
Building-Related Symptoms among Office Employees Associated with Indoor Carbon Dioxide and Total Volatile Organic Compounds

Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire Survey
2.2. Environmental Measurement
2.3. Statistical Analysis

{kind=link}
| Variable | Description |
|---|---|
| Gender | 0: male; 1: female |
| Age | 0: age < 40 years; 1: age ≥ 40 years |
| Carpet | 0: no carpet on workstation; 1: carpet on most or all workspace |
| Smoker | 0: never or former smoker; 1: current smoker |
| Asthma | 0: previously never diagnosed; 1: previously ever diagnosed |
| Nasosinusitis | 0: previously never diagnosed; 1: previously ever diagnosed |
| Atopic rhinitis | 0: previously never diagnosed; 1: previously ever diagnosed |
| Migraine | 0: previously never diagnosed; 1: previously ever diagnosed |
| Dust allergies | 0: previously never diagnosed; 1: previously ever diagnosed |
| Animals allergies | 0: previously never diagnosed; 1: previously ever diagnosed |
| Chemical sensitivity | 0: previously never diagnosed; 1: previously ever diagnosed |
| ETS sensitivity | 0: self-reported “No”; 1: self-reported “Yes” |
| Exposure to ETS | 0: self-reported “No”; 1: self-reported “Yes” |
| Using Sanitizing chemical | 0: self-reported “No”; 1: self-reported “Yes” |
| New furniture | 0: self-reported “No”; 1: self-reported “Yes” |
| New decoration | 0: self-reported “No”; 1: self-reported “Yes” |
| Painting recently | 0: self-reported “No”; 1: self-reported “Yes” |
| Working stress | 0: self-reported “No”; 1: self-reported “Yes” |
| No social support | 0: self-reported “No”; 1: self-reported “Yes” |
| Working time>9 h/day | 0: self-reported “No”; 1: self-reported “Yes” |
| Speck of molds | 0: “No” recorded by sampler; 1: “Yes” recorded by sampler |
| Leaking | 0: “No” recorded by sampler; 1: “Yes” recorded by sampler |
| Season | 0: spring; 1: winter |
| dCO2 | Hourly mean degree per 100 (ppm/100) |
| TVOCsindoor | Hourly mean degree per 100 (ppb/100) |
| RH | Hourly mean degree (%) |
| Temperature | Hourly mean degree (°C) |
3. Results and Discussion
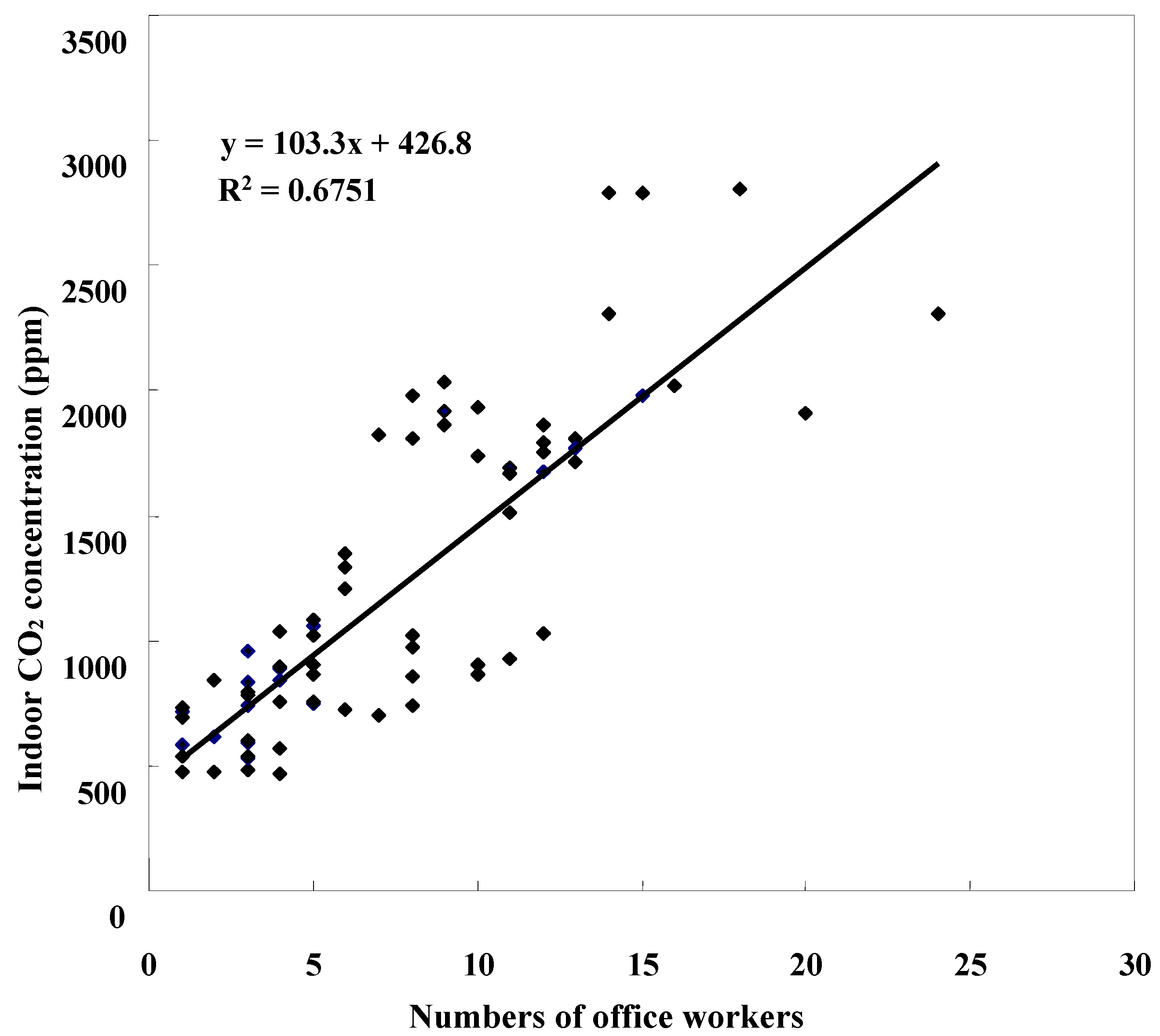
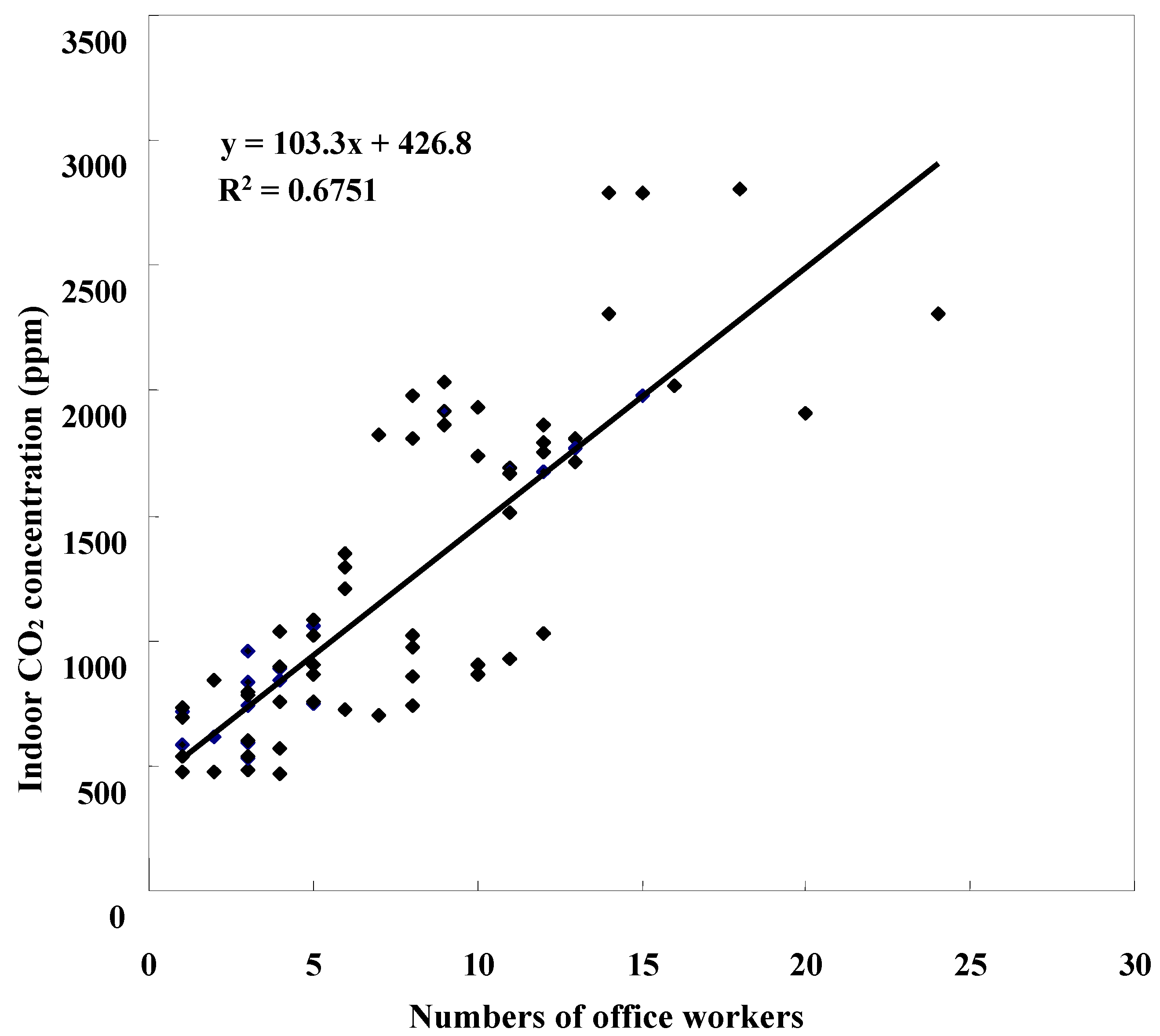
