Improving Physical Activity and Dietary Behaviours with Single or Multiple Health Behaviour Interventions? A Synthesis of Meta-Analyses and Reviews

Abstract
:1. Introduction
Pros and cons of multiple health behaviour interventions
Present synthesis
2. Methodology
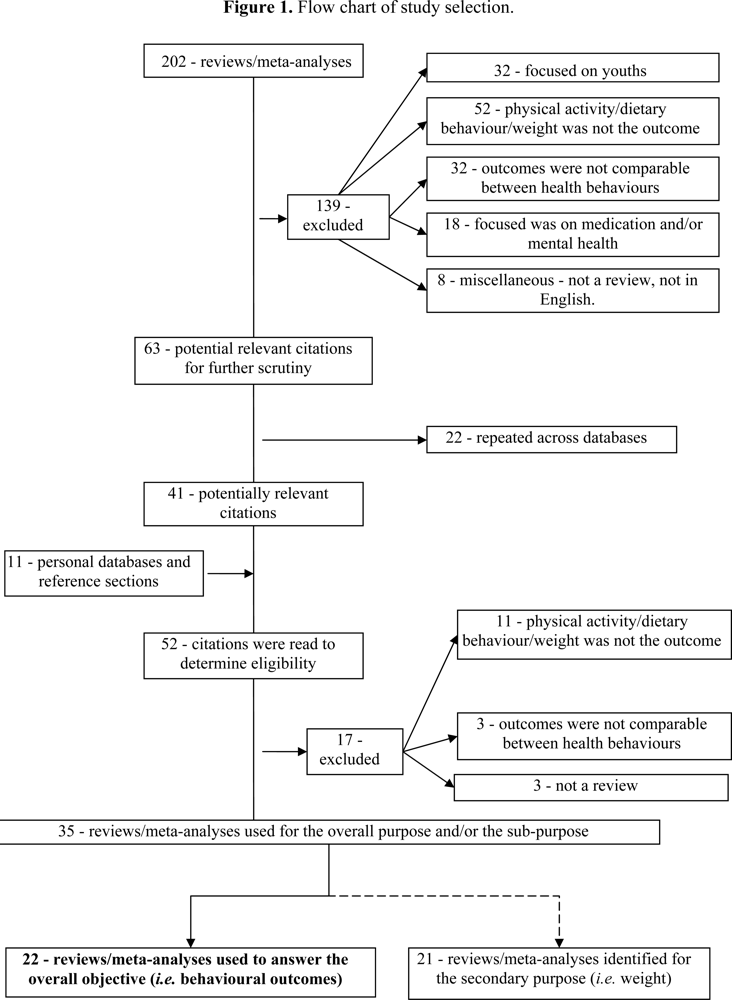
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Description of Meta-Analyses/Reviews of Physical Activity Interventions
2.4. Description of Meta-Analyses/Reviews of Dietary Interventions
2.5. Description of Meta-Analyses/Reviews of Multiple Health Behaviour Interventions
2.6. Data Reporting
3. Results—Overall Objective: Behavioural Outcomes
3.1. Physical Activity Interventions
3.2 Dietary Behaviour Interventions
3.3. Multiple Health Behaviours Intervention for Physical Activity and Diet
3.4. Comparing Single and Multiple Health Behaviour Interventions for Physical Activity and Diet
4. Results—Sub-Purpose: Weight changes
4.1. Physical Activity Interventions for Changes in Weight
4.2. Dietary Behaviour Interventions for Changes in Weight
4.3. Multiple Health Behaviour Interventions for Changes in Weight
4.4. Comparing Single and Multiple Health Behaviour Interventions for Changes in Weight
5. Discussion
Next steps in behavioural health interventions?
6. Conclusion
Acknowledgments
- 1Unless otherwise indicated, reference to single health behaviour will correspond to either physical activity or dietary behaviours while physical activity and dietary behaviours will represent multiple health behaviours. Although we recognize that physical activity and dietary behaviours can be comprised of multiple sub-behaviours (i.e., walking for physical activity, fat intake for dietary), the labels of physical activity and dietary behaviours will reflect the behaviours as a whole unless specified differently.
