Decreased Survival of Glioma Patients with Astrocytoma Grade IV (Glioblastoma Multiforme) Associated with Long-Term Use of Mobile and Cordless Phones

Abstract
:1. Introduction
1.1. Background
1.2. Some Technical Aspects
1.3. Aim of the Study
2. Materials and Methods
2.1. Study Design
2.2. Statistical Methods
3. Results
3.1. Overall Results
3.2. All Glioma
3.3. Low-Grade Astrocytoma
3.4. Astrocytoma Grade III
3.5. Astrocytoma Grade IV
3.6. Oligodendroglioma
3.7. Other/Mixed Glioma
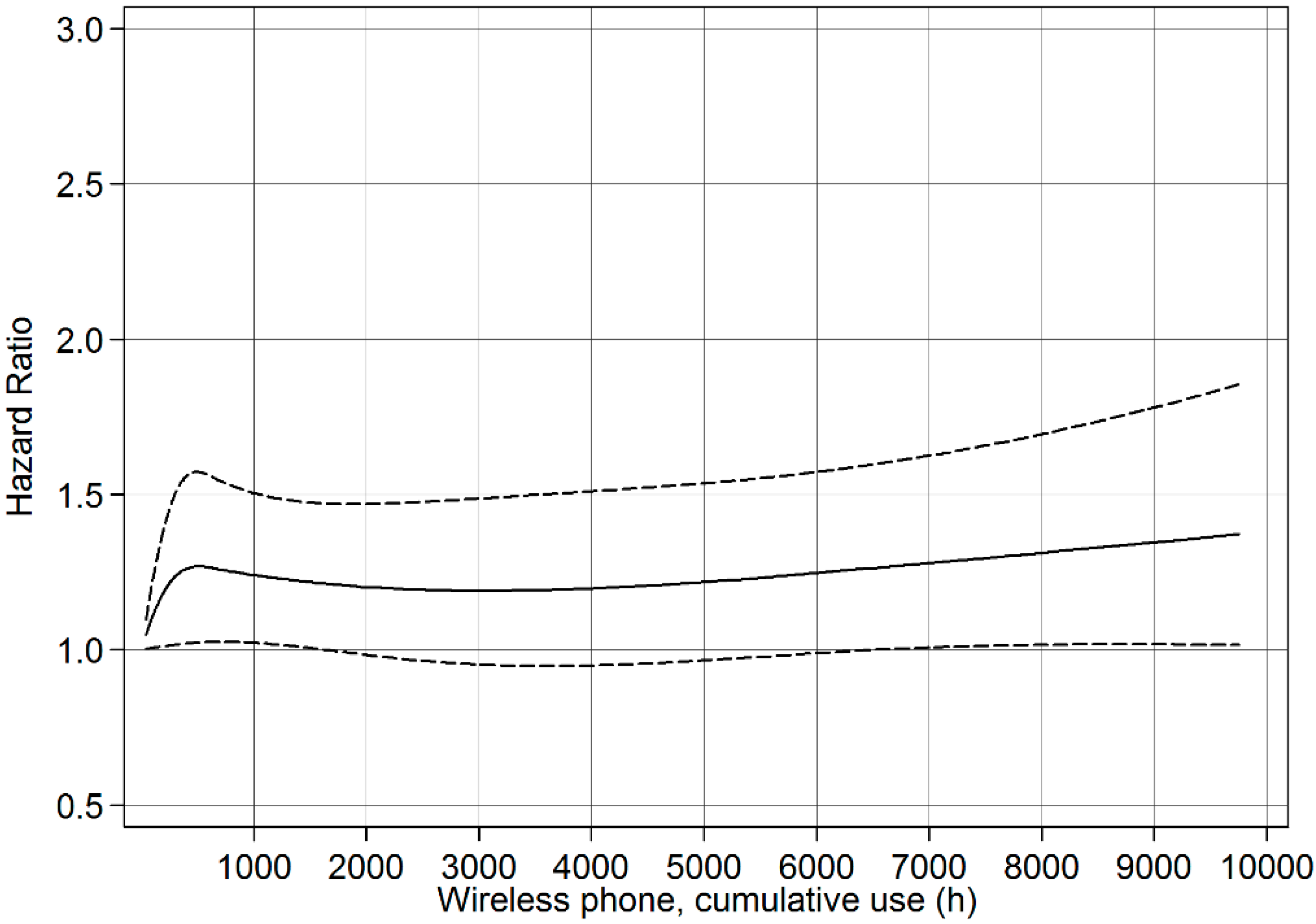
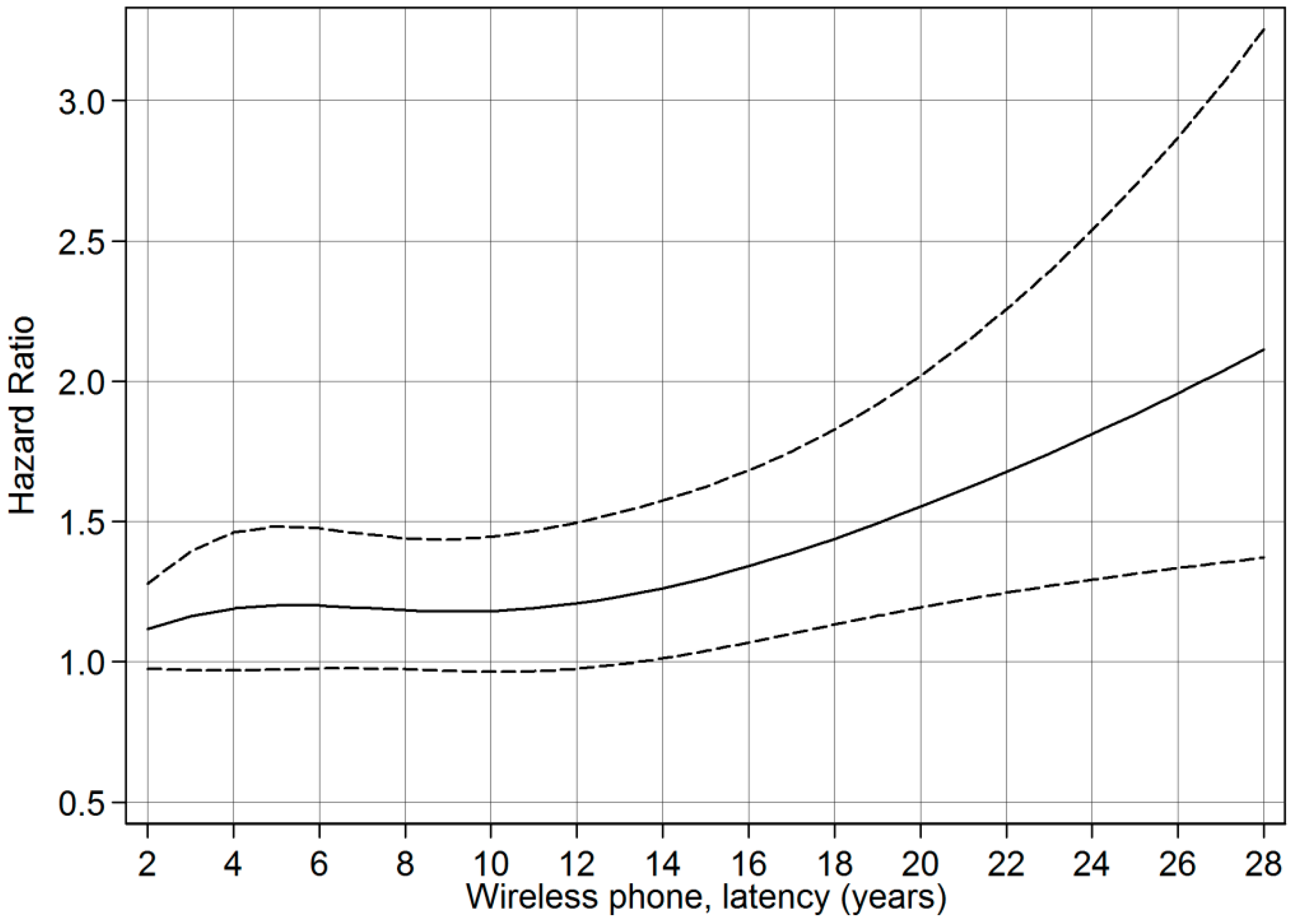
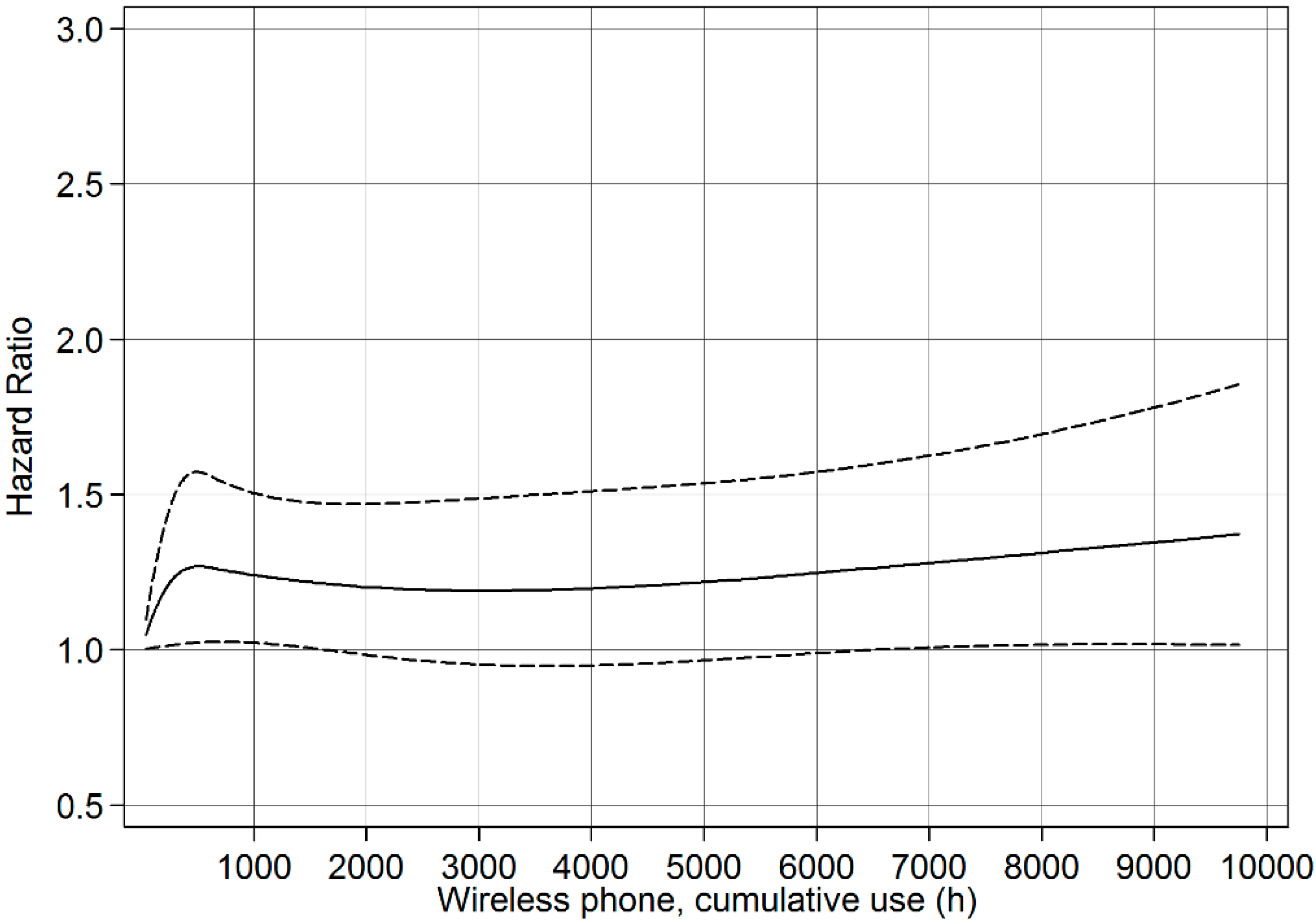
3.8. Restricted Cubic Spline Plots

{kind=link}
{kind=link}
| Exposed Wireless Phone | Unexposed Wireless Phone | p * | All | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | Median | Min | Max | n | Mean | Median | Min | Max | n | Mean | Median | Min | Max | ||
| Glioma | 1198 | 52 | 54 | 19 | 80 | 480 | 61 | 63 | 21 | 80 | <0.0001 | 1678 | 54 | 57 | 19 | 80 |
| -Astrocytoma | 951 | 53 | 56 | 19 | 80 | 402 | 62 | 64 | 23 | 80 | <0.0001 | 1353 | 56 | 58 | 19 | 80 |
| -grade I–II | 189 | 41 | 39 | 19 | 74 | 39 | 48 | 52 | 23 | 71 | 0.02 | 228 | 42 | 40 | 19 | 74 |
| -grade III ** | 143 | 48 | 50 | 20 | 80 | 53 | 60 | 63 | 27 | 77 | <0.0001 | 196 | 51 | 54 | 20 | 80 |
| -grade IV ** | 618 | 58 | 59 | 21 | 79 | 308 | 64 | 66 | 29 | 80 | <0.0001 | 926 | 60 | 61 | 21 | 80 |
| -Oligodendroglioma | 135 | 48 | 48 | 20 | 73 | 36 | 54 | 57 | 22 | 75 | 0.02 | 171 | 49 | 50 | 20 | 75 |
| -Other/mixed glioma | 112 | 48 | 47 | 20 | 75 | 42 | 50 | 54 | 21 | 79 | 0.33 | 154 | 48 | 48 | 20 | 79 |
