
Short-Term Effects of Fine Particulate Matter and Temperature on Lung Function among Healthy College Students in Wuhan, China

 ,
, 
Abstract
:1. Introduction
2. Objects and Methods
2.1. Study Participants and Design
2.2. Lung Function Testing
2.3. Environmental Measurements
2.4. Statistical Analysis
3. Results
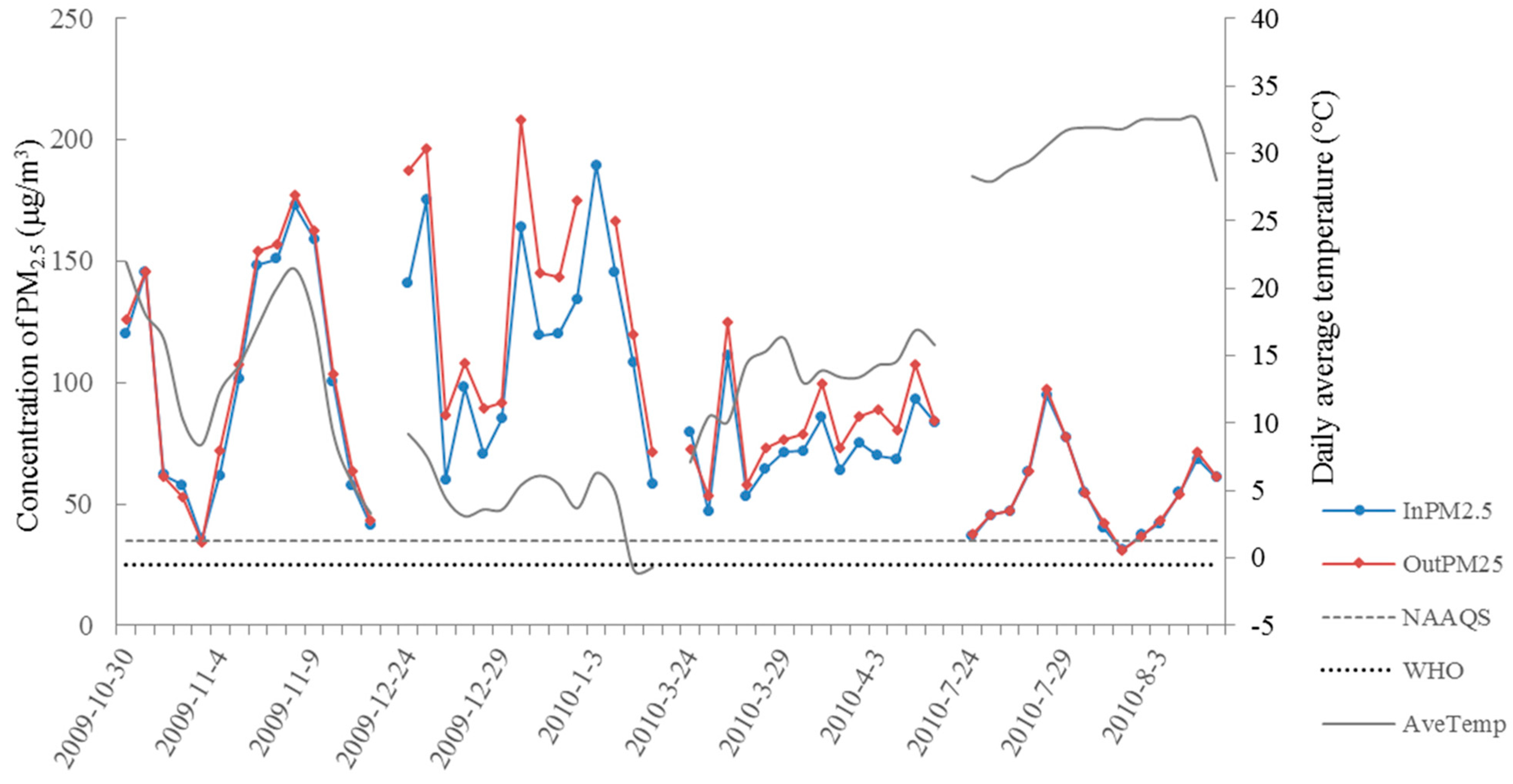
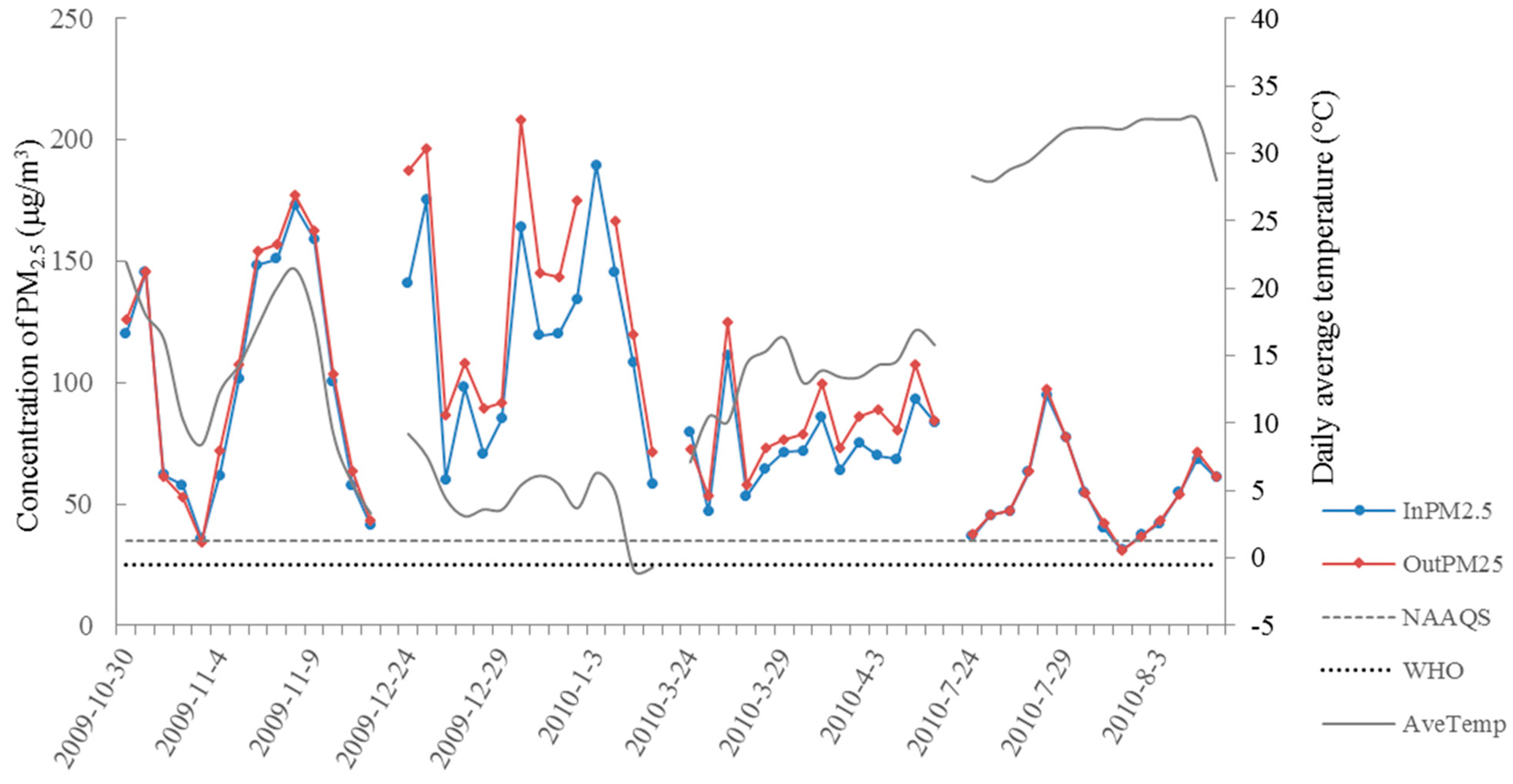
3.1. Descriptive Statistics of Health and Exposure Data

{kind=link}
{kind=link}
| Characteristics | Male | Female | All |
|---|---|---|---|
| (n = 18) | (n = 19) | (n = 37) | |
| Basic information of subjects | |||
| Age (year) a | 22.0(0.9) b | 21.5(0.6) | 21.7(0.8) |
| Height (cm) | 171.7(6.0) | 158.6(3.8) | 164.9(8.3) |
| Weight (kg) | 59.1(5.8) | 50.6(5.8) | 54.7(7.1) |
| Out time (hours/day) c | 1.2(0.9) | 2.1(1.0) | 1.7(1.1) |
| No. of PEF measurements | |||
| N a.m. | 46.9(10.1) | 48.1(7.1) | 47.5(8.9) |
| N p.m. | 46.9(11.2) | 49.3(6.4) | 48.1(9.0) |
| Mean PEF (L/min) | |||
| Morning PEF | 580.2(98.9) | 378.1(53.8) | 475.2(128.1) |
| Evening PEF | 582.9(94.9) | 381.6(50.2) | 477.0(125.3) |
| Spring (N = 14) | Summer (N = 14) | Autumn (N = 14) | Winter (N = 14) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean(sd) | Median | Min/Max | Mean(sd) | Median | Min/Max | Mean(sd) | Median | Min/Max | Mean(sd) | Median | Min/Max | |
| Indoor | ||||||||||||
| PM2.5 (μg/m3) | 74.1(16.2) | 71.5 | 46.9/110.8 | 53.8(17.8) | 50.8 | 31.1/94.5 | 91.3(43.7) | 93.5 | 29.2/149.6 | 110.6(42.3) | 112.1 | 49.3/184.2 |
| Temperature (°C) | 18.5(2.8) | 19.1 | 14.2/22.7 | 33.9(2.5) | 34.5 | 29.4/37.4 | 19.6(2.2) | 19.5 | 16.3/23.0 | 11.4(0.8) | 11.2 | 10.3/12.6 |
| Humidity (%) | 55.6(6.5) | 54.5 | 45.7/69.1 | 64.3(7.8) | 64.0 | 54.2/74.8 | 56.0(11.7) | 55.3 | 36.0/75.2 | 62.4(6.3) | 61.9 | 50.6/75.8 |
| Outdoor | ||||||||||||
| PM2.5 (μg/m3) a | 82.6(18.7) | 79.5 | 53.4/124.7 | 54.5(18.3) | 50.5 | 31.0/97.4 | 104.2(49.4) | 106.6 | 34.0/177.7 | 143.5(51.2) | 144.9 | 71.2/288.9 |
| Temperature (°C) | 15.7(2.8) | 16.0 | 9.6/20.4 | 33.3(1.9) | 33.5 | 29.8/36.1 | 16.7(5.2) | 18.3 | 7.0/22.4 | 7.8(2.5) | 7.9 | 3.8/12.0 |
| Humidity (%) | 61.0(12.2) | 58.2 | 44.2/82.4 | 66.4(6.3) | 66.9 | 57.3/76.3 | 64.4(13.7) | 66.8 | 38.0/80.0 | 55.7(10.2) | 57.9 | 37.9/67.0 |
| Liyuan b | ||||||||||||
| PM10 (μg/m3) | 112.7(38.9) | 118.0 | 60.0/190.0 | 67.6(16.7) | 66.0 | 43.0/102.0 | 94.4(54.9) | 83.0 | 20.0/176.0 | 151.3(45.9) | 161.0 | 52.0/240.0 |
