
Associations of Age, BMI, and Years of Menstruation with Proximal Femur Strength in Chinese Postmenopausal Women: A Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Bone Densitometry and Hip Structure Analysis
2.3. Exposure and Covariate Measurements
2.4. Statistical Methods
3. Results
3.1. General Characteristics of the Subjects

{kind=link}
| Variable | Mean/n | SD/Percentage |
|---|---|---|
| Age (year) | 59.6 | 5.0 |
| Height (cm) | 154.9 | 5.4 |
| Weight (kg) | 56.0 | 8.4 |
| BMI (kg/m2) | 23.4 | 3.3 |
| Years of menstruation (year) | 36.3 | 3.4 |
| Age at menarche | 14.1 | 1.7 |
| Total daily physical activity (MET·h/d) | 17.0 | 6.5 |
| Education | ||
| primary school or below | 105 | 7.9% |
| junior high school | 315 | 23.8% |
| senior high school | 654 | 49.5% |
| college degree or above | 248 | 18.8% |
| Smoking status | ||
| passive smokers | 354 | 26.8% |
| no | 968 | 73.2% |
| Calcium tablet intake | ||
| yes | 463 | 35.0% |
| no | 859 | 65.0% |
3.2. Associations of Age, BMI, and Years of Menstruation with BMD and HSA Indices
| ROI Site | Variable | Cumulative Variability Explained | Age | BMI | Years of Menstruation | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| β | p | Variability Explained by Variable | β | p | Variability Explained by Variable | β | p | Variability Explained by Variable | |||
| NN | BMD | 23.1% | −0.008 | <0.001 | 8.4% | 0.014 | <0.001 | 13.0% | 0.005 | <0.001 | 1.7% |
| CSA | 29.9% | −0.018 | <0.001 | 7.9% | 0.046 | <0.001 | 20.7% | 0.012 | <0.001 | 1.3% | |
| OD | 2.1% | 0.005 | <0.001 | 1.2% | 0.006 | 0.003 | 0.7% | −0.005 | 0.026 | 0.3% | |
| CT | 22.4% | −0.002 | <0.001 | 8.3% | 0.003 | <0.001 | 12.4% | 0.001 | <0.001 | 1.7% | |
| SM | 16.1% | −0.007 | <0.001 | 3.3% | 0.020 | <0.001 | 12.0% | 0.005 | 0.002 | 0.7% | |
| BR | 12.7% | 0.149 | <0.001 | 6.8% | −0.177 | <0.001 | 4.6% | −0.101 | <0.001 | 1.3% | |
| IT | BMD | 22.0% | −0.007 | <0.001 | 6.9% | 0.015 | <0.001 | 13.0% | 0.006 | <0.001 | 2.0% |
| CSA | 27.2% | −0.031 | <0.001 | 5.6% | 0.092 | <0.001 | 19.6% | 0.029 | <0.001 | 1.9% | |
| OD | 4.4% | 0.008 | <0.001 | 1.1% | 0.020 | <0.001 | 3.3% | −0.002 | 0.572 | 0.0% | |
| CT | 21.3% | −0.004 | <0.001 | 7.0% | 0.007 | <0.001 | 12.4% | 0.003 | <0.001 | 1.9% | |
| SM | 24.7% | −0.018 | <0.001 | 2.1% | 0.094 | <0.001 | 21.3% | 0.023 | <0.001 | 1.3% | |
| BR | 16.1% | 0.096 | <0.001 | 7.1% | -0.136 | <0.001 | 6.7% | −0.085 | <0.001 | 2.3% | |
| FS | BMD | 19.6% | −0.008 | <0.001 | 4.3% | 0.021 | <0.001 | 13.9% | 0.007 | <0.001 | 1.4% |