3.1. Indoor CO2 and TVOCs Measurement
3.2. Self-Reported Sick Building Syndrome Risk
| Environmental Variables | Mean | SD | Range |
|---|---|---|---|
| Temperature indoor (°C) | 23.6 | 1.71 | 18.6–28.4 |
| Temperature outdoor (°C) | 25.7 | 4.96 | 16.3–37.8 |
| Difference a | −2.13 | 4.48 | −14.2–5.00 |
| Relative humidityindoor (%) | 57.3 | 6.92 | 45.5–79.7 |
| Relative humidityoutdoor (%) | 60.5 | 13.6 | 34.0–81.3 |
| Difference a | −3.18 | 11.6 | −21.1–24.2 |
| CO2 indoor (100 ppm) | 11.6 | 6.04 | 4.67–28.0 |
| CO2 outdoor (100 ppm) | 4.34 | 0.60 | 3.37–5.63 |
| Difference a | 7.29 | 6.25 | −1.03–23.9 |
| TVOCs indoor (100 ppb) | 11.9 | 60.6 | 0.06–557 |
| TVOCs outdoor (100 ppb) | 1.80 | 1.60 | 0.05–4.25 |
| Difference a | 10.1 | 60.2 | −1.46–553 |
| Individual Characteristics | % | Symptoms | % |
|---|---|---|---|
| Female | 77.9 | Eye, any | 22.5 |
| Age (≥40 years) | 30.0 | Eye dryness | 18.7 |
| Current smoker | 11.3 | Eye irritation | 5.5 |
| Working time >5 days/week | 11.8 | ||
| Working time >9 h/day | 20.9 | Upper respiratory, any | 15.3 |
| Working stress | 14.6 | Nose itching | 2.4 |
| Lacking of family support | 40.3 | Runny nose | 2.4 |
| Asthma | 3.4 | Stuffy nose | 6.2 |
| Nasosinusitis | 7.0 | Sneezing | 2.4 |
| Atopic rhinitis | 29.0 | Dry throat | 6.7 |
| Migraine | 17.0 | ||
| Dust allergy | 24.5 | Lower respiratory, any | 6.5 |
| Animal allergy | 8.6 | Difficulties in breathing | 6.5 |
| Sensitivity to tobacco smoke | 68.3 | ||
| Sensitivity to chemicals in air | 64.5 | Skin, any | 1.9 |
| Exposure to ETS | 15.6 | Skin dryness | 1.9 |
| Using Sanitizing chemical | 29.7 | ||
| Carpet in workspace | 61.4 | Non-specific, any | 25.4 |
| New furniture | 4.6 | Tiredness | 20.9 |
| New decoration | 9.4 | Difficulties in concentrating | 14.6 |
| Painting recently | 5.5 | Irritability | 12.7 |
| Leaking | 10.1 | Dizziness | 7.2 |
| Speck of molds | 7.7 |
| Sick-Building Syndrome Symptom | dCO2 (per 100 ppm) | ||
|---|---|---|---|
| Crude | Adjusted a | Adjusted b | |
| Eye, any | 0.99 (0.97–1.01) | 1.00 (0.96–1.04) | 1.00 (0.96–1.04) |
| Eye dryness | 1.01 (0.99–1.04) | 1.02 (0.99–1.06) | 1.02 (0.98–1.06) |
