Multi-Stakeholder Perspectives of Factors That Influence Contact Centre Call Agents’ Workplace Physical Activity and Sedentary Behaviour


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants and Settings
2.3. Focus Groups and Interviews
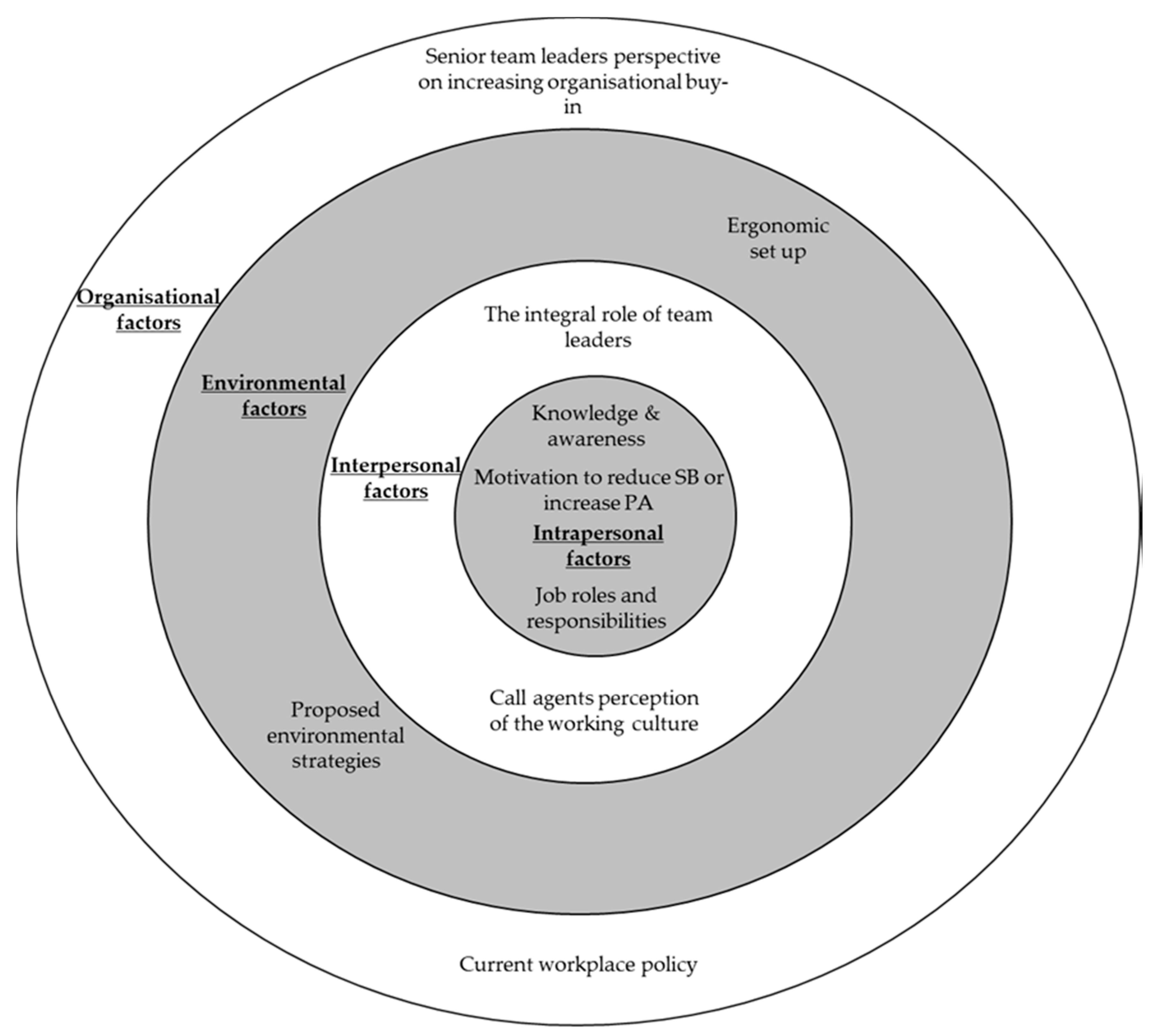
2.4. Focus Groups and Interviews Analysis and Representation
2.5. Surveys and Questionnaires
3. Results
3.1. Intrapersonal Factors
3.1.1. Knowledge and Awareness
“I’m sat down really. I don’t move, I really don’t move. So it’s completely sedentary until break about quarter past one and I’m sat down then as well.”P38 (AG4 FG)
“I’ve put on weight, and my back kills sometimes, yes, from just having like really long days sat down, especially on the days that I don’t do anything after work as well. So like if I’m sat down all day at work, and then I go home and I’m sat in a chair at home or whatever when I go home, my back’s killing me.”P28 (AG4 FG)
“I’ve noticed that you kind of, when you’re up and about, you’re constantly moving and generally sort of feel a bit better by sort of moving and doing more things. (…) You may then get better working environments and more effective work from each individual if you do introduce more activity throughout the day.”P36 (AG4 FG)
“Really? I didn’t know about that (workplace recommendations). I was just more thinking about it’s my eyes. I didn’t actually think me as like my body and everything.”P6 (AG1 FG)
“(Reducing sitting by 2–4 h per day) That’s just not feasible working here, I don’t think. It would just be virtually impossible to cut (sitting) down by so much.”P6 (AG1 FG)
“(I would) just like more information on what the benefits are of doing it (breaking sitting time), be that health-wise or be that job-wise. Because obviously, at the moment you know realistically you shouldn’t be sat down all day, because it’s not good for you, but you don’t know the reasons, like what’s the benefits.”P1 (TL1 FG)
3.1.2. Motivation to Reduce SB or Increase PA
“It’s the fact that I think you just feel so drained and so tired from looking at the screen and just sitting there (…) and I just think you don’t feel motivated.”P4 (AG1 FG)
“I would spend it (break times) at my desk, or if I think I’ve got enough time, I go into the little short room with the sofa. I go and lie on the sofa.”P33 (AG3 FG)
“…so I tend to go in there, plug myself into my iPod, listen to a book, and so three quarters of an hour, just take myself away. I’m still sat. I don’t walk anywhere. But I kind of take myself away from work, and then come back mentally afterwards.”P15 (AG2 FG)
“I find with myself, when I’m sat down for too long, I tend to feel it more than anything, so I find that even if the opportunity to go up and do a brew run, say, getting myself moving, it tends to help kind of getting the blood flowing, shall we say, so when I do sit back down again and I’m back on my calls, it helps with keeping me alert, I think.”P34 (AG3 FG)
“…it’s not really promoted on a daily basis. Because it’s the same with advertising. If you don’t advertise it, if you’re not going to notice it.”P34 (AG3 FG)
“…the challenge they (team leaders) have is getting (health and wellbeing initiatives) off the ground. It’s not because of the effort we put into it, it’s because of the effort that the individual wants to give back. That’s the challenge.”P24 (ST3 I)
“You might find that people will ask for something, even push for, but not use when it’s delivered and the opportunity’s there.”P34 (TL4 I)
“We don’t want to be kind of dictating to people what they do and how they do it you know, poking people when they’ve been sat down for too long.”P18 (ST1 FG)
“…well you can take the horse to water can’t you but you know there’s only so much you can, you can do, you can put it there, you can make it as, you know as available as possible but it then does rely on peoples sense of self responsibility to engage in that.”P11 (ST2 FG)