| CSA | 29.1% | −0.015 | <0.001 | 3.1% | 0.069 | <0.001 | 24.5% | 0.016 | <0.001 | 1.5% | |
| OD | 5.0% | 0.004 | <0.001 | 1.4% | 0.010 | <0.001 | 3.5% | −0.002 | 0.148 | 0.2% | |
| CT | 16.6% | −0.004 | <0.001 | 4.2% | 0.010 | <0.001 | 11.2% | 0.003 | <0.001 | 1.1% | |
| SM | 27.2% | 0.000 | 0.777 | 0.0% | 0.040 | <0.001 | 26.7% | 0.005 | 0.012 | 0.5% | |
| BR | 10.2% | 0.028 | <0.001 | 3.5% | −0.052 | <0.001 | 5.3% | −0.028 | <0.001 | 1.4% | |
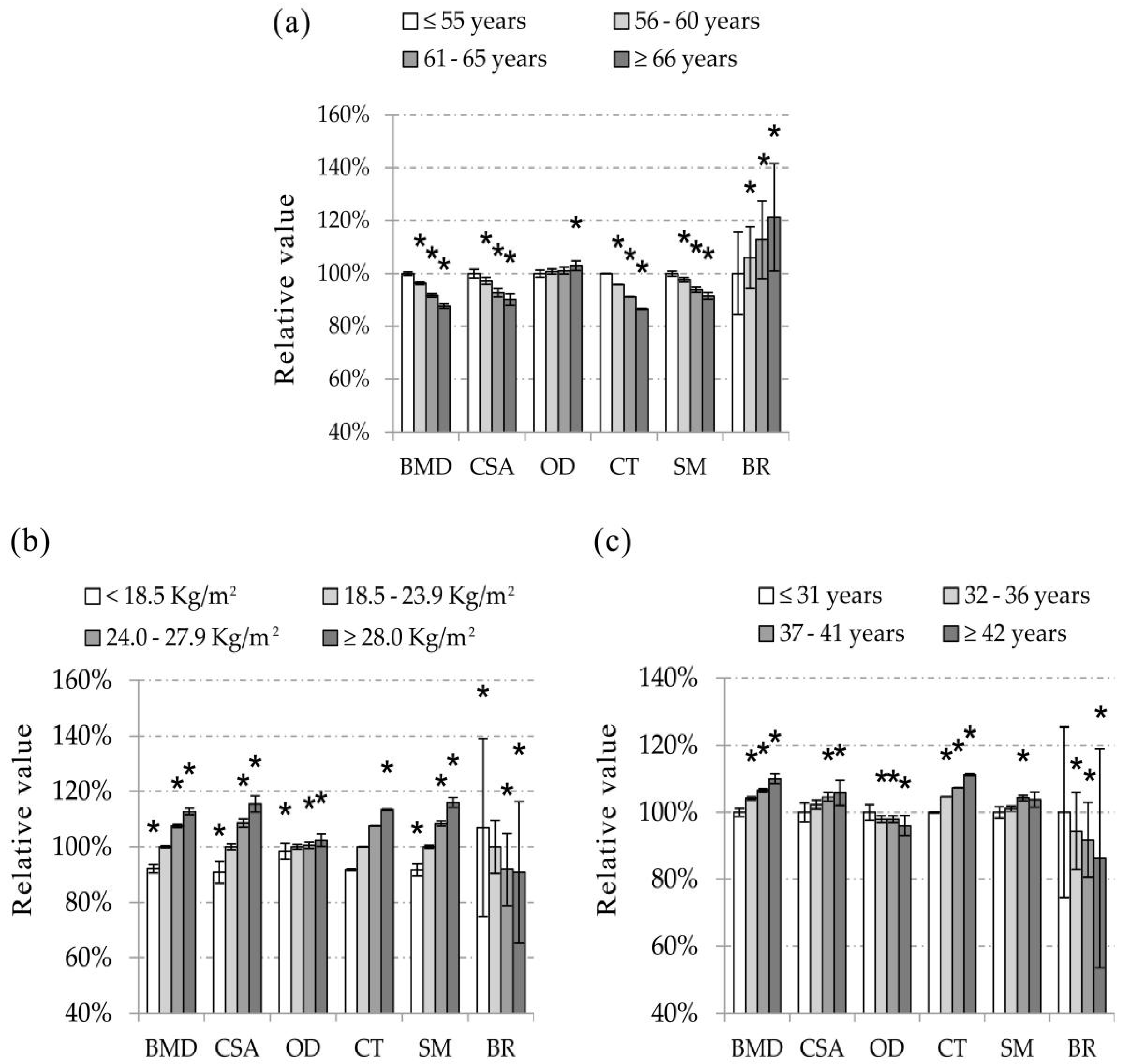
3.3. Age Specific Values of BMD and HSA Indices
| ROI Site | Variable | Age (year) | p | Slope/Year | |||
|---|---|---|---|---|---|---|---|
| ≤55 (n = 300) | 56–60 (n = 519) | 61–65 (n = 327) | ≥66 (n = 176) | ||||
| NN | BMD (g/cm2) | 0.879 (0.007) | 0.847 (0.005) a | 0.806 (0.007)) a | 0.770 (0.009) a | <0.001 | −0.96% |
| CSA (cm2) | 2.508 (0.017) | 2.439 (0.013) a | 2.326 (0.016) a | 2.260 (0.022) a | <0.001 | −0.75% | |
| OD (cm) | 3.013 (0.014) | 3.038 (0.010) | 3.048 (0.013) | 3.105 (0.018) a | 0.001 | 0.16% | |
| CT (cm) | 0.170 (0.001) | 0.163 (0.001) a | 0.155 (0.001) a | 0.147(0.002) a | <0.001 | −1.24% | |
| SM (cm3) | 1.131 (0.010) | 1.105 (0.008) a | 1.062 (0.010) a | 1.035 (0.013) a | <0.001 | −0.64% | |
| BR | 10.235 (0.156) | 10.849 (0.116) a | 11.538 (0.147) a | 12.411 (0.202) a | <0.001 | 1.34% | |
| IT | BMD (g/cm2) | 0.903 (0.008) | 0.858 (0.006) a | 0.823 (0.007) a | 0.794 (0.010) a | <0.001 | −0.82% |
| CSA (cm2) | 4.481 (0.036) | 4.301(0.027) a | 4.153 (0.034) a | 4.020 (0.047) a | <0.001 | −0.73% | |
| OD (cm) | 5.214 (0.021) | 5.279 (0.016) a | 5.295 (0.020) a | 5.346 (0.028) a | 0.002 | 0.15% | |
| CT (cm) | 0.394 (0.004) | 0.376 (0.003) a | 0.359 (0.003) a | 0.343 (0.005) a | 0.001 | −1.08% | |
| SM (cm3) | 3.631 (0.035) | 3.492 (0.026) a | 3.421 (0.033) a | 3.352 (0.045) a | <0.001 | −0.52% | |
| BR | 8.057 (0.099) | 8.583 (0.073) a | 8.927(0.093) a | 9.470 (0.127) a | <0.001 | 1.11% | |
| FS | BMD (g/cm2) | 1.370 (0.010) | 1.344 (0.008) a | 1.314 (0.010) a | 1.258 (0.013) a | <0.001 | −0.60% |
| CSA (cm2) | 3.581 (0.023) | 3.524 (0.017) a | 3.474 (0.022) a | 3.351 (0.030) a | <0.001 | −0.43% | |
| OD (cm) | 2.751 (0.010) | 2.759 (0.008) | 2.783 (0.010) a | 2.804 (0.013) a | 0.006 | 0.14% | |
| CT (cm) | 0.517 (0.005) | 0.506 (0.004) | 0.488 (0.005) a | 0.461 (0.007) a | <0.001 | −0.80% | |
| SM (cm3) | 1.841 (0.013) | 1.837 (0.010) | 1.853 (0.012) | 1.832 (0.017) | 0.681 | 0.00% | |