| Eye irritation | 0.85 (0.73–0.99) | 0.81 (0.67–0.98) | 0.74 (0.59–0.93) |
| Upper respiratory, any | 1.02 (0.91–1.14) | 1.04 (0.93–1.17) | 0.97 (0.89–1.06) |
| Nose itching | 1.02 (0.86–1.21) | 1.03 (0.80–1.32) | 1.03 (0.80–1.32) |
| Runny nose | 0.97 (0.79–1.20) | 0.92 (0.71–1.18) | 0.92 (0.72–1.19) |
| Stuffy nose | 1.03 (0.94–1.13) | 1.11 (0.96–1.28) | 1.07 (0.92–1.25) |
| Sneezing | 1.04 (0.94–1.15) | 0.93 (0.69–1.25) | 0.52 (0.12–2.31) |
| Dry throat | 1.03 (0.89–1.18) | 1.10 (1.00–1.22) | 1.03 (0.91–1.15) |
| Lower respiratory, any | 0.99 (0.94–1.18) | 1.07 (0.96–1.20) | 1.05 (0.94–1.18) |
| Difficulties in breathing | 0.99 (0.94–1.18) | 1.07 (0.96–1.20) | 1.05 (0.94–1.18) |
| Skin, any | 1.03 (0.87–1.22) | 1.04 (0.85–1.28) | 1.05 (0.82–1.34) |
| Dryness | 1.03 (0.87–1.22) | 1.04 (0.85–1.28) | 1.05 (0.82–1.34) |
| Non-specific, any | 1.04 (0.97–1.11) | 1.16 (1.04–1.29) | 1.13 (1.02–1.26) |
| Tiredness | 1.03 (0.97–1.10) | 1.16 (1.07–1.26) | 1.14 (1.06–1.23) |
| Difficulties in concentrating | 1.01 (0.93–1.09) | 1.09 (0.99–1.20) | 1.08 (0.98–1.19) |
| Irritability | 0.97 (0.89–1.05) | 1.13 (0.95–1.35) | 1.09 (0.92–1.29) |
| Dizziness | 1.10 (0.97–1.26) | 1.22 (1.08–1.37) | 1.20 (1.07–1.34) |
| Sick-Building Syndrome Symptom | TVOCs (per 100 ppm) | ||
|---|---|---|---|
| Crude | Adjusted a | Adjusted b | |
| Eye, any | 1.00 (0.99–1.00) | 1.00 (1.00–1.00) | 1.00 (0.99–1.00) |
| Eye dryness | 1.00 (1.00–1.01) | 1.00 (1.00–1.01) | 1.00 (0.99–1.00) |
| Eye irritation | 1.00 (1.00–1.01) | 1.01 (1.00–1.01) | 1.01 (1.00–1.02) |
| Upper respiratory, any | 1.04 (1.02–1.06) | 1.06 (1.04–1.07) | 1.06 (1.05–1.07) |
| Nose itching | 0.98 (0.92–1.04) | 1.00 (0.97–1.03) | 1.00 (0.97–1.03) |
| Runny nose | 0.97 (0.90–1.06) | 1.00 (0.95–1.05) | 1.00 (0.96–1.04) |
| Stuffy nose | 1.01 (1.00–1.01) | 1.01 (1.01–1.02) | 1.01 (1.01–1.02) |
| Sneezing | 1.01 (1.00–1.01) | 1.07 (0.86–1.33) | 2.63 (0.18–38.7) |
| Dry throat | 1.02 (1.00–1.05) | 1.06 (1.03–1.09) | 1.06 (1.02–1.09) |
| Lower respiratory, any | 1.00 (1.00–1.01) | 1.01 (1.00–1.01) | 1.01 (1.00–1.01) |
| Difficulties in breathing | 1.00 (1.00–1.01) | 1.01 (1.00–1.01) | 1.01 (1.00–1.01) |
