Pre-Hospital ECG E-Transmission for Patients with Suspected Myocardial Infarction in the Highlands of Scotland


Abstract
:1. Introduction
1.1. ECG E-transmission Service
1.2. Research Aims
2. Methods
2.1. ECG E-transmission Database
2.2. Qualitative Interview
2.3. Research Governance
3. Results
3.1. Quantitative Data Analysis
3.1.1. Summary of the Study Participants

{kind=link}
{kind=link}
{kind=link}
| Characteristic | % (n) | Population Data | p-value (χ2) | |
|---|---|---|---|---|
| Gender | Male | 61.4 (1,243) | 48.9 (113,471) | p < 0.00001 |
| Female | 36.9 (748) | 51.1 (118,661) | ||
| Missing | 1.7 (34) | |||
| Age (years) | <50 | 16.2 (328) | 62.2 (137,061) | |
| 50–70 | 37.4 (758) | 29.0 (63,963) | ||
| >70 | 43.5 (880) | 8.7 (19,177) | p < 0.00001 | |
| Missing | 2.9 (59) |
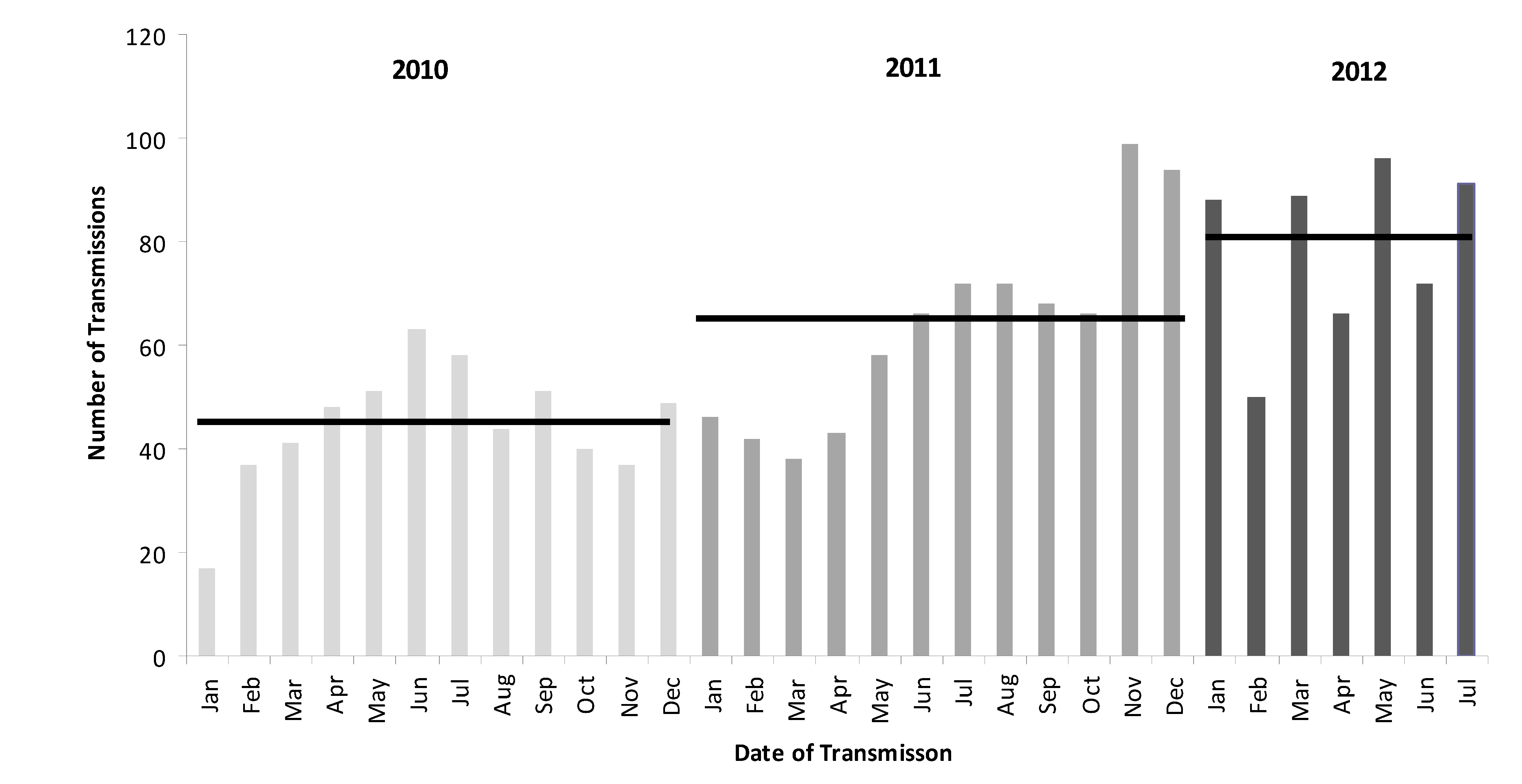
3.1.2. Variation in E-transmission Rates

3.1.3. Treatment Delivery Resulting from Transmission
| Parameter | Groups | % (n) |
|---|---|---|
| Travel time to hospital (n = 1,535) | <30 min | 62.1 (954) |
| 31–60 min | 18.1 (277) | |
| 61–90 min | 10.4 (160) | |