“(We need) wellbeing interventions that are tailored to the specific wants and needs of our agents, and for that, we require agent feedback (…) we need to understand what the specific definition of wellbeing is for the individual to work for us in our contact centres (…) unless we get to that definition, then it’s likely that whatever we try and do, (…), we’ll miss the mark, because we’re not actually creating a solution that is fixing the problem, because the problem hasn’t been identified.”P26 (ST2 FG)
3.1.3. Job Roles and Responsibilities
“That’s the job, isn’t it? You’re employed to be sat down to take calls.”P34 (AG3 FG)
“I just think, well, they’re paying me to do a job, so why should they pay me for doing my exercises.”P9 (AG1 FG)
“There’s no requirement within that role for us to get up and wander around. There’s nothing within the job description that says we need to do that.”P15 (AG2 FG)
“I’ve not been here that long, to be honest, and I think that’s probably why I’m more anxious about security of the job.”P4 (AG1 FG)
“I’d just like to be able to work standing up if I choose to, to have a desk that you can perhaps move up so that I can stand up for half an hour, because I’m fed up of sitting down.”P16 (AG2 FG)
“It’s like me, I choose to sit down all day, I choose to sit in the bistro. It’s not the company making me do that, that’s just the way I am.”P15 (AG2 FG)
“…I manage a team of people and I’ve got you know different types of people, some that are quite active, some that aren’t quite as active as each other.”P23 (TL3)
“I think something that we could tailor to the individual needs as well.”P21 (TL3 FG)
“…you’ve got a pile of escalations that have piled up, a pile of credits that have piled up, a load of emails that your line managers have sent you and they say ‘well why haven’t you done that?’ (…) Sometimes you’re distracted, being a manger because of all the tasks that you have to do in a day, I don’t know how you find the balance to be honest.”P20 (TL3 FG)
“You’ll get a fantastic management buy-in to those kind of theories, because it’s offloading a responsibility to a third party in a recognised format (…) somebody like a workplace champion would (…) decide to be involved, raise awareness (…) none of this would be for everybody, but to have, again, a workplace champion in place that understood, was a point of contact (…) I can see that working really quite well.”P43 (TL4 I)
“…I think that’s definitely something that we can take away isn’t it as an idea. (…) is anybody interested (…) almost like applying for a role.”P18 (ST1 FG)
“Most definitely yeah. I mean well that’s just part and parcel if it isn’t it that you know, in mental health, if someone’s feeling down or you know ‘get up and go and take some fresh air’, ‘take yourself out of a situation’, it all comes part of that (…) it’s definitely within conversations that we have with staff on a day to day basis you know yeah, mentally and physically.”P13 (TL2 I)
“I think we (company 1) should encourage it. I think we should at least make people aware of the things that they can do, and perhaps that’s something we maybe, we don’t talk enough about or promote that we do allow people to go and make themselves a brew and have a walk or if they want to go downstairs then because that is quite a thing to promote and talk about that people can do that kind of thing in the workplace.”P18 (ST1 FG)
“…we have reports which effectively tell us at any given moment of the day, the status of an agent’s phone.”P26 (ST3 FG)
“Am I trying to achieve something that I can turn round to my bosses and go ’look, we improved performance’, or am I actually trying to turn round and say ’people are happier’? You’ve got to prioritise.”P26 (ST3 FG)