| Mobile Phone | Cordless Phone | Wireless Phone | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n, exp | HR | 95% CI | p | n, exp | HR | 95% CI | p | n, exp | HR | 95% CI | p | |
| Glioma, all (ntot = 1678; nunexp = 480) | ||||||||||||
| All | 1037 | 1.1 | 0.9–1.3 | 0.37 | 825 | 1.0 | 0.9–1.2 | 0.85 | 1198 | 1.1 | 0.9–1.2 | 0.32 |
| -Per 100 h cumulative use | 1.000 | 0.997–1.003 | 0.97 | 1.004 | 1.0002–1.009 | 0.04 | 1.001 | 0.999–1.003 | 0.37 | |||
| -Per year of latency | 1.016 | 1.004–1.028 | 0.01 | 1.014 | 0.997–1.030 | 0.10 | 1.015 | 1.003–1.026 | 0.01 | |||
| Astrocytoma, grade I–II (ntot = 228; nunexp = 39) | ||||||||||||
| All | 164 | 0.5 | 0.3–0.9 | 0.02 | 135 | 0.6 | 0.3–1.1 | 0.09 | 189 | 0.6 | 0.3–0.9 | 0.03 |
| -Per 100 h cumulative use | 0.996 | 0.982–1.009 | 0.52 | 0.990 | 0.974–1.006 | 0.21 | 0.995 | 0.986–1.005 | 0.32 | |||
| -Per year of latency | 0.966 | 0.913–1.022 | 0.23 | 0.964 | 0.906–1.027 | 0.26 | 0.966 | 0.920–1.016 | 0.18 | |||
| Astrocytoma, grade III * (ntot = 196; nunexp = 53) | ||||||||||||
| All | 127 | 0.7 | 0.5–1.2 | 0.22 | 95 | 0.7 | 0.4–1.2 | 0.16 | 143 | 0.8 | 0.5–1.3 | 0.38 |
| -Per 100 h cumulative use | 1.000 | 0.993–1.007 | 0.95 | 1.011 | 0.995–1.028 | 0.18 | 1.000 | 0.995–1.006 | 0.87 | |||
| -Per year of latency | 0.988 | 0.953–1.025 | 0.54 | 0.991 | 0.943–1.042 | 0.73 | 0.988 | 0.955–1.023 | 0.49 | |||
| Astrocytoma, grade IV * (ntot = 926; nunexp = 308) | ||||||||||||
| All | 532 | 1.2 | 0.95–1.4 | 0.15 | 415 | 1.1 | 0.9–1.4 | 0.20 | 618 | 1.2 | 0.98–1.4 | 0.08 |
| -Per 100 h cumulative use | 1.002 | 0.998–1.006 | 0.30 | 1.004 | 0.998–1.010 | 0.18 | 1.002 | 0.999–1.005 | 0.14 | |||
| -Per year of latency | 1.017 | 1.004–1.031 | 0.01 | 1.023 | 1.004–1.043 | 0.02 | 1.020 | 1.007–1.033 | 0.003 | |||