| Skin, any | 1.01 (1.01–1.01) | 1.01 (1.00–1.02) | 1.01 (1.00–1.02) |
| Dryness | 1.01 (1.01–1.01) | 1.01 (1.00–1.02) | 1.01 (1.00–1.02) |
| Non-specific, any | 1.03 (1.02–1.04) | 1.03 (1.02–1.05) | 1.02 (1.01–1.03) |
| Tiredness | 1.03 (1.02–1.04) | 1.02 (1.01–1.04) | 1.01 (1.01–1.02) |
| Difficulties in concentrating | 1.00 (1.00–1.01) | 1.00 (1.00–1.01) | 1.00 (1.00–1.01) |
| Irritability | 1.03 (1.02–1.03) | 1.02 (1.01–1.04) | 1.02 (1.00–1.03) |
| Dizziness | 1.01 (1.01–1.01) | 1.01 (1.00–1.02) | 1.01 (1.00–1.01) |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Freijer, J.I.; Bloemen, H.J.T. Modeling relationships between indoor and outdoor air quality. J. Air Waste Manage. Assoc. 2000, 50, 292–300. [Google Scholar] [CrossRef]
- Yassi, A.; Kjellström, T.; de Kok, T.; Guidotti, T.L. Basic Environmental Health, 1st ed.; University Press: Oxford, UK, 2001; pp. 291–292. [Google Scholar]
- Azuma, K.; Ikeda, K.; Kagi, N.; Yanagi, U.; Osawa, H. Prevalence and risk factors associated with nonspecific building-related symptoms in office employees in Japan: Relationships between work environment, Indoor Air Quality, and occupational stress. Indoor Air 2014. [Google Scholar] [CrossRef]
- Redlich, C.A.; Sparer, J.; Cellen, M.R. Sick-building syndrome. Occup. Med. 1997, 349, 1013–1016. [Google Scholar]
- Teculescu, D.B.; Sauleau, E.A.; Massin, N.; Bohadana, A.B.; Buhler, O.; Benamghar, L.; Mur, J.M. Sick-building symptoms in office workers in northeastern France: A pilot study. Int. Arch. Occup. Environ. Health 1998, 71, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Mahnoudi, M.; Gershwin, M.E. Sick building syndrome. Ⅲ. Stachybotrys chartarum. J. Asthma 2000, 37, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Niven, R.M.; Fletcher, A.M.; Pickering, C.A.C.; Faragher, E.B.; Potter, I.N.; Booth, W.B.; Jones, T.J.; Potter, P.D.R. Building sickness syndrome in healthy and unhealthy buildings: An epidemiological and environmental assessment with cluster analysis. Occup. Environ. Med. 2000, 57, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Mendell, M.J. Non-specific symptoms in office workers: A review and summary of the epidemiologic literature. Indoor Air 1993, 3, 227–236. [Google Scholar] [CrossRef]