| >90 min | 9.4 (144) | |
| If STEMI/presumed new LBBB, was thrombolysis given? (n = 301) | Yes | 40.9 (123) |
| No | 59.1 (178) | |
| ST Elevation Detail (n = 147) | Inferior STEMI | 55.8 (82) |
| Anterior STEMI | 40.1 (59) | |
| Lateral STEMI | 4.1 (6) | |
| Location thrombolysis given (n = 123) | Pre-hospital | 74.8 (92) |
| CCU | 8.9 (11) | |
| A&E | 4.9 (6) | |
| Other | 1.6 (2) | |
| Missing | 9.8 (12) | |
| PHT given by (n = 92) | Paramedic | 78.3 (72) |
| GP | 15.2 (14) | |
| Missing | 6.5 (6) | |
| If given PHT admitted to (n = 92) | CCU | 80.4 (74) |
| A&E | 44 (8) | |
| Caithness General | 16.7 (3) | |
| Broadford Hospital | 11.1 (2) | |
| Stornoway Hospital | 11.1 (2) | |
| Medical Receiving | 5.6 (1) | |
| Aberdeen Royal CCU | 5.6 (1) | |
| Belford Hospital | 5.6 (1) |
| Travel Time to Hospital (mins) | Thrombolysis Administration % (n) * | Total % (n) | ||
|---|---|---|---|---|
| Pre-hospital Thrombolysis | Hospital Thrombolysis | |||
| Paramedic | GP | |||
| <30 | 76.5 (39) | 5.9 (3) | 17.6 (9) | 26.2 (51) |
| 31–60 | 88.2 (15) | 11.8 (2) | 0 (0) | 20.2 (17) |
