The Drinker’s Effect on the Social Environment: A Conceptual Framework for Studying Alcohol’s Harm to Others

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Behind the Neglect of Alcohol’s Harm to Others
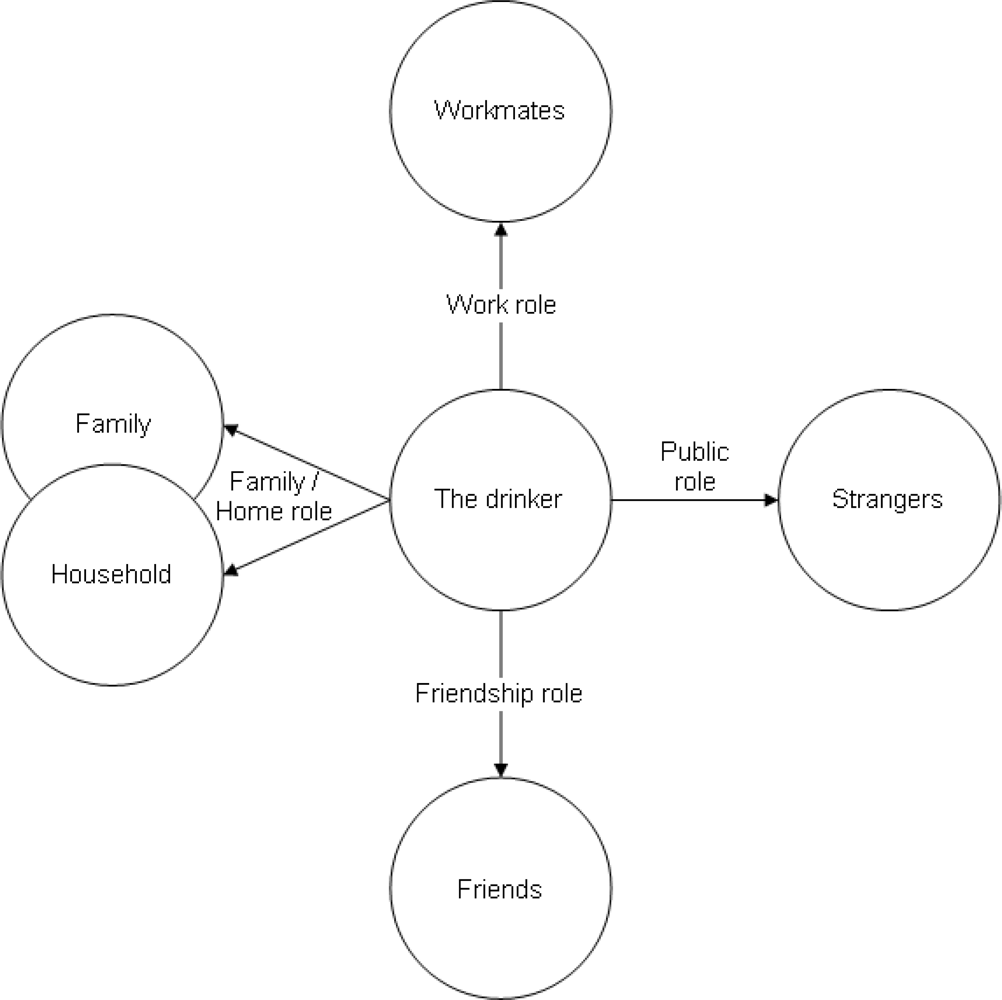
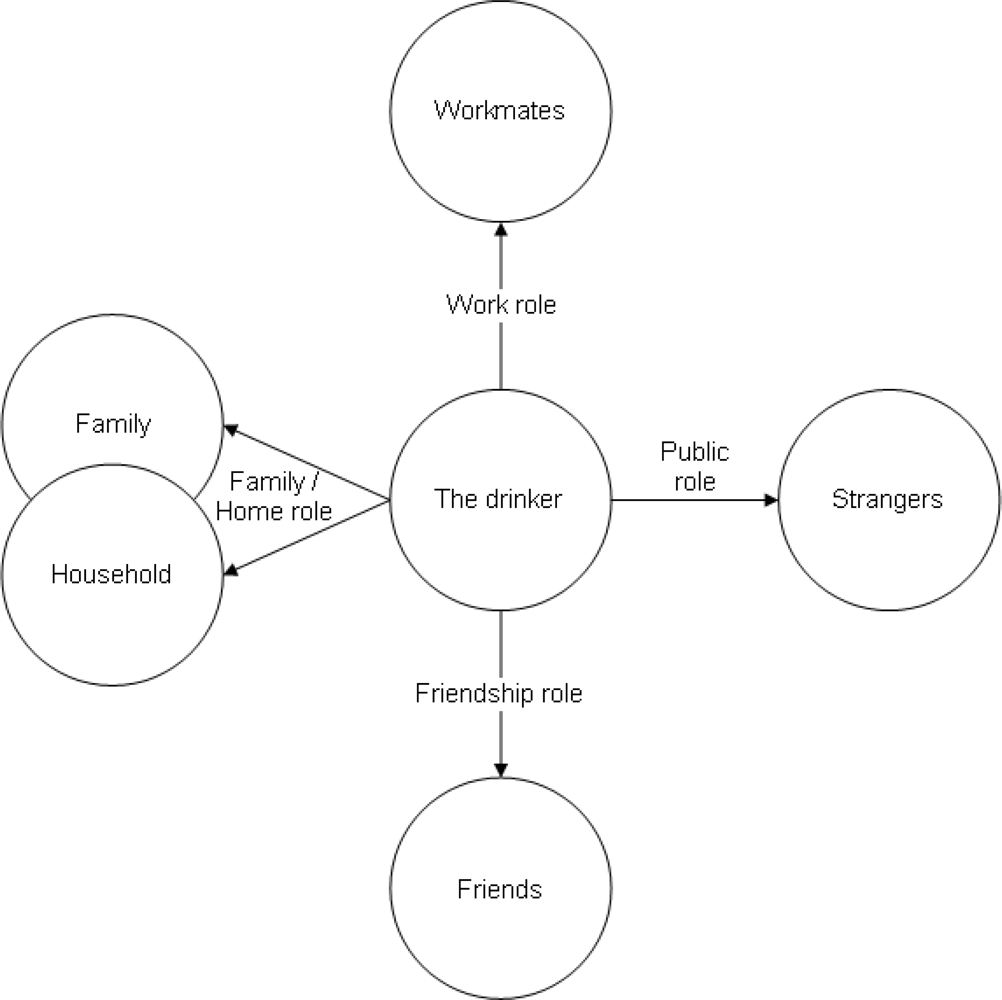