- Skyberg, K.; Skulberg, K.R.; Eduard, W.; Skåret, E.; Levy, F.; Kjuus, H. Symptoms prevalence among office employees and associations to building characteristics. Indoor Air 2003, 13, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Bourbeau, J.; Brisson, C.; Allaire, S. Prevalence of the sick building syndrome symptoms in office workers before and six months and three years after being exposed to a building with an improved ventilation system. Occup. Environ. Med. 1997, 54, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Backman, H.; Haghighat, F. Indoor-air quality and ocular discomfort. Amer. Optom. Assoc. 1999, 70, 309–316. [Google Scholar]
- Seppänen, O.A.; Fisk, W.J.; Merdell, M.J. Association of ventilation rates and CO2 concentrations with health and other responses in commercial and institutional buildings. Indoor Air 1999, 9, 226–252. [Google Scholar] [CrossRef] [PubMed]
- Apte, M.G.; Fisk, W.J.; Daisey, J.M. Associations between indoor CO2 concentrations and sick building syndromes in U.S. office buildings: An analysis of the 1994–1996 BASE study data. Indoor Air 2000, 10, 246–257. [Google Scholar] [CrossRef] [PubMed]
- Engvall, K.; Norrby, C.; Norbäck, D. Sick building syndrome in relation to building dampness in multi-family residential buildings in Stockholm. Int. Arch. Occup. Environ. Health 2001, 74, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Tsai, D.H.; Lin, J.S.; Chan, C.C. Office workers’ sick building syndrome and indoor carbon dioxide concentrations. J. Occup. Environ. Hyg. 2012, 9, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Norback, D.; Torgen, M.; Edling, C. Volatile organic compounds, respirable dust, and personal factors related to prevalence and incidence of sick building syndrome in primary schools. Brit. J. Ind. Med. 1990, 47, 733–741. [Google Scholar]