| Oligodendroglioma (ntot = 171; nunexp = 36) | ||||||||||||
| All | 119 | 1.0 | 0.5–2.1 | 0.92 | 99 | 0.6 | 0.2–1.3 | 0.17 | 135 | 1.1 | 0.6–2.2 | 0.72 |
| -Per 100 h cumulative use | 0.992 | 0.969–1.016 | 0.52 | 0.988 | 0.952–1.026 | 0.55 | 0.992 | 0.975–1.010 | 0.40 | |||
| -Per year of latency | 1.000 | 0.947–1.057 | 0.996 | 0.917 | 0.837–1.006 | 0.07 | 0.973 | 0.922–1.026 | 0.31 | |||
| Other/mixed glioma (ntot = 154; nunexp = 42) | ||||||||||||
| All | 95 | 1.7 | 0.9–3.4 | 0.12 | 80 | 1.7 | 0.9–3.3 | 0.10 | 112 | 1.7 | 0.9–3.1 | 0.11 |
| -Per 100 h cumulative use | 0.996 | 0.984–1.008 | 0.54 | 1.010 | 0.997–1.023 | 0.13 | 1.000 | 0.993–1.008 | 0.90 | |||
| -Per year of latency | 1.039 | 0.984–1.098 | 0.17 | 1.021 | 0.943–1.106 | 0.61 | 1.048 | 0.993–1.107 | 0.09 | |||
| Mobile Phone | Cordless Phone | Wireless Phone | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n, exp | HR | 95% CI | p | n, exp | HR | 95% CI | p | n, exp | HR | 95% CI | p | |
| Glioma, all (ntot = 1,678; nunexp = 480) | ||||||||||||
| Latency * | ||||||||||||
| >1–5 year | 291 | 1.0 | 0.8–1.2 | 0.97 | 299 | 0.9 | 0.8–1.1 | 0.35 | 307 | 1.0 | 0.8–1.2 | 0.90 |
| >5–10 year | 331 | 1.2 | 0.95–1.4 | 0.15 | 328 | 1.1 | 0.9–1.4 | 0.18 | 399 | 1.2 | 0.99–1.4 | 0.06 |
| >10–15 year | 229 | 1.1 | 0.9–1.4 | 0.45 | 142 | 1.2 | 0.9–1.5 | 0.21 | 273 | 1.1 | 0.9–1.4 | 0.32 |
| >15–20 year | 107 | 1.2 | 0.9–1.6 | 0.19 | 50 | 0.9 | 0.6–1.3 | 0.53 | 136 | 1.1 | 0.8–1.4 | 0.54 |
| >20 year | 79 | 1.8 | 1.3–2.5 | <0.001 | 6 | 1.3 | 0.5–3.7 | 0.56 | 83 | 1.7 | 1.2–2.3 | 0.001 |
| Hours * | ||||||||||||
| First quartile ** | 428 | 1.0 | 0.9–1.2 | 0.66 | 190 | 0.9 | 0.7–1.1 | 0.19 | 290 | 1.0 | 0.9–1.2 | 0.92 |