References
- World Health Organization. WHO: Global Strategy on Diet, Physical Activity and Health Physical Activity. World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Lives. World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Public Health Agency of Canada. Chronic Disease Infobase. 2009. Available online: http://204.187.39.30/surveillance/Trends.aspx (accessed on July 14, 2009).
- King, DE; Mainous, AG; Canemolla, M; Everett, CJ. Adherence to healthy lifestyle habits in US adults, 1988–2006. Am. J. Med 2009, 122, 528–534. [Google Scholar]
- García-Alvarez, A; Serra-Majem, L; Ribas-Barba, L; Castell, C; Foz, M; Uauy, R; Plasencia, A; Salleras, L. Obesity and overweight trends in Catalonia, Spain (1992–2003): gender and socio-economic determinants. Public Health Nutr 2007, 10, 1368–1378. [Google Scholar]
- Charles, M; Eschwège, E; Basdevant, A. Monitoring the obesity epidemic in France: the Obepi surveys 1997–2006. Obesity 2008, 16, 2182–2186. [Google Scholar]
- Haskell, WL; Lee, I; Pate, RR; Powell, KE; Blair, SN; Franklin, BA; Macera, CA; Heath, GW; Thompson, PD; Bauman, A. Physical Activity and Public Health: Updated Recommendation for Adults From the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081–1093. [Google Scholar]
- Poortinga, W. The prevalence and clustering of four major lifestyle risk factors in an English adult population. Prev. Med 2007, 44, 124–128. [Google Scholar]
- Reeves, MJ; Rafferty, AP. Healthy Lifestyle Characteristics Among Adults in the United States, 2000. Arch. Intern. Med 2005, 165, 854–857. [Google Scholar]
- Schuit, AJ; van Loon, JM; Tijhuis, M; Ocke, MC. Clustering of lifestyle risk factors in a general adult population. Prev. Med 2002, 35, 219–224. [Google Scholar]
- Berrigan, D; Dodd, K; Troiano, RP; Krebs-Smith, SM; Barbash, RB. Patterns of health behavior in U.S. adults. Prev. Med 2003, 36, 615–623. [Google Scholar]
- Bucksch, J; Schlicht, W. Health-enhancing physical activity and the prevention of chronic diseases—An epidemiological review. Sozial- und Präventivmedizin 2006, 51, 281–301. [Google Scholar]
- Popkin, BM; Kim, S; Rusev, ER; Du, S; Zizza, C. Measuring the full economic costs of diet, physical activity and obesity-related chronic diseases. Obes. Rev 2006, 7, 271–293. [Google Scholar]
- Ford, ES; Bergmann, MM; Kroger, J; Schienkiewits, A; Weikert, C; Boeing, H. Healthy living is the best revenge: Findings from the European prospective investigation into cancer and nutrition-potsdam study. Arch. Intern. Med 2009, 169, 1355–1362. [Google Scholar]
- Nigg, C; Allegrante, JP; Ory, M. Theory-comparison and multiple-behavior research: common themes advancing health behavior research. Health Educ. Res 2002, 17, 670–679. [Google Scholar]
- Boutelle, KN; Murray, DM; Jeffery, RW; Hennrikus, DJ; Lando, HA. Associations between exercise and health behaviors in a community sample of working adults. Prev. Med 2000, 30, 217–224. [Google Scholar]
- Blakely, F; Dunnagan, T; Haynes, G; Moore, S; Pelican, S. Moderate physical activity and its relationship to select measures of a healthy diet. J. Rural Health 2004, 20, 160–165. [Google Scholar]
