Early Childhood Caries and Body Mass Index in Young Children from Low Income Families

Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Participants

{kind=link}
{kind=link}
| Variable | Mean | Standard deviation | Minimum | Maximum |
|---|---|---|---|---|
| Family monthly income (as a fold-value compared to the average Brazilian minimum wage) | 2.3 | 1.5 | 0.5 | 10.0 |
| Mothers’ formal education (in years) | 9.8 | 3.1 | 0 | 22.0 |
| Caregivers’ age (in years) | 35.3 | 12.0 | 12.0 | 69.0 |
| Children’s age (in months) | 68.7 | 3.8 | 61.0 | 79.0 |
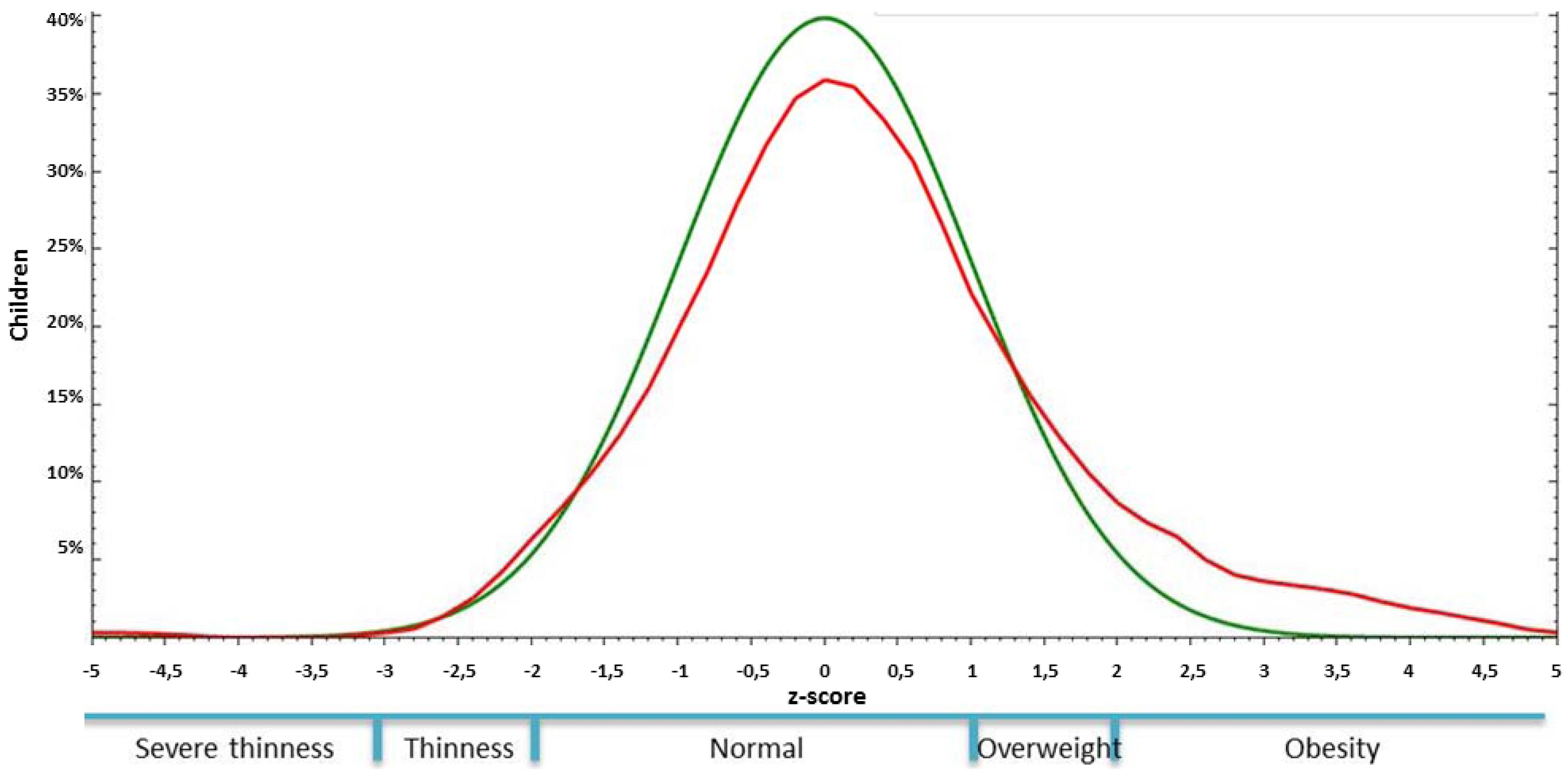
3.2. Early Childhood Caries (ECC) and Body Mass Index (BMI)

