Does a Classroom Standing Desk Intervention Modify Standing and Sitting Behaviour and Musculoskeletal Symptoms during School Time and Physical Activity during Waking Time?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Outcome Measures
2.3.1. Accelerometer Data
2.3.2. Musculoskeletal Discomfort
2.4. Analysis
3. Results
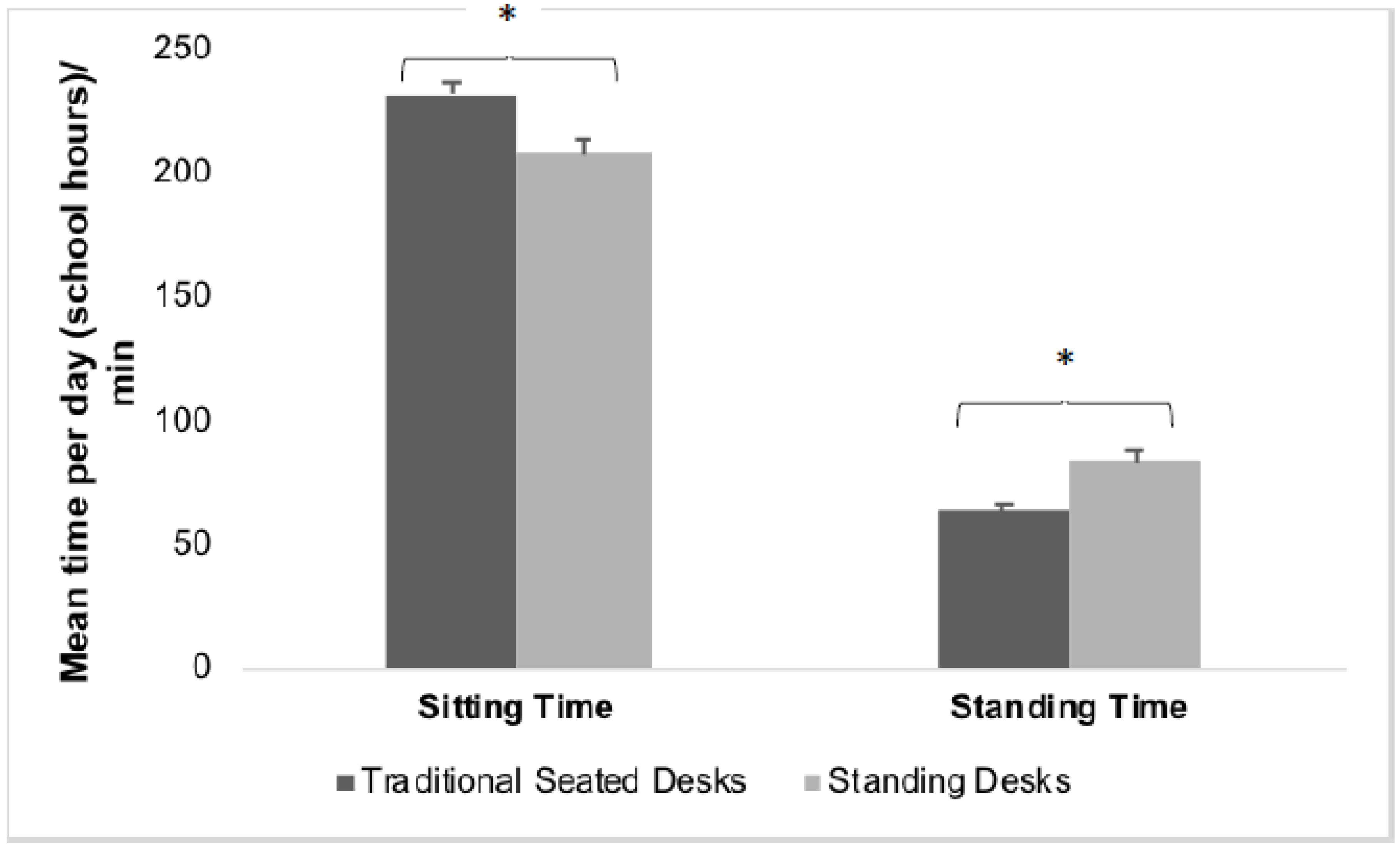
