1. Introduction
Globally air quality has deteriorated seriously in the past few decades with economic development and modern industrialization [
1,
2,
3]. Air pollution and its adverse effects on human health have drawn more global attention since the smog incident in Donora, Pennsylvania in 1948 [
4] and the killer London smog event of 1952 [
5]. Up to now, air pollution is estimated to cause 3.7 million premature deaths per year worldwide [
6]. It has become the leading global risk for public health, and most megacities in developing countries are experiencing the worst air pollution [
7]. Urban dwellers in developing countries are at higher risk of cardiovascular diseases, respiratory diseases and other illnesses [
8,
9,
10]. Due to the pressures of social and economic development, many megacities in developing countries are facing more complicated and serious environmental problems and challenges. Air pollution in urban areas is a complex mixture of particles and gas-phase pollutants arising from a myriad of sources. Most megacities in low- and middle-income level countries experience extremely high levels of both visible (particulate matter) and invisible (gases) forms of air pollution [
11,
12,
13], and their dwellers are at the highest risk [
14].
There are more than 700 million urban populations in China. The recent migrations and relocation from rural areas to urban have directly resulted in more than 15 megacities with a population of more than 10 million [
15]. According to China Environmental Bulletin, only 16 out of the 161 nationally selected cities have met the New Air Quality Standard for Testing launched in 2014 in China, yielding a 9.9% compliance rate [
16]. The Organization for Economic Cooperation and Development (OECD) estimated that urban air pollution contributed to about 350,000 to 500,000 deaths per year in China’s major cities [
17]. Large scale urbanization in China with unprecedented urban expansion and infrastructure development has led to the release of large amount of harmful pollutants to the atmosphere, seriously threatening people’s health [
18,
19].
Studies on public environmental health related risk perception originated in developed countries between the 1960s and 1970s, and most recent studies in this area were mainly conducted in Western countries [
20,
21]. In China, risk management on atmospheric pollution has been one of main important topics for the government [
22], as urban air pollution has become a major health hazard to its people. Successful management of environmental risks, especially the urban air pollution risk, can hardly be achieved without the public’s understandings and cooperation [
23]. Public perception of air pollution related health risks could also affect their personal environmental habits and behavior, and influence their judgments toward relevant risk management policy in a direct or indirect manner [
24,
25]. We are interested in evaluating the awareness of urban air pollution-health risk, and this study was designed to identify the main factors associated with the public’s health risk awareness toward urban air pollution, and to explore more effective way for urban air pollution control by bridging the gap between scientific research and public health risk awareness on urban air pollution.
To understand the megacity inhabitants’ health risk awareness of urban air pollution and its potential effect on public health, this study is aimed at assessing the first steps of developing a model of the social dilemma of unsafe air quality in Chinese megacities. In this paper, we evaluated the public’s awareness of health risk of urban air pollution using data from the three megacities along middle and lower reaches of the Yangtze River: Shanghai, Nanchang and Wuhan. The findings will not only have a huge impact on residents’ health-related behavior, but also provide the necessary scientific basis for government in their risk management of urban air pollution and better urban governance in the future [
26,
27,
28].
4. Discussion
China has been going through a rapid development of urbanization and accelerated growth of its economy [
30]. Many problems can be expected to occur at this stage, and urban air pollution is one of the most notable and challenging issues that must be faced [
31,
32]. As many major cities in China are undergoing an “urban reconstruction and modern industrialization” period, a substantial amount of infrastructure improvement has been undertaken. For instance, the fast-growing cities like Shanghai, Wuhan and Nanchang are racing to build subway systems that have attracted more migrant workers moving to these cities. Increased level of urban air pollution in these cities have placed the residents to more vulnerable adverse health condition: current researches have shown that many respiratory diseases werTABLEe due to air pollution, and long-term exposure to polluted air could damage people’s immune function [
9,
10,
33,
34,
35].
This paper assessed the first steps in developing a model of the social dilemma of unsafe air quality in Chinese megacities and provided valuable insight to bridge the gap between scientific research and public health risk awareness of urban air pollution. Our study provides important theoretical references for air pollution risk management and decision-makers, as well as useful measures for risk prevention and reduction [
36]. Understandings of the public perceptions of urban air pollution and related health risks and their influential factors are very important for the policymakers in their designing the relevant intervention programs [
37]. On the other hand, it is critical for all individuals to rectify the misunderstanding of urban air pollution and related health risks, to enhance more comprehension and cooperation with environmental policy managements, and to lower the policy execution cost.
