1. Introduction
The Australian government has an increasing focus on public health approaches to the health of the community with the objective of providing ‘more preventive care for older Australians’, and ‘improving co-ordination of care for people with chronic conditions and complex care needs’ [
1]. The Medicare Chronic Disease Management (CDM) Allied Health Program was introduced nationwide in 2004 to aid this objective [
2].
As in other countries, an aging population with increasing incidence of chronic diseases such as cardiac disease, diabetes, or hypertension, led to this policy change. In Australia, chronic medical conditions are responsible for over 80% of the overall burden of disease and injury [
3]. This adds to already high health care costs and raises a dilemma in relation to public health policy: how to reverse this trend?
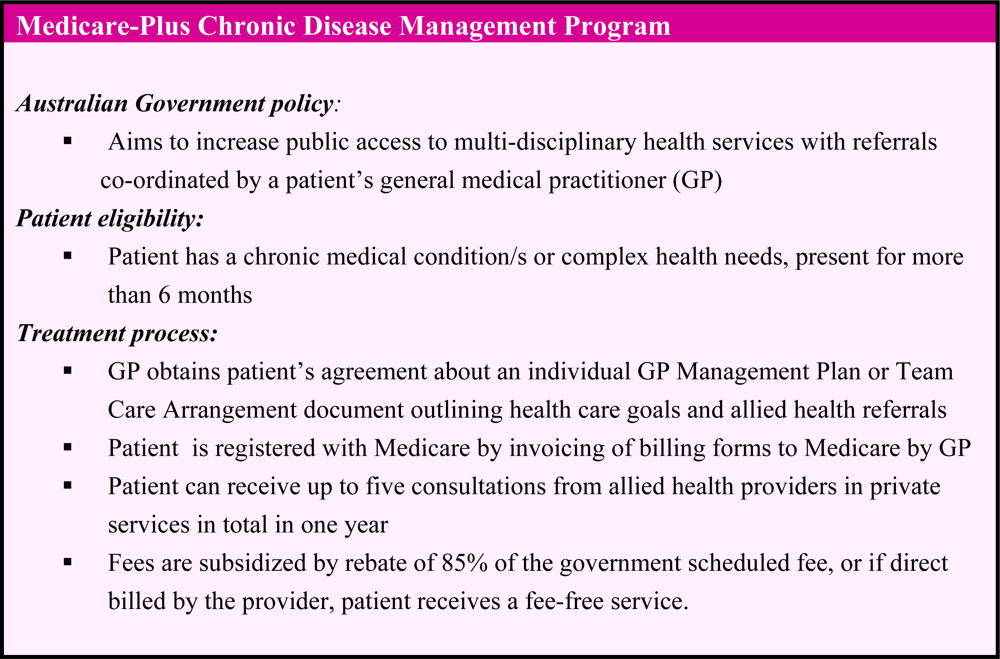
The Enhanced Primary Care (EPC) program that was commenced in 1999 aimed to engage general medical practitioners (GPs) in the coordination of the medical care of their patients using subsidized medical services. These are funded under the national taxation-based health insurance: Medicare. The Medicare-Plus Chronic Disease Management (CDM) Allied Health Program aims to positively impact the health of patients with chronic disease or complex health needs [
2]. This allows eligible patients access to various allied health professional services in private clinics at subsidized fee rates. The program supplements public services in hospitals, hospital clinics and community-based health and medical services such as multidisciplinary community health services. A summary of the program is given in
Figure 1 and further details are described below.
In order to be eligible for access to Medicare CDM, a patient’s GP is required to prepare an individual written care plan. This is a GP Management Plan (GPMP) or a Team Care Arrangement (TCA). These processes are complex: details of GP, dietetic and other allied health services funded under Medicare are given on the website of Medicare Australia (
http://www.medicareaustralia.org). For a GPMP, a GP collaborates with a patient; assesses the patient, agrees their goals for health improvement, identifies actions to be taken by patient, identifies treatment/ongoing services to be provided, and documents the plan. A TCA requires GPs to coordinate team-based care for a patient with a chronic condition and complex, multi-disciplinary care needs and this should involve at least three professionals in planning [
2].
Patients agree to the care plan and the suggested allied health consultations and receive a copy of their plan with the treatment goals. Allied health interventions aim to engage patients in learning, including of new skills and this concurs with chronic disease management principles that show that increase in the self-management skills of patients is associated with improvements in their health outcomes [
4]. Each eligible patient is entitled to up to five subsidized consultations from approved allied health services in private clinics each year [
2]. In the case of a patient with diabetes, this potentially includes, diabetes educator, dietitian and/or podiatrist so that these consultations must be shared between provider professions. Patients have renewed entitlements annually.