| 61–90 | 100 (7) | 0 (0) | 0 (0) | 8.3 (7) |
| >90 | 11.1 (1) | 66.7 (6) | 22.2 (2) | 10.7 (9) |
| Sub-total | 73.8 (62) | 13.1 (11) | 13.1 (11) | 100 (84) |
3.2. Qualitative Data
3.2.1. Summary of the Study Participants
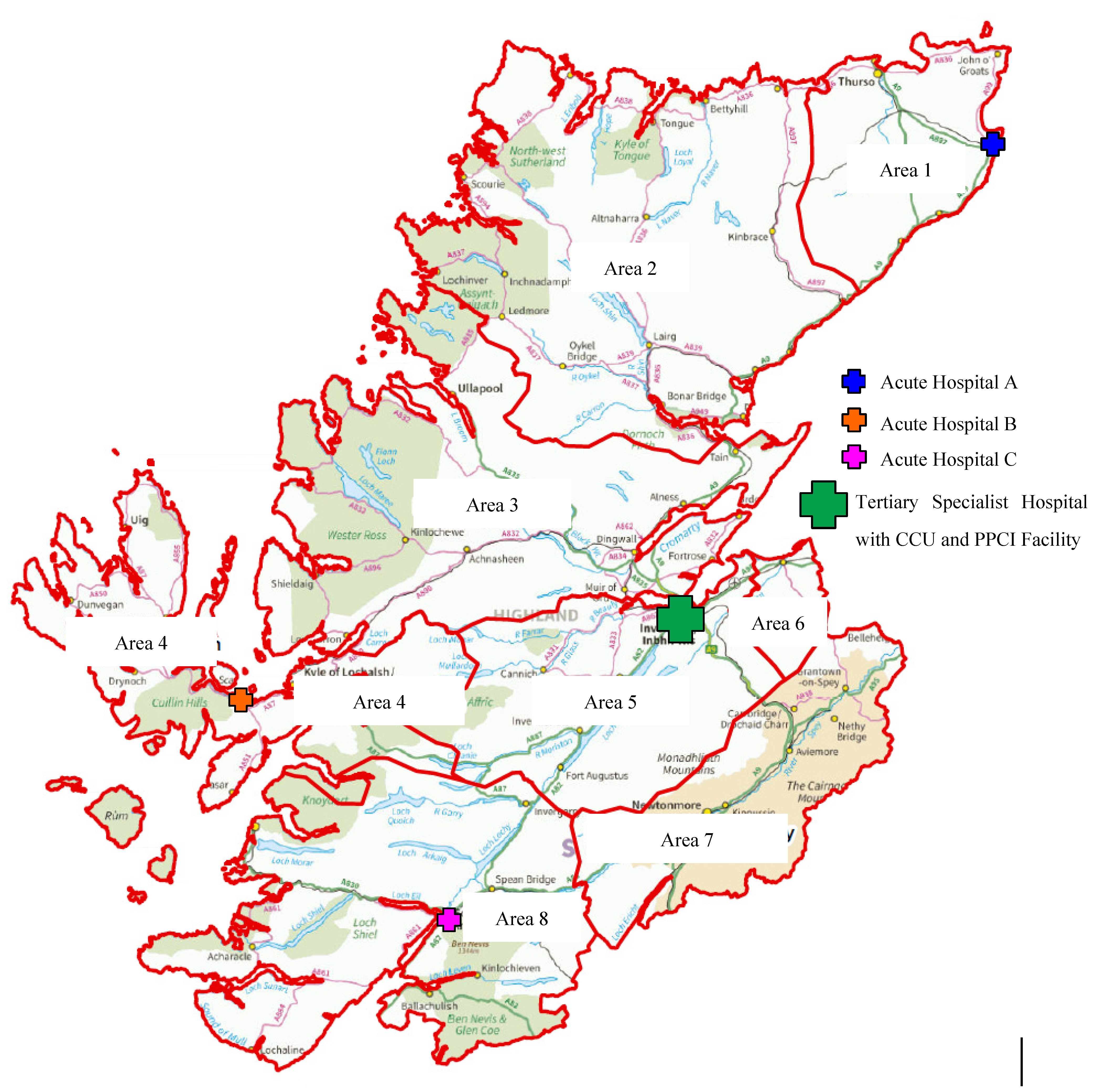
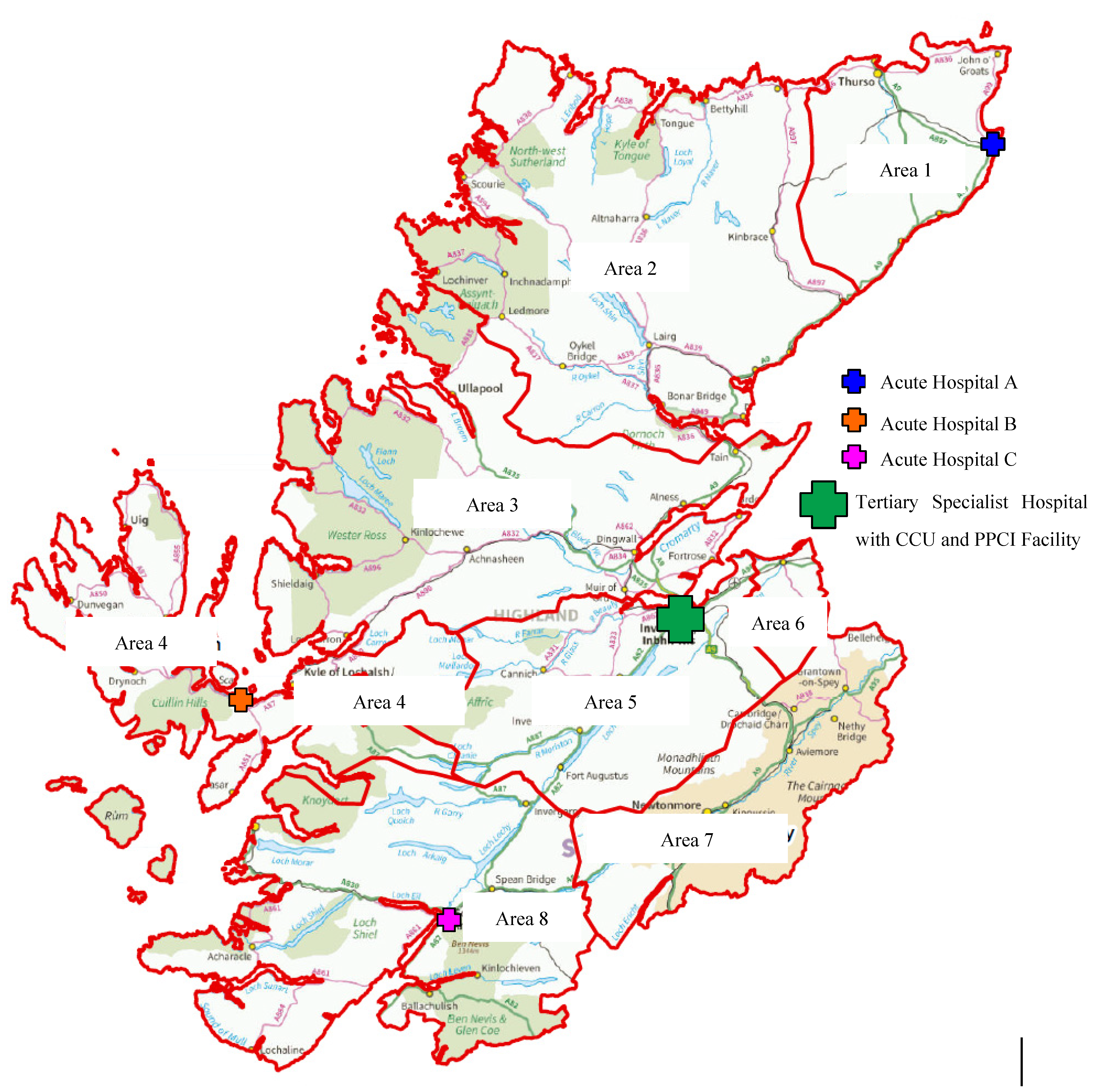
| Highland Area | Population of area (n = 222,370) | E-transmissions * | Supported PHT delivered | ||||
|---|---|---|---|---|---|---|---|
| N (n = 1,395) | Per 10,000 population | Range | N (n = 66) | Per 10,000 population | Range | ||
| 1 | 25,160 | 30 | 11.9 | 3 | 1.19 | ||
| 2 | 13,520 | 129 | 95.4 | 4 | 2.96 | ||
| 3 | 51,450 | 473 | 91.9 | 11.9–95.4 | 21 | 4.08 | 0.52–7.29 |
| 4 | 12,680 | 32 | 25.2 | 3 | 2.37 | ||
| 5 | 74,950 | 515 | 68.7 | 19 | 2.54 | ||
| 6 | 12,340 | 70 | 56.7 | 9 | 7.29 | ||
| 7 | 12,890 | 114 | 88.4 | 6 | 4.65 | ||
| 8 | 19,290 | 32 | 16.6 | 1 | 0.52 | ||
| Mean 62.7 | Mean 2.97 | ||||||
| Participant Code | Gender | Years of Experience | Frequency of Direct Involvement in Reception/ Transmission of an ECG to CCU via Telemetry Service | Frequency of Administration of PHT (SAS only) |