- Gillman, MW; Pinto, BM; Tennstedt, S; Glanz, K; Marcus, B; Friedman, RH. Relationships of physical activity with dietary behaviors among adults. Prev. Med 2001, 32, 295–301. [Google Scholar]
- de Vries, H; Kremers, SPJ; Smeets, T; Brug, J; Eijmael, K. The effectiveness of tailored feedback and action plans in an intervention addressing multiple health behaviors. Am. J. Health Promot 2008, 22, 417–425. [Google Scholar]
- Daubenmier, JJ; Weidner, G; Summer, MD; Mendell, N; Worden, T; Studley, J; Ornish, D. The contributions of changes in diet, exercise and stress management to changes in coronary risk in women and men in the multisite cardiac lifestyle intervention program. Ann. Behav. Med 2007, 33, 57–68. [Google Scholar]
- Yancey, AK; McCarthy, WJ; Harrison, GG; Wong, WK; Siegel, JM; Leslie, J. Challenges in improving fitness: Results of a community-based, randomized, controlled lifestyle change intervention. J. Womens Health 2006, 15, 412–429. [Google Scholar]
- Riebe, D; Blissmer, B; Greene, G; Caldwell, M; Ruggiero, L; Stillwell, KM; Nigg, CR. Long-term maintenance of exercise and healthy eating behaviors in overweight adults. Prev. Med 2005, 40, 769–778. [Google Scholar]
- Prochaska, JJ; Spring, B; Nigg, CR. Multiple health behavior change research: An introduction and overview. Prev. Med 2008, 46, 181–188. [Google Scholar]
- Niederhauser, VP; Maddock, J; LeDoux, F; Amold, M. Building strong and ready army families: A multirisk reduction health promotion pilot study. Mil. Med 2005, 170, 227–233. [Google Scholar]
- Emmons, KM. Behavioral and social science contributions to the health of adults in the United States. In Promoting Health: Interventions Strategies from Social and Behavioral Research; Smedley, BD, Syme, SL, Eds.; National Academy Press: Washinton, DC, USA, 2000; p. 254. [Google Scholar]
- Prochaska, JJ; Sallis, JF. A randomized controlled trial of single versus multiple health behavior change: Promoting physical activity and nutrition among adolescents. Health Psychol 2004, 23, 314–318. [Google Scholar]
- Dutton, GR; Napolitano, MA; Whiteley, JA; Marcus, BH. Is physical activity a gateway behavior for diet? Findings from a physical activity trial. Prev. Med 2008, 46, 216–221. [Google Scholar]
- Anderssen, SA; Carroll, S; Urdal, P; Holme, I. Combined diet and exercise intervention reverses the metabolic syndrome in middle-aged males: results from the Oslo Diet and Exercise Study. Scand. J. Med. Sci. Sports 2007, 17, 687–695. [Google Scholar]
- You, T; Murphy, KM; Lyles, MF; Demons, JL; Lenchik, L; Nicklas, BJ. Addition of aerobic exercise to dietary weight loss preferentially reduces abdominal adipocyte size. Int. J. Obes 2006, 30, 1211–1216. [Google Scholar]
- Ebrahim, S; Beswick, A; Burke, M; Davey Smith, G. Multiple risk factor interventions for primary prevention of coronary heart disease (Review). Cochrane Database Syst. Rev 2006, 4, 1–59. [Google Scholar]
- Francke, A; Smit, MC; de Veer, AJE; Mistiaen, P. Factors influencing the implementation of clinical guidelines for health care professionals: A systematic meta-review. BMC Med. Inform. Decis. Mak 2008, 8, 38–48. [Google Scholar]