| SO2 (μg/m3) | 39.1(18.9) | 42.5 | 9.0/62.0 | 19.0(8.0) | 19.0 | 5.0/30.0 | 39.7(21.8) | 45.0 | 11.0/80.0 | 56.0(11.9) | 58.0 | 26.0/80.0 |
| NO2 (μg/m3) | 41.9(12.8) | 41.6 | 20.8/64.0 | 26.3(7.2) | 25.6 | 14.4/41.6 | 50.0(26.2) | 40.8 | 22.4/95.2 | 53.5(17.8) | 50.4 | 22.4/86.4 |
3.2. Correlation Matrix between Environmental Variables
| InPM2.5 | SO2 a | NO2 a | InTemp. | OutTemp. | InRh (%) | OutRh (%) | |
|---|---|---|---|---|---|---|---|
| OutPM2.5 | 0.942 | 0.589 | 0.759 | −0.529 | −0.406 | 0.202 | −0.038 |
| InPM2.5 | — | 0.505 | 0.693 | −0.406 | −0.260 | 0.245 | 0.046 |
| SO2 a | — | — | 0.712 | −0.571 | −0.419 | −0.138 | −0.519 |
| NO2 a | — | — | — | −0.500 | −0.326 | −0.003 | −0.248 |
| InTemp. | — | — | — | — | 0.921 | 0.256 | 0.354 |
| OutTemp. | — | — | — | — | 0.329 | 0.219 | |
| InRh (%) | — | — | — | — | — | 0.612 |
3.3. Global and Seasonally Stratified Analysis of the Estimated Effects of PM2.5 and Temperature
3.3.1. Global Analysis of the Effects of PM2.5 and Temperature on lag 0
| Morning PEF | Evening PEF | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Indoor | Outdoor | Indoor | Outdoor | |||||||||
| β | 95%CI | P | β | 95%CI | P | β | 95%CI | P | β | 95%CI | P | |
| Single-pollutant model | ||||||||||||
| PM2.5, 10 μg/m3 | −1.08 | (−2.95,0.80) | 0.262 | 0.07 | (−1.44,1.57) | 0.929 | −2.09 | (−3.73,−0.51) | 0.015 | −1.29 | (−2.75,0.17) | 0.084 |
| Temp., 1 °C | −1.58 | (−2.86,−0.30) | 0.016 | −0.84 | (−1.63,−0.04) | 0.039 | −2.16 | (−3.67,−0.65) | 0.005 | −1.22 | (−2.22,−0.22) | 0.017 |
| PM2.5*Temp. | 0.00 | (−0.01,0.01) | 0.598 | 0.00 | (−0.01,0.01) | 0.968 | 0.01 | (0.00,0.02) | 0.033 | 0.01 | (0.00,0.02) | 0.043 |
| Two-pollutant model (SO2) | ||||||||||||
| SO2, 10 μg/m3 | −0.12 | (−1.41,0.17) | 0.851 | 0.31 | (−1.11,1.72) | 0.670 | 0.74 | (−0.10,1.59) | 0.086 | 1.14 | (−0.29,2.57) | 0.205 |
| PM2.5, 10 μg/m3 | −1.05 | (−2.96,0.85) | 0.279 | −0.01 | (−1.51,1.48) | 0.987 | −2.17 | (−3.81,−0.52) | 0.010 | −1.27 | (−2.73,0.18) | 0.087 |
| Temp., 1 °C | −1.60 | (−2.93,−0.26) | 0.019 | −0.83 | (−1.63,−0.03) | 0.043 | −2.12 | (−3.62,−0.63) | 0.005 | −1.27 | (−2.28,−0.26) | 0.014 |
| PM2.5*Temp. | 0.00 | (−0.01,0.02) | 0.592 | 0.00 | (−0.01,0.01) | 0.967 | 0.01 | (0.00,0.02) | 0.038 | 0.01 | (0.00,0.02) | 0.067 |
| Two-pollutant model (NO2) | ||||||||||||
| NO2, 10 μg/m3 | 0.41 | (−1.20,2.02) | 0.619 | 1.01 | (−0.65,2.67) | 0.232 | 0.25 | (−1.12,1.61) | 0.724 | 1.17 | (−0.44,2.79) | 0.153 |
| PM2.5, 10 μg/m3 | −1.23 | (−3.24,0.77) | 0.228 | −0.34 | (−1.99,1.31) | 0.686 | −2.18 | (−3.96,−0.41) | 0.016 | −1.54 | (−3.03,−0.04) | 0.044 |