|---|---|---|---|---|
| CCU 1 | Male | 28 | Daily | |
| CCU 2 | Female | 23 | Daily | |
| CCU 3 | Female | 10 | Daily | |
| CCU 4 | Female | 5 | Daily | |
| CCU 5 | Female | 12 | Daily | |
| CCU 6 | Female | 14 | Daily | |
| SAS 1 | Male | 18 | On average six times per week | Three times in the last year |
| SAS 2 | Male | 9 | Varies-sent four last week | Once in two years |
| SAS 3 | Female | <1 | On average weekly | Assisted once |
| SAS 4 | Male | 20 | Monthly | Four in the last year |
| SAS 5 | Male | 9 | Once or twice a week | Once in the last year |
| SAS 6 | Male | 13 | Once a week | Three in the last year |
“…the benefit to the patient is a much earlier intervention with a consequence of less damage to the heart and therefore better outlook for them.”[CCU1]
“If someone is acutely unwell and they present as a STEMI then they can come directly to ourselves whereas before normally they might have just been transferred straight to A&E and it’s better if we see the ECG because we can tell if the person is having an acute MI they come directly here and it saves a lot of time as well.”[CCU3]
“…it’s great because they can give us more insight and they can look up patient records. What we’re seeing, we might see something, eh, not normal but it’s normal for that patient because they have already seen the previous ECGs.”[SAS2]
“…it’s good contact, a discussion with another professional so we can actually, you know, feed off each other as well during the process of passing over the information.”[SAS4]
“I think we all work together as a team. Paramedics value our support and we are very open to receiving the calls…”[CCU3]
“Since it was first introduced I think there is probably a better understanding between the two of us now…there is more of a connection now I think between the staff in the CCU and ourselves. Eh, I definitely think there is a better working ethic in there.”[SAS6]
“when you are doing telemetric advice, you’re using someone at the end of a phone as your eyes and ears and they’re looking at the patient trying to convey their clinical opinion to you and whereas all you’re seeing is the ECG.”[CCU1]