- Richard, FD; Bond, CF; Stokes-Zoota, JJ. One hundred years of social psychology quantitatively described. Rev. Gen. Psychol 2003, 7, 331–363. [Google Scholar]
- Sharma, M. Behavioural interventions for preventing and treating obesity in adults. Obes. Rev 2007, 8, 441–449. [Google Scholar]
- Conn, VS; Valentine, JC; Cooper, HM. Interventions to increase physical activity among aging adults: A meta-analysis. Ann. Behav. Med 2002, 24, 190–200. [Google Scholar]
- Conn, VS; Hafdahl, AR; Brown, SA; Brown, LM. Meta-analysis of patient education interventions to increase physical activity among chronically ill adults. Patient Educ. Couns 2008, 70, 157–172. [Google Scholar]
- Conn, VS; Hafdahl, AR; Moore, SM; Nielsen, PJ; Brown, LM. Meta-analysis of interventions to increase physical activity among cardiac subjects. Int. J. Cardiol 2009, 133, 307–320. [Google Scholar]
- Eakin, EG; Lawler, SP; Vandelanotte, C; Owen, N. Telephone interventions for physical activity and dietary behavior change: A systematic review. Am. J. Prev. Med 2007, 32, 419–434. [Google Scholar]
- Foster, C; Hillsdon, M; Thorogood, M. Interventions for promoting physical activity. Cochrane Database Syst Rev 2005, 1. [Google Scholar]
- Eakin, EG; Smith, BJ; Bauman, AE. Evaluating the population health impact of physical activity interventions in primary care-are we asking the right questions? J. Phys. Act. Health 2005, 2, 197–215. [Google Scholar]
- Janer, G; Sala, M; Kogevinas, M. Health promotion trials at worksites and risk factors for cancer. Scand. J. Work Environ. Health 2002, 28, 141–157. [Google Scholar]
- Kavookjian, J; Elswick, BM; Whetsel, T. Interventions for being active among individuals with diabetes: A systematic review of the literature. Diabetes Educ 2007, 33, 962–988. [Google Scholar]
- Kahn, EB; Ramsey, LT; Brownson, RC; Heath, GW; Howze, EH; Powell, KE; Stone, EJ; Rajab, MW; Corso, P. The Effectiveness of Interventions to Increase Physical Activity: A Systmatic Review. Am. J. Prev. Med 2002, 22, 73–107. [Google Scholar]
- Kroeze, W; Werkman, A; Brug, J. A Systematic Review of Randomized Trials on the Effectiveness of Computer-Tailored Education on Physical Activity and Dietary Behaviors. Ann. Behav. Med 2006, 31, 205–223. [Google Scholar]
- Neville, LM; O'Hara, B; Milat, AJ. Computer-tailored physical activity behavior change interventions targeting adults: a systematic review. Int. J. Behav. Nutr. Phys. Act 2009, 6, 1–38. [Google Scholar]
- Norris, SL; Engelgau, MM; Venkat Narayan, KM. Effectiveness of self-management training in type 2 diabetes: A systematic review of randomized controlled trials. Diabetes Care 2001, 24, 561–587. [Google Scholar]
- Ogilvie, D; Foster, CE; Rothnie, H; Cavill, N; Hamilton, V; Fitzsimons, CF; Mutrie, N. Interventions to promote walking: systematic review. Br. Med. J 2007, 334, 1204–1207. [Google Scholar]
- Shilts, MK; Horowitz, M; Townsend, MS. Goal setting as a strategy for dietary and physical activity behavior change: A review of the literature. Am. J. Health Promot 2004, 19, 81–93. [Google Scholar]