| Second quartile | 203 | 1.1 | 0.9–1.4 | 0.25 | 218 | 1.0 | 0.8–1.2 | 0.80 | 260 | 1.1 | 0.9–1.3 | 0.44 |
| Third quartile | 181 | 1.3 | 0.99–1.6 | 0.06 | 233 | 1.2 | 0.95–1.5 | 0.13 | 261 | 1.2 | 0.98–1.5 | 0.08 |
| Fourth quartile | 225 | 1.1 | 0.9–1.4 | 0.41 | 184 | 1.3 | 0.99–1.6 | 0.06 | 387 | 1.2 | 0.97–1.4 | 0.09 |
| Age, first use | ||||||||||||
| <20 years old | 69 | 1.0 | 0.6–1.7 | 0.97 | 46 | 0.9 | 0.5–1.7 | 0.83 | 81 | 1.0 | 0.6–1.6 | 0.91 |
| 20–49 years old | 646 | 1.1 | 0.9–1.4 | 0.16 | 457 | 1.0 | 0.8–1.3 | 0.72 | 724 | 1.1 | 0.9–1.3 | 0.23 |
| ≥50 years old | 322 | 1.0 | 0.9–1.2 | 0.81 | 322 | 1.0 | 0.8–1.2 | 0.96 | 393 | 1.0 | 0.9–1.2 | 0.54 |
| Astrocytoma, grade IV (ntot = 926; nunexp = 308) | ||||||||||||
| Latency *** | ||||||||||||
| >1–5 year | 137 | 1.2 | 0.9–1.5 | 0.18 | 137 | 1.0 | 0.8–1.3 | 0.76 | 145 | 1.1 | 0.9–1.4 | 0.24 |
| >5–10 year | 157 | 1.1 | 0.9–1.4 | 0.47 | 174 | 1.2 | 0.9–1.5 | 0.14 | 201 | 1.1 | 0.9–1.4 | 0.24 |
| >10–15 year | 120 | 1.2 | 0.9–1.6 | 0.17 | 77 | 1.5 | 1.1–2.1 | 0.01 | 142 | 1.3 | 1.01–1.7 | 0.04 |
| >15–20 year | 66 | 1.2 | 0.8–1.6 | 0.35 | 24 | 1.2 | 0.7–2.0 | 0.43 | 76 | 1.3 | 0.9–1.7 | 0.14 |
| >20 year | 52 | 2.0 | 1.4–2.9 | <0.001 | 3 | 3.4 | 1.04–11 | 0.04 | 54 | 2.1 | 1.5–3.0 | <0.001 |
| Hours *** | ||||||||||||
| First quartile ** | 228 | 1.1 | 0.9–1.4 | 0.25 | 97 | 0.9 | 0.7–1.2 | 0.67 | 159 | 1.1 | 0.9–1.3 | 0.54 |
| Second quartile | 105 | 1.1 | 0.9–1.5 | 0.32 | 97 | 1.1 | 0.9–1.5 | 0.36 | 129 | 1.2 | 0.9–1.5 | 0.21 |
| Third quartile | 87 | 1.4 | 1.01–1.8 | 0.045 | 121 | 1.4 | 1.04–1.8 | 0.02 | 140 | 1.3 | 1.1–1.7 | 0.02 |
| Fourth quartile | 112 | 1.2 | 0.9–1.6 | 0.34 | 100 | 1.2 | 0.9–1.6 | 0.12 | 190 | 1.3 | 0.99–1.6 | 0.06 |
