
Patterns in PARTNERing across Public Health Collaboratives

Abstract
:1. Introduction
2. Experimental Section
2.1. Data Sets and Sources
2.2. Analysis
3. Results and Discussion
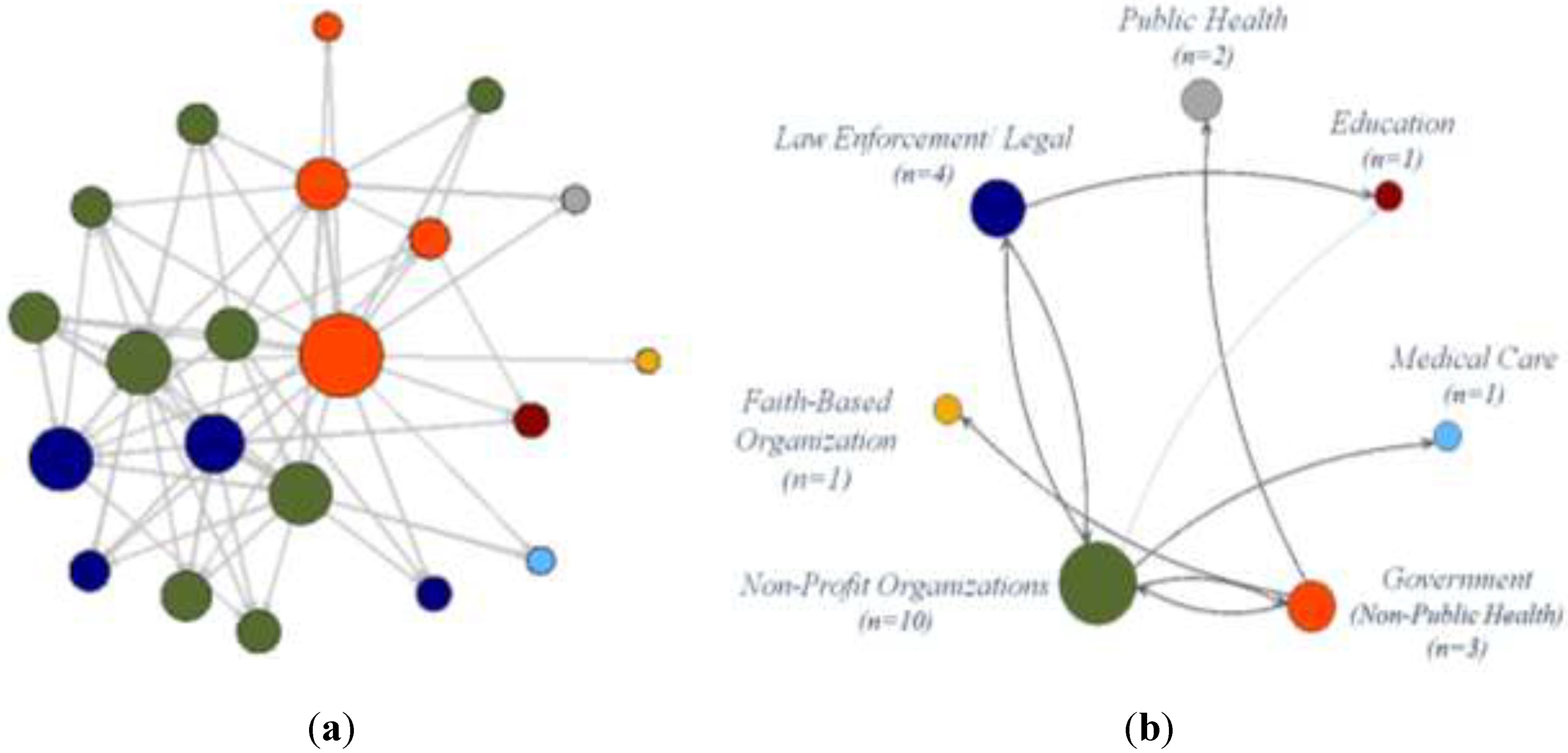
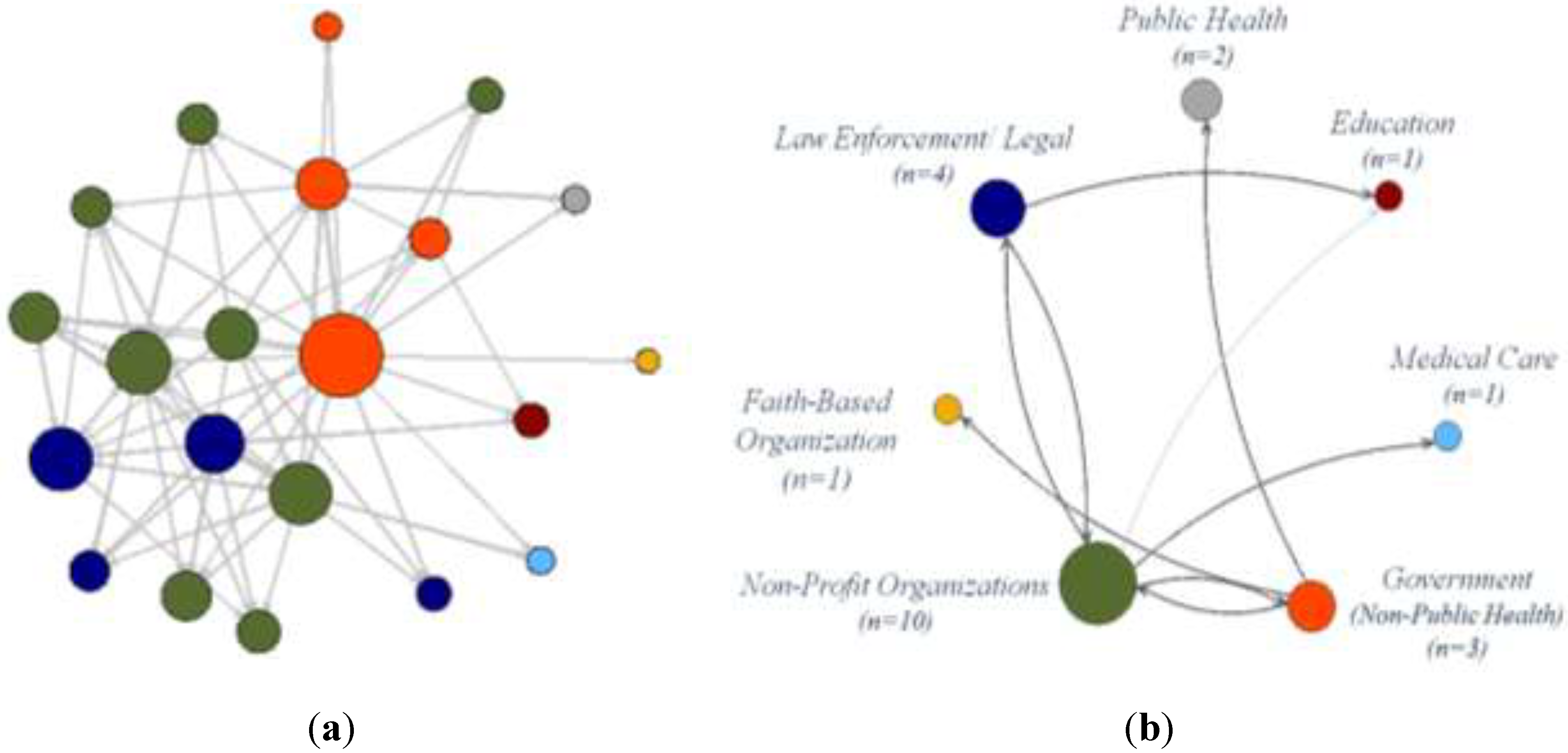
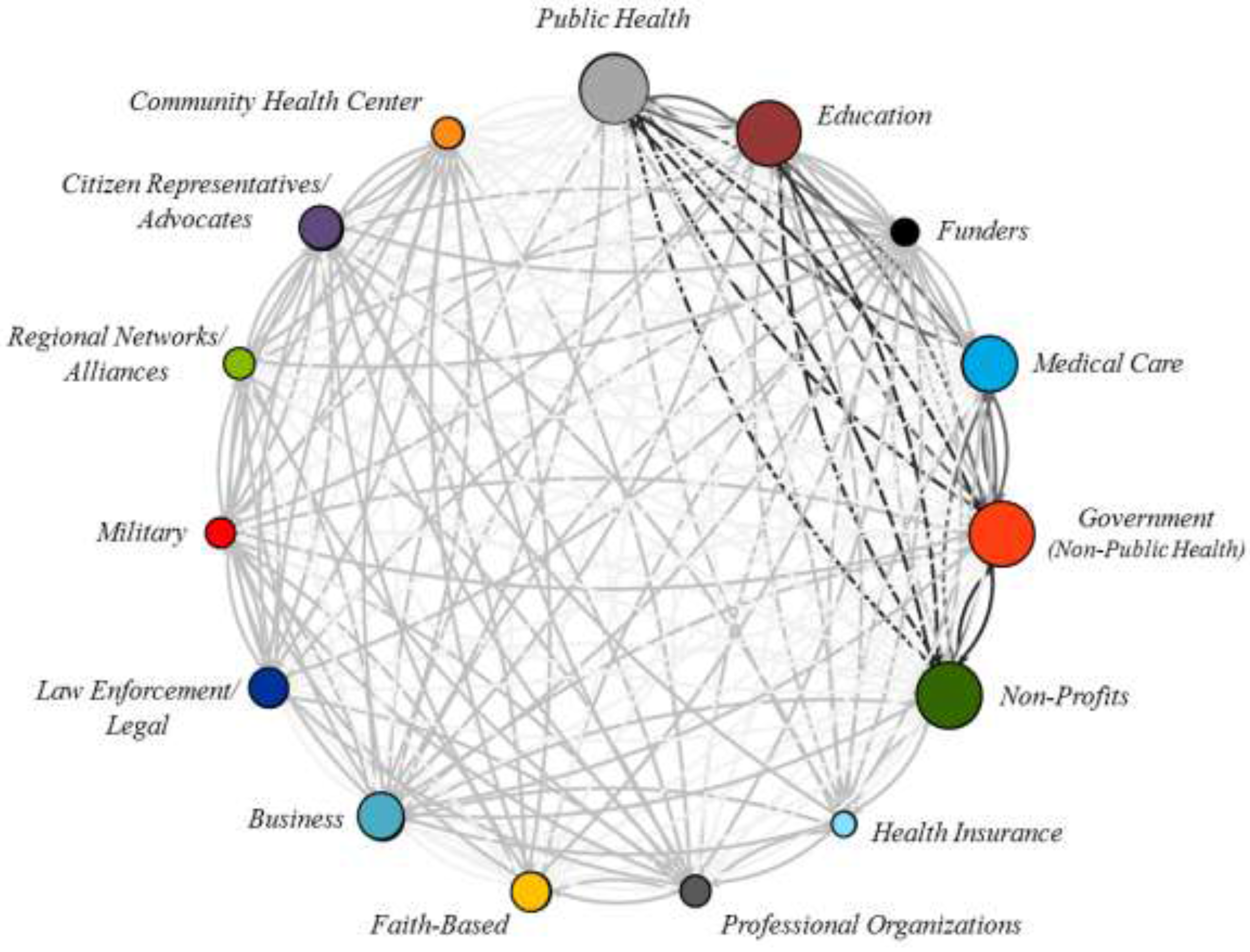
3.1. Frequency of Partnerships

{kind=link}
{kind=link}
| Organization Type | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | (13) | (14) | (15) | Total Organizations | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) | Public Health | 123 | 162 | ||||||||||||||
| (2) | Education | 84 | 102 | 113 | |||||||||||||
| (3) | Funders | 4 | 2 | 7 | 11 | ||||||||||||