3.1. School Standing and Sitting Time
3.2. Whole Day Physical Activity and Sedentary Time
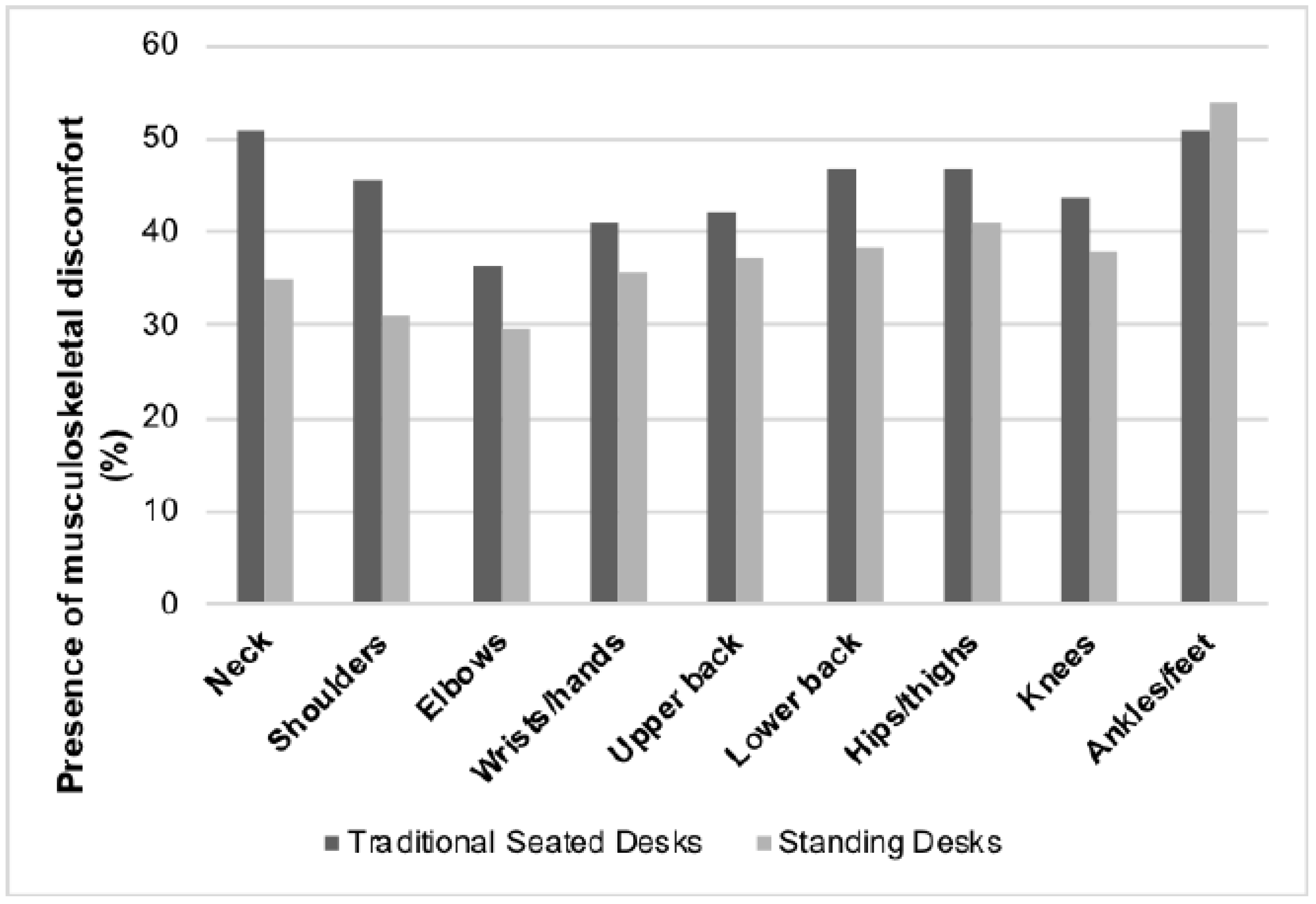
3.3. Musculoskeletal Discomfort
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Australia’s Physical Activity and Sedentary Behaviour Guidelines. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-strateg-phys-act-guidelines (accessed on 1 July 2018).