3.2. Interpersonal Factors
3.2.1. Call Agents’ Perception of the Working Culture
“…we’re in the culture that we are in where we are just quite happy to sit at our desks (…) There needs to be a bit of enthusiasm led by the business.”P35 (AG4 FG)
“…if everyone was doing it, everybody else would just go ‘look at them skiving again going outside’, and ‘how many calls have you took today?’”P9 (AG 1 FG)
“…some staff probably feel as though, ‘if I go away from my desk, they’re (team leaders) going to think I’m skiving or not doing my work’.”P2 (TL1 FG)
3.2.2. The Integral Role of Team Leaders
“So if all team managers and whoever and it came from top down and led by example; so if there all acting a certain way, it becomes the culture within the contact centre and then subconsciously you are going to be more active because you’re not realising it. You’re not making a conscious effort to a certain point because everybody is doing it and then it becomes normal.”P35 (AG4 FG)
“So everybody does need to have a break so that they come back fresh, but what we do is, we just slog through it, because everybody just does now, (…) our leaders do that as well. I’m not saying it’s their fault, it’s absolutely not their fault, but no one else will change until they see them (team leaders) actually changing first.”P25 (ST 3 FG)
3.3. Environmental Factors
3.3.1. Ergonomic Set-Up
“You can’t leave. You’ve got to capture the information whilst you’re on the phone. It’s got to be correct and accurate. So I think that’s a major barrier.”P36 (AG4 FG)
“The headset, you know, you’d be bending over again and again. It’s not ideal. The best way to actually do the job I do, is actually being sat down.”P38 (AG4 FG)
3.3.2. Proposed Environmental Strategies
“I’d like to see us (…) come up with a, not radical but something different like we might have banks of desks that you know that are permanently up or different ways that they can sit, or when they’ve been sat for a few hours and think ‘I’m going to move over to this hot desk and I’m going to work here because I can stand.”P12 (ST2 FG)
“I can absolutely see the benefits of them (height-adjustable workstations) I really, truly can it’s just thinking about how you practically do it within this kind of working environment isn’t it, without incurring a massive cost.”P18 (ST1 FG)
“So it’s just a standing up desk? I probably wouldn’t. I think that’s more due to a bit of laziness, or it’s, what can I say? I think it’d be more the novelty of it might wear off after a certain amount of time, and then I’d probably think ‘I want to sit down now’.”P3 (AG3 FG)
“You don’t have to do your 1:1 sat in a room do you? You could go for a walk.”P20 (TL3 FG)
“We (team leaders) could promote it, walking up the stairs let’s have a challenge for the week, whoever does the most steps, get in stepometers or something.”P13 (TL2 I)
“(In relation to using a hot desk) the IT never works somewhere else, and you get your own desk with your stuff, your information and everything. You can’t transport all that around.”P16 (AG2 FG)
“(Regarding short frequent breaks) there’s more opportunity to not be adhering to it.”P26 (ST3 FG)
“I mean, five minutes. What would you do in five minutes? You may as well just stand up at your desk and then sit back down again.”P28 (AG3 FG)
“I think it’s trying to build it into your job (…) I like standing up or moving around a bit and twisting, so you can do that on the phone, but it’s how to do all the typing things and other things as well.”P8 (AG 1 FG)
“… also so that it (reducing sitting) can be done no matter whether it’s busy or it’s quiet, because again, I think we too easily take on ideas when it’s really easy to do it, but if it becomes harder, obviously they go out the window (…). If we hit red alert, it means we’ve got two to three calls queuing, then everything is pulled.”P32 (TL3 FG)