| Temp., 1 °C | −1.51 | (−2.86,−0.16) | 0.029 | −0.79 | (−1.61,0.03) | 0.060 | −2.15 | (−3.67,0.63) | 0.006 | −1.34 | (−2.37,−0.30) | 0.011 |
| PM2.5*Temp. | 0.00 | (−0.01,0.01) | 0.613 | 0.00 | (−0.01,0.01) | 0.979 | 0.01 | (0.00,0.02) | 0.033 | 0.01 | (0.00,0.02) | 0.058 |
3.3.2. Lagged and Cumulative Effects of PM2.5 and Temperature on PEF

3.3.3. Seasonally Stratified Analysis of the Effects of PM2.5 and Temperature
| Variables | Morning PEF | Evening PEF | ||||
|---|---|---|---|---|---|---|
| β | 95%CI | P | β | 95%CI | P | |
| Spring | ||||||
| PM2.5, 10 μg/m3 | 0.53 | (−0.91,1.96) | 0.472 | −0.81 | (−3.11,1.49) | 0.490 |
| Temp., 1 °C | −0.44 | (−1.65,0.77) | 0.477 | −0.46 | (−1.59,0.68) | 0.430 |
| Summer | ||||||
| PM2.5, 10 μg/m3 | −1.77 | (−4.51,0.97) | 0.204 | −1.14 | (−4.11,1.83) | 0.452 |
| Temp.,1 °C | −7.75 | (−21.66,6.16) | 0.275 | 1.66 | (−7.58,10.91) | 0.724 |
| Autumn | ||||||
| PM2.5, 10 μg/m3 | 0.30 | (−0.77,1.37) | 0.585 | 0.62 | (−0.40,1.65) | 0.233 |
| Temp., 1 °C | −1.01 | (−1.88,−0.13) | 0.024 | −0.93 | (−1.89,0.04) | 0.060 |
| Winter | ||||||
| PM2.5, 10 μg/m3 | −0.40 | (−2.08,1.28) | 0.639 | −1.28 | (−2.50,−0.06) | 0.040 |
| Temp., 1 °C | −0.24 | (−2.95,2.48) | 0.865 | 2.07 | (0.34,3.80) | 0.019 |
4. Discussion
4.1. Effects of PM2.5 on Lung Function
4.2. Effects of Temperature on Lung Function
4.3. Interactive Effects between PM2.5 and Temperature on Lung Function
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Anderson, J.O.; Thundiyil, J.G.; Stolbach, A. Clearing the air: A review of the effects of particulate matter air pollution on human health. J. Med. Toxicol. 2012, 8, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Dockery, D.W.; Stone, P.H. Cardiovascular risks from fine particulate air pollution. N. Engl. J. Med. 2007, 356, 511–513. [Google Scholar] [CrossRef] [PubMed]
- Strak, M.; Janssen, N.A.; Godri, K.J.; Gosens, I.; Mudway, I.S.; Cassee, F.R.; Lebret, E.; Kelly, F.J.; Harrison, R.M.; Brunekreef, B.; et al. Respiratory health effects of airborne particulate matter: The role of particle size, composition, and oxidative potential-the RAPTES project. Environ. Health Perspect. 2012, 120, 1183–1189. [Google Scholar] [CrossRef] [PubMed]