| (4) | Medical Care | 67 | 57 | 4 | 82 | 87 | |||||||||||
| (5) | Government (Non-Public Health) | 92 | 85 | 4 | 65 | 115 | 121 | ||||||||||
| (6) | Non-Profits | 101 | 87 | 5 | 65 | 105 | 127 | 130 | |||||||||
| (7) | Health Insurance | 6 | 5 | 2 | 5 | 7 | 6 | 8 | 9 | ||||||||
| (8) | Professional Organizations | 13 | 9 | 1 | 8 | 12 | 14 | 1 | 14 | 19 | |||||||
| (9) | Faith-Based Organizations | 31 | 27 | 2 | 26 | 32 | 33 | 0 | 4 | 34 | 37 | ||||||
| (10) | Business | 37 | 41 | 2 | 30 | 45 | 43 | 5 | 7 | 15 | 47 | 49 | |||||
| (11) | Law Enforcement/Legal | 25 | 26 | 1 | 22 | 27 | 29 | 0 | 5 | 17 | 16 | 32 | 34 | ||||
| (12) | Military | 7 | 6 | 0 | 7 | 6 | 8 | 0 | 1 | 4 | 4 | 4 | 8 | 8 | |||
| (13) | Regional Networks/Alliances | 10 | 9 | 1 | 7 | 10 | 10 | 0 | 1 | 7 | 6 | 5 | 1 | 10 | 12 | ||
| (14) | Citizen Representatives/Advocates | 33 | 22 | 2 | 22 | 24 | 25 | 1 | 1 | 6 | 10 | 4 | 1 | 3 | 39 | 49 | |
| (15) | Community Health Center | 12 | 12 | 0 | 12 | 13 | 14 | 0 | 4 | 6 | 6 | 4 | 4 | 3 | 4 | 14 | 19 |

3.2. ERGM Results
3.3. Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bang, H.; Esmark, A. Good governance in network society: Reconfiguring the political from politics to policy. Adm. Theory Prax. 2009, 31, 7–37. [Google Scholar] [CrossRef]
- Hirst, P. Democracy and Governance. Available online: https://www.giz.de/en/ourservices/governance_and_democracy.html (accessed on 30 June 2015).