3.4. Organisational Factors
3.4.1. Senior Team Leaders’ Perspective on Increasing Organisational Buy-In
“…if staff are healthier and happier then they’re going to be more engaged within the workplace.”(P18 ST1 FG)
“They (the senior team) want to understand the usual things, why you want to do it (reduce sitting and increase PA), what the benefits for the business is going to be, the benefit to the individual, what are the risks associated if you don’t do it (reduce sitting and increase PA), a cost, and then what’s their return on investment for doing it (reduce sitting and increase PA).”P42 (ST4 FG)
“I would love to be able to measure the output of the wellbeing intervention from the perspective of engagement/other business metrics such as absence (…) So we’re trying to make a culture change, but you can’t make a culture change without your leaders, but you also can’t make a culture change without investment, and you don’t get investment unless you can prove the benefit.”P26 (ST3 FG)
“…there’s an uncomfortable sort of, it’s almost a paradox to talk about ROI (return on investment) and wellbeing in the same breath.”P26 (ST3 FG)
3.4.2. Current Workplace Policy
“We are trying to pull together a health and wellbeing strategy for (employee), but (…) I would say at the moment (sitting time and PA) it’s probably not defined.”P25 (ST3 FG)
“… it is very easy just to sit there when you’re having your breaks or your lunches and stay behind your computer and actually do anything.”P23 (TL3 FG)
“They have the choice of standing or sitting, depending on what they want to do. We have at least two of those (height-adjustable workstations) sets here, but they’re for occupational health reasons only.”P32 (TL3 FG)
“There’s no requirement within that role for us to get up and wander around. There’s nothing within the job description that says we need to do that.”P15 (AG2 FG)
“…if (promotion of active breaks and sitting reduction) was in the team leader’s job description it might be a help.”P9 (AG1 FG)
“…that comes down to your employees that are happy to come into work and of course with initiatives like this it’s that whole sense of the employees that they feel the companies invested in them, values them which again can of course have positive effects in terms of things we’ve kind of touched on, morale, productivity, things like that.”P17 (ST1 FG)
4. Discussion
Strengths and Challenges for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; SBRN Terminology Consensus Project Participants. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes 2007, 56, 2655–2667. [Google Scholar] [CrossRef] [PubMed]
- Burton, J. WHO Healthy Workplace Framework and Model; World Health Organisation: Geneva, Switzerland, 2010. [Google Scholar]
- Dunstan, D.W.; Thorp, A.A.; Healy, G.N. Prolonged sitting: Is it a distinct coronary heart disease risk factor? Curr. Opin. Cardiol. 2011, 26, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Cerin, E.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Breaks in sedentary time—Beneficial associations with metabolic risk. Diabetes Care 2008, 31, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, D.W.; Wiesner, G.; Eakin, E.G.; Neuhaus, M.; Owen, N.; LaMontagne, A.D.; Moodie, M.; Winkler, E.A.; Fjeldsoe, B.S.; Lawler, S.; et al. Reducing office workers’ sitting time: Rationale and study design for the Stand Up Victoria cluster randomized trial. BMC Public Health 2013, 13, 1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health. Start Active Stay Active: A Report on Physical Activity for Health from the Four Home Countries’ Chief Medical Officers; Department of Health: London, UK, 2011.
