1. Introduction
Obesity is a serious public health problem that needs to be addressed urgently both in developed and developing countries [
1,
2,
3,
4]. Along with economic development and social changes, the epidemic of obesity is rapidly growing among men and women in China [
5]. According to the Chinese Nutrition and Chronic Disease Survey report in 2015, the obesity rates among men and women were 12.1% and 14.4%, respectively. Moreover, excessive body weight is an important risk factor for mortality and morbidity from cardiovascular diseases, type-2 diabetes, musculoskeletal disorders, and cancers, causing nearly 3 million deaths annually worldwide [
6,
7,
8]. There is a myriad of studies that have tried to address the role of insurance in obesity rates over the past decades. While there is no argument that genetic predisposition plays an important role in obesity, the increase in obesity is mostly attributed to lifestyle choices and environmental factors, including a high-fat food dietary preference and a shift toward a sedentary lifestyle, and sex may play a role in such an association [
9]. These lifestyle choices may be driven in part by the moral hazard effect.
Economic theories have indicated that an insurance-related ex ante moral hazard causes a reduction in self-protection behaviors and in turn leads to obesity [
10,
11]. While expanding universal health insurance coverage has been the primary health policy in health care reform around the world in recent years, the question of whether health insurance matters for health has long been a central issue for debate. Previous studies have suggested that rural residents are more often overweight and obese than urban residents [
12,
13,
14,
15]. Although those living outside of urban areas tend to be of lower socioeconomic position [
16,
17], rurality increases the risk of being overweight or obese independent of compositional factors, such as age, education, income, and marital status [
13,
14]. This suggests that the rural context has an important role to play in obesity development. In the rural areas of China, the rapid increase of the New Rural Cooperative Medical Insurance (NRCMS) coverage rate is certainly striking. The key issue, however, is whether it would result in an improvement in the health of its participants.
China’s health care system did not match its rapid economic development during the same period. To bridge this gap, the Chinese government has substantially reformed its health care system in recent years [
18,
19]. The goal is to provide universal coverage for basic health care to every Chinese citizen. However, it has been shown that health insurance could have negative outcomes and can lead to deadweight loss in social welfare. Rural residents make up almost half of China’s total population. Mortality in the rural population is also substantially higher than that in the urban population. In addition, a higher proportion of rural residents are below the average poverty levels compared with urban residents. Therefore, it is meaningful to study the effect of the NRCMS on the health of Chinese rural residents.
Evidence addressing the causal effect of insurance on the risk of obesity in rural areas is sparse, so more study is warranted. The main challenge for evaluating the effects of health insurance on obesity risk is the endogeneity problem caused by simultaneity and omitted variables. Endogeneity refers to the fact that an explanatory variable is correlated with unobservable heterogeneity that is relegated to an error term. Several studies to date have adopted different econometric approaches to deal with these issues. Courbage and Coulon used an instrumental variable (IV) approach to explore the effect of as one method for controlling the unobservable heterogeneity that jointly determines health insurance and health behavior [
20]. Anderson used data from the U.S. Panel Study of Income Dynamics (1991–2003) to estimate a structural model and found that health insurance has significant incentive effects of unhealthy lifestyle choices, all of which have been shown by the medical literature to cause serious long-term health damage [
21].
This study attempts to fill the theoretical and practical gap by exploring the effects of the NRCMS scheme on the risk of obesity in rural China while correcting for underlying endogeneity. Our instrument for a respondent’s NRCMS health insurance status is the data of county-level NRCMS inception, an instrument used in the previous literature to estimate the impact of NRCMS on health status and the utilization of preventive care [
22]. We attempt to isolate the effects of an “ex ante moral hazard”, where people with insurance may change their lifestyle choices towards weight control. This study utilizes the China Health and Nutrition Survey (CHNS, 2004–2011), a nation-wide longitudinal survey including the whole period of the NRCMS, to analyze the impact of the NRCMS. With the advantage of updated and comprehensive data, our findings may also be meaningful to other developing countries facing similar challenges on the way to establishing universal health insurance coverage.
3. Statistical Analysis
Statistical analyses were performed using STATA 13.0 (STATA, Stata Corp, College Station, TX, USA). The values were reported as means and standard errors for continuous variables or as proportions of the total for categorical variables. We subdivided data according to different demographic characteristics. Among all the variables, we adjusted age, sedentary activity time, daily calorie intake, the share of calories from carbohydrate, and the share of calories from fat as continuous variables and gender, drinking, smoking, education level, marital status, employment status, general obesity, and abdominal obesity as dummy variables.