- Straker, L.M.; Howie, E.K.; Cliff, D.P.; Davern, M.T.; Engelen, L.; Gomersall, S.; Ziviani, J.; Schranz, N.K.; Olds, T.; Tomkinson, G.R. Australia and other nations are failing to meet sedentary behaviour guidelines for children: Implications and a way forward. J. Phys. Act. Health 2016, 13, 177–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, B.M.; Pate, R.R.; Troiano, R.P. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am. J. Epidemiol. 2008, 167, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Colley, R.C.; Garriguet, D.; Janssen, I.; Craig, C.L.; Clarke, J.; Tremblay, M.S. Physical activity of Canadian children and youth: Accelerometer results from the 2007 to 2009 Canadian health measures survey. Health Rep. 2011, 22, 15–23. [Google Scholar] [PubMed]
- Tremblay, M.S.; LeBlanc, A.G.; Kho, M.E.; Saunders, T.J.; Larouche, R.; Colley, R.C.; Goldfield, G.; Gorber, S.C. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hancox, R.J.; Milne, B.J.; Poulton, R. Association between child and adolescent television viewing and adult health: A longitudinal birth cohort study. Lancet 2004, 364, 257–262. [Google Scholar] [CrossRef]
- Biddle, S.J.; Pearson, N.; Ross, G.M.; Braithwaite, R. Tracking of sedentary behaviours of young people: A systematic review. Prev. Med. 2010, 51, 345–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary behavior research network (SBRN)—Terminology consensus project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gomez, D.; Eisenmann, J.C.; Healy, G.N.; Gomez-Martinez, S.; Diaz, L.E.; Dunstan, D.W.; Veiga, O.L.; Marcos, A. Sedentary behaviors and emerging cardiometabolic biomarkers in adolescents. J. Pediatr. 2012, 160, 104–110.e2. [Google Scholar] [CrossRef] [PubMed]
- Sardinha, L.B.; Andersen, L.B.; Anderssen, S.A.; Quitério, A.L.; Ornelas, R.; Froberg, K.; Riddoch, C.J.; Ekelund, U. Objectively measured time spent sedentary is associated with insulin resistance independent of overall and central body fat in 9- to 10-year-old Portuguese children. Diabetes Care 2008, 31, 569–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lajous, M.; Chavarro, J.; Peterson, K.E.; Hernández-Prado, B.; Cruz-Valdéz, A.; Hernández-Ávila, M.; Lazcano-Ponce, E. Screen time and adiposity in adolescents in Mexico. Public Health Nutr. 2009, 12, 1938–1945. [Google Scholar] [CrossRef] [PubMed]
- Russ, S.A.; Larson, K.; Franke, T.M.; Halfon, N. Associations between media use and health in US children. Acad. Pediatr. 2009, 9, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Sibley, B.A.; Etnier, J.L. The relationship between physical activity and cognition in children: A meta-analysis. Pediatr. Exerc. Sci. 2003, 15, 243–256. [Google Scholar] [CrossRef]
- Hakala, P.T.; Rimpelä, A.H.; Saarni, L.A.; Salminen, J.J. Frequent computer-related activities increase the risk of neck–shoulder and low back pain in adolescents. Eur. J. Public Health 2006, 16, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, K.; Hudak, S.; McGiffert, J. Computer-related posture and musculoskeletal discomfort in middle school students. Work 2009, 32, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Torsheim, T.; Eriksson, L.; Schnohr, C.W.; Hansen, F.; Bjarnason, T.; Välimaa, R. Screen-based activities and physical complaints among adolescents from the Nordic countries. BMC Public Health 2010, 10, 324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Straker, L.M.; Coleman, J.; Skoss, R.; Maslen, B.A.; Burgess-Limerick, R.; Pollock, C.M. A comparison of posture and muscle activity during tablet computer, desktop computer and paper use by young children. Ergonomics 2008, 51, 540–555. [Google Scholar] [CrossRef] [PubMed]