- Pommer, L.; Fick, J.; Sundell, J.; Nilsson, C.; Sjöström, M.; Stenberg, B.; Andersson, B. Class separation of buildings with high and low prevalence of SBS by principal component analysis. Indoor Air 2004, 14, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Bako-Biro, Z.; Wargocki, P.; Weschler, C.J.; Fanger, P.O. Effects of pollution from personal computers on perceived air quality, SBS symptoms and productivity in offices. Indoor Air 2004, 14, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.L.; Elfman, L.; Mi, Y.; Wieslander, G.; Smedje, G.; Norbäck, D. Indoor molds, bacteria, microbial volatile organic compounds and plasticizers in schools—Associations with asthma and respiratory symptoms in pupils. Indoor Air 2007, 17, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Takigawa, T.; Saijo, Y.; Morimoto, K.; Nakayama, K.; Shibata, E.; Tanaka, M.; Yoshimura, T.; Chikara, H.; Kishi, R. A longitudinal study of aldehydes and volatile organic compounds associated with subjective symptoms related to sick building syndrome in new dwellings in Japan. Sci. Total Environ. 2012, 417–418, 61–67. [Google Scholar]
- Mølhave, L. Volatile organic compounds, indoor air quality and health. Indoor Air 1991, 1, 357–376. [Google Scholar] [CrossRef]
- Barrefors, G.; Petersson, G. Assessment of ambient volatile hydrocarbons from tobacco smoke and from vehicle emissions. J. Chromatogr. 1993, 643, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.Y.; Ma, Y.C.; Lin, J.M.; Li, C.Y.; Lin, R.S.; Sung, F.C. Oxidative stress associated with indoor air pollution and sick building syndrome-related symptoms among office workers in Taiwan. Inhal. Toxicol. 2007, 19, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.Y.; Ma, Y.C.; Lin, J.M.; Chuang, C.Y.; Sung, F.C. Oxidative DNA damage estimated by urinary 8-hydroxydeoxyguanosine and indoor air pollution among non-smoking office employees. Environ. Res. 2007, 103, 331–337. [Google Scholar] [CrossRef] [PubMed]
- ASHRAE, ASHRAE Standard 62–2001. Ventilation for Acceptable Indoor Air Quality; American Society of Heating, Refrigerating, and Air-conditioning Engineers: Atlanta, GA, USA, 2001.