To investigate the effects of NRCMS on lifestyle behaviors, we first employed a pooled ordinary least square (OLS) model covering the whole period 2004–2011. The equation we used for this model is
where
yipt denotes the heath behavior of individual
i in province
p and year
t. This includes such outcome variables as sedentary time, daily calorie intake, and the proportion of carbohydrates, protein, and fat in total calorie intake.
NRCMSipt is a dummy variable (taking on a value 0 or 1) indicating whether the individual is enrolled in NRCMS in year
t;
Xipt contains a set of control variables including age, education level, income level, marital status, and employment status;
δt indicates time fixed-effects that control for the unobservable characteristics that are constant across all regions; α
p indicates province fixed-effects that control for unobservable characteristics of a province that are constant over time; and
εipt is the random error that varies with individual, province, and year. The parameter
α1 indicates the impact of the NRCMS on the participant’s health behaviors, thus it is the coefficient of interest.
Where our dependent variables were binary, we also estimated a probit model and report the average marginal effects. This includes such outcome variables as whether the respondent currently drinks spirits, smokes, has general obesity, or has abdominal obesity. This is to characterize the potentially non-linear impact of insurance and to avoid the problem of natural heteroscedasticity with OLS. The probit model takes on the following form:
where
yipt is a dummy indicating whether individual
i in province
p and year
t smokes, drinks, is sedentary, has general obesity, or has abdominal obesity.
y′ipt is the latent variable specifying the tendency of such behaviors. If
y′ipt > 0, then
yipt = 1; otherwise
yipt = 0.
G is the cumulative distribution function of random error
εipt. Unlike the OLS model in Equation (1), the
α1 in the probit model only indicates the impact of NRCMS coverage on the tendency of risk-taking (
y′ipt). To obtain the (non-linear) marginal effect of NRCMS on the observed probability of risking-taking behaviors, we use the sample average of individual marginal effects calculated by a finite-difference method.
Note that in Equations (1)–(3), the OLS and probit of α1 and α2 are still heavily biased because of endogeneity, that is, a correlation between insurance status and the error, α1.
The problem of adverse selection in the schemes creates a higher likelihood of correlation between insurance participation and the error term, which induces a bias in the coefficient of health insurance on the health behavior equation. This condition leads to a positive association between insurance status and risk of obesity, because higher health risk people are more likely to enroll in an insurance plan than others.
To address this endogeneity of NRCMS participation, we use the IV method in this paper. We constructed pooled two-stage least squares (2SLS) to calculate IV estimates for insurance status.
There are two requirements for this instrument to be valid. The first requirement is the existence of a high correlation between whether an individual is participating in an NRCMS (NRCMSipt) and whether his/her county of residence has implemented the NRCMS. The second requirement is that it should not directly impact the individual’s health-related behaviors (yipt) independent of NRCMSipt. We use whether the individual’s county of residence has implemented NRCMS in the survey year (Countryipt) as the IV for individual insurance participation. As China’s NRCMS campaign was implemented at the county level after its initiation in 2003, and rural residents could only join the NRCMS after the programme was adopted in her county of residence, there should be a strong correlation between individual participation and county enrollment. In addition, the timing of a county’s NRCMS implementation is centrally planned by the Ministry of Health of China and provincial health bureaus; thus, it is not likely to directly influence the individual health behavior independent of the insurance channel.
The Hausman test was conducted to measure the exogenous status of insurance. The power conditions of the IV are formally tested using the F values for the significance of β1 in the first-stage regressions. Moreover, we use the Basmann test of over-identification restrictions to make sure our approach and instruments are valid.
5. Discussion
Currently, obesity is widespread worldwide. The latest data on the prevalence of overweight and obese adults in 20 European countries shows that more than half of the European population is overweight and obese [
31]. In China, the prevalence of overweight and obese adults has increased rapidly due to large shifts in dietary and lifestyle factors [
32], in which there are considerable regional and gender differences due to regional disparities in social and economic development and gender disparities in physiological and lifestyle factors, etc. [
33]. The gender-specific characteristics of populations at high risk of developing obesity should be taken into consideration when designing interventional programs [
34]. Despite more than a century of research, new health risks and adverse effects have frustrated our ability to produce lasting cost-effective results. This paper explores the impact of insurance itself on lifestyle behaviors and risk of obesity in different gender groups. Using updated longitudinal data, our study provided new evidence on the effect of the NRCMS on health conditions of rural Chinese.