- Brattberg, G. Do pain problems in young school children persist into early adulthood? A 13-year follow-up. Eur. J. Pain 2004, 8, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Mooses, K.; Mäestu, J.; Riso, E.; Hannus, A.; Mooses, M.; Kaasik, P.; Kull, M. Different methods yielded two-fold difference in compliance with physical activity guidelines on school days. PLoS ONE 2016, 11, e0152323. [Google Scholar] [CrossRef] [PubMed]
- Bailey, D.P.; Fairclough, S.J.; Savory, L.A.; Denton, S.J.; Pang, D.; Deane, C.S.; Kerr, C.J. Accelerometry-assessed sedentary behaviour and physical activity levels during the segmented school day in 10–14-year-old children: The happy study. Eur. J. Pediatr. 2012, 171, 1805–1813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, J.E.; Greene, J.L.; Gibson, C.A.; Smith, B.K.; Washburn, R.A.; Sullivan, D.K.; DuBose, K.D.; Mayo, M.S.; Schmelzle, K.H.; Ryan, J.J.; et al. Physical activity across the curriculum (PAAC): A randomized controlled trial to promote physical activity and diminish overweight and obesity in elementary school children. Prev. Med. 2009, 49, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.A.; Smith, B.K.; DuBose, K.D.; Greene, J.L.; Bailey, B.W.; Williams, S.L.; Ryan, J.J.; Schmelzle, K.H.; Washburn, R.A.; Sullivan, D.K.; et al. Physical activity across the curriculum: Year one process evaluation results. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 36. [Google Scholar] [CrossRef] [PubMed]
- Erwin, H.E.; Beighle, A.; Morgan, C.F.; Noland, M. Effect of a low-cost, teacher-directed classroom intervention on elementary students’ physical activity. J. Sch. Health 2011, 81, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Naylor, P.; Nettlefold, L.; Race, D.; Hoy, C.; Ashe, M.C.; Wharf Higgins, J.; McKay, H.A. Implementation of school based physical activity interventions: A systematic review. Prev. Med. 2015, 72, 95–115. [Google Scholar] [CrossRef] [PubMed]
- Kober, N.; Rentner, D. Strained Schools Face Bleak Future: Districts Foresee Budget Cuts, Teacher Layoffs, and a Slowing of Education Reform Efforts; Center on Education Policy: Washington, DC, USA, 2011. [Google Scholar]
- Dwyer, J.J.; Allison, K.R.; Barrera, M.; Hansen, B.; Goldenberg, E.; Boutilier, M.A. Teachers’ perspective on barriers to implementing physical activity curriculum guidelines for schoolchildren in Toronto. Can. J. Public Health 2003, 94, 448–452. [Google Scholar] [PubMed]
- Hammerschmidt, P.; Tackett, W.; Golzynski, M.; Golzynski, D. Barriers to and facilitators of healthful eating and physical activity in low-income schools. J. Nutr. Educ. Behav. 2011, 43, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Lees, C.; Hopkins, J. Effect of aerobic exercise on cognition, academic achievement, and psychosocial function in children: A systematic review of randomized control trials. Prev. Chronic Dis. 2013, 10, E174. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.K.; Shortz, A.E.; Benden, M.E. Standing up for learning: A pilot investigation on the neurocognitive benefits of stand-biased school desks. Int. J. Environ. Res. Public Health 2015, 13, 59. [Google Scholar] [CrossRef] [PubMed]
- Minges, K.E.; Chao, A.M.; Irwin, M.L.; Owen, N.; Park, C.; Whittemore, R.; Salmon, J. Classroom standing desks and sedentary behavior: A systematic review. Pediatrics 2016, 137, e20153087. [Google Scholar] [CrossRef] [PubMed]
- Cardon, G.; De Clercq, D.; De Bourdeaudhuij, I.; Breithecker, D. Sitting habits in elementary schoolchildren: A traditional versus a “moving school”. Patient Educ. Couns. 2004, 54, 133–142. [Google Scholar] [CrossRef]
- Aminian, S.; Hinckson, E.A.; Stewart, T. Modifying the classroom environment to increase standing and reduce sitting. Build. Res. Inf. 2015, 43, 631–645. [Google Scholar] [CrossRef]