- Erdmann, C.A.; Apte, M.G. Mucous membrane and lower respiratory building related symptoms in relation to indoor carbon dioxide concentrations in the 100-building BASE dataset. Indoor Air 2004, 14, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.C.; Liang, H.H.; Lee, H.L.; Hsu, N.Y.; Su, H.J. Allostatic load model associated with indoor environmental quality and sick building syndrome among office workers. PLoS One 2014. [Google Scholar] [CrossRef]
- Takigawa, T.; Horike, T.; Ohashi, Y.; Kataoka, H.; Wang, D.H.; Kira, S. Were volatile organic compounds the inducing factors for subjective symptoms of employees working in newly constructed hospital. Environ. Toxic 2004, 19, 280–290. [Google Scholar] [CrossRef]
- Saijo, Y.; Kishi, R.; Sata, F.; Katakura, Y.; Urashima, Y.; Hatakeyama, A.; Kobayashi, S.; Jin, K.; Kurahashi, N.; Kondo, T.; Gong, Y.Y.; Umemura, T. Symptoms in relation to chemicals and dampness in newly built dwellings. Int. Arch. Occup. Environ. Health 2004, 77, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Sahlberg, B.; Gunnbjörnsdottir, M.; Soon, A.; Jogi, R.; Gislason, T.; Wieslander, G.; Janson, C.; Norback, D. Airborne molds and bacteria, microbial volatile organic compounds (MVOC), plasticizers and formaldehyde in dwellings in three North European cities in relation to sick building syndrome (SBS). Sci. Total Environ. 2013, 444, 433–440. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, C.-Y.; Lin, J.-M.; Chen, Y.-Y.; Chen, Y.-C. Building-Related Symptoms among Office Employees Associated with Indoor Carbon Dioxide and Total Volatile Organic Compounds. Int. J. Environ. Res. Public Health 2015, 12, 5833-5845. https://doi.org/10.3390/ijerph120605833
Lu C-Y, Lin J-M, Chen Y-Y, Chen Y-C. Building-Related Symptoms among Office Employees Associated with Indoor Carbon Dioxide and Total Volatile Organic Compounds. International Journal of Environmental Research and Public Health. 2015; 12(6):5833-5845. https://doi.org/10.3390/ijerph120605833
Chicago/Turabian StyleLu, Chung-Yen, Jia-Min Lin, Ying-Yi Chen, and Yi-Chun Chen. 2015. "Building-Related Symptoms among Office Employees Associated with Indoor Carbon Dioxide and Total Volatile Organic Compounds" International Journal of Environmental Research and Public Health 12, no. 6: 5833-5845. https://doi.org/10.3390/ijerph120605833