3. Conceptualizing Alcohol’s Harm to Others
4. Relevant Comprehensive Approaches to Measuring Harms from Drinking
4.1. Survey Research Traditions
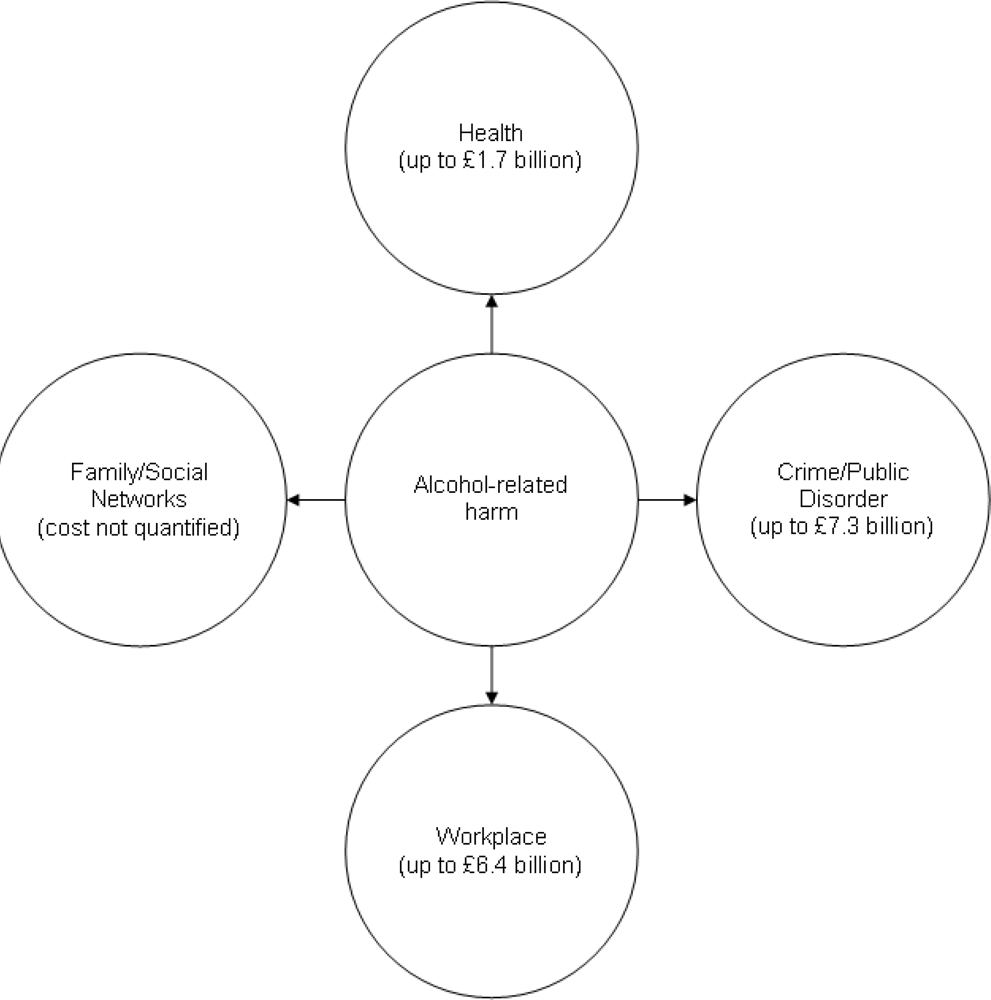
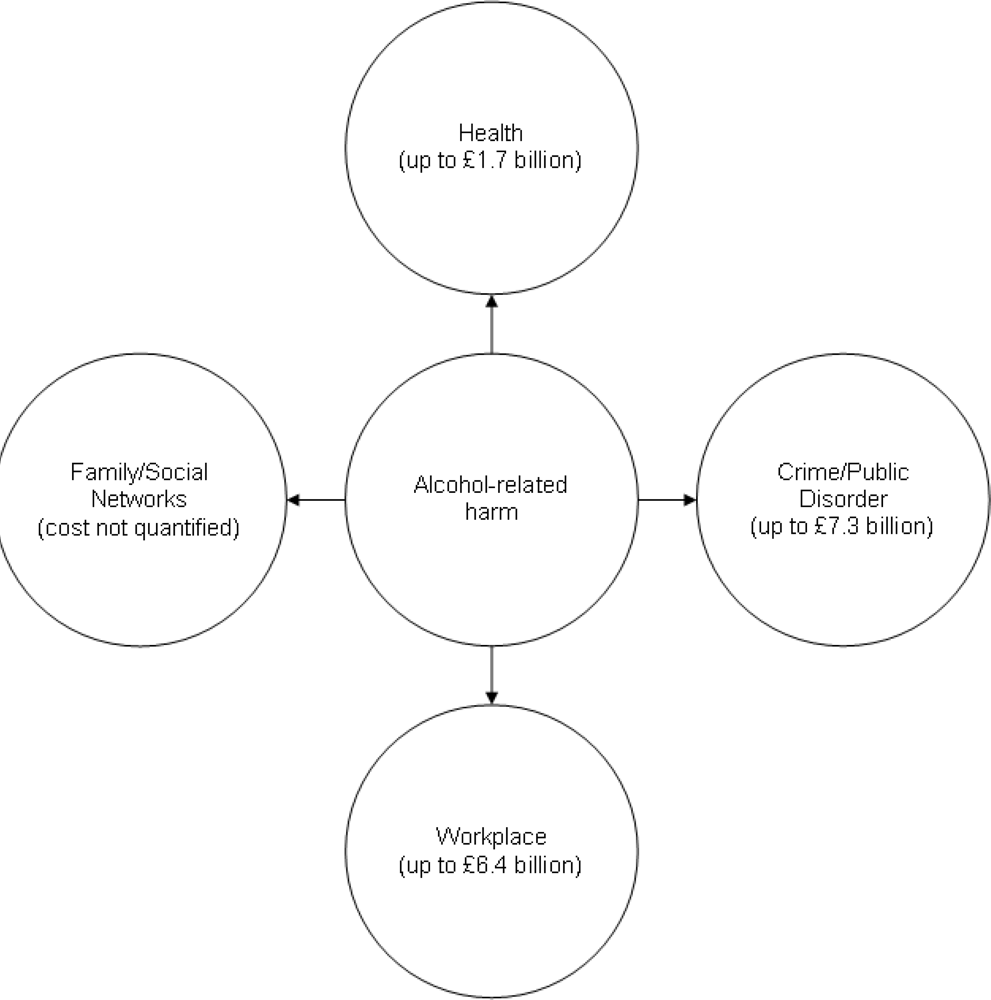
4.2. The Cost of Alcohol Tradition
5. Approaches to Studying Alcohol’s Harm to Others
- The fact of an occurrence, for instance, a death or a traffic crash, can be viewed as an indicator of harm for the person affected. Thus a count of deaths, or of years of life lost (YLLs) short of a full life, is one kind of metric of harm to the individual.
