrient intake and food choice of British teenagers aged 16–17 years. J. Epidemiol. Community Health 1996, 50, 306–312. [Google Scholar]
- Strauss, RS. Environmental tobacco smoke and serum vitamin C levels in children. Pediatrics 2001, 107, 540–542. [Google Scholar]
- Preston, AM; Rodriguez, C; Rivera, CE. Plasma ascorbate in a population of children: Influence of age, gender, vitamin C intake BMI and smoke exposure. Puerto Rico Health Sci. J 2006, 25, 137–142. [Google Scholar]
- Väänänen, MK; Markkanen, HA; Tuovinen, VJ; Kulla, AM; Karinpää, AM; Luoma, H; Kumpusalo, EA. Dental caries and mutans streptococci in relation to plasma ascorbic acid. Scand. J. Dent. Res 1994, 102, 103–108. [Google Scholar]
- Ruottinen, S; Karjalainen, S; Pienihäkkinen, K; Lagström, H; Niinikoski, H; Salminen, M; Rönnemaad, T; Simellc, O. Sucrose intake since infancy and dental health in 10-year-old children. Caries Res 2004, 38, 142–148. [Google Scholar]
- Alm, A; Wendt, LK; Koch, G; Birkhed, D. Oral hygiene and parent related factors during early childhood in relation to approximal caries at 15 years of age. Caries Res 2008, 42, 28–36. [Google Scholar]
- Heintze, U. Secretion rate, buffer effect and number of lactobacilli and Streptococcus mutans of whole saliva of cigarette smokers and nonsmokers. Scand. J. Dent. Res 1984, 92, 294–301. [Google Scholar]
- Avşar, A; Darka, O; Topaloğlu, B; Bek, Y. Association of passive smoking with caries and related salivary biomarkers in young children. Arch. Oral Biol 2008, 53, 969–974. [Google Scholar]
- Lingström, P; Moynihan, P. Nutrition, saliva, and oral health. Nutrition 2003, 19, 567–569. [Google Scholar]
- De, S; Fenton, JE; Jones, AS; Clarke, RW. Passive smoking, allergic rhinitis and nasal obstruction in children. J. Laryngol. Otol 2005, 119, 955–957. [Google Scholar]
- Dahlström, A; Ebersjö, C; Lundell, B. Nicotine exposure in breastfed infants. Acta Paediatr 2004, 93, 810–816. [Google Scholar]
- Sakki, T; Knuuttila, M. Controlled study of the association of smoking with lactobacilli, mutans streptococci and yeasts in saliva. Eur. J. Oral Sci 1996, 104, 619–622. [Google Scholar]
- Alaluusua, S; Renkonen, OV. Streptococcus mutans establishment and dental caries experience in children from 2 to 4 years old. Scand. J. Dent. Res 1983, 91, 453–457. [Google Scholar]
- Wan, AK; Seow, WK; Purdie, DM; Bird, PS; Walsh, LJ; Tudehope, DI. A longitudinal study of Streptococcus mutans colonization in infants after tooth eruption. J. Dent. Res 2003, 82, 504–508. [Google Scholar]


{kind=link}
{kind=link}
| Study and focal factor | Setting | Statistical method and non-respondent rate | Funding |
|---|---|---|---|
| Bolin, 1997 [13], SES a | CS b data of school children in 8 European countries | Logistic RA c adjusted for country, type of household, number of siblings, parent’s age and social class; non-respondent rate of 4.6% | PHOs d, OHCs e |
| Williams, 2000 [14], SHS | CS b data from the UK NDNSf (1995) | Logistic RA c adjusted for age g, gender, social class g, household expenditure on confectionery g, and height; non-respondent rate of 23% | PHO d |
| Aligne, 2003 [15], SHS | CS b data from the NHANESh III (1988–1994) in the US | Logistic RA c, i adjusted for age, region of residence, race/ethnicity, time since last dental visit, poverty status and education level, non-respondent rate ND j | PHOs d |
| Shenkin, 2004 [16], SHS | CS b data from IFS k in 8 hospitals in the US | Logistic RA c adjusted for age, toothbrushing frequency, total infested fluoride, and SES b; non-respondent rate ND j | PHOs d |