| BR | 2.863 (0.042) | 2.965 (0.031) | 3.043 (0.040) a | 3.278 (0.054) a | <0.001 | 0.93% | |
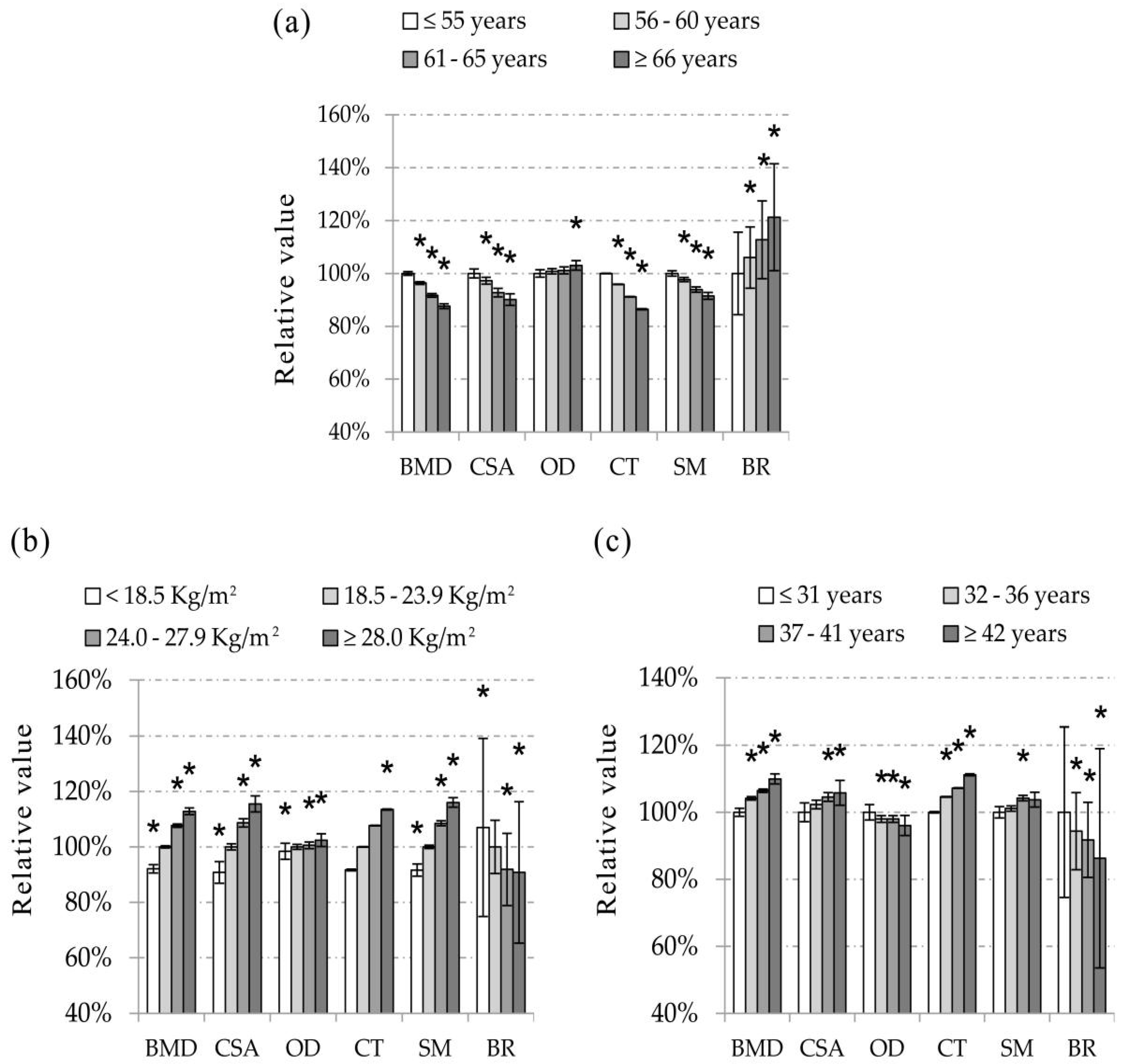
3.4. BMI Specific Values of BMD and HSA Indices
3.5. Years of Menstruation Specific Values of BMD and HSA Indices
| ROI Site | Variable | BMI (kg/m2) | p | Slope/BMI | |||
|---|---|---|---|---|---|---|---|
| <18.5 (n = 67) | 18.5–23.9 (n = 743) | 24.0–27.9 (n = 405) | ≥28.0 (n = 107) | ||||
| NN | BMD (g/cm2) | 0.746 (0.015) a | 0.810 (0.004) | 0.872 (0.006) a | 0.914 (0.012) a | <0.001 | 1.68% |
| CSA (cm2) | 2.109 (0.039) a | 2.323 (0.011) | 2.524 (0.015) a | 2.683 (0.029) a | <0.001 | 1.91% | |
| OD (cm) | 2.987 (0.029) | 3.035 (0.009) | 3.052 (0.012) | 3.109 (0.023) a | 0.004 | 0.20% | |
| CT (cm) | 0.143 (0.003) a | 0.156 (0.001) | 0.168 (0.001) a | 0.177 (0.002) a | <0.001 | 1.86% | |
| SM (cm3) | 0.966 (0.022) a | 1.054 (0.006) | 1.144 (0.009) a | 1.223 (0.017) a | <0.001 | 1.83% | |
| BR | 12.216 (0.321) a | 11.414 (0.096) | 10.486 (0.130) a | 10.363 (0.255) a | <0.001 | −1.60% | |
| IT | BMD (g/cm2) | 0.746 (0.016) a | 0.826 (0.005) | 0.891 (0.006) a | 0.944 (0.013) a | <0.001 | 1.76% |
| CSA (cm2) | 3.647 (0.076) a | 4.114 (0.023) | 4.508 (0.031) a | 4.813 (0.060) a | <0.001 | 2.16% | |
| OD (cm) | 5.074 (0.044) a | 5.251 (0.013) | 5.337 (0.018) a | 5.356 (0.035) a | <0.001 | 0.38% | |
| CT (cm) | 0.324 (0.008) a | 0.360 (0.002) | 0.389 (0.003) a | 0.414 (0.006) a | <0.001 | 1.89% | |
| SM (cm3) | 2.780 (0.074) a | 3.331 (0.022) | 3.752 (0.030) a | 4.009 (0.058) a | <0.001 | 2.70% | |
| BR | 9.688 (0.203) a | 8.890 (0.061) | 8.267 (0.082) a | 7.989 (0.161) a | <0.001 | −1.57% | |
| FS | BMD (g/cm2) | 1.165 (0.021) a | 1.300 (0.006) | 1.383 (0.009) a | 1.455 (0.017) a | <0.001 | 1.58% |
| CSA (cm2) | 2.979 (0.049) a | 3.397 (0.015) | 3.672 (0.020) a | 3.908 (0.039) a | <0.001 | 1.97% | |
| OD (cm) | 2.703 (0.021) a | 2.749 (0.006) | 2.800 (0.009) a | 2.831 (0.017) a | <0.001 | 0.36% | |
| CT (cm) | 0.425 (0.011) a | 0.483 (0.003) | 0.522 (0.004) a | 0.556 (0.009) a | <0.001 | 2.01% | |
| SM (cm3) | 1.539 (0.027) a | 1.780 (0.008) | 1.942 (0.011) a | 2.077 (0.022) a | <0.001 | 2.17% | |
| BR | 3.455 (0.087) a | 3.065 (0.026) | 2.887 (0.035) a | 2.727 (0.069) a | <0.001 | −1.73% | |
| ROI Site | Variable | Years of Menstruation (year) | p | Slope/Year of Menstruation | |||
|---|---|---|---|---|---|---|---|
| ≤31 (n = 112) | 32–36 (n = 556) | 37–41 (n = 586) | ≥42 (n = 68) | ||||