| Age, first use | ||||||||||||
| <20 years old | 10 | 2.2 | 1.04–4.8 | 0.04 | 6 | 1.8 | 0.7– 4.7 | 0.24 | 11 | 2.3 | 1.1–4.7 | 0.03 |
| 20–49 years old | 296 | 1.2 | 0.98–1.6 | 0.07 | 177 | 1.3 | 1.001–1.7 | 0.049 | 328 | 1.2 | 0.99–1.5 | 0.07 |
| ≥50 years old | 226 | 1.1 | 0.9–1.4 | 0.31 | 232 | 1.1 | 0.9–1.3 | 0.43 | 279 | 1.1 | 0.9–1.4 | 0.17 |

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Cardis, E.; Deltour, I.; Mann, S.; Moissonnier, M.; Taki, M.; Varsier, N.; Wake, K.; Wiart, J. Distribution of RF energy emitted by mobile phones in anatomical structures of the brain. Phys. Med. Biol. 2008, 53, 2771–2783. [Google Scholar] [CrossRef]
- Gandhi, O.P.; Morgan, L.L.; de Salles, A.A.; Han, Y.Y.; Herberman, R.B.; Davis, D.L. Exposure limits: The underestimation of absorbed cell phone radiation, especially in children. Electromagn. Biol. Med. 2012, 31, 34–51. [Google Scholar] [CrossRef]
- Linde, T.; Hansson Mild, K. Measurement of low frequency magnetic fields from digital cellular telephones. Bioelectromagnetics 1997, 18, 184–186. [Google Scholar] [CrossRef]
- Baan, R.; Grosse, Y.; Lauby-Secretan, B.; El Ghissassi, F.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Islami, F.; Galichet, L.; Straif, K. Carcinogenicity of radiofrequency electromagnetic fields. Lancet Oncol. 2011, 12, 624–626. [Google Scholar] [CrossRef]
- IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Volume 102. Non-Ionizing Radiation, Part 2: Radiofrequency Electromagnetic Fields. International Agency for Research on Cancer: Lyon, France, 2013. Available online: http://monographs.iarc.fr/ENG/Monographs/vol102/mono102.pdf (accessed on 2 September 2014).