“I think one of the barriers is technical, we have a history of problems with just technical issues with the signals not coming through.”[CCU2]
“I suppose it takes up more nursing time and takes us away from our patients…”[CCU3]
“A national issue but the JR-CALC guidelines are always an issue because their thrombolysis guidelines differ from us.”[CCU5]
4. Discussion
4.1. Summary of Main Findings
4.2. Strengths and Limitations
4.2.1. Quantitative Data
4.2.2. Qualitative Data
4.3. Interpretation of Findings
4.3.1. Remote Area Service Variation
4.3.2. Seasonal Variation
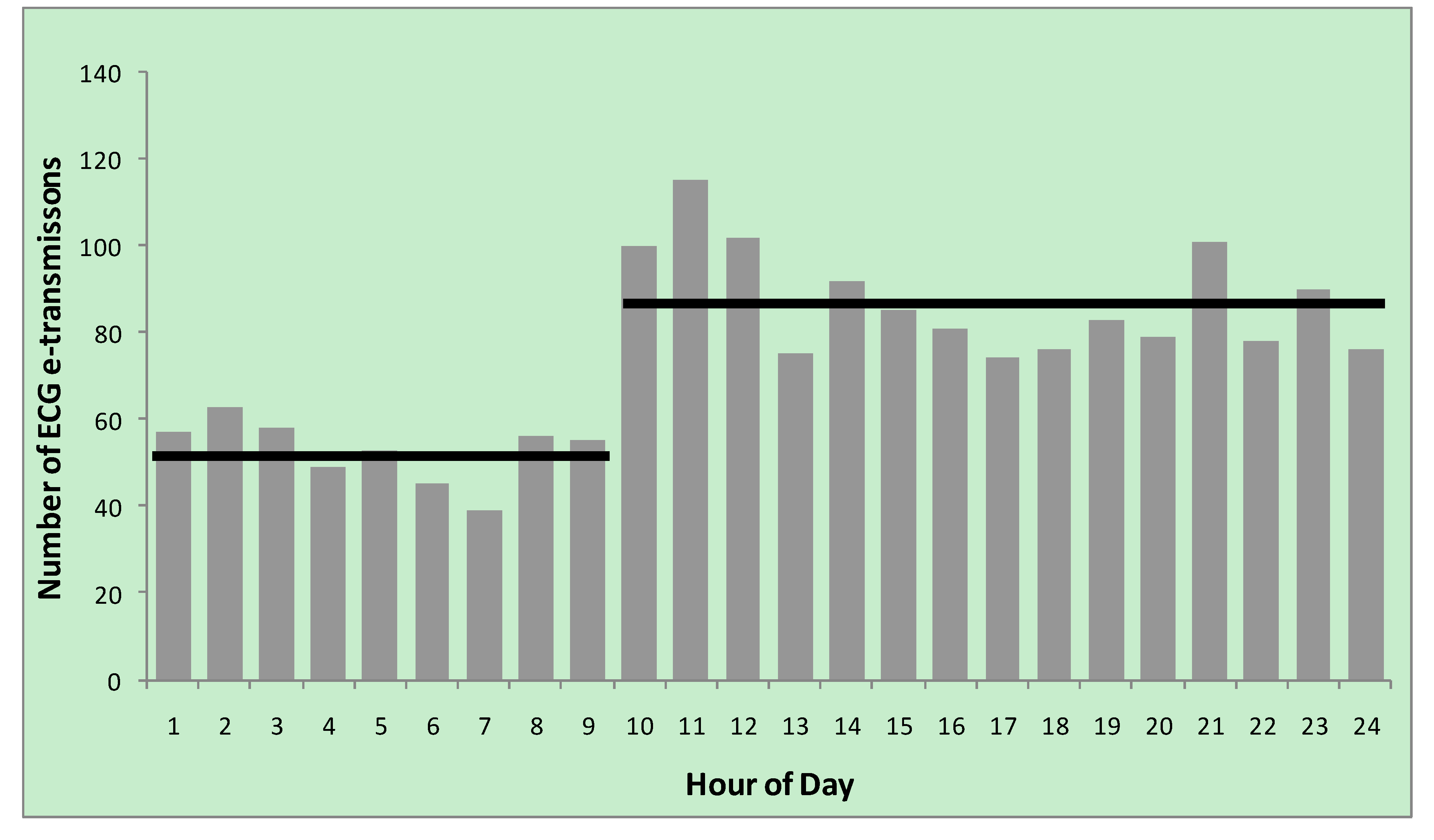
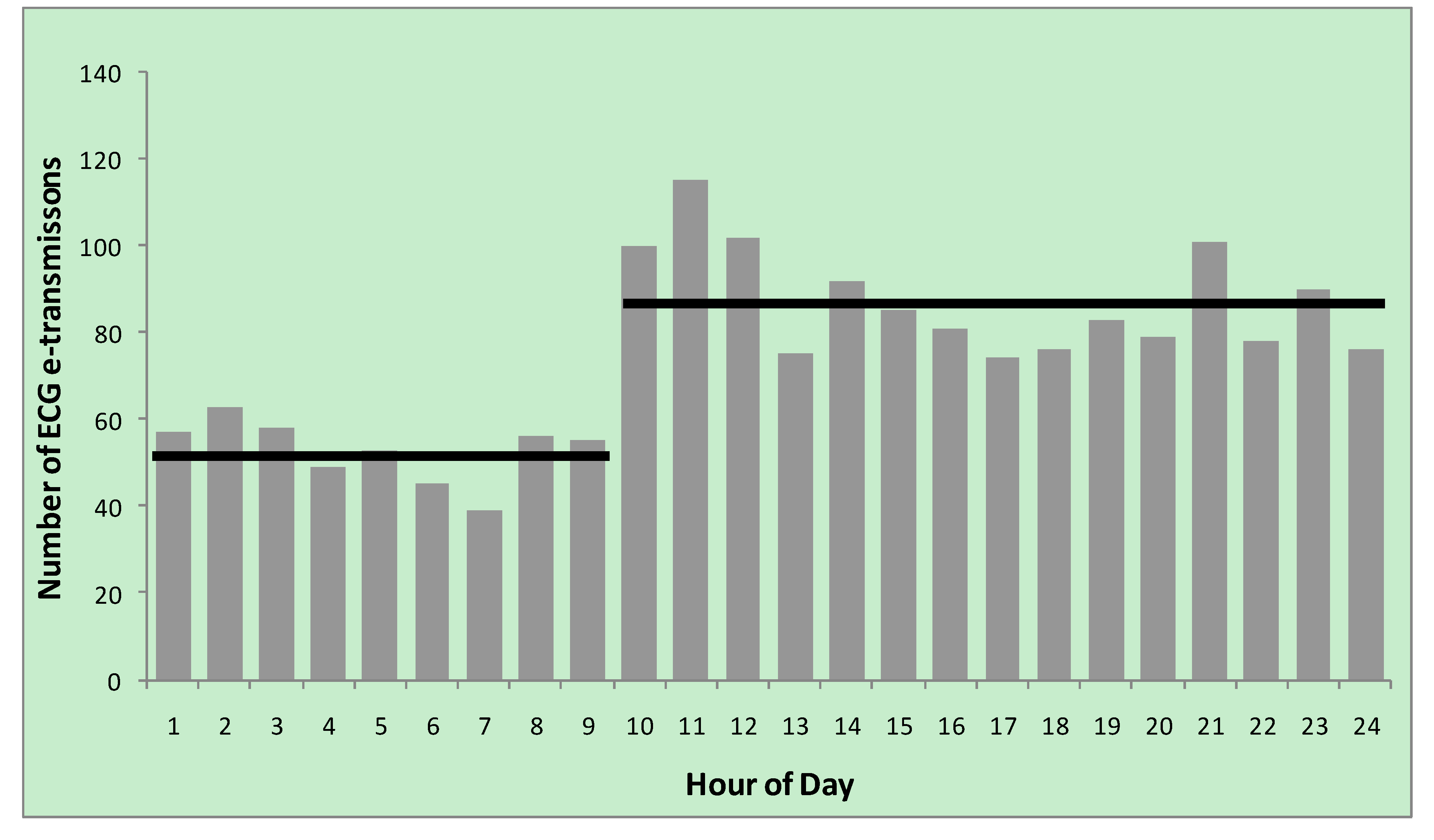
4.3.3. Diurnal Variation
4.3.4. Facilitators and Barriers to Uptake
4.4. Future Directions and Studies
5. Conclusion
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Scarborough, P.; Wickramasinghe, K.; Bhatnagar, P.; Rayner, M. Trends in Coronary Heart Disease 1961–2009, 2011. Available online: http://www.bhf.org.uk/publications/view-publication.aspx? ps=1001933 (accessed 4 November 2013).