| NN | BMD (g/cm2) | 0.793 (0.012) | 0.826 (0.005) a | 0.844 (0.005) a | 0.872 (0.015) a | <0.001 | 0.60% |
| CSA (cm2) | 2.326 (0.028) | 2.380 (0.013) | 2.432 (0.013) a | 2.461 (0.037) a | 0.001 | 0.50% | |
| OD (cm) | 3.104 (0.023) | 3.042 (0.010) a | 3.042 (0.010) a | 2.982 (0.030) a | 0.011 | −0.16% | |
| CT (cm) | 0.152 (0.002) | 0.159 (0.001) a | 0.163 (0.001) a | 0.169 (0.003) a | <0.001 | 0.62% | |
| SM (cm3) | 1.064 (0.017) | 1.076 (0.008) | 1.109 (0.008) a | 1.104 (0.022) | 0.012 | 0.46% | |
| BR | 11.887 (0.254) | 11.218 (0.115) a | 10.909 (0.112) a | 10.255 (0.327) a | <0.001 | −0.91% | |
| IT | BMD (g/cm2) | 0.799 (0.012) | 0.841 (0.006) a | 0.866 (0.006) a | 0.895 (0.016) a | <0.001 | 0.71% |
| CSA (cm2) | 4.052 (0.059) | 4.211 (0.027) a | 4.343 (0.026) a | 4.441 (0.076) a | <0.001 | 0.68% | |
| OD (cm) | 5.325 (0.035) | 5.265 (0.016) a | 5.283 (0.015) a | 5.248 (0.045) a | 0.351 | −0.04% | |
| CT (cm) | 0.349 (0.006) | 0.366 (0.003) a | 0.379 (0.003) a | 0.389 (0.008) a | <0.001 | 0.81% | |
| SM (cm3) | 3.316 (0.057) | 3.445 (0.026) a | 3.543 (0.025) a | 3.636 (0.074) a | 0.001 | 0.66% | |
| BR | 9.332 (0.160) | 8.827 (0.072) a | 8.448 (0.071) a | 8.141 (0.206) a | <0.001 | −0.98% | |
| FS | BMD (g/cm2) | 1.282 (0.017) | 1.313 (0.008) | 1.351 (0.007) a | 1.382 (0.021) a | <0.001 | 0.53% |
| CSA (cm2) | 3.393 (0.038) | 3.457 (0.017) | 3.550 (0.017) a | 3.627 (0.049) a | <0.001 | 0.46% | |
| OD (cm) | 2.794 (0.017) | 2.774 (0.008) | 2.761 (0.008) | 2.757 (0.022) | 0.316 | −0.07% | |
| CT (cm) | 0.475 (0.009) | 0.490 (0.004) | 0.507 (0.004) a | 0.521 (0.011) a | <0.001 | 0.60% | |
| SM (cm3) | 1.821 (0.021) | 1.823 (0.010) | 1.855 (0.009) | 1.903 (0.027) a | 0.018 | 0.27% | |
| BR | 3.204 (0.068) | 3.078 (0.031) | 2.914 (0.030) a | 2.828 (0.088) a | <0.001 | −0.93% | |
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| BMD | Bone mineral density |
| HSA | Hip Structure Analysis |
| ROI | Regions of interest |
| NN | Narrow neck |
| IT | Intertrochanter |
| FS | Femoral shaft |
| CSA | Cross-sectional area |
| OD | Outer diameter |
| CT | Cortical thickness |
| SM | Section modulus |
| BR | Buckling ratio |
References
- Kanis, J.A. Diagnosis of osteoporosis and assessment of fracture risk. Lancet 2002, 359, 1929–1936. [Google Scholar] [CrossRef]
