
Secondhand Smoke Is an Important Modifiable Risk Factor in Sickle Cell Disease: A Review of the Current Literature and Areas for Future Research

 , ,
, ,
Abstract
:1. Introduction
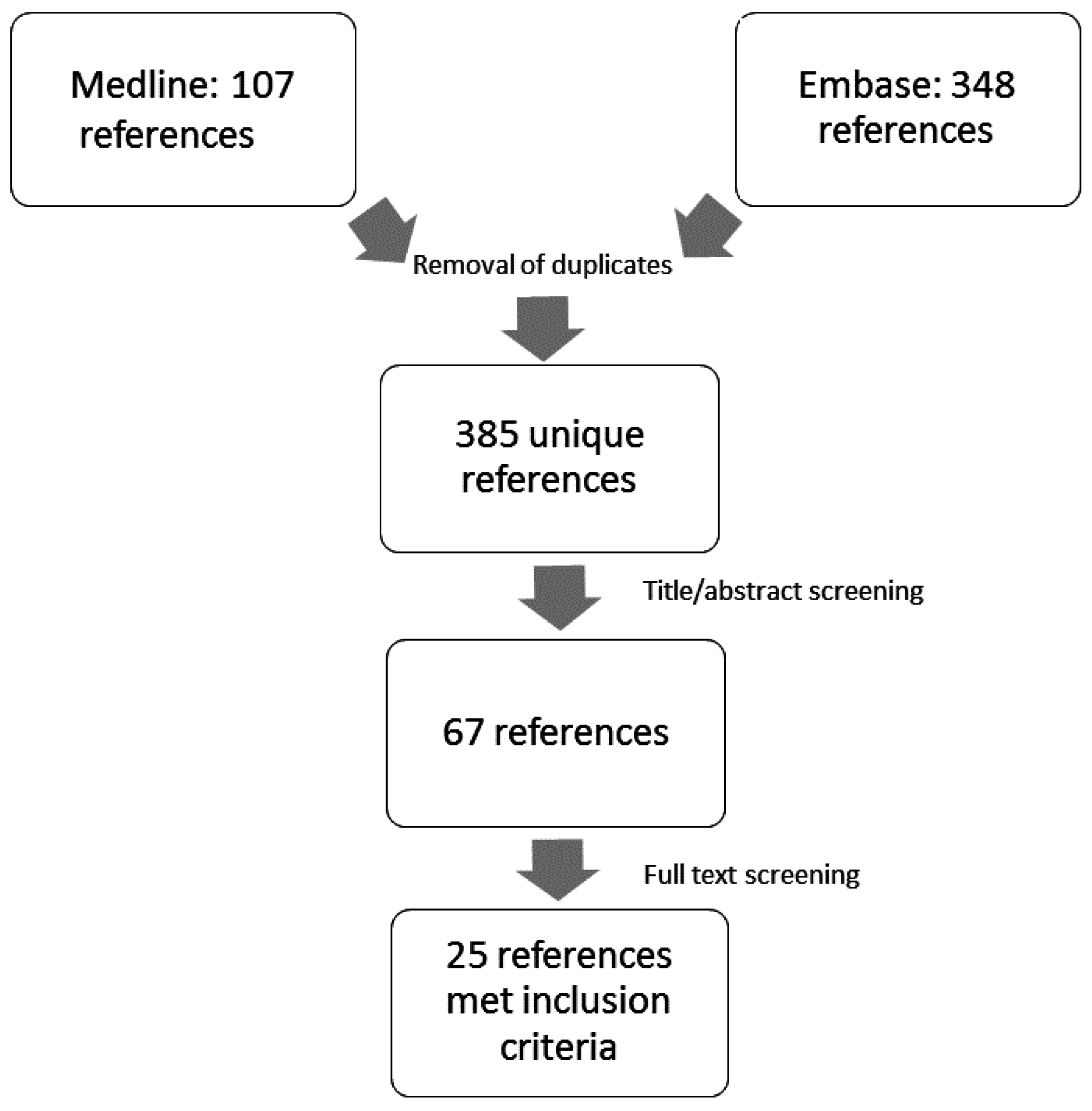
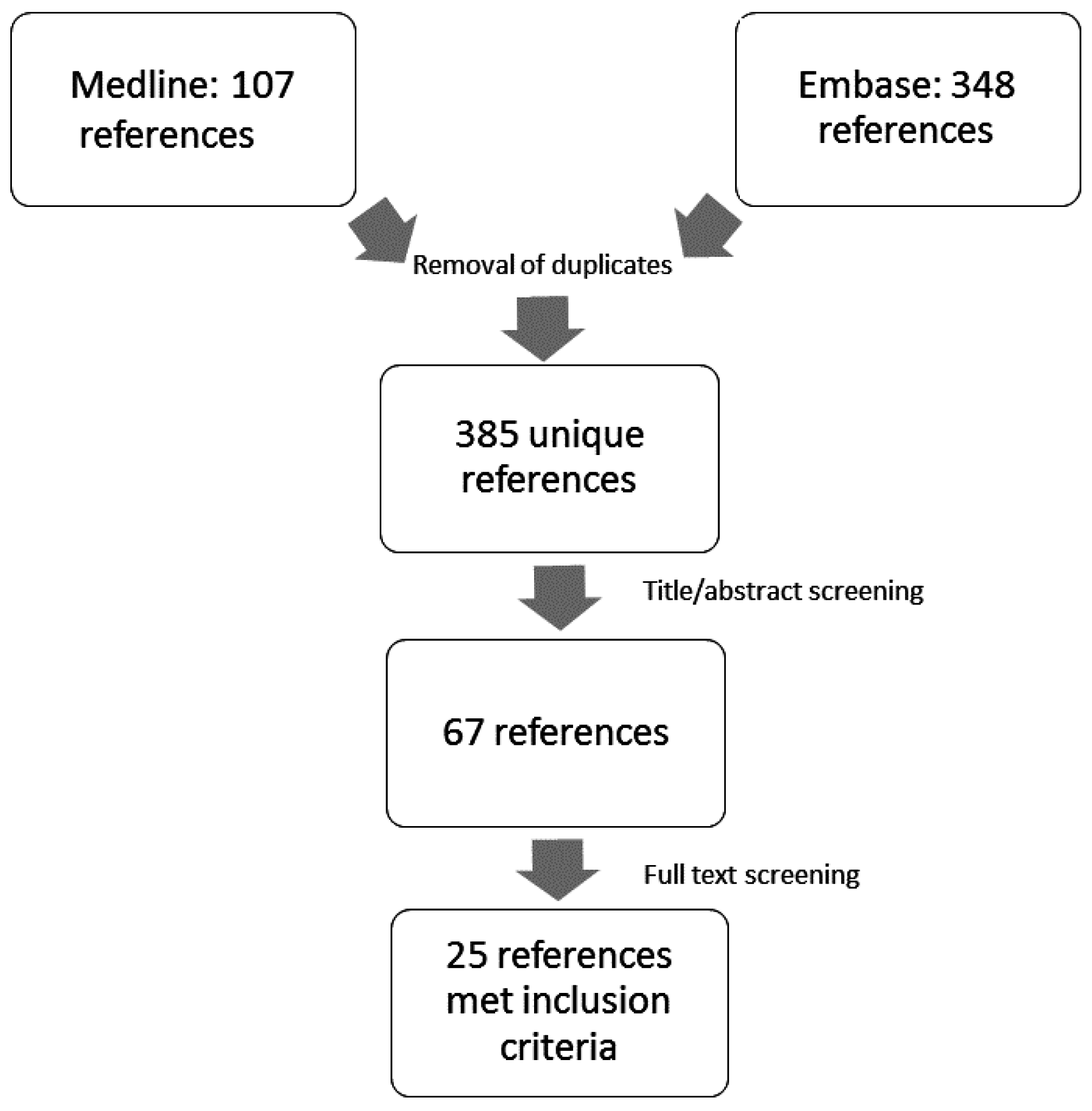
2. Methods
3. Results
3.1. Tobacco Smoke Exposure: Sources and Measurement
3.2. Tobacco Smoke Exposure in SCD: Prevalence and Associations
3.3. Tobacco Smoke Exposure: SCD Complications
3.3.1. Painful Vaso-Occlusive Crisis
3.3.2. Acute Chest Syndrome
3.3.3. Lower Airway Disease: Asthma and Pulmonary Function Abnormalities
3.3.4. Cardiovascular Morbidity
3.3.5. Other Effects of Tobacco Smoke Exposure in SCD
3.3.6. Tobacco Smoke Exposure and Mortality
3.3.7. Tobacco Smoke Exposure and SCD Morbidity: Potential Mechanisms
4. Areas for Future Research
5. Summary and Clinical Practice Recommendations
6. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kavanagh, P.L.; Sprinz, P.G.; Vinci, S.R.; Bauchner, H.; Wang, C.J. Management of children with sickle cell disease: A comprehensive review of the literature. Pediatrics 2011, 128, e1552–e1574. [Google Scholar] [CrossRef] [PubMed]
- Hassell, K.L. Population estimates of sickle cell disease in the U.S. Am. J. Prev. Med. 2010, 38, S512–S521. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Genomic Resource Centre: Genes and Human Disease. Available online: http://www.who.int/genomics/public/geneticdiseases/en/index2.html#SCA (accessed on 16 September 2016).