- Tulloch, H; Fortier, M; Hogg, W. Physical activity counseling in primary care: Who has and who should be counseling? Patient Educ. Couns 2006, 64, 6–20. [Google Scholar]
- van der Bij, A; Laurant, M; Wensing, M. Effectiveness of physical activity interventions for older adults: A review. Am. J. Prev. Med 2002, 22, 120–133. [Google Scholar]
- Amorim Adegboye, AR; Linne, YM; Lourenco, PMC. Diet or exercise, or both, for weight reduction in women after childbirth. Cochrane Database Syst Rev 2007, 3. [Google Scholar]
- Shaw, K; Gennat, H; O’Rourke, P; Del Mar, C. Exercise for overweight or obesity. Cochrane Database Syst Rev 2006, 4. [Google Scholar]
- Brunner, EJ; Rees, K; Ward, K; Burke, M; Thorogood, M. Dietary advice for reducing cardiovascular risk. Cochrane Database Syst Rev 2007, 4. [Google Scholar]
- Pignone, MP; Ammerman, A; Fernandez, L; Orleans, CT; Pender, N; Woolf, S; Lohr, K; Sutton, S. Counseling to Promote a Healthy Diet in Adults A Summary of the Evidence for the U.S. Preventive Services Task Force. Am. J. Prev. Med 2003, 24, 75–92. [Google Scholar]
- Povey, RC; Clark-Carter, D. Diabetes and healthy eating: A systematic review of the literature. Diabetes Educ 2007, 33, 931–959. [Google Scholar]
- Rolls, BJ; Ello-Martin, JA; Tohill, BC. What can intervention studies tell us about the relationship between fruit and vegetable consumption and weight management? Nutr. Rev 2004, 62, 1–17. [Google Scholar]
- Hooper, L; Bartlett, C; Davey Smith, G; Ebrahim, S. Advice to reduce dietary salt for prevention of cardiovascular disease. Cochrane Database Syst Rev 2004, 1. [Google Scholar]
- Rooney, M; Wald, A. Interventions for the management of weight and body composition change in women with breast cancer. Clin. J. Oncol. Nurs 2007, 11, 41–52. [Google Scholar]
- Blue, CL; Black, DR. Synthesis of intervention research to modify physical activity and dietary behaviours. Res. Theory Nurs. Pract 2005, 19, 25–61. [Google Scholar]
- Curioni, CC; Lourenco, PM. Long-term weight loss after diet and exercise: a systematic review. Int. J. Obes 2005, 29, 1168–1174. [Google Scholar]
- Hawthorne, K; Robles, Y; Cannings-John, R; Edwards, AGK. Culturally appropriate health education for type 2 diabetes mellitus in ethnic minority groups. Cochrane Database Syst Rev 2008, 3. [Google Scholar]
- Nield, L; Moore, HJ; Hooper, L; Cruickshank, JK; Vyas, A; Whittaker, V; Summerbell, CD. Dietary advice for treatment of type 2 diabetes mellitus in adults. Cochrane Database Syst. Rev 2007, 4, 1–73. [Google Scholar]
- Norris, SL; Zhang, X; Avenell, A; Gregg, E; Brown, TJ; Schmid, CH; Lau, J. Long-term non-pharmacological weight loss interventions for adults with type 2 diabetes mellitus. Cochrane Database Syst Rev 2005, 2. [Google Scholar]
- Norris, SL; Zhang, X; Avenell, A; Gregg, E; Schmid, CH; Lau, J. Long-term non-pharmacological weight loss interventions for adults with prediabetes. Cochrane Database Syst Rev 2005, 2. [Google Scholar]
- Orozco, LJ; Buchleitner, AM; Gimenez-Perez, G; Roqué i Figuls, M; Richter, B; Mauricio, D. Exercise or exercise and diet for preventing type 2 diabetes mellitus. Cochrane Database Syst Rev 2008, 4. [Google Scholar]