| Shulman, 2005 [17], low birth weight | CS b data from the NHANESh III (1988–1994) in the US | Poisson RA c adjusted for age, race/ethnicity, income, history of breast-feeding, and bottle use after 19 months; non-respondent rate ND j | ND j |
| Tanaka, 2006 [18], SHS | CS b data from the NNSl, NSDD m (1999) in Japan | Logistic RA c adjusted for age, sex, region of residence, tooth brushing frequency, experience of topical fluoride application, and body mass index; non-respondent rate of 45.9% of participants of the NNS l | PHOs d |
| Iida, 2007 [19], infant breastfeeding | CS b data from the NHANES h (1999–2002) in the US | Logistic RA c and Poisson RA c adjusted for age, race/ethnicity, time since last dental visit, poverty status, history of breast feeding, birth weight, and maternal age; non-respondent rate ND j | PHOs d |
| Ayo-Yusuf, 2007 [20], SHS | CS b data in 21 high schools in South Africa | Logistic RA c adjusted for age, sex, ethnicity/race, family structure, sugar intake frequency, daily brushing frequency, time since dental visit, income of breadwinner, and current smoking status of the respondent; non-respondent rate ND j | PHOs d |
| Hanioka, 2008 [21], SHS | CS b data from records of health checkup at a public health facility in Japan | Logistic RA c adjusted for order of birth, types of main drink, frequency of daily intake of sugar-containing snacks, daily toothbrushing by parents, use of fluoridated toothpaste, and residential location; non-respondent rate of 15.9% | PHOs d |
| Aida, 2008 [22], social context to inequality | CS b data from records of health checkup at facilities in 39 municipalities in Japan | Multilevel RA c adjusted for age, order of birth, living with grandparents, toothbrushing-related habits, use of fluoride paste, taking sweet foods and drinks, occupation of household and termination of breast feeding, and 9 community-level variables; non-respondent rate of 20.1% for municipalities and 6.5% for participants of the participated municipalities | ND j |
| Leroy, 2008 [23], SHS | CS b data from the Smile for Life project in 4 distinct geographical areas in Flanders, Belgium | Logistic RA c adjusted for sex, home situation, dental plaque, age at start brushing, help with brushing, brushing frequency, use of nursing bottle, application of sweetener on a pacifier, cleaning a pacifier in the own mouth and in between meals/drinks, drinks/snacks at night, and educational level; non-respondent rate of 17.0% and 14.8% of children aged three and five years, respectively | OHCs e |
| Tanaka, 2009 [24], SHS | CS b data from the FCHSn in 7 public health centers in Japan | Binomial RA c with log link function adjusted for sex, toothbrushing frequency, use of fluoride, between-meal snack frequency, and paternal and maternal educational level; non-respondent rate of 74.5% | PHOs d |
| Julihn, 2009 [25], associated factors | Cohort data from the SMBRo and SNR p available at Statistics Sweden | Logistic RA c, g adjusted for child’s country of birth, sex, maternal age, parental country of birth, education level, marital status, mother receiving social welfare allowance, and the interaction term “unmarried mothers” and “mother receiving social welfare allowance;” non-respondent rate of 14% | PHOs d |
| Tanaka, 2010 [26], SHS | CS b data from school records in Okinawa, Japan | Binomial RA c with the log link function adjusted for age, sex, region of residence, toothbrushing frequency, use of fluoride, sugar intake, and paternal and maternal educational level; non-respondent rate of 24.4% | PHOs d |
| Ditmyer, 2010 [27], associated factors | CS b data in schools in Nevada | Logistic RA c adjusted for age, sex, race, living in an area with or without community water fluoridation, applied dental sealants, dental insurance status, and smoking habits; non-respondent rate ND j | PHOs d |