- Particularly in population survey data, the respondent’s report of an adverse occurrence—for example, something being broken or damaged that mattered to the respondent—is often used as an indication of harm to the respondent.
- The frequency and intensity of such harms can also be indicated by the respondent, for instance by asking how often it happened, and whether the adverse effect was a lot or a little.
- Another measure used of the degree of harm to the respondent can be in terms of the respondent’s report on items indicating a degree of wellbeing or of health disability (e.g., impact on health related quality of life, HRQoL), which can then be compared with the reports of others similarly situated.
- For harms where it is possible, a monetary measure of the amount of harm can be calculated. This can be measured in various frames of reference, depending on the harm: e.g., in terms of the wages which could have been earned in time which was lost, in terms of the loss of monetary value of something broken or damaged, in terms of the conventional monetary value assigned by econometric studies to an increment of health disability.
- In data drawn from population surveys, alcohol’s causal involvement in the harm is commonly measured directly by the attribution of the person affected. Thus a question like “How many times in the last 12 months were you physically hurt by them because of their drinking?” has built into the question an attribution (in a “yes” response) of the occurrence to the other’s drinking.
- For some harms, the alcohol attribution is commonly made by the personnel of the health or social response system—for instance, a child protection worker coding that the parent’s drinking is involved in a child endangerment case. Sometimes the attribution is built into the system’s categorization of the case—for instance, a Foetal Alcohol Syndrome diagnosis, or a “drunk and disorderly” arrest.
- For harms measured by the health system without any routine coding of alcohol involvement, meta-analyses of special studies have often relied on to measure an “alcohol attributable fraction” (AAF). AAFs are usually concerned with the drinking of the person with the illness, but it is possible to develop analogous fractions concerning the drinking of another, for instance, in estimating the proportion of child traffic deaths where another’s drinking played a causal role.
- In studying the effects of others’ drinking on personal wellbeing and health disability, the alcohol attribution can be imputed from differences in wellbeing or disability scores between those similarly situated who are affected by heavy drinkers and those who are not.
6. Getting the Right Focus in a Binocular View
7. Conclusion
Acknowledgments
References
- Rehm, J; Baliunas, D; Borges, GLG; Graham, K; Irving, H; Kehoe, T; Parry, CD; Patra, J; Popova, S; Poznyak, V; Roerecke, M; Room, R; Samokhvalov, AV; Taylor, B. The relation between different dimensions of alcohol consumption and burden of disease—an overview. Addiction 2010, in press. [Google Scholar]
- Room, R. Alcohol consumption and social harm—conceptual issues and historical perspectives. Contemp. Drug Probl 1996, 23, 373. [Google Scholar]
- Levine, HG. The “good creature of God” and demon rum: Colonial American and 19th century ideas about alcohol, crime and accidents. In Alcohol and Disinhibition: Nature and Meaning of the Link; Room, C, Ed.; NIAAA Research Monograph, USGPO: Washington, DC, USA, 1983; pp. 111–161. [Google Scholar]
- Room, R; Rossow, I. The share of violence attributable to drinking. J. Subst. Use 2001, 6, 218–228. [Google Scholar]
- Herd, D. Ideology, history and changing models of liver cirrhosis epidemiology. Brit. J. Addict 1992, 87, 1113–1126. [Google Scholar]
- Wikipedia. Griswold vs. Connecticut. Available online: http://en.wikipedia.org/wiki/Griswold_v_Connecticut/ (accessed on 31 December 2009).