The expansion of health insurance is a popular public issue in China, and the Chinese government has made great efforts to launch public health programs for various populations to improve the accessibility, affordability, and quality of health care. However, health insurance is not without costs and the ex ante moral hazard problems (changing health-related behaviors) associated with insurance add to these costs. Some domestic and international preliminary explorations have linked insurance with obesity risk from the view of identifying ex ante moral hazards, but the results are inconsistent. For example, Jay Bhattacharya used data from the Rand Health Insurance experiment and found that being insured increased BMI and obesity [
35]. Ir Kelly and S. Markowitz used data from the Behavioral Risk Factor Surveillance System to determine the potential effect of having health insurance on measures of body weight and found that having insurance is associated with a higher body mass but not a higher probability of being obese [
10], consistent with the conclusion of kenkel and card [
36]. Xue Zheng Q. used data from the China health and nutrition survey and found that NRCMS participation increased unhealthy lifestyles that in turn lead to a risk of being overweight, indicating that an insurance-induced ex ante moral hazard is present in rural China [
37].
In the present study, OLS, Probit, and IV estimation are conducted to fully investigate how the NRCMS affects the lifestyle behaviors of its participants, such as dietary preference, smoking, drinking, sedentary activities, and obesity-related conditions. The sub-sample results of our study reflect noticeable gender differences in health-related behavior and obesity conditions. Besides this, our study shows that insurance coverage provides a significant incentive to consume a larger proportion of daily calories from fat but a smaller proportion from carbohydrates. Supportive evidence can be found in, for example, Shuang M., who studied the effect of the NRCMS