| Study | Selection | Comparability | Exposurea/Outcomeb | Total stars | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 c | 2 c | 3 c | 4 c | 5 d | 6 c | 7 c | 8 c | |||
| Bolin, 1997 [13] | * | * | * | * | * | * | * | * | 8 | |
| Williams, 2000 [14] | * | * | * | * | * | * | * | * | * | 9 |
| Aligne, 2003 [15] | * | * | * | * | * | * | * | * | 8 | |
| Shenkin, 2004 [16] | * | * | * | * | * | * | * | 7 | ||
| Shulman, 2005 [17] | * | * | * | * | * | * | * | 7 | ||
| Tanaka, 2006 [18] | * | * | * | * | * | * | * | 7 | ||
| Iida, 2007 [19] | * | * | * | * | * | * | * | 7 | ||
| Ayo-Yusuf, 2007 [20] | * | * | * | * | * | * | * | 7 | ||
| Hanioka, 2008 [21] | * | * | * | * | * | * | * | * | 8 | |
| Aida, 2008 [22] | * | * | * | * | * | * | * | * | 8 | |
| Leroy, 2008 [23] | * | * | * | * | * | * | * | * | * | 9 |
| Tanaka, 2009 [24] | * | * | * | * | * | * | * | 7 | ||
| Julihn, 2009 [25] | * | * | * | * | * | * | * | 7 | ||
| Tanaka, 2010 [26] | * | * | * | * | * | * | * | * | * | 9 |
| Ditmyer, 2010 [27] | * | * | * | * | * | * | * | 7 | ||
| Study | Age (n) | SHS | Dental caries | Effect size OR c (95% CI d) | ||
|---|---|---|---|---|---|---|
| Def a | % | Def b | % | |||
| Leroy, 2008 [23] | 3 (1,038) | HS | 30.9 | dmft | 6.7 | 1.98 (0.68, 5.76) |
| 5 (1,093) | HS | 30.2 | dmft | 30.2 | 3.36 (1.49, 7.58) | |
| Aida, 2008 [22] | 3 (3,086) | PS, MS | 20.4 | dmft | 31.3 e | 2.14 (1.59, 2.87) e |
| Hanioka, 2008 [21] | 3 (711) | PS, MS | 34.5 | dmft | 35.7 | 2.25 (1.51, 3.37) |
| Tanaka, 2009 [24] | 3 (2,015) | MSP only | 2.3 | dmft | 20.8 | 1.78 (1.16, 2.75) f |
| HS only | 31.8 | dmft | 20.8 | 1.26 (1.04, 1.53) f | ||
| Both | 10.7 | dmft | 20.8 | 1.40 (1.08, 1.81) f | ||
| Iida, 2007 [19] | 2–5 (1,563) | MSP | 14.5 | dfs | 27.2 | 1.68 (1.01, 2.79) |
| Williams, 2000 [14] | 3–4.5 (729) | MS | 33 | dmft | 25.2 | 1.54 (1.07, 2.21) |
| Shulman, 2005 [17] | 2–6 (4,207) | MSP | 5.2 | dfs count | NA | Not significant g |
| Bolin, 1997 [13] | 5 (1,423) | MS | 36.8 e | dmfs | 46.9 e | 1.52 (1.18, 1.95) e |
| Shenkin, 2004 [16] | 4–7 (637) | HS | 10.2 | dfs | 26.2 e | 3.38 (1.68, 6.79) |
| Aligne, 2003 [15] | 4–11 (3,531) | SCL | 55.4 | ds | 25.7 | 1.8 (1.2, 2.7) |
| Fs | 33.2 | 1.4 (1.1, 2.0) | ||||
| Tanaka, 2010 [26] | 6–15 (13,863) | HS h | 15.9 | dft | 78.5 | 1.06 (1.04, 1.08) f |
| Study | Age (n) | SHS | Dental caries | Effect size OR c (95% CI d) | ||
|---|---|---|---|---|---|---|
| Def a | % | Def b | % | |||
| Tanaka, 2006 [18] | 1–14 (925) | HS | 42.5 | dft, DFT | 61.2 | 1.26 (0.93, 1.69) |
| Aligne, 2003 [15] | 4–11 (2,930) | SCL | 54.2 | DS | 9.0 | 1.2 (0.8, 1.9) |
| FS | 18.9 | 0.9 (0.6, 1.3) | ||||
| Tanaka, 2010 [26] | 6–15 (20,253) | HSe | 16.5 | DFT | 55.1 | 1.03 (1.00, 1.06) f |
| 6–15 (20,703) | dft, DFT | 83.0 | 1.04 (1.03, 1.06) f | |||
| Bolin, 1997 [13] | 12 (1,265) | MS | 31.4 g | DMFS | 62.8 g | 1.40 (1.11, 1.78) g |
| Ayo-Yusuf, 2007 [20] | 14.6 h (1,873) | HS | 36.9 | DT i | 16.4 | 2.02 (1.22, 3.33) |
| Julihn, 2009 [25] | 13, 19 j (15,538) | MSP | 21.0 | ACI k | 38.6 | 1.33 (1.22, 1.44) |
| Ditmyer, 2010 [27] | 12–19 (4,169) | HS | 34.6 | DMFT | NA l | 1.42 (1.03, 1.53) |
| Study | Age | SHS a | Dental caries b | Effect size (95% CI d) | ||
|---|---|---|---|---|---|---|
| Def c | SHS exposure | |||||
| Former | Current | |||||
| Leroy, 2008 [23] | 3 | HS | dmft | OR | 1.71 (0.30, 9.65) | 1.98 (0.68, 5.76) |
| 5 | HS | dmft | OR | 0.55 (0.19, 1.65) | 3.36 (1.49, 7.58) | |
| Tanaka, 2009 [24] | 3 | MSP | dmft | PR | 1.21 (0.91, 1.59) | 1.43 (1.07, 1.91) |
| HS | dmft | PR | 1.23 (0.88, 1.71) | 1.25 (1.04, 1.50) | ||
| Tanaka, 2010 [26] | 6–15 | HS | dft | PR | 1.02 (0.99, 1.06) | 1.06 (1.04, 1.08) |