- Townsend, N.; Wickramasinghe, K.; Bhatnagar, P.; Smolina, K.; Nichols, M.; Leal, J.; Luengo-Fernandez, R.; Rayner, M. Coronary Heart Disease Statistics: A Compendium of Health Statistics, 2012 ed.; British Hearth Foundation: London, UK, 2012. [Google Scholar]
- Van de Werf, F.; Bax, J.; Betriu, A.; Blomstrom-Lundqvist, C.; Crea, F.; Falk, V.; Filippatos, G.; Fox, K.; Huber, K.; Kastrati, A.; et al. Management of acute myocardial infarction in patients presenting with persistent ST-segment elevation: The Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology. Eur. Heart J. 2008, 29, 2909–2945. [Google Scholar]
- National Institute for Health and Clinical Excellence. Myocardial Infarction with ST-segment Elevation; CG167; NICE: London, UK, 2013. [Google Scholar]
- De Luca, G.; Suryapranata, H.; Zijlstra, F.; van’t Hof, A.W.J.; Hoorntje, J.C.A.; Gosselink, A.T.M.; Dambrink, J.; de Boer, M. Symptom-onset-to-balloon time and mortality in patients with acute myocardial infarction treated by primary angioplasty. J. Amer. Coll. Cardiol. 2003, 42, 991–997. [Google Scholar] [CrossRef]
- Scottish Intercollegiate Guidelines Network. Acute Coronary Syndromes; SIGN93; SIGN: Edinburgh, UK, 2013. [Google Scholar]
- Widimsky, P.; Bilkova, D.; Penicka, M.; Novak, M.; Lanikova, M.; Porizka, V.; Groch, L.; Zelizko, M.; Budesinsky, T.; Aschermann, M. Long-term outcomes of patients with acute myocardial infarction presenting to hospitals without catheterization laboratory and randomized to immediate thrombolysis or interhospital transport for primary percutaneous coronary intervention. Five years’ follow-up of the PRAGUE-2 trial. Eur. Heart J. 2007, 28, 679–684. [Google Scholar] [CrossRef]
- Morrison, L.J.; Verbeek, P.R.; McDonald, A.C.; Sawadsky, B.V.; Cook, D.J. Mortality and prehospital thrombolysis for acute myocardial infarction: A meta-analysis. JAMA 2000, 283, 2686–2692. [Google Scholar] [CrossRef]
- Boersma, E.; Maas, A.C.P.; Deckers, J.W.; Simoons, M.L. Early thrombolytic treatment in acute myocardial infarction: Reappraisal of the “golden hour”. Lancet 1996, 348, 771–775. [Google Scholar] [CrossRef] [Green Version]
- The GUSTO Investigators. An international randomized trial comparing four thrombolytic stategies for acute myocardial infarction. N. Engl. J. Med. 1993, 329, 673–682. [Google Scholar] [CrossRef]
- Fibrinolytic Therapy Trialist’s (FFT) Collaborative Group. Indications for fibrinolytic therapy in suspected acute myocardial infarction: Collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1,000 patients. Lancet 1994, 343, 311–322.