- Black, D.M.; Steinbuch, M.; Palermo, L.; Dargent-Molina, P.; Lindsay, R.; Hoseyni, M.S.; Johnell, O. An assessment tool for predicting fracture risk in postmenopausal women. Osteoporos. Int. 2001, 12, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Lyles, K.W.; Colon-Emeric, C.S.; Magaziner, J.S.; Adachi, J.D.; Pieper, C.F.; Mautalen, C.; Hyldstrup, L.; Recknor, C.; Nordsletten, L.; Moore, K.A.; et al. Zoledronic acid in reducing clinical fracture and mortality after hip fracture. N. Engl. J. Med. 2007. [Google Scholar] [CrossRef]
- LaCroix, A.Z.; Beck, T.J.; Cauley, J.A.; Lewis, C.E.; Bassford, T.; Jackson, R.; Wu, G.; Chen, Z. Hip structural geometry and incidence of hip fracture in postmenopausal women: What does it add to conventional bone mineral density? Osteoporos. Int. 2010, 21, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Kaptoge, S.; Beck, T.J.; Reeve, J.; Stone, K.L.; Hillier, T.A.; Cauley, J.A.; Cummings, S.R. Prediction of incident hip fracture risk by femur geometry variables measured by hip structural analysis in the study of osteoporotic fractures. J. Bone Miner. Res. 2008, 23, 1892–1904. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, K.G.; Wacker, W.K.; Barden, H.S.; Simonelli, C.; Burke, P.K.; Ragi, S.; Del Rio, L. Femur strength index predicts hip fracture independent of bone density and hip axis length. Osteoporos. Int. 2006, 17, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Manolagas, S.C.; Parfitt, A.M. What old means to bone. Trends Endocrinol. Metab. 2010, 21, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Skrzek, A.; Koziel, S.; Ignasiak, Z. The optimal value of BMI for the lowest risk of osteoporosis in postmenopausal women aged 40–88 years. HOMO 2014, 65, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Oldroyd, A.; Mitchell, K.; Bukhari, M. The prevalence of osteoporosis in an older population with very high body mass index: Evidence for an association. Int. J. ClinPract. 2014, 68, 771–774. [Google Scholar] [CrossRef] [PubMed]
- De Laet, C.; Kanis, J.A.; Oden, A.; Johanson, H.; Johnell, O.; Delmas, P.; Eisman, J.A.; Kroger, H.; Fujiwara, S.; Garnero, P.; et al. Body mass index as a predictor of fracture risk: A meta-analysis. Osteoporos. Int. 2005, 16, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Ong, T.; Sahota, O.; Tan, W.; Marshall, L. A United Kingdom perspective on the relationship between body mass index (BMI) and bone health: A cross sectional analysis of data from the Nottingham Fracture Liaison Service. Bone 2014, 59, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Manolagas, S.C.; Kousteni, S.; Jilka, R.L. Sex steroids and bone. Recent Prog. Horm. Res. 2002, 57, 385–409. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.E.; Troisi, R.; Wise, L.A.; Palmer, J.R.; Titus-Ernstoff, L.; Strohsnitter, W.C.; Hatch, E.E. Menarche, menopause, years of menstruation, and the incidence of osteoporosis: The influence of prenatal exposure to diethylstilbestrol. J. Clin. Endocrinol. Metab. 2014, 99, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Sioka, C.; Fotopoulos, A.; Georgiou, A.; Xourgia, X.; Papadopoulos, A.; Kalef-Ezra, J.A. Age at menarche, age at menopause and duration of fertility as risk factors for osteoporosis. Climacteric 2010, 13, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.Q.; He, L.P.; Liu, Y.H.; Su, Y.X.; Chen, Y.M. Association between dietary intake of flavonoid and bone mineral density in middle aged and elderly Chinese women and men. Osteoporos. Int. 2014, 25, 2417–2425. [Google Scholar] [CrossRef] [PubMed]
- Beck, T.J. Extending DXA beyond bone mineral density: Understanding hip structure analysis. Curr. Osteoporos. Rep. 2007, 5, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Iki, M.; DongMei, N.; Tamaki, J.; Sato, Y.; Kagamimori, S.; Kagawa, Y.; Yoneshima, H.; Japanese Population-based Osteoporosis Study Group. Age-specific reference values of hip geometric indices from a representative sample of the Japanese female population: Japanese Population-based Osteoporosis (JPOS) Study. Osteoporos. Int. 2011, 22, 1987–1996. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Hu, Y.Q.; Zhang, Z.L. Age trends for hip geometry in Chinese men and women and the association with femoral neck fracture. Osteoporos. Int. 2011, 22, 2513–2522. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.; Turner, C.H.; Kim, B.T.; Seeman, E. Sexual dimorphism in vertebral fragility is more the result of gender differences in age-related bone gain than bone loss. J. Bone Miner. Res. 2001, 16, 2267–2275. [Google Scholar] [CrossRef] [PubMed]
- Beck, T.J.; Petit, M.A.; Wu, G.; LeBoff, M.S.; Cauley, J.A.; Chen, Z. Does obesity really make the femur stronger? BMD, geometry, and fracture incidence in the women’s health initiative-observational study. J. Bone Miner. Res. 2009, 24, 1369–1379. [Google Scholar] [CrossRef] [PubMed]