- Hardell, L.; Carlberg, M.; Hansson Mild, K. Pooled analysis of two case-control studies on use of cellular and cordless telephones and the risk for malignant brain tumours diagnosed in 1997–2003. Int. Arch. Occup. Environ. Health 2006, 79, 630–639. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M.; Hansson Mild, K. Pooled analysis of two case-control studies on the use of cellular and cordless telephones and the risk of benign brain tumours diagnosed during 1997–2003. Int. J. Oncol. 2006, 28, 509–518. [Google Scholar]
- Hardell, L.; Carlberg, M.; Hansson Mild, K. Pooled analysis of case-control studies on malignant brain tumours and the use of mobile and cordless phones including living and deceased subjects. Int. J. Oncol. 2011, 38, 1465–1474. [Google Scholar] [CrossRef]
- Interphone Study Group. Brain tumour risk in relation to mobile telephone use: Results of the INTERPHONE international case-control study. Int. J. Epidemiol. 2010, 39, 675–694. [Google Scholar]
- Interphone Study Group. Acoustic neuroma risk in relation to mobile telephone use: Results of the INTERPHONE international case-control study. Cancer Epidemiol. 2011, 35, 453–464. [Google Scholar]
- Cardis, E.; Armstrong, B.K.; Bowman, J.D.; Giles, G.G.; Hours, M.; Krewski, D.; McBride, M.; Parent, M.E.; Sadetzki, S.; Woodward, A.; et al. Risk of brain tumours in relation to estimated RF dose from mobile phones: Results from five Interphone countries. Occup. Environ. Med. 2011, 68, 631–640. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M.; Hansson Mild, K. Mobile phone use and the risk for malignant brain tumours: A case-control study on deceased cases and controls. Neuroepidemiology 2010, 35, 109–114. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M.; Söderqvist, F.; Hansson Mild, K. Case-control study of the association between malignant brain tumours diagnosed between 2007 and 2009 and mobile and cordless phone use. Int. J. Oncol. 2013, 43, 1833–1845. [Google Scholar]
- Hardell, L.; Carlberg, M. Use of mobile and cordless phones and survival of patients with glioma. Neuroepidemiology 2013, 40, 101–108. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr. Regression Modeling Strategies. With Application to Linear Models, Logistic Regression and Survival Analysis; Springer: New York, NY, USA, 2001; pp. 20–26. [Google Scholar]
- Hutter, H.P.; Ehrenhöfer, L.; Freuis, E.; Hartl, P.; Kundi, M. Poor-to-moderate agreement between self and proxy interviews of mobile phone use. Bioelectromagnetics 2012, 33, 561–567. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M. Mobile phones, cordless phones and the risk for brain tumours. Int. J. Oncol. 2009, 35, 5–17. [Google Scholar] [CrossRef]
- Vertosick, F.T., Jr.; Selker, R.G.; Arena, V.C. Survival of patients with well-differentiated astrocytomas diagnosed in the era of computed tomography. Neurosurgery 1991, 28, 496–501. [Google Scholar] [CrossRef]
- Ohgaki, H.; Kleihues, P. Population-based studies on incidence, survival rates, and genetic alterations in astrocytic and oligodendroglial gliomas. J. Neuropathol. Exp. Neurol. 2005, 64, 479–489. [Google Scholar]
- Akhavan-Sigari, R.; Baf, M.M.; Ariabod, V.; Rohde, V.; Rahighi, S. Connection between cell phone use, p53 gene expression in different zones of glioblastoma multiforme and survival prognoses. Rare Tumors 2014, 6. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M. Using the Hill viewpoints from 1965 for evaluating strengths of evidence of the risk for brain tumors associated with use of mobile and cordless phones. Rev. Environ. Health 2013, 28, 97–106. [Google Scholar] [CrossRef]