- Krewski, D. Evaluating the effects of ambient air pollution on life expectancy. N. Engl. J. Med. 2009, 360, 413–415. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., 3rd; Ezzati, M.; Dockery, D.W. Fine-particulate air pollution and life expectancy in the United States. N. Engl. J. Med. 2009, 360, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010 a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Kesavachandran, C.; Pangtey, B.S.; Bihari, V.; Fareed, M.; Pathak, M.K.; Srivastava, A.K.; Mathur, N. Particulate matter concentration in ambient air and its effects on lung functions among residents in the National Capital Region, India. Environ. Monit. Assess. 2013, 185, 1265–1272. [Google Scholar] [CrossRef] [PubMed]
- Penttinen, P.; Timonen, K.L.; Tiittanen, P.; Mirme, A.; Ruuskanen, J.; Pekkanen, J. Number concentration and size of particles in urban air: Effects on spirometric lung function in adult asthmatic subjects. Environ. Health Perspect. 2001, 109, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Deng, F.; Wang, X.; Wei, H.; Shima, M.; Huang, J.; Lv, H.; Hao, Y.; Zheng, C.; Qin, Y.; et al. Association of lung function in a panel of young healthy adults with various chemical components of ambient fine particulate air pollution in Beijing, China. Atmos. Environ. 2013, 77, 873–884. [Google Scholar] [CrossRef]
- Yamazaki, S.; Shima, M.; Ando, M.; Nitta, H.; Watanabe, H.; Nishimuta, T. Effect of hourly concentration of particulate matter on peak expiratory flow in hospitalized children: A panel study. Environ. Health 2011, 10, 944–956. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Raaschou-Nielsen, O. Impact of fine particles in ambient air on lung cancer. Chin. J. Cancer 2014, 33, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Peng, R.D.; Meng, X.; Zhou, Z.; Chen, B.; Kan, H. Seasonal variation in the acute effect of particulate air pollution on mortality in the China Air Pollution and Health Effects Study (CAPES). Sci. Total Environ. 2013, 450–451, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Li, S.; Zhang, Y.; Armstrong, B.; Jaakkola, J.J.; Tong, S.; Pan, X. Extremely cold and hot temperatures increase the risk of ischaemic heart disease mortality: Epidemiological evidence from China. Heart 2013, 99, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Stafoggia, M.; Schwartz, J.; Forastiere, F.; Perucci, C.A.; Group, S. Does temperature modify the association between air pollution and mortality? A multicity case-crossover analysis in Italy. Am. J. Epidemiol. 