- Gusfield, J. The Culture of Public Problems: Drinking-Driving and the Symbolic Order; University of Chicago Press: Chicago, IL, USA, 1981. [Google Scholar]
- Babor, T; Caetano, R; Casswell, S; Edwards, G; Giesbrecht, N; Graham, K; Grube, J; Gruenewald, P; Hill, L; Holder, H; Homel, R; Österberg, E; Rehm, J; Room, R; Rossow, I. Alcohol: No Ordninary Commodity—Research and Public Policy; Oxford University Press: Oxford, UK, 2003. [Google Scholar]
- Bard, M; Zacker, J. Assaultiveness and alcohol use in family disputes: Police perceptions. Criminology 1974, 12, 281–293. [Google Scholar]
- Mapping the Social Consequences of Alcohol Consumption; Klingemann, H; Gmel, G (Eds.) Kluwer Academic Publishers: Dordrecht, The Netherlands, 2001.
- Goffman, E. The Presentation of Self in Everyday Life; Anchor Books: New York, NY, USA, 1959. [Google Scholar]
- Sackett, L. Liquor and the law: Wiluna, Western Australia. In Aborigines and Change: Australia in the '70s; Berndt, RM, Ed.; Australian Institute of Aboriginal Studies: Canberra, Australia, 1977; pp. 90–99. [Google Scholar]
- Room, R; Jernigan, D; Carlini Cotrim, B; Gureje, O; Mäkelä, K; Marshall, M; Medina-Mora, ME; Monteiro, M; Parry, C; Partanen, J; Riley, L; Saxena, S. Alcohol in Developing Societies: A Public Health Approach; Finnish Foundation for Alcohol Studies: Helsinki, Finland, 2002. [Google Scholar]
- Cahalan, D; Room, R. Problem Drinking among American Men; Rutgers Center of Alcohol Studies: New Brunswick, NJ, USA, 1974. [Google Scholar]
- Room, R. Concepts and items in measuring social harm from drinking. J. Subst. Abuse 2000, 12, 93–111. [Google Scholar]
- Holmila, M; Mustonen, H; Rannik, E. Alcohol use and its control in Finnish and Soviet marriages. Brit. J. Addict 1990, 85, 509–520. [Google Scholar]
- Room, R. The USA general population’s experiences of responding to alcohol problems. Brit. J. Addict 1989, 84, 1291–1304. [Google Scholar]
- Joosten, J; Knibbe, RA; Derickx, M; Morin, D; Hradilova Selin, K; Holmila, M. Criticism of drinking as informal social control: A study in 18 countries. Contemp. Drug Probl 2009, 36, 85–109. [Google Scholar]
- Room, R; Bondy, S; Ferris, J. Determinants of suggestions for alcohol treatment. Addiction 1996, 91, 643–655. [Google Scholar]
- Wells, S; Graham, K. Verbal versus physical victimisation from other people’s drinking: How do gender, age and their interactions with drinking patterns affect vulnerability? J. Stud. Alcohol Drugs 2007, 68, 582–586. [Google Scholar]
- Greenfield, TK; Ye, Y; Kerr, W; Bond, J; Rehm, J; Giesbrecht, N. Externalities from alcohol consumption in the 2005 US National Alcohol Survey: implications for policy. Int. J. Environ. Res. Public Health 2009, 6, 3205–3224. [Google Scholar]
- Eliany, M; Giesbrecht, N; Belson, M; Wellman, B; Wortley, S. Alcohol and Other Drug Use by Canadians: A National Alcohol and Other Drugs Survey 1989: Technical Report; Health Canada: Ottawa, Canada, 1992. [Google Scholar]
- Mäkelä, P; Fonager, K; Hibell, B; Nordlund, S; Sabroe, S; Simpura, J. Drinking Habits in the Nordic Countries; National Institute for Alcohol and Drug Research: Oslo, Norway, 1999. [Google Scholar]
- Fillmore, K. The social victims of drinking. Brit. J. Addict 1985, 80, 307–314. [Google Scholar]