- Piel, F.B.; Patil, A.P.; Howes, R.E.; Nyangiri, O.A.; Gething, P.W.; Dewi, M.; Temperley, W.H.; Williams, T.N.; Weatherall, D.J.; Hay, S.I. Global epidemiology of sickle haemoglobin in neonates: A contemporary geostatistical model-based map and population estimates. Lancet 2013, 381, 142–151. [Google Scholar] [CrossRef]
- Gaston, M.H.; Verter, J.I.; Woods, G.; Pegelow, C.; Kelleher, J.; Presbury, G.; Zarkowsky, H.; Vichinsky, E.; Iyer, R.; Lobel, J.S.; et al. Prophylaxis with oral penicillin in children with sickle cell anemia. A randomized trial. N. Engl. J. Med. 1986, 314, 1593–1599. [Google Scholar] [CrossRef] [PubMed]
- Resar, L.M.; Oski, F.A. Cold water exposure and vaso-occlusive crises in sickle cell anemia. J. Pediatr. 1991, 118, 407–409. [Google Scholar] [CrossRef]
- Olaosebikan, R.; Ernest, K.; Bojang, K.; Mokuolu, O.; Rehman, A.M.; Affara, M.; Nwakanma, D.; Kiechel, J.R.; Ogunkunle, T.; Olagunju, T.; et al. A randomized trial to compare the safety, tolerability, and effectiveness of 3 antimalarial regimens for the prevention of malaria in nigerian patients with sickle cell disease. J. Infect. Dis. 2015, 212, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.T.; DeBaun, M.R.; Blinder, M.A.; Strunk, R.C.; Field, J.J. Smoking is associated with an increased risk of acute chest syndrome and pain among adults with sickle cell disease. Blood 2010, 115, 3852–3854. [Google Scholar] [CrossRef] [PubMed]
- Sadreameli, S.C.; Eakin, M.N.; Robinson, K.T.; Alade, R.O.; Strouse, J.J. Secondhand smoke is associated with more frequent hospitalizations in children with sickle cell disease. Am. J. Hematol. 2016, 91, 313–317. [Google Scholar] [CrossRef] [PubMed]
- West, D.C.; Romano, P.S.; Azari, R.; Rudominer, A.; Holman, M.; Sandhu, S. Impact of environmental tobacco smoke on children with sickle cell disease. Arch. Pediatr. Adolesc. Med. 2003, 157, 1197–1201. [Google Scholar] [CrossRef] [PubMed]
- Glassberg, J.A.; Wang, J.; Cohen, R.; Richardson, L.D.; DeBaun, M.R. Risk factors for increased ed utilization in a multinational cohort of children with sickle cell disease. Acad. Emerg. Med. 2012, 19, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Young, R.C., Jr.; Rachal, R.E.; Hackney, R.L., Jr.; Uy, C.G.; Scott, R.B. Smoking is a factor in causing acute chest syndrome in sickle cell anemia. J. Natl. Med. Assoc. 1992, 84, 267–271. [Google Scholar] [PubMed]
- Cohen, R.T.; Strunk, R.C.; Field, J.J.; Rosen, C.L.; Kirkham, F.J.; Redline, S.; Stocks, J.; Rodeghier, M.J.; DeBaun, M.R. Environmental tobacco smoke and airway obstruction in children with sickle cell anemia. Chest 2013, 144, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.; Bennett, J.; Brady, C.; Griffin, J. Tobacco smoke exposure and pulmonary function in children with sickle cell disease. Pediatr. Blood Cancer 2011, 56, 953. [Google Scholar]
- World Health Organization. Who Report on the Global Tobacco Epidemic. The Mpower Package. Available online: http://www.who.int/tobacco/mpower/en/ (accessed on 4 November 2016).