2008, 167, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- Nawrot, T.S.; Torfs, R.; Fierens, F.; de Henauw, S.; Hoet, P.H.; van Kersschaever, G.; de Backer, G.; Nemery, B. Stronger associations between daily mortality and fine particulate air pollution in summer than in winter: Evidence from a heavily polluted region in western Europe. J. Epidemiol. Community Health 2007, 61, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Zhang, Y.; Zhao, Z.; Duan, X.; Xu, X.; Kan, H. Temperature modifies the acute effect of particulate air pollution on mortality in eight Chinese cities. Sci. Total Environ. 2012, 435–436, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; He, Q.; Lin, H.M.; Kong, L.; Bentley, C.M.; Liu, W.; Zhou, D. High temperatures enhanced acute mortality effects of ambient particle pollution in the “oven” city of Wuhan, China. Environ. Health Perspect. 2008, 116, 1172–1178. [Google Scholar] [CrossRef] [PubMed]
- Shaposhnikov, D.; Revich, B.; Bellander, T.; Bedada, G.B.; Bottai, M.; Kharkova, T.; Kvasha, E.; Lezina, E.; Lind, T.; Semutnikova, E.; et al. Mortality related to air pollution with the Moscow heat wave and wildfire of 2010. Epidemiology 2014, 25, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Collaco, J.M.; McGready, J.; Green, D.M.; Naughton, K.M.; Watson, C.P.; Shields, T.; Bell, S.C.; Wainwright, C.E.; Group, A.S.; Cutting, G.R. Effect of temperature on cystic fibrosis lung disease and infections: A replicated cohort study. PLoS ONE 2011, 6, e27784. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, G.C.; Seemungal, T.; Jeffries, D.J.; Wedzicha, J.A. Effect of temperature on lung function and symptoms in chronic obstructive pulmonary disease. Eur. Respir. J. 1999, 13, 844–849. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Baker, P.J.; Jalaludin, B.B.; Marks, G.B.; Denison, L.S.; Williams, G.M. Ambient temperature and lung function in children with asthma in Australia. Eur. Respir. J. 2014, 43, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Deng, F.; Hao, Y.; Wang, X.; Zheng, C.; Lv, H.; Lu, X.; Wei, H.; Huang, J.; Qin, Y.; et al. Fine particulate matter, temperature, and lung function in healthy adults: Findings from the HVNR study. Chemosphere 2014, 108, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Gehring, U.; Gruzieva, O.; Agius, R.M.; Beelen, R.; Custovic, A.; Cyrys, J.; Eeftens, M.; Flexeder, C.; Fuertes, E.; Heinrich, J.; et al. Air pollution exposure and lung function in children: The ESCAPE project. Environ. Health Perspect. 2013, 121, 1357–1364. [Google Scholar] [PubMed]