- Mansoubi, M.; Pearson, N.; Biddle, S.J.; Clemes, S. The relationship between sedentary behaviour and physical activity in adults: A systematic review. Prev. Med. 2014, 69, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U. Toward an experimental ecology of human development. Am. Psychol. 1977, 32, 513–531. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N.; Fisher, E.B. Ecological models of health behavior. Health Behav. Health Educ. 2008, 4, 465–486. [Google Scholar]
- Alkhajah, T.A.; Reeves, M.M.; Eakin, E.G.; Winkler, E.A.; Owen, N.; Healy, G.N. Sit-Stand Workstations A Pilot Intervention to Reduce Office Sitting Time. Am. J. Prev. Med. 2012, 43, 298–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackenzie, K.; Goyder, E.; Eves, F. Acceptability and feasibility of a low-cost, theory-based and co-produced intervention to reduce workplace sitting time in desk-based university employees. BMC Public Health 2015, 15, 1294. [Google Scholar] [Green Version]
- Coenen, P.; Gilson, N.; Healy, G.N.; Dunstan, D.W.; Straker, L.M. A qualitative review of existing national and international occupational safety and health policies relating to occupational sedentary behaviour. Appl. Ergon. 2017, 60, 320–333. [Google Scholar] [CrossRef] [PubMed]
- Black, C.M. Working for a Healthier Tomorrow: Dame Carol Black’s Review of the Health of Britain’s Working Age Population; The Stationery Office: London, UK, 2008. [Google Scholar]
- NICE (National Institute for Health and Care Excellence). Physical Activity in the Workplace. Available online: https://www.nice.org.uk/guidance/ph13/resources/physical-activity-in-the-workplace-pdf-1996174861765 (accessed on 7 July 2016).
- Hadgraft, N.T.; Brakenridge, C.L.; Lamontagne, A.D.; Fjeldsoe, B.S.; Lynch, B.M.; Dunstan, D.W.; Owen, N.; Healy, G.V.; Lawler, S.P. Feasibility and acceptability of reducing workplace sitting time: A qualitative study with Australian office workers. BMC Public Health 2016, 16, 933. [Google Scholar] [CrossRef] [PubMed]
- Such, E.; Mutrie, N. Using organisational cultural theory to understand workplace interventions to reduce sedentary time. Int. J. Health Promot. Educ. 2017, 55, 18–29. [Google Scholar]
- De Cocker, K.; Veldeman, C.; De Bacquer, D.; Braeckman, L.; Owen, N.; Cardon, G.; De Bourdeaudhuij, I. Acceptability and feasibility of potential intervention strategies for influencing sedentary time at work: Focus group interviews in executives and employees. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrestha, N.; Kukkonen-Harjula, K.T.; Verbeek, J.H.; Ijaz, S.; Hermans, V.; Pedisic, Z. Workplace interventions for reducing sitting at work. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Eakin, E.G.; Owen, N.; LaMontagne, A.D.; Moodie, M.; Winkler, E.A.; Fjeldsoe, B.S.; Wiesner, G.; Willenberg, L.; Dunstan, D.W. A Cluster Randomized Controlled Trial to Reduce Office Workers’ Sitting Time: Effect on Activity Outcomes. Med. Sci. Sports Exerc. 2016, 48, 1787–1797. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.H.; Blake, H.; Suggs, L.S. A systematic review of workplace health promotion interventions for increasing physical activity. Br. J. Health Psychol. 2014, 19, 149–180. [Google Scholar] [CrossRef] [PubMed]
- Sprigg, C.A.; Smith, P.R.; Jackson, P.R. Psychosocial Risk Factors in Call Centres: An Evaluation of Work Design and Well-Being; HSE: Bootle, UK, 2003. [Google Scholar]
- Toomingas, A. Working conditions and health at call centres. In Worklife and Health in Sweden 2004; National Institute for Working Life: Lund, Sweden, 2005; pp. 341–366. [Google Scholar]
- Toomingas, A.; Forsman, M.; Mathiassen, S.E.; Heiden, M.; Nilsson, T. Variation between seated and standing/walking postures among male and female call centre operators. BMC Public Health 2012, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- Thorp, A.A.; Healy, G.N.; Winkler, E.; Clark, B.K.; Gardiner, P.A.; Owen, N.; Dunstan, D.W. Prolonged sedentary time and physical activity in workplace and non-work contexts: A cross-sectional study of office, customer service and call centre employees. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 128. [Google Scholar] [CrossRef] [PubMed]