- U.S. Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2006.
- Yawn, B.P.; Buchanan, G.R.; Afenyi-Annan, A.N.; Ballas, S.K.; Hassell, K.L.; James, A.H.; Jordan, L.; Lanzkron, S.M.; Lottenberg, R.; Savage, W.J.; et al. Management of sickle cell disease: Summary of the 2014 evidence-based report by expert panel members. JAMA 2014, 312, 1033–1048. [Google Scholar] [CrossRef] [PubMed]
- Castro, O.; Brambilla, D.; Thorington, B.; Reindorf, C.; Scott, R.; Gillette, P.; Vera, J.; Levy, P. The acute chest syndrome in sickle cell disease: Incidence and risk factors. The cooperative study of sickle cell disease. Blood 1994, 84, 643–649. [Google Scholar] [PubMed]
- Martins-Green, M.; Adhami, N.; Frankos, M.; Valdez, M.; Goodwin, B.; Lyubovitsky, J.; Dhall, S.; Garcia, M.; Egiebor, I.; Martinez, B.; et al. Cigarette smoke toxins deposited on surfaces: Implications for human health. PLoS ONE 2014, 9, e86391. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, N.; Ozel, M.Z.; Lewis, A.C.; Marce, R.M.; Borrull, F.; Hamilton, J.F. Exposure to nitrosamines in thirdhand tobacco smoke increases cancer risk in non-smokers. Environ. Int. 2014, 71, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Glover, M.; Hadwen, G.; Chelimo, C.; Scragg, R.; Bullen, C.; Gentles, D.; Nosa, V.; McCool, J. Parent versus child reporting of tobacco smoke exposure at home and in the car. N. Z. Med. J. 2013, 126, 37–47. [Google Scholar] [PubMed]
- Spanier, A.J.; Kahn, R.S.; Xu, Y.; Hornung, R.; Lanphear, B.P. Comparison of biomarkers and parent report of tobacco exposure to predict wheeze. J. Pediatr. 2011, 159, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Kohler, E.; Sollich, V.; Schuster, R.; Thal, W. Passive smoke exposure in infants and children with respiratory tract diseases. Hum. Exp. Toxicol. 1999, 18, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.H.; Gomez, Y.; Homa, D.M.; King, B.A. Tobacco use, secondhand smoke, and smoke-free home rules in multiunit housing. Am. J. Prev. Med. 2016, 51, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Florescu, A.; Ferrence, R.; Einarson, T.; Selby, P.; Soldin, O.; Koren, G. Methods for quantification of exposure to cigarette smoking and environmental tobacco smoke: Focus on developmental toxicology. Ther. Drug Monit. 2009, 31, 14–30. [Google Scholar] [CrossRef] [PubMed]
- Lal, A.; Patterson, L.; Goldrich, A.; Marsh, A. Point-of-care end-tidal carbon monoxide reflects severity of hemolysis in sickle cell anemia. Pediatr. Blood Cancer 2015, 62, 912–914. [Google Scholar] [CrossRef] [PubMed]
- Britto, M.T.; Garrett, J.M.; Dugliss, M.A.J.; Daeschner, C.W., Jr.; Johnson, C.A.; Leigh, M.W.; Majure, J.M.; Schultz, W.H.; Konrad, T.R. Risky behavior in teens with cystic fibrosis or sickle cell disease: A multicenter study. Pediatrics 1998, 101, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Asnani, M.R.; Bhatt, K.; Younger, N.; McFarlane, S.; Francis, D.; Gordon-Strachan, G.; Reid, M.E. Risky behaviours of jamaican adolescents with sickle cell disease. Hematology 2014, 19, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Platt, O.S.; Brambilla, D.J.; Rosse, W.F.; Milner, P.F.; Castro, O.; Steinberg, M.H.; Klug, P.P. Mortality in sickle cell disease. Life expectancy and risk factors for early death. N. Engl. J. Med. 1994, 330, 1639–1644. [Google Scholar] [CrossRef] [PubMed]
- Vichinsky, E.P.; Neumayr, L.D.; Earles, A.N.; Williams, R.; Lennette, E.T.; Dean, D.; Nickerson, B.; Orringer, E.; McKie, V.; Bellevue, R.; et al. Causes and outcomes of the acute chest syndrome in sickle cell disease. National acute chest syndrome study group. N. Engl. J. Med. 2000, 342, 1855–1865. [Google Scholar] [CrossRef] [PubMed]