on rural household food consumption and found that insurance participants have higher calorie, carbohydrate, fat, and protein intakes than those who are uninsured [
38]. Due to a high-calorie diet having long been considered a risk factor for being overweight or obese or having other chronic diseases, unhealthy eating habits once again show that the participation in the NRCMS may cause problems with efforts to reduce the number of self-protected people in the rural population.
The result on the positive relationship between insurance participation and the tendency for females to have an alcohol problem indicates that the NRCMS has gender-specific influences on people’s tendency towards heavy drinking. Meanwhile, the harmful consequences of alcohol consumption are well-documented. At a personal level, alcohol consumption is causally related to cardiovascular diseases, various cancers, liver diseases, and psychiatric ailments [
39]. Additionally, it is worth noting that women’s alcohol consumption may potentially affect the growth of children in a family, domestic violence, and economic instability. Some previous research, such as Andersen, found that joining catastrophic public insurance programs increases the likelihood of a person’s drinking alcohol. Our results suggest that NRCMS coverage leads to an increase in smoking behavior of males in rural China.
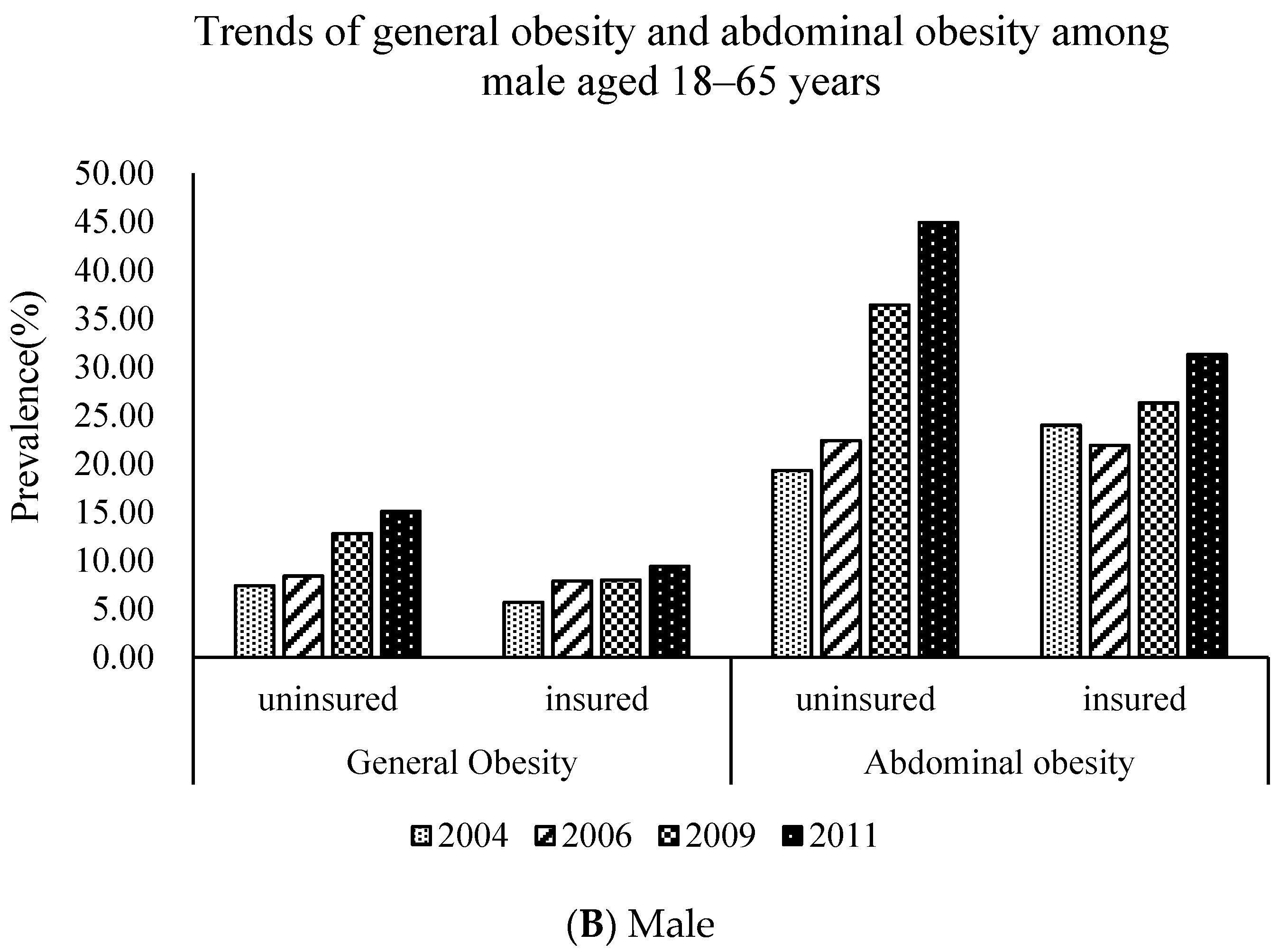
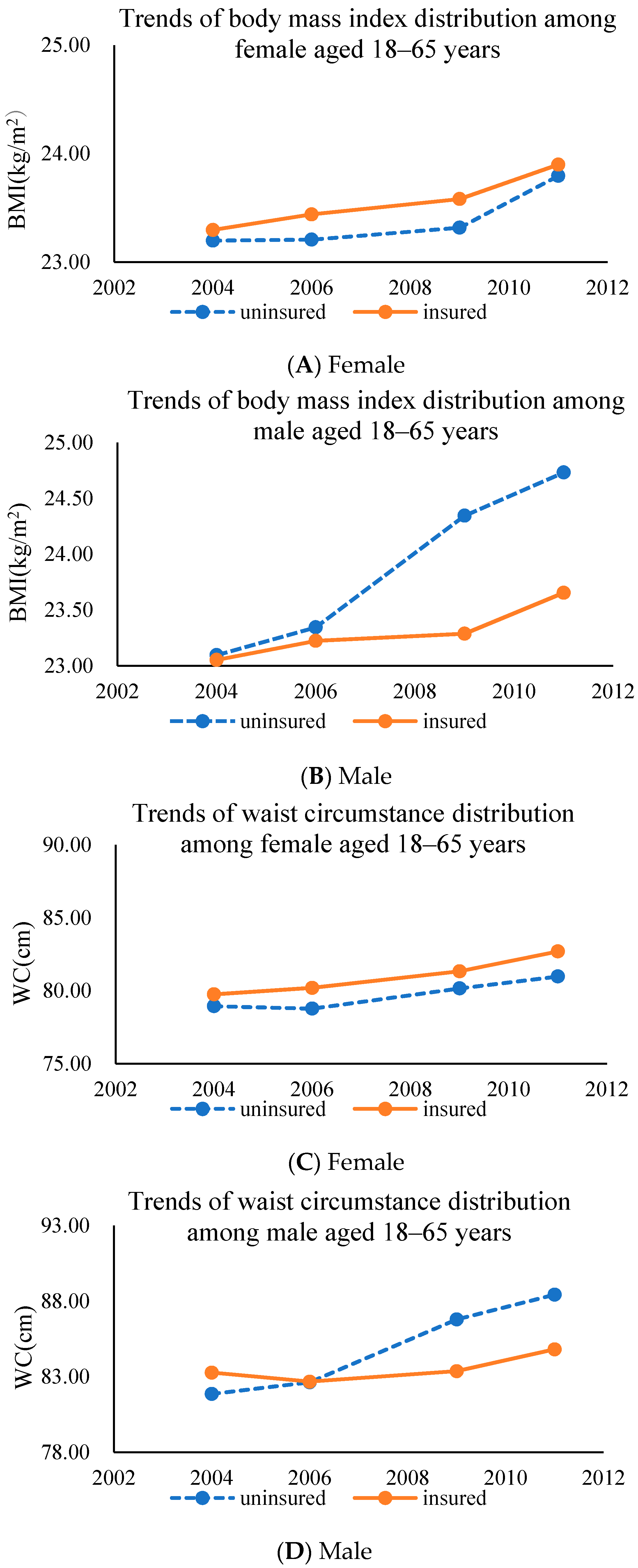
In addition, our results indicate that the coverage of the NRCMS can increase the intensity of sedentary activity, which in turn leads to higher risks of chronic diseases. This finding is also supported by Dave and Kaestner who found that receiving insurance has positive impacts on drinking and negative impacts on exercise, which is generally consistent with an increase in unhealthy behavior [
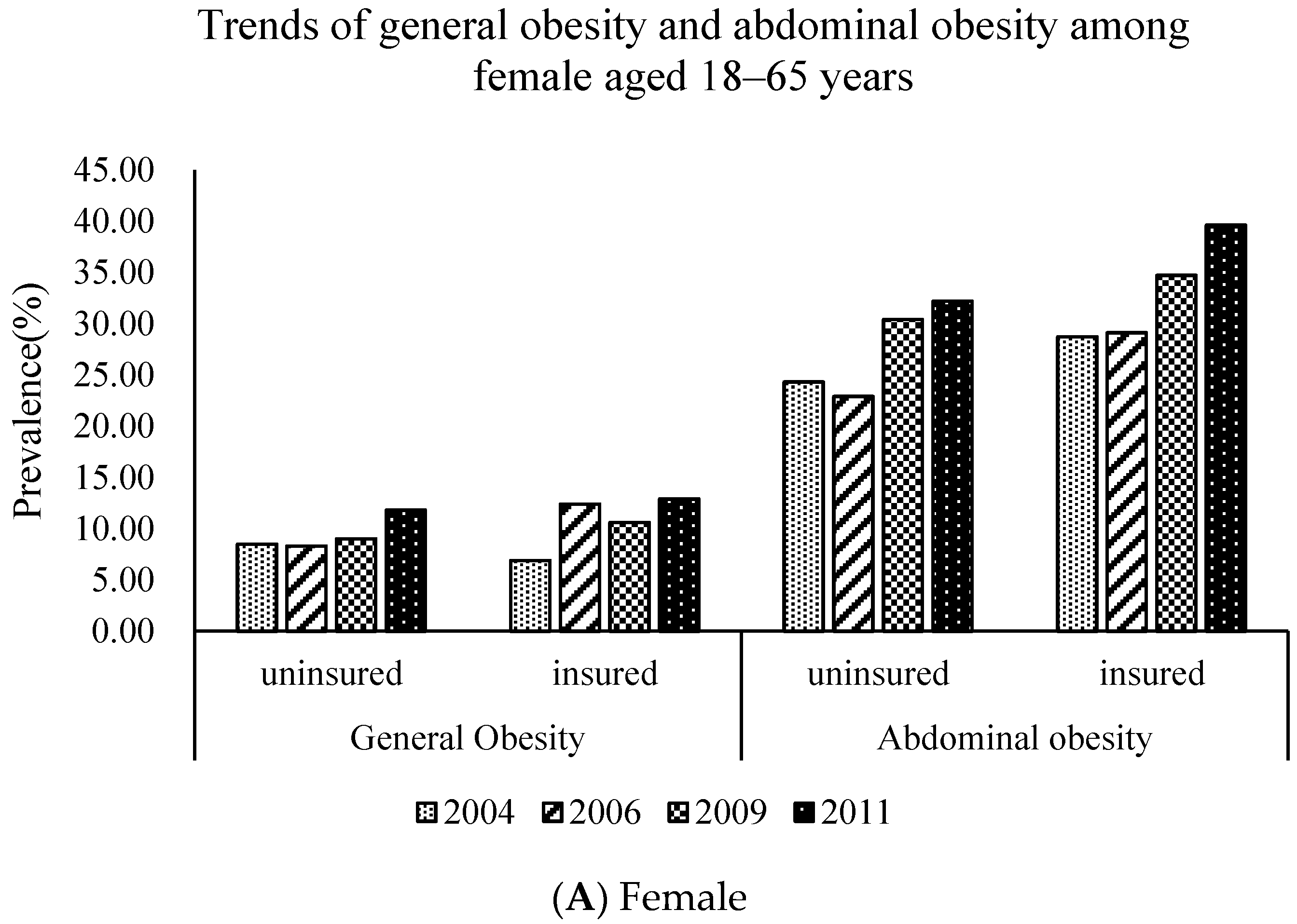
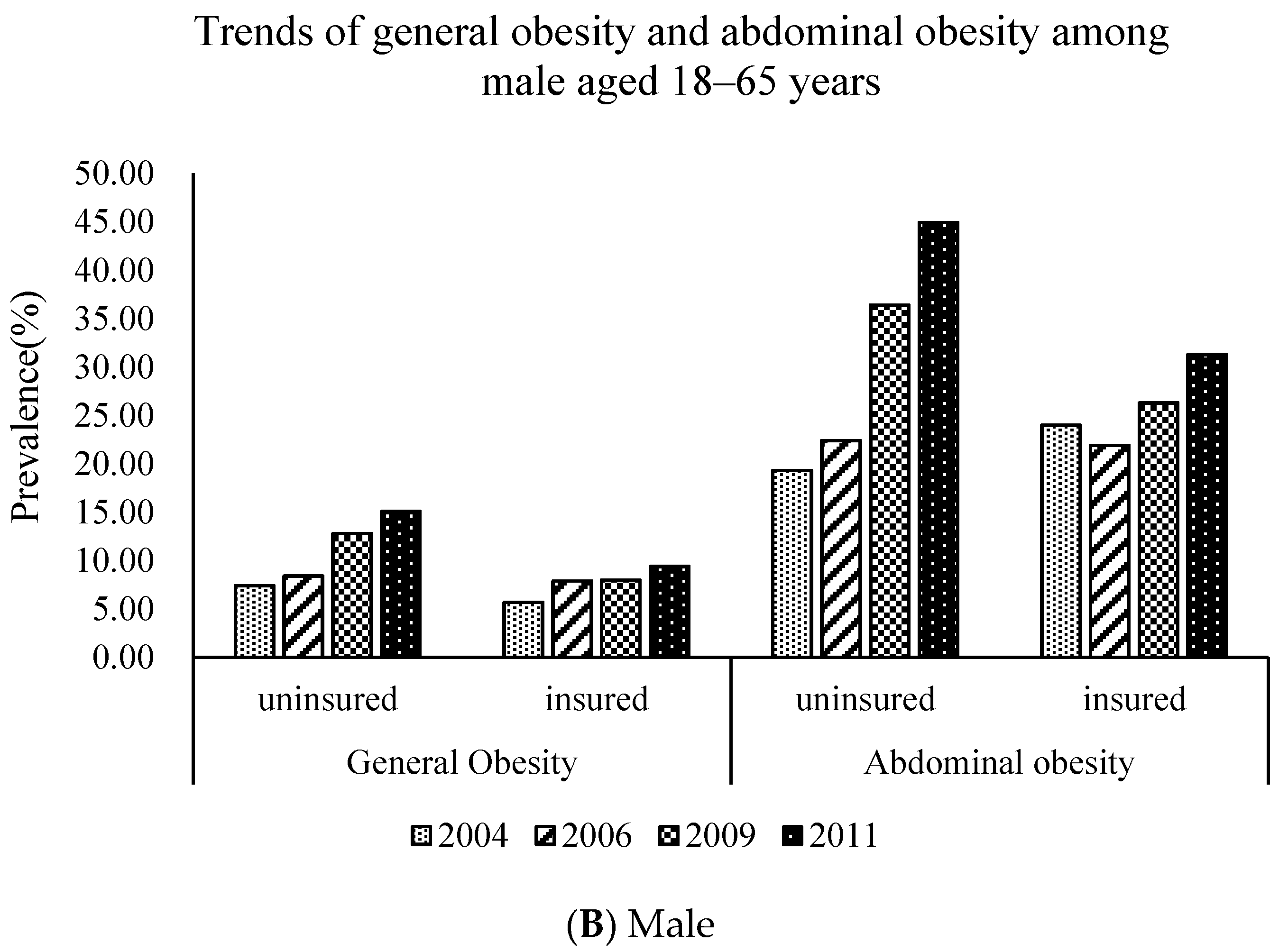
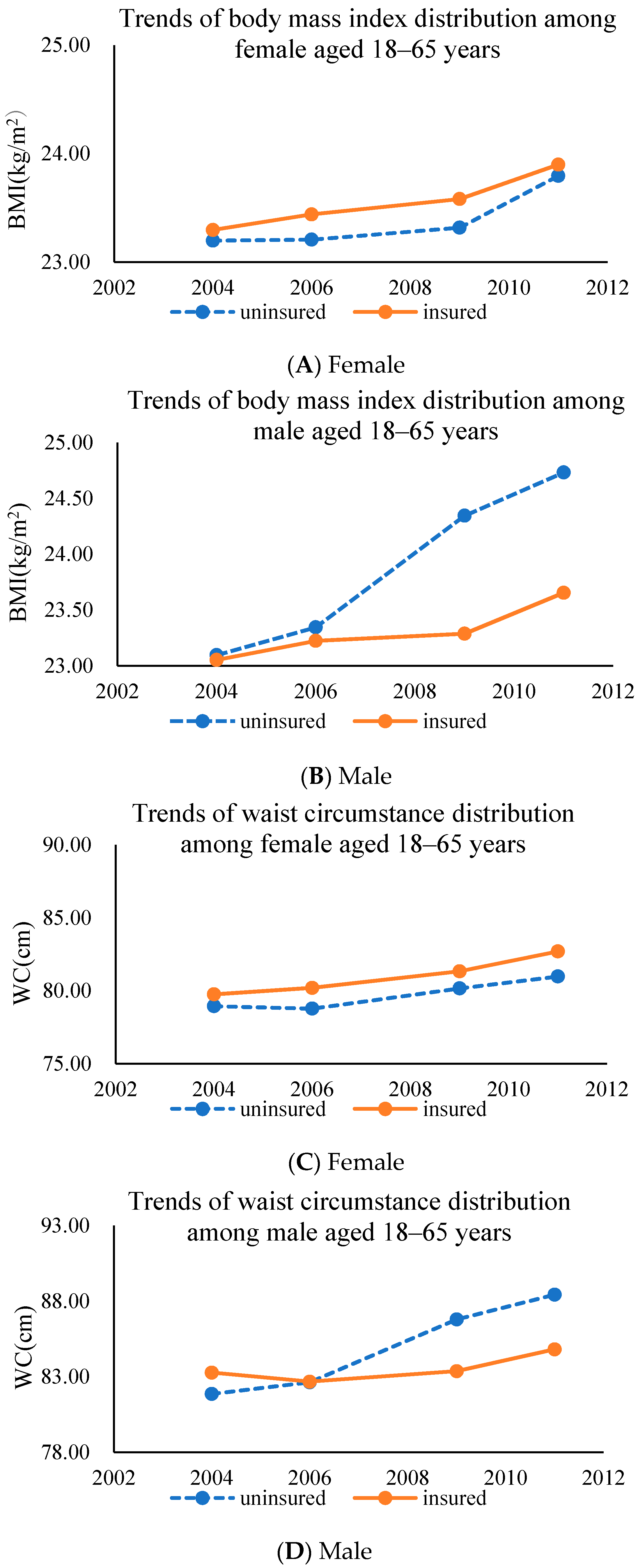
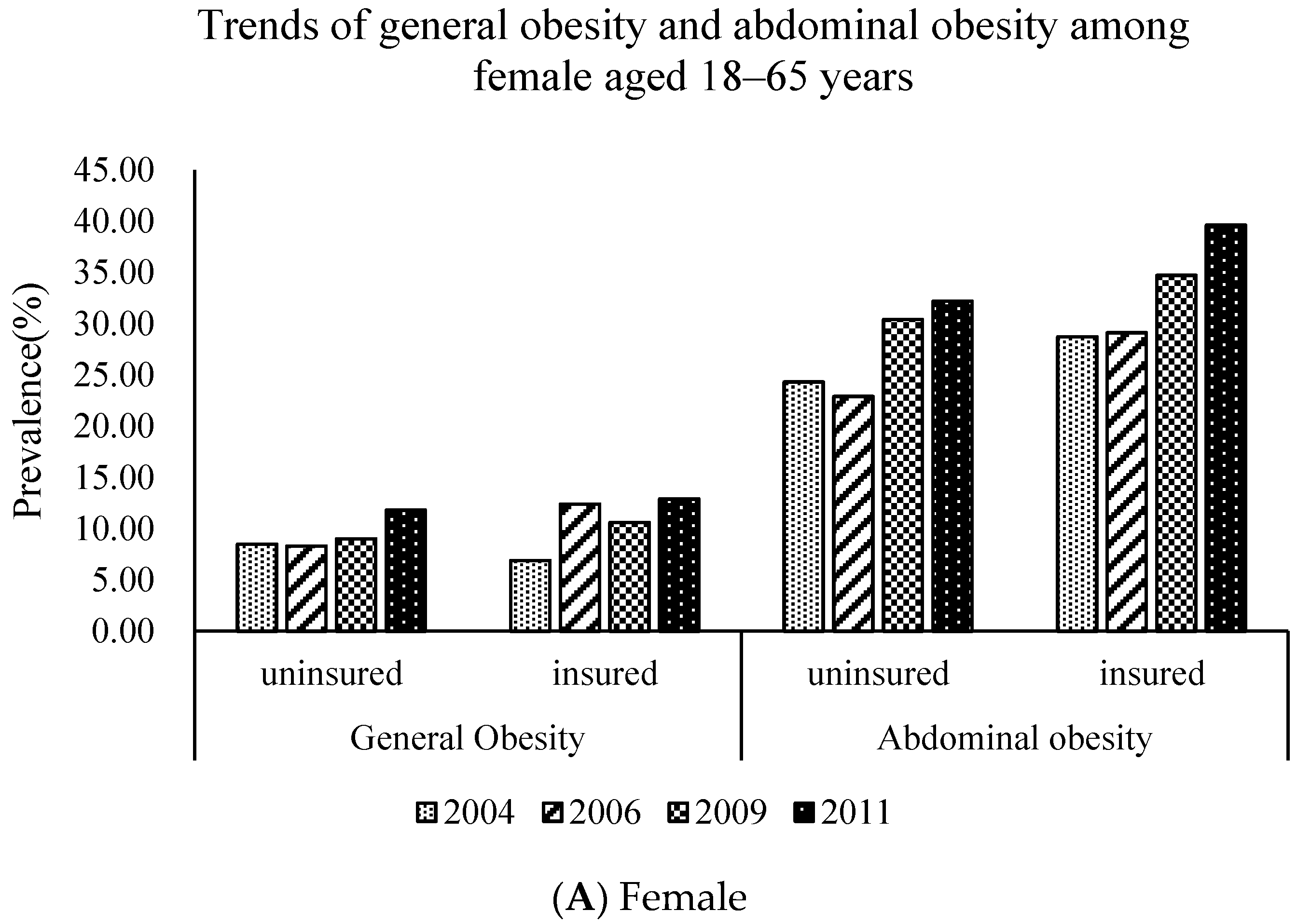