- Straker, L.; Abbott, R.A.; Heiden, M.; Mathiassen, S.E.; Toomingas, A. Sit-stand desks in call centres: Associations of use and ergonomics awareness with sedentary behavior. Appl. Ergon. 2013, 44, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Renton, S.J.; Lightfoot, N.E.; Maar, M.A. Physical activity promotion in call centres: Employers’ perspectives. Health Educ. Res. 2011, 26, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Garrett, G.; Benden, M.; Mehta, R.; Pickens, A.; Peres, S.C.; Zhao, H. Call Center Productivity Over 6 Months Following a Standing Desk Intervention. IIE Trans. Occup. Ergon. Hum. Factors 2016, 4, 188–195. [Google Scholar] [CrossRef]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An Ecological Perspective on Health Promotion Programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, M.; Healy, G.N.; Dunstan, D.W.; Owen, N.; Eakin, E. Workplace Sitting and Height-Adjustable Workstations A Randomized Controlled Trial. Am. J. Prev. Med. 2014, 46, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.Y.; Sukala, W.; Fedel, K.; Do, A.; Engelen, L.; Kingham, M.; Sainsbury, A.; Bauman, AE. More standing and just as productive: Effects of a sit-stand desk intervention on call center workers’ sitting, standing, and productivity at work in the Opt to Stand pilot study. Prev. Med. Rep. 2016, 3, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.Y.; Engelen, L.; Burks-Young, S.; Daley, M.; Maxwell, J.K.; Milton, K.; Bauman, A. Perspectives on a “Sit Less, Move More” Intervention in Australian Emergency Call Centres. AIMS Public Health 2016, 3, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Wierenga, D.; Engbers, L.H.; Van Empelen, P.; Duijts, S.; Hildebrandt, V.H.; Van Mechelen, W. What is actually measured in process evaluations for worksite health promotion programs: A systematic review. BMC Public Health 2013, 13, 1190. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- HSE (Health and Safety Executive). Display Screen Equipment. Available online: http://www.hse.gov.uk/msd/dse/assessment.htm (accessed on 5 March 2018).
- Chau, J.Y.; Daley, M.; Srinivasan, A.; Dunn, S.; Bauman, A.E.; nvan der Ploeg, H.P. Desk-based workers’ perspectives on using sit-stand workstations: A qualitative analysis of the Stand@Work study. BMC Public Health 2014, 14, 752. [Google Scholar] [CrossRef] [PubMed]
- Robinson, N. The use of focus group methodology—With selected examples from sexual health research. J. Adv. Nurs. 1999, 29, 905–913. [Google Scholar] [CrossRef] [PubMed]
- Kitzinger, J. Qualitative research. Introducing focus groups. BMJ Br. Med. J. 1995, 311, 299. [Google Scholar] [CrossRef]
- Shenton, A.K. Strategies for ensuring trustworthiness in qualitative research projects. Educ. Inf. 2004, 22, 63–75. [Google Scholar] [CrossRef]
- Neuhaus, M.; Healy, G.N.; Fjeldsoe, B.S.; Lawler, S.; Owen, N.; Dunstan, D.W.; LaMontagne, A.D.; Eakin, E.G. Iterative development of Stand Up Australia: A multi-component intervention to reduce workplace sitting. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.P.; Hdege, A.; Yates, T.; Copeland, R.J.; Loosemore, M.; Hamer, M.; Bradley, G.; Dunstan, D.W. The sedentary office: An expert statement on the growing case for change towards better health and productivity. Br. J. Sports Med. 2015, 49, 1357–1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. What can “thematic analysis” offer health and wellbeing researchers? Int. J. Q. Stud. Health Well-Being 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graves, L.E.F.; Murphy, R.C.; Shepherd, S.O.; Cabot, J.; Hopkins, N.D. Evaluation of sit-stand workstations in an office setting: A randomised controlled trial. BMC Public Health 2015, 15, 1145. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 195, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.Y.; van der Ploeg, H.P.; Dunn, S.; Kurko, J.; Bauman, A.E. A tool for measuring workers’ sitting time by domain: The Workforce Sitting Questionnaire. Br. J. Sports Med. 2011, 45, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of Scales and Preliminary Tests of Reliability and Validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E. User’s Manual for the SF-36v2 Health Survey; Quality Metric: Lincoln, RI, USA, 2008. [Google Scholar]