As chronic disease risk is commonly related to dietary choices [
3,
5], dietetics referrals may relate to diagnoses such as diabetes, or a cardiac or other condition. A GP or practice nurse in consultation with the patient sets dietary goals for patients to achieve with a dietitian’s counselling assistance. Each consultation must be at least 20 minutes duration face to face with a practitioner, and the patient can receive a rebate of 85% of the scheduled fee when the scheduled fee is charged. The scheduled fee for both initial and follow-up dietetics consultations was AU$58.85 at November 2009, and the rebated remuneration for providers per visit AU$50.05 [
6].
Dietetics is the third most utilized of 14 allied heath provider groups, including physiotherapy, podiatry/chiropody, chiropractic, speech pathology, exercise physiology, diabetes education [
7]. The number of dietetics consultations conducted nationally has been rising every year [
8]. This program offers substantial business opportunity to private practices to increase their workloads in clinic environments which include multidisciplinary practices with a GP or without a GP, sole practices, or group practices comprising a group of dietitians [
8].
Published evaluation of Medicare CDM policy implementation is lacking and no data is available about the health outcomes of chronic disease patients. However, several studies have explored providers’ perceptions of the program’s impact. Foster
et al. reported results of a qualitative study of five professions in Queensland (exercise physiologists, occupational therapists, physiotherapists, social workers and speech pathologists) in 2006 [
9]. They reported care provision was affected by the small remuneration paid. Practitioners who were constrained by the prescribed consultation or repeat visit limits condensed their time management in caring for a patient, resulting in an ‘abbreviated care’ model. There was a need for resolution of some issues, including health practitioners’ obligation to provide an adequate professional service whilst ensuring the financial viability of the business practice. This concurred with the views of 15 dietetics providers who were interviewed in the first twelve months of the program in 2005. The initial, or first, consultation time they allowed a patient (which they perceived as limited by the set remuneration) was largely inadequate time to help patients to achieve their dietary goals [
10].
A national survey of Australian dietitians in private practice (n = 356; 47%) by the author in 2007 reported a need to review a number of areas of the Medicare-CDM policy to prompt an increase in dietitians’ endorsement of the program [
11]. Both the funded initial consultation time and the available consultation frequency were, in the main, seen as inadequate to allow dietitians to assist patients to achieve the dietary goals set by GPs. Dietitians needed more time with a patient to assess, educate, set dietary goals and to monitor progress- as confirmed in dietetics practice principles for chronic disease management [
12]. Income from the Medicare fee rebate was said to be less than their usual fee scale.
The quantitative results of the survey of dietitians were reported earlier [
11]. Due to the Medicare policy constraints, dietitians applied various consultation strategies in developing their service for Medicare- eligible patients. These adaptations of practice have broad implications for both patients and practitioners in the delivery of CDM dietetics services. This paper aims to explore the care models of Medicare CDM service provision that dietitians adopt in order to comply with the policy guidelines and yet maintain their business plan and the economic viability of private clinics. A qualitative approach will be used.
2. Methods
Interview technique was utilized as the primary data source [
13]. A purposive sample of 20 dietitians who were Medicare providers was selected from those who consented to be interviewed when responding to the national survey mentioned above; nine were then interviewed. Sample selection was made on the basis of capturing the variation apparent in practice environments [
14]. This was firstly, sampling both low use Medicare providers of <10 referrals per month and high use (>26 referrals per month), and then the clinic category in which they were employed (sole practice or group practice) and providers in the major dietetic provider states (NSW, Victoria, Queensland, South Australia, West Australia). Second, both those who were satisfied with the Medicare program and those who were not satisfied were purposely selected. Each interview time was pre-arranged and if a dietitian was not readily available for interview within the next week, then the next on the list was contacted for interview.
A single experienced researcher (RC) interviewed the dietitians by telephone over 25 to 40 minutes each in 2008 using a semi-structured interview technique. An interview schedule built on data from the national survey was used to initiate discussion. This asked about matters such as the time given to consultations, perceptions of patients’ needs and detail of reporting methods. Questions were intended to clarify responses or comments these same individuals had made in their returned surveys and/or to further focus the themes identified in the overall survey results. Each participant had already responded to a questionnaire and given their identity and practice details so previous responses were summarized for the interviewer for each participant on a running sheet prior to interview. Some questions were leading in order to gain further perspectives on overall responses. Examples of questions are given in
Table 1.