- Jacobson, L.S.V.; Hacon Sde, S.; Castro, H.A.; Ignotti, E.; Artaxo, P.; Ponce de Leon, A.C. Association between fine particulate matter and the peak expiratory flow of schoolchildren in the Brazilian subequatorial Amazon: A panel study. Environ. Res. 2012, 117, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Meneses, F.; Ruiz, S.; Sienra, J.J.; Huerta, J.; White, M.C.; Etzel, R.A. Effects of air pollution on the respiratory health of asthmatic children living in Mexico City. Am. J. Respir. Crit. Care Med. 1996, 154, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Ward, D.J.; Ayres, J.G. Particulate air pollution and panel studies in children: A systematic review. Occup. Environ. Med. 2004, 61, e13. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Zanobetti, A.; Dominici, F. Evidence on vulnerability and susceptibility to health risks associated with short-term exposure to particulate matter: A systematic review and meta-analysis. Am. J. Epidemiol. 2013, 178, 865–876. [Google Scholar] [CrossRef] [PubMed]
- Tiittanen, P.; Timonen, K.L.; Ruuskanen, J.; Mirme, A.; Pekkanen, J. Fine particulate air pollution, resuspended road dust and respiratory health among symptomatic children. Eur. Respir. J. 1999, 13, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Roemer, W.; Hoek, G.; Brunekreef, B.; Haluszka, J.; Kalandidi, A.; Pekkanen, J. Daily variations in air pollution and respiratory health in a multicentre study: The PEACE project. Pollution Effects on Asthmatic Children in Europe. Eur. Respir. J. 1998, 12, 1354–1361. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Shima, M.; Yoda, Y.; Yamamoto, H.; Nakai, S.; Tamura, K.; Nitta, H.; Watanabe, H.; Nishimuta, T. Effects of airborne particulate matter on respiratory morbidity in asthmatic children. J. Epidemiol. 2008, 18, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Delfino, R.J.; Quintana, P.J.E.; Floro, J.; Gastañaga, V.M.; Samimi, B.S.; Kleinman, M.T.; Liu, L.J.S.; Bufalino, C.; Wu, C.-F.; McLaren, C.E. Association of FEV1 in asthmatic children with personal and microenvironmental exposure to airborne particulate matter. Environ. Health Perspect. 2004, 112, 932–941. [Google Scholar] [CrossRef] [PubMed]
- Long, C.M.; Suh, H.H.; Kobzik, L.; Catalano, P.J.; Ning, Y.Y.; Koutrakis, P. A pilot investigation of the relative toxicity of indoor and outdoor fine particles: In vitro effects of endotoxin and other particulate properties. Environ. Health Perspect. 2001, 109, 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Mann, M.; Patel, K.; Reardon, J.Z.; Goldstein, M.; Godar, T.J.; ZuWallack, R.L. The influence of spring and summer New England meteorologic conditions on the respiratory status of patients with chronic lung disease. Chest 1993, 103, 1369–1374. [Google Scholar] [CrossRef] [PubMed]