- GREAT Group. Feasibility, safety, and efficacy of domiciliary thrombolysis by general practitioners: Grampian region early anistreplase trial. Br. Med. J. 1992, 305, 548–553. [Google Scholar] [CrossRef]
- Rawles, J.; Sinclair, C.; Jennings, K.; Ritchie, L.; Waugh, N. Audit of prehospital thrombolysis by general practitioners in peripheral practices in Grampian. Heart 1998, 80, 231–234. [Google Scholar]
- Nallamothu, B.K.; Fox, K.A.A.; Kennelly, B.M.; van de Werf, F.; Gore, J.M.; Steg, P.G.; Granger, C.B.; Dabbous, O.H.; Kline-Rogers, E.; Eagle, K.A. Relationship of treatment delays and mortality in patients undergoing fibrinolysis and primary percutaneous coronary intervention. The Global Registry of Acute Coronary Events. Heart 2007, 93, 1552–1555. [Google Scholar]
- De Waure, C.; Cadeddu, C.; Gualano, M.R.; Ricciardi, W. Telemedicine for the reduction of myocardial infarction mortality: A systematic review and meta-analysis of published studies. Telemed J. E-Health 2012, 18, 323–328. [Google Scholar]
- MacLeod, M.C.M.; Finlayson, A.R.; Pell, J.P.; Findlay, I.N. Geographic, demographic, and socioeconomic variations in the investigation and management of coronary artery disease in Scotland. Heart 1999, 81, 252–256. [Google Scholar]
- Leslie, S.J.; Henriksen, P.A.; Timlin, H.; Stanton, T.; Spratt, J.C.; Denvir, M.A. Urgent in-patient coronary angiography: A comparison of centres with and without cardiac catheter facilities. Scot. Med. J. 2006, 51, 24–26. [Google Scholar]
- Madsen, J.K.; Grande, P.; Saunamäki, K.; Thayssen, P.; Kassis, E.; Eriksen, U.; Rasmussen, K.; Haunsø, S.; Nielsen, T.T.; Haghfelt, T.; et al.; on behalf of the DANAMI Study Group Danish multicenter randomized study of invasive versus conservative treatment in patients with inducible ischemia after thrombolysis in acute myocardial infarction (DANAMI). Circulation 1997, 96, 748–755. [Google Scholar] [CrossRef]
- Bloe, C.; Mair, C.; Call, A.; Fuller, A.; Menzies, S.; Leslie, S.J. Identification of barriers to the implementation of evidence-based practice for pre-hospital thrombolysis. Rural Remote Health. 2009, 9. Available online: http://www.rrh.org.au/articles/subviewnew.asp?ArticleID=1100 (accessed on 17 February 2014).
- Rawles, J. Attitudes of general practitioners to prehospital thrombolysis. Br. Med. J. 1994, 309, 379–382. [Google Scholar] [CrossRef]
- The Scottish Government. Scotland’s Census 2011. Available online: http://www.scotlandscensus.gov.uk (accessed on 7 December 2013).
- The Highland Council. Highland Facts and Figures. Available online: http://www.highland.gov.uk/yourcouncil/highlandfactsandfigures/highlandprofile.htm (accessed on 7 December 2013).
- Hanson, T.C.; Wilkiamson, D. Identifying barriers to prehospital thrombolysis in the treatment of acute myocardial infarction. Emerg. Med. J. 2006, 23, 650–653. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Rushworth, G.F.; Bloe, C.; Diack, H.L.; Reilly, R.; Murray, C.; Stewart, D.; Leslie, S.J. Pre-Hospital ECG E-Transmission for Patients with Suspected Myocardial Infarction in the Highlands of Scotland. Int. J. Environ. Res. Public Health 2014, 11, 2346-2360. https://doi.org/10.3390/ijerph110202346
Rushworth GF, Bloe C, Diack HL, Reilly R, Murray C, Stewart D, Leslie SJ. Pre-Hospital ECG E-Transmission for Patients with Suspected Myocardial Infarction in the Highlands of Scotland. International Journal of Environmental Research and Public Health. 2014; 11(2):2346-2360. https://doi.org/10.3390/ijerph110202346
Chicago/Turabian StyleRushworth, Gordon F., Charlie Bloe, H. Lesley Diack, Rachel Reilly, Calum Murray, Derek Stewart, and Stephen J. Leslie. 2014. "Pre-Hospital ECG E-Transmission for Patients with Suspected Myocardial Infarction in the Highlands of Scotland" International Journal of Environmental Research and Public Health 11, no. 2: 2346-2360. https://doi.org/10.3390/ijerph110202346