Subsequent questions aimed to further clarify an issue pertaining the particular category of practice or the management process used. For example, a dietitian co-located with a GP might manage referrals, billing and communications quite differently to those in sole practices. Furthermore, as the interview process was iterative, questions were altered to probe for more detail depending upon the responses of a previous interviewee, as expected according to in-depth interviewing technique [
13].
The interviews were audio-recorded with each participant’s consent. Interviews were subsequently ceased after analysis of nine interviews as no new topics were raised and it was thought that a ‘saturation’ of topics was evident [
13]. In part, this was due to questionnaire data having already provided much detail of customary practice, including narratives given in the invited open-ended comments. The audiotapes were studied with notation of the narrative themes to develop a matrix of various responses and this analysis continued simultaneously with interviewing. A constant comparative technique was used to compare similarities or differences between the views of dietitians from different employment environments, practices, and states of employment [
15]. The findings were subsequently compared with themes from the questionnaire results, including those from open-ended comments- in a process of triangulation [
13].
The study was approved by the human ethics committee of the sponsoring university. No financial or other inducement was offered to participants for their contribution to the study.
3. Findings
The findings from analysis of the interview data are presented in order to build a logical chain of evidence about practice conditions. Some quotations from the narratives were selected and are presented as indicative of the views of one sector of dietetics practice.
3.1. Participant Characteristics
The nine female dietitians interviewed were employed in a wide range of clinic businesses including (i) sole practice, (ii) multi-professional allied health practice (iii) group dietetics practice (iv) group practice with GP, in both metropolitan and country regions. This encompassed the states with the largest number of dietetics Medicare transactions: NSW, Victoria, Queensland, South Australia, and West Australia. Several were located with a GP referrer in the same building, and all received their CDM referrals by letter. Their hours of work in private practice ranged from seven hours per week to full-time. They first qualified for dietetics between 1972 and 2006, although most were experienced with at least five years of experience. Some were satisfied with the Medicare CDM program and some were dissatisfied, and thus were able to give diverse views about the impact of the program.
3.2. Initial Consultation Strategies
The Medicare fee rebate was thought by all to fund a short consultation of 20–30 minutes, given the cost of extra time for writing reports to doctors and cost of office overheads and administration. Four main strategies were applied to first consultation arrangements in an endeavor to meet CDM patients’ needs for nutrition education whilst also complying with the policy guidelines and their business principles. There was no overall pattern of consultation management strategy found by any particular employment environment: all differed in their decisions. No major new themes were identified, as each dietitian voiced issues that were apparent in the earlier survey, but through the interview data, enabled more detailed perspectives and filled in information gaps.
Much of the interview discussion applied to a first consultation, which was of principal concern to all the dietitians due the high frequency of occurrence of these referrals and the perceived high degree of difficulty of the counselling for some patients. Dietitians might see a patient once or twice for a consultation. They made a choice of these initial consultation arrangements:
to limit all consultations to 20–30 minutes
to deliver a longer initial consultation of 45 to 60 minutes and charge patients a fee gap
to deliver an initial consultation longer than 20–30 minutes at no extra fee
to choose not to accept (or to accept few) CDM patients.
The second option involving an increase in fees was the most common, thus adding to a patient’s out-of-pocket costs. Interviews provided detailed information about how the consultations were managed.
(a) The 20-minute consultation
Several dietitians had experience of conducting short initial consultations, depending on the clinic environment, although this was much more common for review consultations. One dietitian routinely scheduled 20-minute initial and review consultations for all Medicare CDM patients, working within the current national fee scale for bulk-billed consultations. This fulltime employee in a group dietetic practice was a high use provider, seeing 50–100 CDM patients per month. Receptionists handled administration and the bulk- billing of invoices to Medicare, which meant that patients were not required to pay any fee contribution for their consultation. She stated that the allowed number of visits was sometimes adequate but “
most often it is not”, and patients were often asked to return for additional follow-up consultations for which they themselves would pay:
“Because I am not fitting as much in my initial [consultation], then there is always more that we can go through. And so these people are happy to come back for a review, and then er pay for a review, and some people are happy to continue for an ongoing period of time. …For some people two, three, four, five visits is adequate, but usually up to ten.”
The 20-minute process was in contrast to her other fee-paying patients for whom a first consultation was 40 minutes and the fee was correspondingly doubled. Consultation report letter-writing to GP referrers required additional time, although this was greatly facilitated by use of entries in case notes using electronic software which was shared by GP and other allied health providers. For other referrals from outside this clinic, consultation report letters were written.
(b) Longer consultation, charge patients a fee gap
Several dietitians saw the need to provide longer consultations of up to one hour at the first visit. For example, a medium volume provider working in several private clinics in a capital city, both located within a GP clinic and in a multidisciplinary practice without a GP, stated:
“the rebate for dietitians needs to be higher- we can’t do our job properly in 30 minutes!”