Our study showed that the public was generally satisfied with current air quality, however their anxious feelings about air pollution remained, especially among females and older adults. Zhang [
31] reported that the females were particularly concerned about urban air pollution and related health risks, and ranked it in the first place. Our study also found that female expressed more negative and dissatisfied feelings when exposed to air pollutants. Kim et al. [
32] showed that younger people had lower satisfaction levels with urban air quality; however we found that older respondents were less satisfied and more anxious. This disagreement could be due to the difference in general physical health condition between older adults and the younger. In addition, people who had a previous travel experience had lower satisfactions on local urban air quality because of their travel. In addition, public’s anxious feelings towards urban air pollution were also influenced by their health condition—healthier people were less anxious.
Previous studies showed that the public’s knowledge of air quality was associated with demographic characteristics [
36,
37,
38]. Our study observed that educational level, income, health status and study sites were related to respondents’ understanding of air pollution related indicator (API). Those individuals with higher education, higher monthly income, and at good health status, had better knowledge about API. In addition, no differences of respondents’ general satisfaction and anxious feelings were found among the three study sites (
Table 2,
Table 3 and
Table 5). However, the public’s knowledge of the API varies significantly among the three megacities (
Table 4 and
Table 5), which might be a reflection of variations in education and income level among these cities as shown in
Table 1. This result is consistent with the findings reported in 1960s and some recent studies conducted in China [
21,
25,
29].