- Belli, A.; Diette, G.; Williams, D.; Matsui, E.; Peng, R.; Breysse, P.; Hansel, N.; McCormack, M.; Paulin, L. Colder outdoor temperature is associated with increased copd morbidity. Am. J. Respir. Crit. Care Med. 2014, 189, A2202. [Google Scholar]
- Pierse, N.; Arnold, R.; Keall, M.; Howden-Chapman, P.; Crane, J.; Cunningham, M.; Heating, H.; Health Study, G. Modelling the effects of low indoor temperatures on the lung function of children with asthma. J. Epidemiol. Community Health 2013, 67, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Barnett, A.G.; Pan, X.; Yu, W.; Tong, S. The impact of temperature on mortality in Tianjin, china: A case-crossover design with a distributed lag nonlinear model. Environ. Health Perspect. 2011, 119, 1719–1725. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Mengersen, K.; Wang, X.; Ye, X.; Guo, Y.; Pan, X.; Tong, S. Daily average temperature and mortality among the elderly: A meta-analysis and systematic review of epidemiological evidence. Int. J. Biometeorol. 2012, 56, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Medina-Ramon, M.; Schwartz, J. Temperature, temperature extremes, and mortality: A study of acclimatisation and effect modification in 50 US cities. Occup. Environ. Med. 2007, 64, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Cirendunzhu; Woodward, A.; Dawa; Zhaxisangmu; Chen, B.; Liu, Q. Temperature, hospital admissions and emergency room visits in Lhasa, Tibet: A time-series analysis. Sci. Total Environ. 2014, 490, 838–848. [Google Scholar] [CrossRef] [PubMed]
- Park, A.K.; Hong, Y.C.; Kim, H. Effect of changes in season and temperature on mortality associated with air pollution in Seoul, Korea. J. Epidemiol. Community Health 2011, 65, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Pan, W.H.; Li, L.A.; Tsai, M.J. Temperature extremes and mortality from coronary heart disease and cerebral infarction in elderly Chinese. Lancet 1995, 345, 353–355. [Google Scholar] [CrossRef]
- Ye, X.; Wolff, R.; Yu, W.; Vaneckova, P.; Pan, X.; Tong, S. Ambient temperature and morbidity: A review of epidemiological evidence. Environ. Health Perspect. 2012, 120, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.D.; Daviskas, E. The mechanism of exercise-induced asthma is …. J. Allergy Clin. Immunol. 2000, 106, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.D.; Dominici, F.; Pastor-Barriuso, R.; Zeger, S.L.; Samet, J.M. Seasonal analyses of air pollution and mortality in 100 US cities. Am. J. Epidemiol. 