- Coenen, P.; Willenberg, L.; Parry, S.; Shi, J.W.; Romero, L.; Blackwood, D.M.; Maher, C.G.; Healy, G.N.; Dunstan, D.W.; Straker, L.M. Associations of occupational standing with musculoskeletal symptoms: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, A.V. Accelerometer assessment of physical activity in children: An update. Pediatr. Exerc. Sci. 2007, 19, 252–266. [Google Scholar] [CrossRef] [PubMed]
- Steeves, J.A.; Bowles, H.R.; McClain, J.J.; Dodd, K.W.; Brychta, R.J.; Wang, J.; Chen, K.Y. Ability of thigh-worn actigraph and activpal monitors to classify posture and motion. Med. Sci. Sports Exerc. 2015, 47, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Edwardson, C.L.; Rowlands, A.V.; Bunnewell, S.; Sanders, J.; Esliger, D.W.; Gorely, T.; O’Connell, S.; Davies, M.; Khunti, K.; Yates, T. Accuracy of posture allocation algorithms for thigh- and waist-worn accelerometers. Med. Sci. Sports Exerc. 2016, 48, 1085–1090. [Google Scholar] [CrossRef] [PubMed]
- Borghese, M.M.; Tremblay, M.S.; LeBlanc, A.G.; Leduc, G.; Boyer, C.; Chaput, J.P. Comparison of Actigraph GT3X+ and Actical accelerometer data in 9–11-year-old Canadian children. J. Sports Sci. 2017, 35, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Robusto, K.M.; Trost, S.G. Comparison of three generations of Actigraph™ activity monitors in children and adolescents. J. Sports Sci. 2012, 30, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- McVeigh, J.A.; Winkler, E.A.H.; Healy, G.N.; Slater, J.; Eastwood, P.R.; Straker, L.M. Validity of an automated algorithm to identify waking and in-bed wear time in hip-worn accelerometer data collected with a 24 h wear protocol in young adults. Physiol. Meas. 2016, 37, 1636–1652. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Rich, C.; Geraci, M.; Griffiths, L.; Sera, F.; Dezateux, C.; Cortina-Borja, M. Quality control methods in accelerometer data processing: Defining minimum wear time. PLoS ONE 2013, 8, e67206. [Google Scholar] [CrossRef] [PubMed]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Hinckson, E.A.; Aminian, S.; Ikeda, E.; Stewart, T.; Oliver, M.; Duncan, S.; Schofield, G. Acceptability of standing workstations in elementary schools: A pilot study. Prev. Med. 2013, 56, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Straker, L.M. Body discomfort assessment tools. In The Occupational Ergonomics Handbook; Karwowski, W., Marras, W.S., Eds.; CRC Press: Boca Raton, FL, USA, 1999; pp. 1239–1252. [Google Scholar]
- Clemes, S.A.; Barber, S.E.; Bingham, D.D.; Ridgers, N.D.; Fletcher, E.; Pearson, N.; Salmon, J.; Dunstan, D.W. Reducing children’s classroom sitting time using sit-to-stand desks: Findings from pilot studies in UK and Australian primary schools. J. Public Health 2016, 38, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Koepp, G.A.; Snedden, B.J.; Flynn, L.; Puccinelli, D.; Huntsman, B.; Levine, J.A. Feasibility analysis of standing desks for sixth graders. Infant Child Adolesc. Nutr. 2012, 4, 89–92. [Google Scholar] [CrossRef]
- Gomersall, S.R.; Rowlands, A.V.; English, C.; Maher, C.G.; Olds, T.S. The activitystat hypothesis. Sports Med. 2013, 43, 135–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkin, T.J. Can we modulate physical activity in children? Int J. Obes. 2011, 35, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Long, M.W.; Sobol, A.M.; Cradock, A.L.; Subramanian, S.V.; Blendon, R.J.; Gortmaker, S.L. School-day and overall physical activity among youth. Am. J. Prev. Med. 2013, 45, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Brink, Y.; Louw, Q.A.; Grimmer, K.; Jordaan, E. The relationship between sitting posture and seated-related upper quadrant musculoskeletal pain in computing South African adolescents: A prospective study. Man. Ther. 2015, 20, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Brink, Y.; Crous, L.C.; Louw, Q.A.; Grimmer-Somers, K.; Schreve, K. The association between postural alignment and psychosocial factors to upper quadrant pain in high school students: A prospective study. Man. Ther. 2009, 14, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Straker, L.; Mathiassen, S.E. Increased physical work loads in modern work—A necessity for better health and performance? Ergonomics 2009, 52, 1215–1225. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean (SE) (Waking Time) | Standing Desks | Seated Desks | p-Value | |