- Field, J.J.; Stocks, J.; Kirkham, F.J.; Rosen, C.L.; Dietzen, D.J.; Semon, T.; Kirkby, J.; Bates, P.; Seicean, S.; DeBaun, M.R.; et al. Airway hyperresponsiveness in children with sickle cell anemia. Chest 2011, 139, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Ozbek, O.Y.; Malbora, B.; Sen, N.; Yazici, A.C.; Ozyurek, E.; Ozbek, N. Airway hyperreactivity detected by methacholine challenge in children with sickle cell disease. Pediatr. Pulmonol. 2007, 42, 1187–1192. [Google Scholar] [CrossRef] [PubMed]
- Shilo, N.R.; Lands, L.C. Asthma and chronic sickle cell lung disease: A dynamic relationship. Paediatr. Respir. Rev. 2011, 12, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Stein, R.T.; Holberg, C.J.; Morgan, W.J.; Wright, A.L.; Lombardi, E.; Taussig, L.; Martinez, F.D. Peak flow variability, methacholine responsiveness and atopy as markers for detecting different wheezing phenotypes in childhood. Thorax 1997, 52, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Sears, M.R.; Jones, D.T.; Holdaway, M.D.; Hewitt, C.J.; Flannery, E.M.; Herbison, G.P.; Silva, P.A. Prevalence of bronchial reactivity to inhaled methacholine in New Zealand children. Thorax 1986, 41, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Anim, S.O.; Strunk, R.C.; DeBaun, M.R. Asthma morbidity and treatment in children with sickle cell disease. Expert Rev. Respir. Med. 2011, 5, 635–645. [Google Scholar] [CrossRef] [PubMed]
- Caboot, J.B.; Allen, J.L. Pulmonary complications of sickle cell disease in children. Curr. Opin. Pediatr. 2008, 20, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Manci, E.A.; Culberson, D.E.; Yang, Y.M.; Gardner, T.M.; Powell, R.; Haynes, J., Jr.; Shah, A.K.; Mankad, V.N. Causes of death in sickle cell disease: An autopsy study. Br. J. Haematol. 2003, 123, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Boyd, J.H.; Macklin, E.A.; Strunk, R.C.; DeBaun, M.R. Asthma is associated with acute chest syndrome and pain in children with sickle cell anemia. Blood 2006, 108, 2923–2927. [Google Scholar] [CrossRef] [PubMed]
- Boyd, J.H.; Macklin, E.A.; Strunk, R.C.; DeBaun, M.R. Asthma is associated with increased mortality in individuals with sickle cell anemia. Haematologica 2007, 92, 1115–1118. [Google Scholar] [CrossRef] [PubMed]
- Boyd, J.H.; DeBaun, M.R.; Morgan, W.J.; Mao, J.; Strunk, R.C. Lower airway obstruction is associated with increased morbidity in children with sickle cell disease. Pediatr. Pulmonol. 2009, 44, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Koumbourlis, A.C.; Zar, H.J.; Hurlet-Jensen, A.; Goldberg, M.R. Prevalence and reversibility of lower airway obstruction in children with sickle cell disease. J. Pediatr. 2001, 138, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.; Dottin, N.; Hughes, S.; Strachan, D.; Davis, G.; Charles, K.S.; Rios, M.; Seemungal, T.A. Restriction is related to stable hemoglobin in adult west indian sickle cell disease patients. Am. J. Respir. Crit. Care Med. 2011, 183, A3043. [Google Scholar]
- Helvaci, M.R.; Acipayam, C.; Aydogan, A.; Akkucuk, S.; Oruc, C.; Gokce, C. Acute chest syndrome in severity of sickle cell diseases. Int. J. Clin. Exp. Med. 2014, 7, 5790–5795. [Google Scholar] [PubMed]
- Helvaci, M.R.; Gokce, C.; Sahan, M.; Hakimoglu, S.; Coskun, M.; Gozukara, K.H. Venous involvement in sickle cell diseases. Int. J. Clin. Exp. Med. 2016, 9, 11950–11957. [Google Scholar]
- Bennett, J.M.; Nelson, S.C. Tobacco smoke exposure and stroke risk in children with sickle cell disease. Am. J. Hematol. 2012, 87, E62. [Google Scholar]
- Helvaci, M.R.; Gokce, C.; Davran, R.; Akkucuk, S.; Ugur, M.; Oruc, C. Mortal quintet of sickle cell diseases. Int. J. Clin. Exp. Med. 2015, 8, 11442–11448. [Google Scholar] [PubMed]