Correlation analyses indicated weak positive correlations between respondents’ anxious feeling—general satisfaction, knowledge of API—general satisfaction and knowledge of API—anxious feeling. Hence, there is a need to establish the links between the urban air pollutant emissions and control, and public’s general feelings and attitudes toward the urban air quality and management actions through the investigation of public’s general satisfaction. It may veritably reflect and systematically understand the current situation of urban air quality management and its health related risk management from the angle of responders’ perception. This information could be very valuable for enhanced environmental management to local government. Since little was done in this study to explore the reasons why respondents’ general satisfaction, anxious feeling and knowledge of API toward current air quality attitudes correlated with each other, more in-depth investigation or open-ended questions survey to address this point needs to be designed and conducted in future.
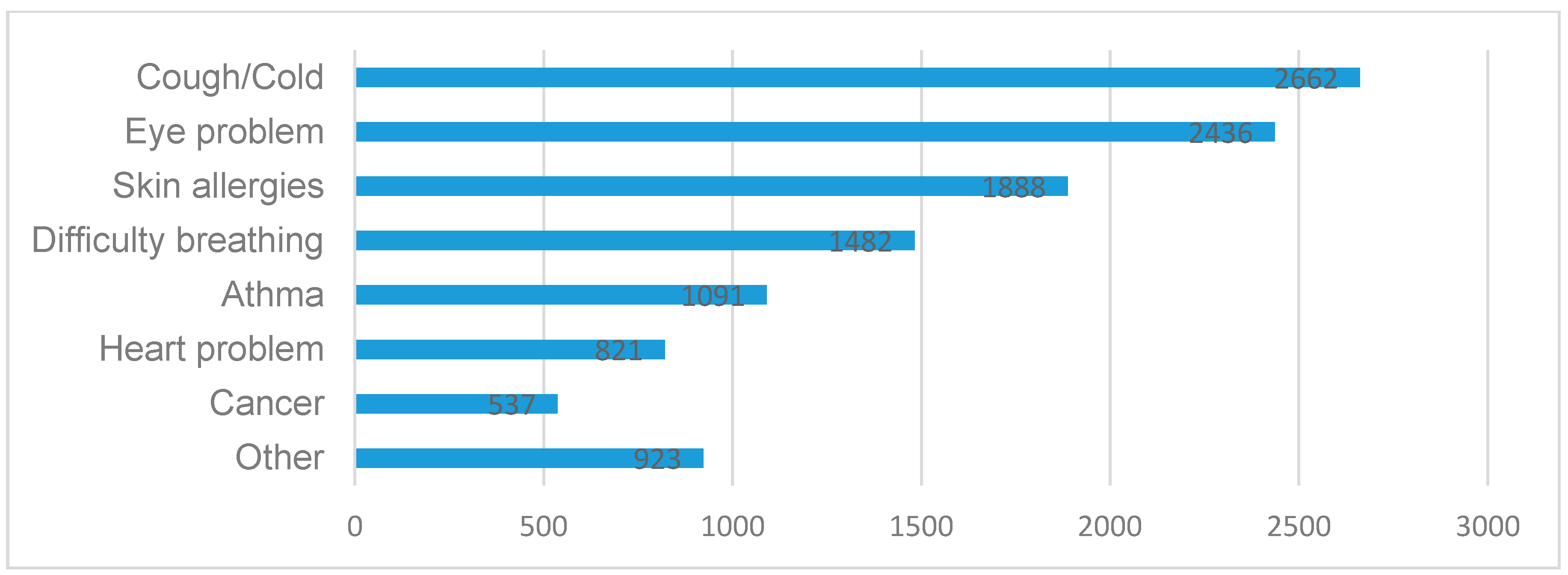
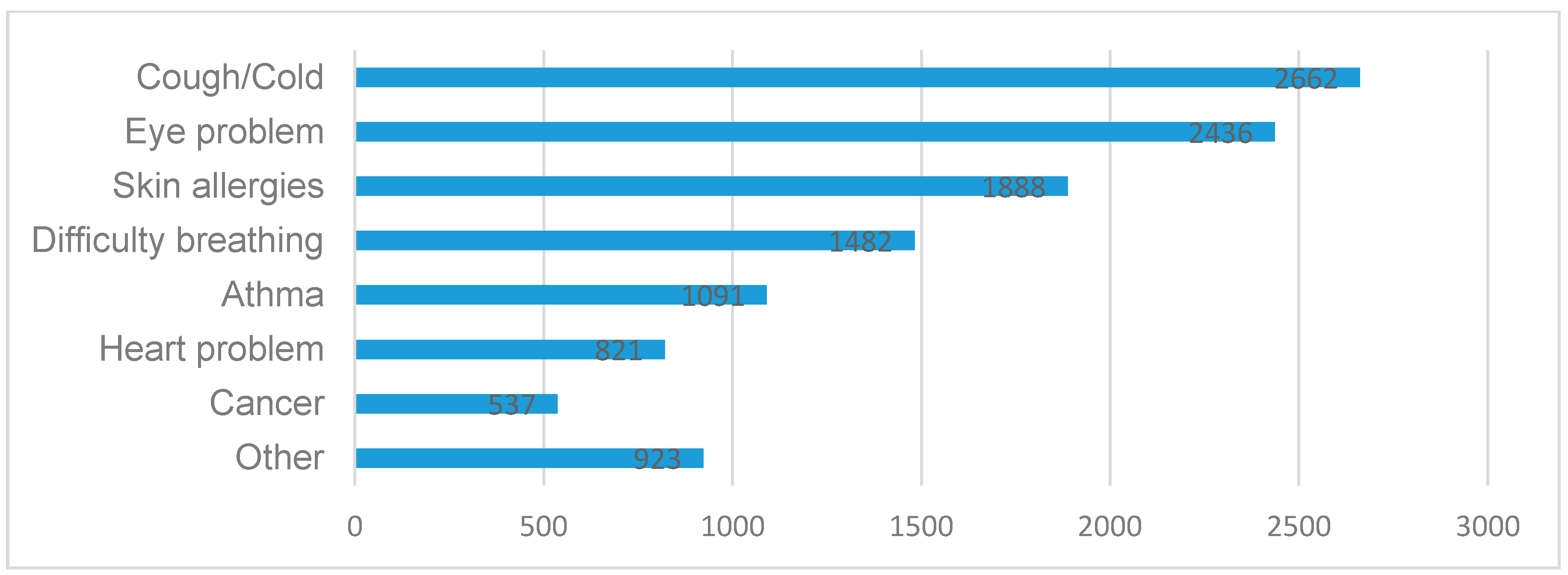
There are many studies suggesting that the serious effects of poor air quality on the human respiratory system have become much more apparent [
33,
34,
35]. Some studies [
39,
40] reveal that gender and individual’s health status significantly affect the public’s perceptions of air pollution and related health risks. It is widely believed that air pollution can cause or aggravate respiratory and lung diseases. Particularly, individuals who frequently suffer from asthma or respiratory diseases such as coughs are more sensitive to atmospheric pollutants, since these illnesses are triggered by air pollution. In this study, most megacity inhabitants believed that coughs/colds, eye problems and skin allergies were the three highest health risks due to urban air pollution, especially to the females and the older adults.