- El Hage, R. Geometric indices of hip bone strength in obese, overweight, and normal-weight adolescent boys. Osteoporos. Int. 2012, 23, 1593–1600. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Xu, Y.; Guo, B.; Xu, H. DXA femoral neck strength analysis in Chinese overweight and normal weight adolescents. J. Clin. Densitom. 2012, 15, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Beck, T.J.; Oreskovic, T.L.; Stone, K.L.; Ruff, C.B.; Ensrud, K.; Nevitt, M.C.; Genant, H.K.; Cummings, S.R. Structural adaptation to changing skeletal load in the progression toward hip fragility: The study of osteoporotic fractures. J. Bone Miner. Res. 2001, 16, 1108–1119. [Google Scholar] [CrossRef] [PubMed]
- Ilich, J.Z.; Kelly, O.J.; Inglis, J.E.; Panton, L.B.; Duque, G.; Ormsbee, M.J. Interrelationship among muscle, fat, and bone: Connecting the dots on cellular, hormonal, and whole body levels. Ageing Res. Rev. 2014, 15, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.J.; Liu, Y.J.; Liu, P.Y.; Hamilton, J.; Recker, R.R.; Deng, H.W. Relationship of obesity with osteoporosis. J. Clin. Endocrinol. Metab. 2007, 92, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.H.; Venners, S.A.; Terwedow, H.A.; Feng, Y.; Niu, T.; Li, Z.; Laird, N.; Brain, J.D.; Cummings, S.R.; Bouxsein, M.L.; Rosen, C.J.; Xu, X. Relation of body composition, fat mass, and serum lipids to osteoporotic fractures and bone mineral density in Chinese men and women. Am. J. Clin. Nutr. 2006, 83, 146–154. [Google Scholar] [PubMed]
- Travison, T.G.; Araujo, A.B.; Esche, G.R.; Beck, T.J.; McKinlay, J.B. Lean mass and not fat mass is associated with male proximal femur strength. J. Bone Miner. Res. 2008, 23, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Braun, T.; Schett, G. Pathways for bone loss in inflammatory disease. CurrOsteoporos Rep. 2012, 10, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Pitroda, A.P.; Harris, S.S.; Dawson-Hughes, B. The association of adiposity with parathyroid hormone in healthy older adults. Endocrine 2009, 36, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.V.; Jones, G.; Sambrook, P.N.; White, C.P.; Kelly, P.J.; Eisman, J.A. Effects of estrogen exposure and reproductive factors on bone mineral density and osteoporotic fractures. J. Clin. Endocrinol. Metab. 1995, 80, 2709–2714. [Google Scholar] [PubMed]
- El Maghraoui, A.; Guerboub, A.A.; Mounach, A.; Ghozlani, I.; Nouijai, A.; Ghazi, M.; Achemlal, L.; Bezza, A.; Tazi, M.A. Body mass index and gynecological factors as determinants of bone mass in healthy Moroccan women. Maturitas 2007, 56, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Hagemans, M.L.; van der Schouw, Y.T.; de Kleijn, M.J.; van Staveren, W.A.; Pop, V.J.; Leusink, G.L.; Grobbee, D.E. Indicators for the total duration of premenopausal endogenous estrogen exposure in relation to BMD. Hum. Reprod. 2004, 19, 2163–2169. [Google Scholar] [CrossRef] [PubMed]