- Chaston, TB; Dixon, JB; O’Brien, PE. Changes in fat-free mass during significant weight loss: a systematic review. Int. J. Obes 2007, 31, 743–750. [Google Scholar]
- Ketola, E; Sipila, R; Makela, M. Effectiveness of individual lifestyle interventions in reducing cardiovascular disease and risk factors. Ann. Med 2000, 32, 239–252. [Google Scholar]
- Churche, TS; Martin, CK; Thompson, AM; Earnest, CP; Mikus, CR; Blair, SN. Changes in weight, waist circumference and compensatory responses with different doses of exercise among sedentary, overweight postmenopausal women. PLoS ONE 2009, 4, e4515. [Google Scholar]
- Soderlund, A; Fischer, A; Johansson, T. Physical activity, diet and behaviour modification in the treatment of overweight and obese adults: a systematic review. Perspect. Public Health 2009, 129, 132–142. [Google Scholar]
- Fogelholm, M; Kukkonen-Harjula, K. Does physical activity prevent weight gain—a systematic review. Obes. Rev 2000, 1, 95–111. [Google Scholar]
- Franz, MJ; van Wormer, JJ; Crain, AL; Boucher, JL; Histon, T; Caplan, W; Bowman, JD; Ponk, NP. Weight loss outcomes: A systematic review and meta-analysis of weight loss clinical trials with a minimum of 1-year follow-up. J. Am. Diet. Assoc 2007, 107, 1755–1767. [Google Scholar]
- Ross, R; Bradshaw, AJ. The future of obesity reduction: beyond weight loss. Nat. Rev. Endocrinol 2009, 5, 319–326. [Google Scholar]
- Prochaska, JJ; Velicer, WF; Nigg, CR; Prochaska, JO. Methods of quantifying change in multiple risk factor interventions. Prev Med 2008, 46, 260–265. [Google Scholar]
- Egan, M; Tannahill, C; Petticrew, M; Thomas, S. Psychosocial risk factors in home and community settings and their associations with population health and health inequalities: A systematic meta-review. BMC Public Health 2008, 8, 239–251. [Google Scholar]
- Vandelanotte, C; De Bourdeaudhuij, I; Sallis, JF; Spittaels, H; Brug, J. Efficacy of sequential or simultaneous interactive computer-tailored interventions for increaseing physical activity and decreasing fat intake. Ann. Behav. Med 2005, 29, 138–146. [Google Scholar]
- Vandelanotte, C; Reeves, MM; Brug, J; De Bourdeaudhuij, I. A randomized trial of sequential and simultaneous multiple behavior change interventions for physical activity and fat intake. Prev. Med 2008, 46, 232–237. [Google Scholar]
- Hyman, DJ; Pavlik, VN; Taylor, WC; Goodrick, GK; Moye, L. Simultaneous vs. sequential counseling for multiple behavior change. Arch. Intern. Med 2007, 167, 1152–1158. [Google Scholar]
- Vandelanotte, C; De Bourdeaudhuij, I; Brug, J. Two-year follow-up of sequential and simultaneous interactive computer-tailored interventions for increasing physical activity and decreasing fat intake. Ann. Behav. Med 2007, 33, 213–219. [Google Scholar]
- Spring, B; Doran, N; Pagoto, S; Schneider, K; Pingitore, R; Hedeker, D. Randomized controlled trial for behavioral smoking and weight control treatment: Effect of concurrent versus sequential intervention. J. Consult. Clin. Psychol 2004, 72, 785–796. [Google Scholar]
- Improved Clinical Effectiveness through Behavioural Research Group Designing theoretically-informed implementation interventions. Implement. Sci 2006, 1, 4–11.