|---|---|---|---|---|
| Mean (SD) number of wear days | 4 (2) | 4 (2) | ||
| Mean (SD) total waking time/day (min) | 972 (160) | 1004 (167) | ||
| Sedentary | Min/day | 674 (23) | 686 (26) | 0.790 |
| Percentage/day | 68.7 (1.1) | 67.3 (1.3) | ||
| Light Activity | Min/day | 241 (7) | 256 (6) | 0.111 |
| Percentage/day | 25.3 (0.8) | 26.2 (0.9) | ||
| Moderate Activity | Min/day | 39 (2) | 42 (2) | 0.260 |
| Percentage/day | 4.1 (0.2) | 4.4 (0.3) | ||
| Vigorous Activity | Min/day | 18 (1) | 20 (1) | 0.330 |
| Percentage/day | 2.1 (0.3) | 2.0 (0.2) | ||
| Body Part | Condition | Transformed Pain Scores Using a Zero One Inflated Beta Distribution | Logistic Regression on Pain Indicator | ||||||
|---|---|---|---|---|---|---|---|---|---|
| B Coefficient (Pain Score) | SE(B) | Predicted Mean | 95% CI Mean | p-Value | OR (Outcome = Any Pain) | 95%CI OR | p-Value | ||
| Neck | Sit | 1.31 | 0.81–1.81 | 1.00 | |||||
| Stand | −0.280 | 0.100 | 1.10 | 0.67–1.60 | 0.005 | 0.52 | 0.41–0.67 | <0.001 | |
| Shoulders | Sit | 1.23 | 0.68–1.79 | 1.00 | |||||
| Stand | −0.150 | 0.102 | 1.13 | 0.67–1.60 | 0.142 | 0.54 | 0.42–0.70 | <0.001 | |
| Elbows | Sit | 1.02 | 0.55–1.49 | 1.00 | |||||
| Stand | −0.092 | 0.106 | 0.97 | 0.50–1.45 | 0.384 | 0.74 | 0.57–0.96 | 0.023 | |
| Wrists/hands | Sit | 1.25 | 0.69–1.82 | 1.00 | |||||
| Stand | −0.084 | 0.104 | 1.20 | 0.68–1.71 | 0.419 | 0.80 | 0.62–1.03 | 0.089 | |
| Upper back | Sit | 1.30 | 0.83–1.77 | 1.00 | |||||
| Stand | −0.132 | 0.100 | 1.21 | 0.74–1.68 | 0.189 | 0.81 | 0.63–1.04 | 0.103 | |
| Lower back | Sit | 1.42 | 0.85–1.98 | 1.00 | |||||
| Stand | −0.111 | 0.103 | 1.33 | 0.80–1.86 | 0.281 | 0.71 | 0.55–0.91 | 0.007 | |
| Hips/thighs | Sit | 1.53 | 0.98–2.08 | 1.00 | |||||
| Stand | −0.177 | 0.097 | 1.38 | 0.90–1.87 | 0.07 | 0.79 | 0.62–1.02 | 0.070 | |
| Knees | Sit | 1.40 | 0.79–2.02 | 1.00 | |||||
| Stand | −0.172 | 0.121 | 1.28 | 0.77–1.79 | 0.156 | 0.80 | 0.62–1.03 | 0.079 | |
| Ankles/feet | Sit | 2.07 | 1.38–2.76 | 1.00 | |||||
| Stand | −0.179 | 0.123 | 1.90 | 1.28–2.52 | 0.145 | 1.12 | 0.88–1.44 | 0.350 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ee, J.; Parry, S.; IR de Oliveira, B.; McVeigh, J.A.; Howie, E.; Straker, L. Does a Classroom Standing Desk Intervention Modify Standing and Sitting Behaviour and Musculoskeletal Symptoms during School Time and Physical Activity during Waking Time? Int. J. Environ. Res. Public Health 2018, 15, 1668. https://doi.org/10.3390/ijerph15081668
Ee J, Parry S, IR de Oliveira B, McVeigh JA, Howie E, Straker L. Does a Classroom Standing Desk Intervention Modify Standing and Sitting Behaviour and Musculoskeletal Symptoms during School Time and Physical Activity during Waking Time? International Journal of Environmental Research and Public Health. 2018; 15(8):1668. https://doi.org/10.3390/ijerph15081668
Chicago/Turabian StyleEe, Jolyn, Sharon Parry, Beatriz IR de Oliveira, Joanne A. McVeigh, Erin Howie, and Leon Straker. 2018. "Does a Classroom Standing Desk Intervention Modify Standing and Sitting Behaviour and Musculoskeletal Symptoms during School Time and Physical Activity during Waking Time?" International Journal of Environmental Research and Public Health 15, no. 8: 1668. https://doi.org/10.3390/ijerph15081668