- Passos, C.P.; Santos, P.R.; Aguiar, M.C.; Cangussu, M.C.; Toralles, M.B.; da Silva, M.C.; Nascimento, R.J.; Campos, M.I. Sickle cell disease does not predispose to caries or periodontal disease. Spec. Care Dent. 2012, 32, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.; Chughtai, M.; Malik, A.A.; Qureshi, A.I.; Suri, F.K. Central retinal artery occlusion in patients with sickle cell disease. Stroke 2015, 46. [Google Scholar]
- Helvaci, M.R.; Sevinc, A.; Camci, C.; Keskin, A. Smoking and sickle cell diseases. Exp. Clin. Cardiol. 2014, 20, 3706–3722. [Google Scholar]
- Novelli, E.M.; Huynh, C.; Gladwin, M.T.; Moore, C.G.; Ragni, M.V. Pulmonary embolism in sickle cell disease: A case-control study. JTH 2012, 10, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Rajpal, S.; Hilbun, J.; Dwary, A.; Smith, T.; Mina, G.; Reddy, P.C.; Akkus, N.I. Troponin elevation correlates with pulmonary hypertension and hemolytic burden in sickle cell pain crisis. Eur. Heart J. 2013, 34, 39. [Google Scholar] [CrossRef]
- Sarrai, M.; Duroseau, H.; D’Augustine, J.; Moktan, S.; Bellevue, R. Bone mass density in adults with sickle cell disease. Br. J. Haematol. 2007, 136, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Drake, M.T.; Murad, M.H.; Mauck, K.F.; Lane, M.A.; Undavalli, C.; Elraiyah, T.; Stuart, L.M.; Prasad, C.; Shahrour, A.; Mullan, R.J.; et al. Clinical review. Risk factors for low bone mass-related fractures in men: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2012, 97, 1861–1870. [Google Scholar] [CrossRef] [PubMed]
- Ward, K.D.; Klesges, R.C. A meta-analysis of the effects of cigarette smoking on bone mineral density. Calcif. Tissue Int. 2001, 68, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Maluf, S.; Pra, D.; Friedrisch, J.R.; Bittar, C.; da Silva, M.A.; Henriques, J.A.; Silla, L. Length of treatment and dose as determinants of mutagenicity in sickle cell disease patients treated with hydroxyurea. Environ. Toxicol. Pharmacol. 2009, 27, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Pulte, D.; Axelrod, D. Erythropoietin level in sickle cell disease patients not in crisis. Haematologica 2013, 98, 693. [Google Scholar]
- Knight-Madden, J.M.; Barton-Gooden, A.; Weaver, S.R.; Reid, M.; Greenough, A. Mortality, asthma, smoking and acute chest syndrome in young adults with sickle cell disease. Lung 2013, 191, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Adams, T.; Wan, E.; Wei, Y.; Wahab, R.; Castagna, F.; Wang, G.; Emin, M.; Russo, C.; Homma, S.; Le Jemtel, T.H.; et al. Secondhand smoking is associated with vascular inflammation. Chest 2015, 148, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.W.; Shelton, L.; Watanabe, I.S.; Arnold, J. Passive smoking affects endothelium and platelets. Arch. Intern. Med. 1989, 149, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Gentner, N.J.; Weber, L.P. Secondhand tobacco smoke, arterial stiffness, and altered circadian blood pressure patterns are associated with lung inflammation and oxidative stress in rats. Am. J. Physiol. Heart Circ. Physiol. 2012, 302, H818–H825. [Google Scholar] [CrossRef] [PubMed]
- Niki, E.; Minamisawa, S.; Oikawa, M.; Komuro, E. Membrane damage from lipid oxidation induced by free radicals and cigarette smoke. Ann. N. Y. Acad. Sci. 1993, 686, 29–37. [Google Scholar] [CrossRef] [PubMed]
- German, A.K. The erythrocyte composition of the peripheral blood in tobacco smokers. Lik. Sprava. 1992, 7, 40–42. [Google Scholar]
- Minamisawa, S.; Komuro, E.; Niki, E. Hemolysis of rabbit erythrocytes induced by cigarette smoke. Life Sci. 1990, 47, 2207–2215. [Google Scholar] [CrossRef]