- Carlberg, M.; Hardell, L. On the association between glioma, wireless phones, heredity and ionising radiation. Pathophysiology 2012, 19, 243–252. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlberg, M.; Hardell, L. Decreased Survival of Glioma Patients with Astrocytoma Grade IV (Glioblastoma Multiforme) Associated with Long-Term Use of Mobile and Cordless Phones. Int. J. Environ. Res. Public Health 2014, 11, 10790-10805. https://doi.org/10.3390/ijerph111010790
Carlberg M, Hardell L. Decreased Survival of Glioma Patients with Astrocytoma Grade IV (Glioblastoma Multiforme) Associated with Long-Term Use of Mobile and Cordless Phones. International Journal of Environmental Research and Public Health. 2014; 11(10):10790-10805. https://doi.org/10.3390/ijerph111010790
Chicago/Turabian StyleCarlberg, Michael, and Lennart Hardell. 2014. "Decreased Survival of Glioma Patients with Astrocytoma Grade IV (Glioblastoma Multiforme) Associated with Long-Term Use of Mobile and Cordless Phones" International Journal of Environmental Research and Public Health 11, no. 10: 10790-10805. https://doi.org/10.3390/ijerph111010790
APA StyleCarlberg, M., & Hardell, L. (2014). Decreased Survival of Glioma Patients with Astrocytoma Grade IV (Glioblastoma Multiforme) Associated with Long-Term Use of Mobile and Cordless Phones. International Journal of Environmental Research and Public Health, 11(10), 10790-10805. https://doi.org/10.3390/ijerph111010790