Another dietitian explained why this was so:
“Oh, my initial consult needs to be about 45 to 50 minutes, usually at least an hour. You see, the whole thing is- creating rapport with these patients, taking a really good history of where they have been at. And then, when you are working with them, to try and identify the places that they are at, you know? What they are happy to work with [to try and change]. And that takes a good part of an hour!”
A dietitian working in a large provincial town with up to 25 CDM new patients per month justified this process:
“I treat them like any other client that comes and sees me. And I feel in a way, you know, that these clients need more time, they need more attention, because mostly they’ve got a heap- a heap of chronic conditions, and they need a lot more management, a lot more counselling. So- basically, everyone I see in the initial consult, it’s an hour. It’s that same for everybody. I don’t charge them less because I am putting in just as much effort. In fact, more! You know? …It is $80, and I tell the people this when they book in.”
However, introduction of higher payments without direct billing to Medicare meant that patients paid a fee gap and did not receive a low-cost service. In the above case, a patient would pay AU$30.05 from their pocket. As some patients were under the impression that they could receive a ‘fee-free’ service upon referral, one effect of this was that some doctors referred to other lower cost practices. Dietitians were asked about the impact of higher fees for longer consultations. A low volume Medicare provider (<10 referrals per month) in sole suburban practice commented when asked about feedback from patients about how much they have to pay in the gap payment:
“Most are fine. I mean, they understand generally that there is going to be a gap. There are some who, once they realise there is going to be a gap, then they won’t make an appointment. Um- so for those, obviously, I mean, it’s definitely an issue. And it will impact on whether they have any input from anyone.”
There were various comments about patients’ ability to continue attending the clinic according to their ability to pay for follow-up consultations, even though this involved shorter and cheaper consultations. Patients possessing private health insurance were thought to more often attend for review appointments.
(d) Limit CDM patients, or not accept them
Part of the patient referral process is that medical clinics should seek the approval of dietitians for the ‘care plan’ of a patient before sending the referral to a dietetics clinic. However, this did not work effectively. Dietitians were not always asked to have input into the plan. Some dietitians were ambivalent about the number of CDM patient referrals they would accept and interview discussions revealed two main reasons why dietitians might place these limits. Dietitians may have waiting lists for patients and not be intending to increase the overall number of referred patients, and/or they may wish to limit the proportion of CDM patients in their practice because of the relative difference in the remuneration and perceptions of greater reward from other paying private patients. This refers not only to the difference in fees. Dietitians also commented on expectations of professional reward they might receive due to assisting the patients. This was interpreted as applying through their main objective: “giving a quality service” to patients. This theme recurred in interviews and conversely, concerns about short initial consultations were linked with dialogues about not meeting the needs of patients. CDM patient referrals were often seen by dietitians who voiced these attitudes as complex, burdensome, unprofitable, and also costly in terms of the extra administration time and the required report-writing.
3.3. Administrative Costs
While several dietitians received assistance from administrative staff who facilitated appointments, copying, billing and so on, some providers managed these tasks alone. Workforce statistics indicate that a number of providers work sessional or part-time hours in sole positions and these may be less likely to receive administrative help. These factors may negatively influence acceptance of the program, for it was clear that dietitians preferred patient contact to dealing with administrative “red tape”. Administrative costs were thus both finite and also induced.
Prominent in the discussions were issues of the time required for mandatory report-writing under the Medicare CDM policy. It was clear that dietitians regarded these tasks as costly because they were unpaid additions to the care of patients in an environment where time had a price. A dietitian commented:
“I am not getting paid for the time I take to write reports”.
Another dietitian commented
“I write my reports after; I have a writing day when I do my reports, my admin. …Its all personalized. And that’s where I have templates…and it takes time.”
Dietitians are required to provide written reports to GPs on completion of the initial CDM consultation and the final visit, often requiring two letters after two visits. One reason for dietitians’ reluctance may be the use of paper-based or open text letters rather then more structured letters that can be populated with patient information more easily and quickly. A letter was reported to take “
five to ten minutes”. Two interviewed dietitians worked in clinics that shared electronic medical records between doctor and dietitian via shared computer software and this appeared to facilitate the communication:
“We’re all computerized and um, we’ve got templates. So I just put in the individual details into the template and then send it. …Its fantastic!”
This illustrates the potential for cost containment if electronic systems are available for reporting back to referring GPs. All the operations of the dietetics clinics were reportedly constrained by economic factors that they related as being vital to the viability of the clinic business.


{kind=link}