| HS | DFT | PR | 1.03 (1.00, 1.06) | 1.03 (1.00, 1.06) | ||
| Study | Age | SHS a/Dental caries b | Level of exposure/Effect size | |||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| Hanioka, | 3 | PS | None | Father only | Both parents | |
| 2008 [21] | dmft | 1.00 c | 1.52 (1.01, 2.30) c | 2.25 (1.51, 3.37) c | ||
| Aida, | 3 | PS | None | Either parent | Both parents | |
| 2008 [22] | dmft | 1.00 c | 1.40 (1.15, 1.71) c, d | 2.14 (1.59, 2.87) c, d | ||
| Tanaka, | 3 | MS | None | 0.1–17.9 e | 18.0– e | |
| 2009 [24] | dmft | 1.00 f | 1.16 (0.93, 1.44) f | 1.33 (1.09, 1.63) f | ||
| Aligne, | 4–11 | SCL | <0.05 g | 0.05–<0.2 g | 0.2–1.0 g | >1.0 g |
| 2003 [15] | ds | 1.0 c | 1.3 (0.8, 2.3) c | 2.2 (1.3, 3.6) c | 2.3 (1.4, 3.9) c | |
| fs | 1.0 c | 1.1 (0.7, 1.8) c | 1.6 (1.0, 2.4) c | 1.5 (1.0, 2.3) c | ||
| Tanaka, | 6–15 | HS | None | 0.1–2.9 h | 3.0–6.9 h | ≥7.0 h |
| 2010 [26] | dft | 1.00 e | 1.04 (1.00, 1.09) f | 1.12 (1.07, 1.17) f | 1.11 (1.06, 1.16) f | |
| DFT | 1.00 e | 1.12 (1.06, 1.20) e | 1.18 (1.12, 1.26) e | 1.17 (1.11, 1.24) e | ||
| Tooth type | Element | Description for consistency (number of study) | Evidence synthesis according to study quality | Perceived shortcoming | Evidence synthesis |
|---|---|---|---|---|---|
| Deciduous tooth | Strength of association | Strong (2), moderate (5), weak and moderate (2), weak (1), no association (1) | Moderate to strong evidence for weak to moderate association | There was no control group in current smokers in natural experiment. | Possible evidence |
| Natural experiment | Smaller effect size and no association (3) in previous exposure group | Strong evidence for natural experiment | Natural experiment and dose-response relationship were reported from two countries. Cohort study was not conducted. | ||
| Dose-response relationship | Obvious relationship between level of exposure and the effect size (5) | Strong evidence for dose-response relationship. | |||
| Permanent tooth | Strength of association | Moderate (1), weak (5 a), and no association (2) | Moderate evidence for weak association | Only one study reported results of natural experiment and dose-response relationship. | Insufficient evidence |
| Natural experiment | Effect size was similar in previous and current exposure groups (1) | Limited evidence for natural experiment | |||
| Dose-response relationship | Relationship between level of exposure and the effect size was not clear (1) | Limited evidence for natural experiment | |||
© 2011 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Hanioka, T.; Ojima, M.; Tanaka, K.; Yamamoto, M. Does Secondhand Smoke Affect the Development of Dental Caries in Children? A Systematic Review. Int. J. Environ. Res. Public Health 2011, 8, 1503-1519. https://doi.org/10.3390/ijerph8051503
Hanioka T, Ojima M, Tanaka K, Yamamoto M. Does Secondhand Smoke Affect the Development of Dental Caries in Children? A Systematic Review. International Journal of Environmental Research and Public Health. 2011; 8(5):1503-1519. https://doi.org/10.3390/ijerph8051503
Chicago/Turabian StyleHanioka, Takashi, Miki Ojima, Keiko Tanaka, and Mito Yamamoto. 2011. "Does Secondhand Smoke Affect the Development of Dental Caries in Children? A Systematic Review" International Journal of Environmental Research and Public Health 8, no. 5: 1503-1519. https://doi.org/10.3390/ijerph8051503
APA StyleHanioka, T., Ojima, M., Tanaka, K., & Yamamoto, M. (2011). Does Secondhand Smoke Affect the Development of Dental Caries in Children? A Systematic Review. International Journal of Environmental Research and Public Health, 8(5), 1503-1519. https://doi.org/10.3390/ijerph8051503