11]. Furthermore, the results reveal the positive effect of the NRCMS on general obesity (females) and abdominal obesity (males), once again proving the existence of an ex ante moral hazard in the process of NRCMS universal coverage. Our results show that the NRCMS increases the body mass index and waist circumstance. Supportive evidence can be found in, for example, Jay Bhattacharya, who used data from the Rand Health Insurance experiment and found strong evidence that being insured increases body mass index and obesity.
The present study has many strengths. First, we used updated longitudinal data to observe the dynamic aspects of NRCMS coverage with other control variables. It provides new evidence to improve reforms of the medical and health system and the integration of rural insurance systems. Second, we provide evidence of gender-specific characteristics in exploring the impact of insurance on the risk of developing obesity. Third, the sample size is large with a wide age range, and the staff were trained in the study’s methodology and standardization in different parameters at the same time by the same scientists. In addition to baseline OLS estimation and the Probit model, IV estimation modeling corrects the omitted variable bias and increases the accuracy of the estimates.
While this study provides critical insight into health insurance, it nevertheless has several limitations. First, the CHNS does not present national data, and the vast western areas (north (Heilongjiang and Liaoning), the central areas (Shandong, Jiangsu, and Henan), and the south areas (Hubei, Hunan, Guangxi, and Guizhou) of China were not included in the present study. Second, dietary data were collected using three consecutive 24-h dietary recalls, which might show relatively limited variations for a subject compared to nonconsecutive 24-h recalls. However, the average intake over 3 days can offer a relatively valid estimate of nutrient intake, as shown in an earlier study using the CHNS data [
40].




{kind=link}
{kind=link}
{kind=link}