- Baranowski, T; Anderson, C; Carmack, C. Mediating variable framework in physical activity interventions. How are we doing? How might we do better? Am. J. Prev. Med 1998, 15, 266–297. [Google Scholar]
- Painter, JE; Borba, CPC; Hynes, M; Mays, D; Glanz, K. The Use of Theory in Health Behavior Research from 2000 to 2005: A Systematic Review. Ann. Behav. Med 2008, 35, 358–362. [Google Scholar]
- King, TA; Marcus, BH; Pinto, BM; Emmons, KM; Abrams, DB. Cognitive-Behavioral Mediators of Changing Multiple Behaviors: Smoking and a Sedentary Lifestyle. Prev. Med 1996, 26, 684–691. [Google Scholar]

{kind=link}
| Review/Meta-Analysis | Year | Number of Articles | Percentage | Effect size |
|---|---|---|---|---|
| Physical Activity | ||||
| Conn et al. [34] | 2002 | 43 | N/A | 0.26 |
| Conn et al. [35] | 2008 | 62 | N/A | 0.35 |
| Conn et al. [36] | 2009 | 129 | N/A | 0.45 |
| Eakin et al. [39] | 2005 | 9 (all reviews) | 67% | |
| All 9 reported on short-term PA | 67% | N/A | ||
| All 9 reported on long-term PA | 0% | |||
| Eakin et al. [37] | 2007 | 16 (all studies) | 69% | 0.5 (8 of 16 studies) |
| 15 of 16 reported on short-term PA | 47% | |||
| 6 of 6 reported on long-term PA | 100% | |||
| Foster et al. [38] | 2005 | 29 (all studies) | 31% | |
| 19 (continuous PA) | 37% | 0.28 | ||
| 10 (categorical PA) | 20% | 1.33 (Odds Ratio) | ||
| Janer et al. [40] | 2002 | 15 | 67% | N/A |
| Kavookjian et al. [41] | 2007 | 18 | 78% | N/A |
| Khan et al. [42] | 2002 | 39 | 74% | N/A |
| Kroeze et al. [43] | 2006 | 4 | 25% | N/A |
| Neville et al. [44] | 2009 | 8 | 63% | N/A |
| Norris et al. [45] | 2001 | 6 | 50% | N/A |
| Ogilvie et al. [46] | 2007 | 18 | 89% | N/A |
| Shilts et al. [47] | 2004 | 8 | 75% | N/A |
| Tulloch et al. [48] | 2006 | 20 (all studies) | 75% | |
| 9 of 20 reported on short-term PA | 78% | N/A | ||
| 13 of 20 reported on long-term PA | 69% | |||
| van der Bij et al. [49] | 2002 | 22 (all studies) | 64% | |
| 9 of 22 reported on long-term | 33% | N/A | ||
| Dietary Behaviours | ||||
| Brunner et al. [52] | 2007 | F&V : 18 | F&V : 0.80 | |
| Fiber : 9 | Fiber : 0.75 | |||
| FI : 20 | N/A | FI : 0.65 | ||
| FI : 12 (saturated) | FI : 0.71 (saturated) | |||
| Eakin et al. [37] | 2007 | 6 | 83% | 0.74 (4 of 6 studies) |
| Janer et al. [40] | 2002 | All behaviours: 66% | ||
| V: 7 | V: 86% | |||
| F: 7 | F: 57% | N/A | ||
| FI: 10 | FI: 60% | |||
| Fiber: 5 | Fiber: 60% | |||
| Kroeze et al. [43] | 2006 | All behaviours: 38% | ||
| FI: 5 | FI: 20% | N/A | ||
| F&V: 3 | F&V: 67% | |||
| Norris et al. [45] | 2001 | 11 | 82% | N/A |
| Pignone et al. [53] | 2003 | All behaviours: 91% | ||
| FI : 17 | FI (only 15 studies reported significance): 93% | FI : N/A, but 6 were rated as having a large effect, 5 medium, 6 small | ||
| F&V : 10 | F&V (only 4 of 10 studies reported significance): 75% | F&V: N/A, but 2 were rated as having a large large, 5 medium, 3 small | ||
| Fiber : 7 | Fiber (only 3 studies reported significance): 100% | Fiber: N/A, but 5 were rated as having a medium and 2 a small effect. | ||
| Povey et al. [54] | 2007 | All behaviours: 62% | ||
| FI: 14 | FI: 71% | N/A | ||