- Marshall, G.S. Commanded to enjoy: The waning of traditional authority and its implications for public administration. Adm. Theory Prax. 2007, 29, 102–114. [Google Scholar]
- Pierre, J. Debating Governance: Authority, Steering, and Democracy. Available online: http://econpapers.repec.org/bookchap/oxpobooks/9780198297727.htm (accessed on 30 June 2015).
- Eikenberry, A.M. The present and (normative) future of public administration and implications for ASPA. Public Adm. Rev. 2009, 69, 1060–1067. [Google Scholar] [CrossRef]
- Sørensen, E. Democratic theory and network governance. Adm. Theory Prax. 2002, 24, 693–720. [Google Scholar]
- Sørensen, E.; Torfing, J. Network governance and post-liberal democracy. Adm. Theory Prax. 2005, 27, 197–237. [Google Scholar]
- Powell, W.W.; Koput, K.W.; Smith-Doerr, L. Interorganizational collaboration and the locus of innovation: Networks of learning in biotechnology. Adm. Sci. Q. 1996, 41, 116–145. [Google Scholar] [CrossRef]
- Varda, D.M.; Chandra, A.; Stern, S.; Luri, N. Core dimensions of connectivity in public health collaboratives. J. Public Health Manag. Pract. 2008, 14, E1–E7. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, A.-M.; Jansen, M.W.; Gubbels, J.S.; De Vries, N.K.; Molleman, G.; Kremers, S.P. Local government officials’ views on intersectoral collaboration within their organization—A qualitative exploration. Health Policy Technol. 2015, 4, 47–57. [Google Scholar] [CrossRef]
- Schoen, M.W.; Moreland-Russell, S.; Prewitt, K.; Carothers, B.J. Social network analysis of public health programs to measure partnership. Soc. Sci. Med. 2014, 123, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.M.; Shortell, S.M. The governance and management of effective community health partnerships: A typology for research, policy, and practice. Milbank Q. 2000, 78, 241–289. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N. Positive and negative welfare and Australia’s indigenous communities. Fam. Matters 1999, 54, 30–35. [Google Scholar]
- Rhodes, R.A. Different roads to unfamiliar places: UK experience in comparative perspective. Aust. J. Public Adm. 1998, 57, 19–31. [Google Scholar] [CrossRef]
- Waddock, S.A. A typology of social partnership organizations. Adm. Soc. 1991, 22, 480–515. [Google Scholar] [CrossRef]
- McPherson, M.; Smith-Lovin, L.; Brashears, M.E. Birds of a feather: Homophily in social networks. Annu. Rev. Sociol. 2001, 2, 415–444. [Google Scholar] [CrossRef]
- Bevc, C.A.; Retrum, J.H.; Varda, D.M. New perspectives on the “silo effect”: Initial comparisons of network structures across public health collaboratives. Am. J. Public Health 2015, 105, S230–S235. [Google Scholar] [CrossRef] [PubMed]
- Newman, M.E.; Park, J. Why social networks are different from other types of networks. Phys. Rev. E 2003, 68. [Google Scholar] [CrossRef]
- Varda, D.; Shoup, J.A.; Miller, S. A systematic review of collaboration and network research in the public affairs literature: Implications for public health practice and research. Am. J. Public Health 2011, 102, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Varda, D.M. Data-driven management strategies in public health collaboratives. J. Public Health Manag. Pract. 2011, 17, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Varda, D.M.; Retrum, J.H. An exploratory analysis of network characteristics and quality of interactions among public health collaboratives. J. Public Health Res. 2012, 1, 170–176. [Google Scholar] [CrossRef]
- Wasserman, S.; Faust, K. Social Network Analysis: Methods and Applications; Cambridge University Press: New York, NY, USA, 1994. [Google Scholar]
- Snijders, T.A.; Baerveldt, C. A multilevel network study of the effects of delinquent behavior on friendship evolution. J. Math. Sociol. 2003, 27, 123–151. [Google Scholar] [CrossRef]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Hedges, L.V.; Pigott, T.D. The power of statistical tests in meta-analysis. Psychol. Methods 2001, 6, 203–217. [Google Scholar] [CrossRef] [PubMed]