- Wilkinson, C; Laslett, A-M; Ferris, J; Livingston, M; Mugavin, J; Room, R. The Range and Magnitude of Alcohol’s Harm to Others: Study Design, Data Collection Procedures and Measurement; AER Centre for Alcohol Policy Research, Turning Point Alcohol & Drug Centre: Fitzroy, Australia, 2009. [Google Scholar]
- Rice, DP; Hodgson, TA; Kopstein, AN. The economic costs of illness: a replication and update. Health Care Finance Rev 1985, 7, 61–80. [Google Scholar]
- Single, E; Collins, D; Easton, B; Harwood, H; Lapsley, H; Kopp, P; Wilson, E. International Guidelines for Estimating the Costs of Substance Abuse, 2nd ed; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Collins, DJ; Lapsley, HM. The Costs of Tobacco, Alcohol and Illicit Drug Abuse to Australian Society in 2004/05; Australian Department of Health and Ageing: Canberra, Australia, 2008. [Google Scholar]
- Heien, DM; Pittman, DJ. The external costs of alcohol abuse. J. Stud. Alcohol 1992, 54, 302–307. [Google Scholar]
- Manning, WG; Keller, EB; Newhouse, JP; Sloss, EM; Wasserman, J. The taxes of sin: Do smokers and drinkers pay their way? JAMA 1989, 261, 1604–1609. [Google Scholar]
- Johansson, P; Jarl, J; Eriksson, A; Eriksson, M; Gerdtham, U-G; Hemström, Ö; Hradilova Selin, K; Lenke, L; Ramstedt, M; Room, R. The Social Cost of Alcohol in Sweden 2002. (No. 36); SoRAD, Stockholm University: Stockholm, Sweden, 2006. Available online: http://www2.sorad.su.se/publications.php?Id=469 (accessed on 31 December 2009).
- Gutjahr, E; Gmel, G. The social costs of alcohol consumption. In Mapping the Social Consequences of Alcohol Consumption; Klingemann, H, Gmel, G, Eds.; Kluwer: Dordrecht, The Netherlands, 2002; pp. 133–143. [Google Scholar]
- UK Prime Minister’s Strategy Unit. Interim Analytical Report, Strategy Unit Alcohol Harm Reduction Project; Prime Minister’s Office: London, UK, 2004. [Google Scholar]
- Room, R. Measurements and distribution of drinking patterns and problems in general populations. In Alcohol-Related Disabilities; Edwards, G, Gross, MM, Keller, M, Moser, J, Room, R, Eds.; World Health Organisation: Geneva, Switzerland, 1977; pp. 61–87. [Google Scholar]
- Storbjörk, J; Room, R. The two worlds of alcohol problems: Who is in treatment and who is not? Addiction Res. Theor 2008, 16, 67–84. [Google Scholar]
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Room, R.; Ferris, J.; Laslett, A.-M.; Livingston, M.; Mugavin, J.; Wilkinson, C. The Drinker’s Effect on the Social Environment: A Conceptual Framework for Studying Alcohol’s Harm to Others. Int. J. Environ. Res. Public Health 2010, 7, 1855-1871. https://doi.org/10.3390/ijerph7041855
Room R, Ferris J, Laslett A-M, Livingston M, Mugavin J, Wilkinson C. The Drinker’s Effect on the Social Environment: A Conceptual Framework for Studying Alcohol’s Harm to Others. International Journal of Environmental Research and Public Health. 2010; 7(4):1855-1871. https://doi.org/10.3390/ijerph7041855
Chicago/Turabian StyleRoom, Robin, Jason Ferris, Anne-Marie Laslett, Michael Livingston, Janette Mugavin, and Claire Wilkinson. 2010. "The Drinker’s Effect on the Social Environment: A Conceptual Framework for Studying Alcohol’s Harm to Others" International Journal of Environmental Research and Public Health 7, no. 4: 1855-1871. https://doi.org/10.3390/ijerph7041855