- Ware, J.E.; Gandek, B.; Kosinski, M.; Aaronson, N.K.; Apolone, G.; Brazier, J.; Bullinger, M.; Kaasa, S.; Leplège, A.; Prieto, L.; et al. The equivalence of SF-36 summary health scores estimated using standard and country-specific algorithms in 10 countries: Results from the IQOLA project. J. Clin. Epidemiol. 1998, 51, 1167–1170. [Google Scholar] [CrossRef]
- Healy, G.N.; Winkler, E.A.H.; Eakin, E.G.; Owen, N.; Lamontagne, A.D.; Moodie, M.; Dunstan, D.W. A Cluster RCT to Reduce Workers’ Sitting Time: Impact on Cardiometabolic Biomarkers. Med. Sci. Sports Exerc. 2017, 49, 2032–2039. [Google Scholar] [CrossRef] [PubMed]
- Gilson, N.D.; Burton, N.W.; van Uffelen, J.G.; Brown, W.J. Occupational sitting time: Employees? perceptions of health risks and intervention strategies. Health Promot. J. Aust. 2011, 22, 38–43. [Google Scholar] [CrossRef]
- Edmunds, S.; Clow, A. The role of peer physical activity champions in the workplace: A qualitative study. Perspect. Public Health 2016, 136, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Brakenridge, C.L.; Fjeldsoe, B.S.; Young, D.C.; Winkler, E.A.; Dunstan, D.W.; Straker, L.M.; Brakenridge, C.J.; Healy, G.N. Organizational-Level Strategies With or Without an Activity Tracker to Reduce Office Workers’ Sitting Time: Rationale and Study Design of a Pilot Cluster-Randomized Trial. JMIR Res. Protoc. 2016, 5, e73. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, L.; Pedersen, S.; Cooley, D. The effect of education on compliance to a workplace health and wellbeing intervention: Closing the loop. Univers. J. Public Health 2013, 1, 97–102. [Google Scholar]
- Gittelman, S.; Lange, V.; Cook, W.A.; Frede, S.M.; Lavrakas, P.J.; Pierce, C.; Thomas, R.K. Accounting for Social-Desirability Bias In Survey Sampling. J. Advert. Res. 2015, 55, 242–254. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Senior Team (n = 12) | Team Leaders (n = 11) | Call Agents (n = 20) |
|---|---|---|---|
| Age (years) | 40.3 ± 9.9 | 38.6 ± 12.2 | 41.1 ± 15.3 |
| Female | 7 (58) | 5 (45) | 10 (50) |
| White British | 12 (100) | 10 (91) | 19 (95) |
| Single | 3 (25) | 5 (45) | 15 (75) |
| Full-time employment | 9 (75) | 9 (82) | 15 (75) |
| Tertiary education | 10 (83) | 5 (45) | 10 (50) |
| Tenure (≥3 years) | 6 (50) | 9 (82) | 3 (15) |
| Physical health summary (%) | 52 ± 10 (28–65) | 53 ± 4 (47–58) | 49 ± 9 (30–65) |
| Mental health summary (%) | 51 ± 6 (38–57) | 44 ± 10 (31–50) | 47 ± 10 (24–66) |
| Total PA (MET min·week) | 869 (563) | 1609 (1428) | 964 (1125) |
| Occupational sitting time (min·day) | 390.0 ± 111.4 | 333.0 ± 122.8 | 419.4 ± 57.1 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morris, A.; Murphy, R.; Shepherd, S.; Graves, L. Multi-Stakeholder Perspectives of Factors That Influence Contact Centre Call Agents’ Workplace Physical Activity and Sedentary Behaviour. Int. J. Environ. Res. Public Health 2018, 15, 1484. https://doi.org/10.3390/ijerph15071484
Morris A, Murphy R, Shepherd S, Graves L. Multi-Stakeholder Perspectives of Factors That Influence Contact Centre Call Agents’ Workplace Physical Activity and Sedentary Behaviour. International Journal of Environmental Research and Public Health. 2018; 15(7):1484. https://doi.org/10.3390/ijerph15071484
Chicago/Turabian StyleMorris, Abigail, Rebecca Murphy, Sam Shepherd, and Lee Graves. 2018. "Multi-Stakeholder Perspectives of Factors That Influence Contact Centre Call Agents’ Workplace Physical Activity and Sedentary Behaviour" International Journal of Environmental Research and Public Health 15, no. 7: 1484. https://doi.org/10.3390/ijerph15071484