Current reports have seemed to be inconclusive regarding the relationship between the public risks perception and their income level. Some studies [
41,
42] showed that residents living in the well-developed regions were more prone to believe that poor air quality is responsible for their respiratory health, allergies and skin problems, while other studies [
43,
44] reported that those people with lower income were more likely to believe that there is no connection between poor air quality and health impact. Our study also showed that the public health concerns about air pollution were not affected by their income level. In addition, this study found that people with higher education level were more likely to believe the poor air quality may cause skin allergies, which is worthy of being properly addressed in the future.
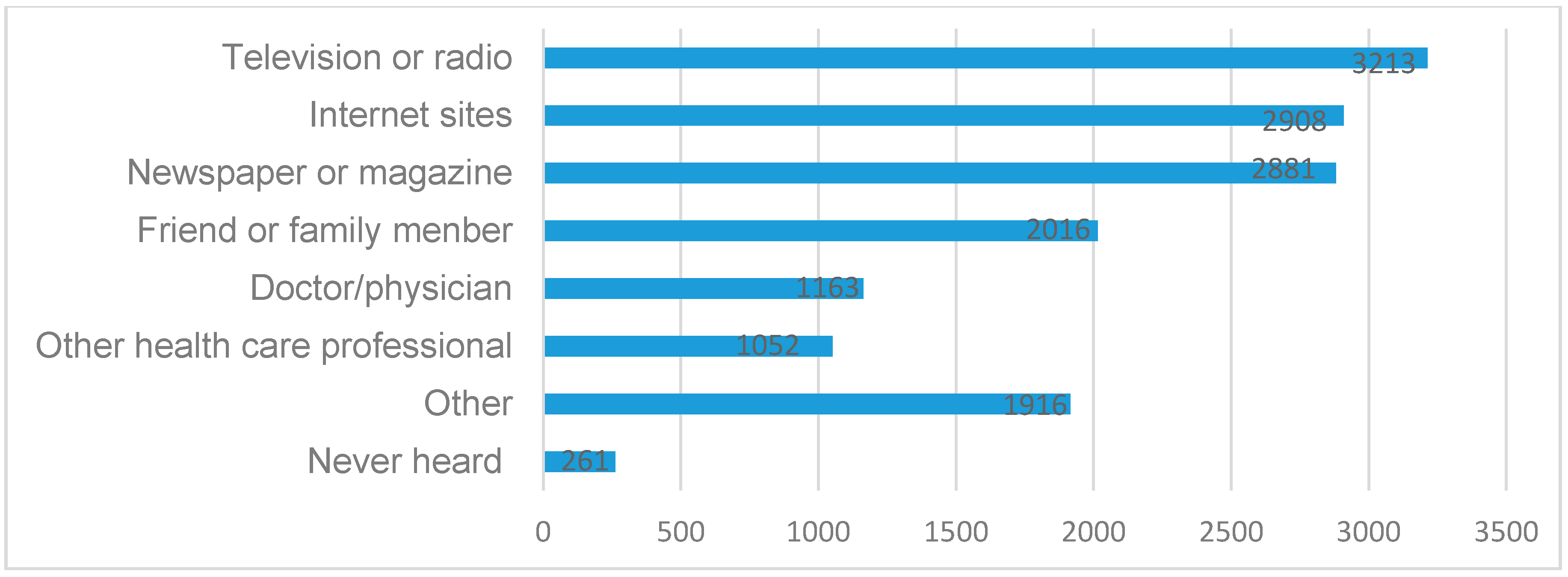
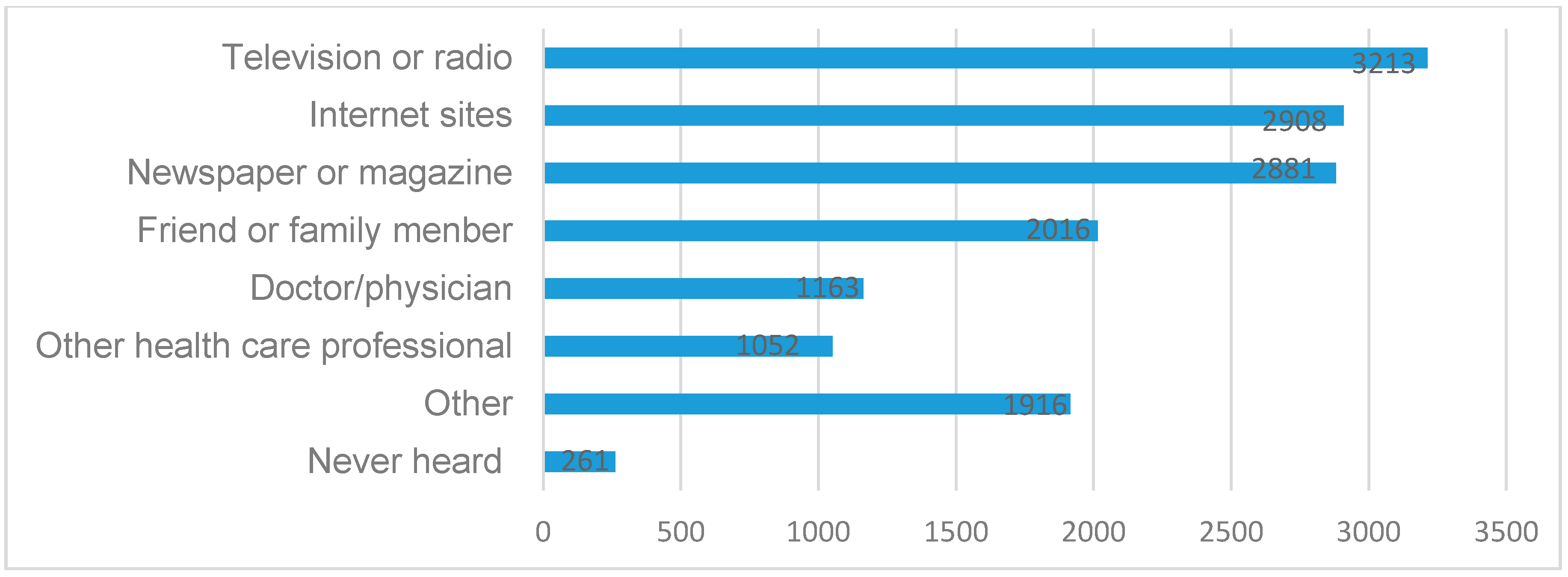
Finally, when the responders were asked where they learned health-related knowledge about urban air pollution, most respondents reported television/radio, internet sites and newspapers/magazines to be the main sources. However, Bickerstaff et al.’s study [
45] showed that very few people judged the quality through the air pollution related indicator released by the media. Even though people usually do not check the API specifically, reports and comments about air pollution problems through different media such as television, radio, internet sites, newspaper or magazine, etc., have increasingly impacted people’s awareness of urban air pollution and its adverse health impact. The diversified communication form, frequency of the reported information, the wording and the channel of promulgating such information can be the important factors affecting the public’s health-related knowledge, attitude and practice on urban air pollution.
Internet and new media like Weibo—the Chinese version of Twitter—and blogs greatly promote the flow and exchange for the information, and will amplify the effect of the environmental health-related risk (the so-called media amplifier effect) [