- Padmavathi, P.; Reddy, V.D.; Kavitha, G.; Paramahamsa, M.; Varadacharyulu, N. Chronic cigarette smoking alters erythrocyte membrane lipid composition and properties in male human volunteers. Nitric Oxide 2010, 23, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Xu, C.; Manwani, D.; Frenette, P.S. Neutrophils, platelets, and inflammatory pathways at the nexus of sickle cell disease pathophysiology. Blood 2016, 127, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Nouraie, M.; Lee, J.S.; Zhang, Y.; Kanias, T.; Zhao, X.; Xiong, Z.; Oriss, T.B.; Zeng, Q.; Kato, G.J.; Gibbs, J.S.; et al. The relationship between the severity of hemolysis, clinical manifestations and risk of death in 415 patients with sickle cell anemia in the U.S. and Europe. Haematologica 2013, 98, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Chikezie, P.C.; Akuwudike, A.R.; Chikezie, C.M. Polymerization studies of sickle cell hemoglobin incubated in aqueous leaf extract of nicotiana tabacum product. Res. J. Med. Plant 2013, 7, 92–99. [Google Scholar] [CrossRef]
- Kassim, A.A.; Payne, A.B.; Rodeghier, M.; Macklin, E.A.; Strunk, R.C.; DeBaun, M.R. Low forced expiratory volume is associated with earlier death in sickle cell anemia. Blood 2015, 126, 1544–1550. [Google Scholar] [CrossRef] [PubMed]
- Kopp, B.T.; Sarzynski, L.; Khalfoun, S.; Hayes, D., Jr.; Thompson, R.; Nicholson, L.; Long, F.; Castile, R.; Groner, J. Detrimental effects of secondhand smoke exposure on infants with cystic fibrosis. Pediatr. Pulmonol. 2014, 50, 25–34. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Authors | N Exposed/N Total (% with Secondhand Smoke Exposure) | Population | Exposure Measure | Outcome(s) | Magnitude of Association (95% CI) |
|---|---|---|---|---|---|
| West et al., 2003 [10] | 22/52 (42%) | Children | Questionnaire | Hospitalizations for pain and ACS (risk ratio) | 1.9 (1.3–2.7) |
| Cohen et al., 2010 [8] | 18/106 (17%) | Adults | Questionnaire | Hospitalizations for ACS (risk ratio) | 2.62 (1.05–6.57) |
| Glassberg et al., 2012 [11] | 218/810 (27%) | Children | Questionnaire | ED visits for ACS (rate ratio) | 1.73 (1.09–2.74) |
| Cohen et al., 2013 [13] | 70/245 (29%) current | Children | Questionnaire | Lower airway obstruction † | 22% vs. 3.1% * (p < 0.001) |
| 126/245 (51%) * any (current or prior) | Bronchodilator response >12% | 23% vs. 11% * (p = 0.03) | |||
| Sadreameli et al., 2015 [9] | 22/49 (45%) | Children | Salivary cotinine ≥0.5 ng/mL | Hospitalizations for pain and ACS (incidence risk ratio) | 3.7 (1.8–8) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sadreameli, S.C.; Kopp, B.T.; Creary, S.E.; Eakin, M.N.; McGrath-Morrow, S.; Strouse, J.J. Secondhand Smoke Is an Important Modifiable Risk Factor in Sickle Cell Disease: A Review of the Current Literature and Areas for Future Research. Int. J. Environ. Res. Public Health 2016, 13, 1131. https://doi.org/10.3390/ijerph13111131
Sadreameli SC, Kopp BT, Creary SE, Eakin MN, McGrath-Morrow S, Strouse JJ. Secondhand Smoke Is an Important Modifiable Risk Factor in Sickle Cell Disease: A Review of the Current Literature and Areas for Future Research. International Journal of Environmental Research and Public Health. 2016; 13(11):1131. https://doi.org/10.3390/ijerph13111131
Chicago/Turabian StyleSadreameli, S. Christy, Benjamin T. Kopp, Susan E. Creary, Michelle N. Eakin, Sharon McGrath-Morrow, and John J. Strouse. 2016. "Secondhand Smoke Is an Important Modifiable Risk Factor in Sickle Cell Disease: A Review of the Current Literature and Areas for Future Research" International Journal of Environmental Research and Public Health 13, no. 11: 1131. https://doi.org/10.3390/ijerph13111131