2005, 161, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; Lin, H.M.; Stewart, W.F.; Kong, L.; Xu, F.; Zhou, D.; Zhu, Z.; Liang, S.; Chen, W.; Shah, N.; et al. Seasonal pattern of the acute mortality effects of air pollution. J. Air Waste Manag. Assoc. 2010, 60, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Ito, K.; Lall, R.; Lippmann, M.; Thurston, G. Time-series analysis of mortality effects of fine particulate matter components in Detroit and Seattle. Environ. Health Perspect. 2011, 119, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C. Role of environmental stress in the physiological response to chemical toxicants. Environ. Res. 2003, 92, 1–7. [Google Scholar] [CrossRef]
- Reid, C.E.; Snowden, J.M.; Kontgis, C.; Tager, I.B. The role of ambient ozone in epidemiologic studies of heat-related mortality. Environ. Health Perspect. 2012, 120, 1627–1630. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.P.; Samet, J.M.; Richardson, D.B. Commentary: Does air pollution confound studies of temperature? Epidemiology 2014, 25, 242–245. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; He, M.; Wu, S.; Zhu, Y.; Wang, S.; Shima, M.; Tamura, K.; Ma, L. Short-Term Effects of Fine Particulate Matter and Temperature on Lung Function among Healthy College Students in Wuhan, China. Int. J. Environ. Res. Public Health 2015, 12, 7777-7793. https://doi.org/10.3390/ijerph120707777
Zhang Y, He M, Wu S, Zhu Y, Wang S, Shima M, Tamura K, Ma L. Short-Term Effects of Fine Particulate Matter and Temperature on Lung Function among Healthy College Students in Wuhan, China. International Journal of Environmental Research and Public Health. 2015; 12(7):7777-7793. https://doi.org/10.3390/ijerph120707777
Chicago/Turabian StyleZhang, Yunquan, Mingquan He, Simin Wu, Yaohui Zhu, Suqing Wang, Masayuki Shima, Kenji Tamura, and Lu Ma. 2015. "Short-Term Effects of Fine Particulate Matter and Temperature on Lung Function among Healthy College Students in Wuhan, China" International Journal of Environmental Research and Public Health 12, no. 7: 7777-7793. https://doi.org/10.3390/ijerph120707777
APA StyleZhang, Y., He, M., Wu, S., Zhu, Y., Wang, S., Shima, M., Tamura, K., & Ma, L. (2015). Short-Term Effects of Fine Particulate Matter and Temperature on Lung Function among Healthy College Students in Wuhan, China. International Journal of Environmental Research and Public Health, 12(7), 7777-7793. https://doi.org/10.3390/ijerph120707777