46]. On the other hand, informal communication or conversation among the public is also an important way for people to apperceive outside health-related risks, which may function as an essential supplement to adjust people’s subjective feelings. Discussion and information exchange on air pollution between relatives, friends and colleagues could also play an influential role on people’s risk perception. This study shows that there are a quite a few respondents reporting that they obtained health-related knowledge about urban air pollution through their friends, family members, doctors, physicians or other health care professional. Findings from this study emphasizes the need for more frequent education campaigns of environmental health risks and protections in order to enhance the public’s self-protection consciousness as well as to monitor and improve air quality.
Despite its vigorous design, there are several limitations in this study. This survey was conducted at three megacities in China, and our inclusion criteria for research object is only for those who aged 18 years and above and living in the those megacities for at least one year, so the design of this study has limited participants from rural areas or temporary migrants. Thus, application of these findings to other areas and other population groups should be done with caution. Moreover, open-ended questions need to be designed to reveal new problems and deepen the understanding of the respondents’ attitudes towards current air quality in China’s megacities. For example, what kind of styles and education campaigns they want to enhance the public’s self-protection consciousness as well as to monitor and improve air quality. These are what need to be properly addressed in further research. In addition, social desirability of the participants may also have an effect on their answers since the results were self-reported from the interviewees.



{kind=link}
{kind=link}