- Clarke, B.L.; Khosla, S. Female reproductive system and bone. Arch. BiochemBiophys. 2010, 503, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Manolagas, S.C.; Jilka, R.L. Bone marrow, cytokines, and bone remodeling. Emerging insights into the pathophysiology of osteoporosis. N. Engl. J. Med. 1995, 332, 305–311. [Google Scholar] [PubMed]
- Manolagas, S.C. Birth and death of bone cells: Basic regulatory mechanisms and implications for the pathogenesis and treatment of osteoporosis. Endocr. Rev. 2000, 21, 115–137. [Google Scholar] [CrossRef] [PubMed]
- Cosman, F.; Nieves, J.; Horton, J.; Shen, V.; Lindsay, R. Effects of estrogen on response to edetic acid infusion in postmenopausal osteoporotic women. J. Clin. Endocrinol. Metab. 1994, 78, 939–943. [Google Scholar] [PubMed]
- Kritz-Silverstein, D.; Barrett-Connor, E. Early menopause, number of reproductive years, and bone mineral density in postmenopausal women. Am. J. Public Health 1993, 83, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Khoo, B.C.; Brown, K.; Zhu, K.; Pollock, M.; Wilson, K.E.; Price, R.I.; Prince, R.L. Differences in structural geometrical outcomes at the neck of the proximal femur using two-dimensional DXA-derived projection (APEX) and three-dimensional QCT-derived (BIT QCT) techniques. Osteoporos. Int. 2012, 23, 1393–1398. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, H.; Chen, Y.-M.; Han, G.; Huang, H.; Chen, W.-Q.; Wang, X.; Zhu, Y.-Y.; Xiao, S.-M. Associations of Age, BMI, and Years of Menstruation with Proximal Femur Strength in Chinese Postmenopausal Women: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2016, 13, 157. https://doi.org/10.3390/ijerph13020157
Kang H, Chen Y-M, Han G, Huang H, Chen W-Q, Wang X, Zhu Y-Y, Xiao S-M. Associations of Age, BMI, and Years of Menstruation with Proximal Femur Strength in Chinese Postmenopausal Women: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2016; 13(2):157. https://doi.org/10.3390/ijerph13020157
Chicago/Turabian StyleKang, Huili, Yu-Ming Chen, Guiyuan Han, Hua Huang, Wei-Qing Chen, Xidan Wang, Ying-Ying Zhu, and Su-Mei Xiao. 2016. "Associations of Age, BMI, and Years of Menstruation with Proximal Femur Strength in Chinese Postmenopausal Women: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 13, no. 2: 157. https://doi.org/10.3390/ijerph13020157