- Snijders, T.; Spreen, M.; Zwaagstra, R. The use of multilevel modeling for analysing personal networks: Networks of cocaine users in an urban area. J. Quant. Anthropol. 1995, 5, 85–105. [Google Scholar]
- Raudenbush, S.W.; Brennan, R.T.; Barnett, R.C. A multivariate hierarchical model for studying psychological change within married couples. J. Fam. Psychol. 1995, 9, 161–174. [Google Scholar] [CrossRef]
- Snijders, T.A.; Kenny, D.A. The social relations model for family data: A multilevel approach. Pers. Relationsh. 1999, 6, 471–486. [Google Scholar] [CrossRef]
- Morris, M.; Handcock, M.S.; Hunter, D.R. Specification of exponential-family random graph models: Terms and computational aspects. J. Stat. Softw. 2008, 24, 1548–7660. [Google Scholar] [CrossRef] [PubMed]
- Handcock, M.S.; Hunter, D.R.; Butts, C.T.; Goodreau, S.M.; Morris, M. Statnet: Software tools for the representation, visualization, analysis and simulation of network data. J. Stat. Softw. 2008, 24, 1548–7660. [Google Scholar] [CrossRef] [PubMed]
- Bavelas, A. A mathematical model for small group structures. Hum. Organ. 1948, 7, 16–30. [Google Scholar] [CrossRef]
- Shaw, M.E. M communication networks. In Advance Experimental Social Psychology; Academic Press: New York, NY, USA, 1964; p. 111. [Google Scholar]
- Jennings, E.T., Jr.; Ewalt, J.A.G. Interorganizational coordination, administrative consolidation, and policy performance. Public Adm. Rev. 1998, 58, 417–428. [Google Scholar] [CrossRef]
- Milward, H.B.; Provan, K.G. Measuring network structure. Public Adm. 1998, 76, 387–407. [Google Scholar] [CrossRef]
- Provan, K.G.; Milward, H.B. A preliminary theory of interorganizational effectiveness: A comparative study of four community mental health systems. Adm. Sci. Q. 1995, 40, 1–33. [Google Scholar] [CrossRef]
- Bardach, E. Getting Agencies to Work Together: The Practice and Theory of Managerial Craftsmanship; Brookings Institution Press: Washingdon, DC, USA, 1998. [Google Scholar]
- Klijn, E.-H.; Koppenjan, J.F. Public management and policy networks: Foundations of a network approach to governance. Public Manag. Int. J. Res. Theory 2000, 2, 135–158. [Google Scholar] [CrossRef]
- Meier, K.J.; O’Toole, L.J. Public management and educational performance: The impact of managerial networking. Public Adm. Rev. 2003, 63, 689–699. [Google Scholar] [CrossRef]
- Roberts, N. Wicked problems and network approaches to resolution. Int. Public Manag. Rev. 2000, 1, 1–19. [Google Scholar]
- Roberts, N.C. The Transformative Power of Dialogue. Available online: http://philpapers.org/rec/ROBTTP-4 (accessed on 30 June 2015).
- Weber, E.P.; Khademian, A.M. Wicked problems, knowledge challenges, and collaborative capacity builders in network settings. Public Adm. Rev. 2008, 68, 334–349. [Google Scholar] [CrossRef]
- Beatty, K.B.; Harris, J.K.; Barnes, P. The role of inter-organizational partnerships in health services provision among rural, metropolitan, and urban local health departments. J. Rural Health 2010, 26, 248–258. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bevc, C.A.; Retrum, J.H.; Varda, D.M. Patterns in PARTNERing across Public Health Collaboratives. Int. J. Environ. Res. Public Health 2015, 12, 12412-12425. https://doi.org/10.3390/ijerph121012412
Bevc CA, Retrum JH, Varda DM. Patterns in PARTNERing across Public Health Collaboratives. International Journal of Environmental Research and Public Health. 2015; 12(10):12412-12425. https://doi.org/10.3390/ijerph121012412
Chicago/Turabian StyleBevc, Christine A., Jessica H. Retrum, and Danielle M. Varda. 2015. "Patterns in PARTNERing across Public Health Collaboratives" International Journal of Environmental Research and Public Health 12, no. 10: 12412-12425. https://doi.org/10.3390/ijerph121012412