| FI: 10 (saturated) | FI: 70% (saturated) | |||
| F&V: 3 | F&V: 100% | |||
| Fiber: 8 | Fiber: 38% | |||
| Rolls et al. [55] | 2004 | F&V: 12 | F&V: 50% | N/A |
| Shilts et al. [47] | 2004 | 4 | 50% | N/A |
| Physical Activity and Diet | ||||
| Blue & Black [58] | 2005 | 6 | 50%a | N/A |
| Eakin et al. [37] | 2007 | 4 | 75%a | .86 (1 study) |
| Kroeze et al. [43] | 2006 | 6 | 17%a | N/A |
| 33%b | ||||
| Neville et al. [44] | 2009 | 6 | 33% | N/A |
| Norris et al. [45] | 2001 | 3 | 33%a | N/A |
| 100%b | ||||
| Sharma [33] | 2007 | 2 | 50%a | N/A |
| 100%b | ||||
| Review/Meta-Analysis | Year | Number of Articles | Percentage | Effect Size |
|---|---|---|---|---|
| Physical Activity | ||||
| Amorim et al. [50] | 2007 | 1 | N/A | 0.00 |
| Conn et al.a [36] | 2009 | 13 | N/A | 0.07 |
| Kavookjian et al.a [41] | 2007 | 4 | 100% | N/A |
| 7 (BMI) | 43% (BMI) | |||
| Shaw et al. [51] | 2006 | 2 | N/A | 0.58 |
| Dietary Behaviours | ||||
| Amorim et al. [50] | 2007 | 1 | N/A | 5.76 |
| Brunner et al.a [52] | 2007 | 21 | 38% | N/A |
| Hooper et al. [56] | 2004 | 5 | 60% | N/A |
| Povey et al.a [54] | 2007 | 6 | 17% | N/A |
| 5 (BMI) | 40% | |||
| Rolls et al.a [55] | 2004 | 16 | 44% | N/A |
| Rooney et al. [57] | 2007 | 4 | 50% | N/A |
| Physical Activity and Diet | ||||
| Amorim et al. [50] | 2007 | 4 | N/A | 1.79i |
| 1 | −0.49ii | |||
| Blue & Blacka [58] | 2005 | 11 | 73%i | N/A |
| Chaston et al. [65] | 2007 | 3 | 100%ii | N/A |
| Curioni et al. [59] | 2005 | 6 | N/A | 0.2ii |
| Hawthorne et al. [60] | 2008 | 3 (BMI) | 0% i (BMI) | 0.31 i (BMI) |
| Ketola et al. [66] | 2000 | 17 | 71% i | N/A |
| Neville et al.a [44] | 2009 | 6 | 50% i | N/A |
| Nield et al. [61] | 2007 | 4 | 100%ii | 0.51ii |
| Norris et al. [63] | 2005 | 9 | 83% i | 0.77i (7 studies) |
| 6 (BMI) | 67% i (BMI) | 0.97i (BMI) | ||
| Norris et al. [62] | 2005b | 8 | N/A | 0.01i |
| Orozco et al. [64] | 2008 | 7 | N/A | 0.66i |
| 6 (BMI) | 0.57i (BMI) | |||
| Povey et al.a [54] | 2007 | 6 | 33%i | N/A |
| Sharmaa [33] | 2007 | 8 | 88%i | N/A |
| 4 (BMI) | 75%i (BMI) | |||
| Shaw et al. [51] | 2006 | 15 | N/A | 0.48ii |
| 6 (BMI) | 0.21ii (BMI) | |||
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Sweet, S.N.; Fortier, M.S. Improving Physical Activity and Dietary Behaviours with Single or Multiple Health Behaviour Interventions? A Synthesis of Meta-Analyses and Reviews. Int. J. Environ. Res. Public Health 2010, 7, 1720-1743. https://doi.org/10.3390/ijerph7041720
Sweet SN, Fortier MS. Improving Physical Activity and Dietary Behaviours with Single or Multiple Health Behaviour Interventions? A Synthesis of Meta-Analyses and Reviews. International Journal of Environmental Research and Public Health. 2010; 7(4):1720-1743. https://doi.org/10.3390/ijerph7041720
Chicago/Turabian StyleSweet, Shane N., and Michelle S. Fortier. 2010. "Improving Physical Activity and Dietary Behaviours with Single or Multiple Health Behaviour Interventions? A Synthesis of Meta-Analyses and Reviews" International Journal of Environmental Research and Public Health 7, no. 4: 1720-1743. https://doi.org/10.3390/ijerph7041720