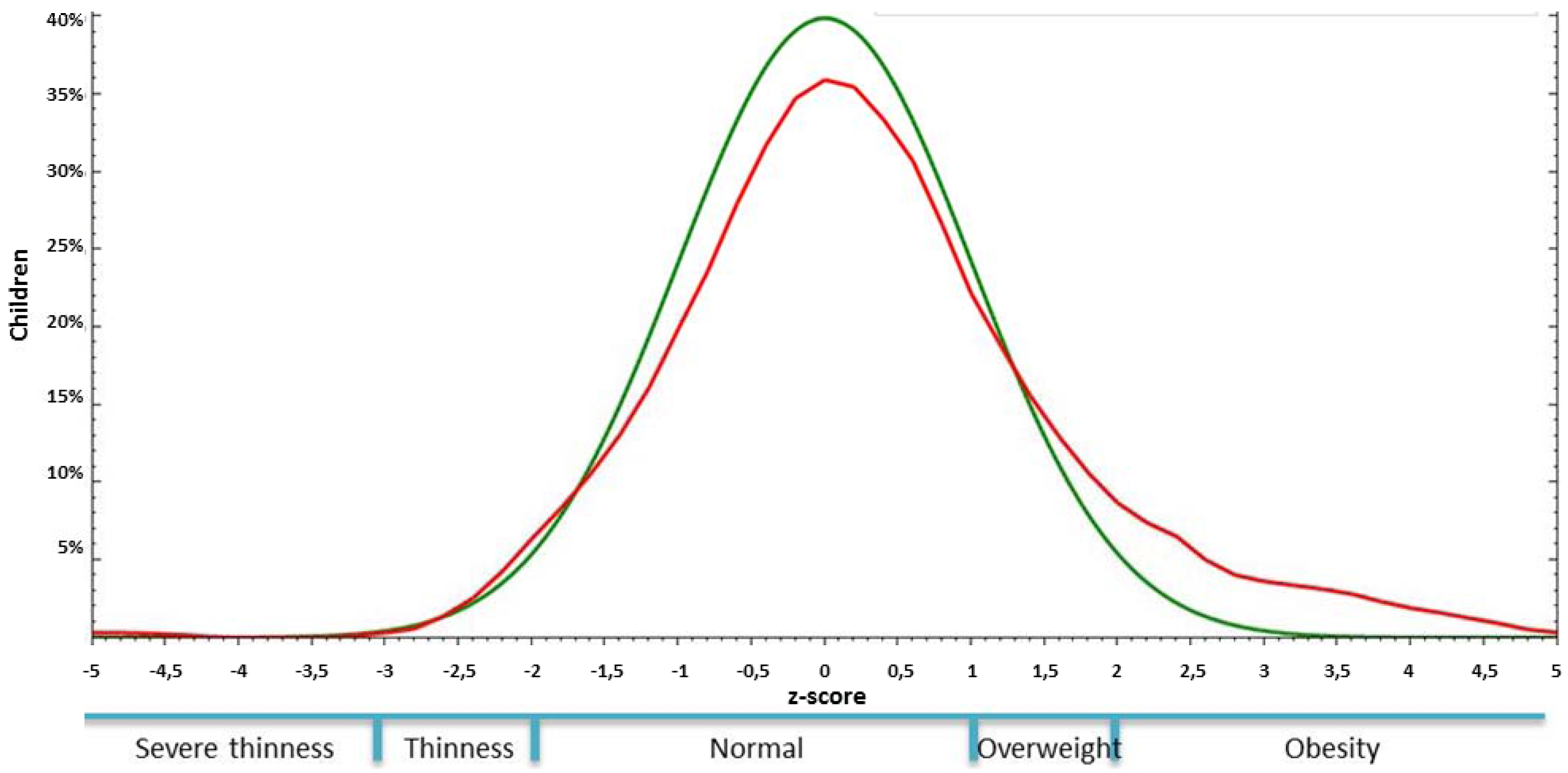
| Body Mass Index Category (a) | Caries experience, n (%) | Active Early Childhood Caries, n (%) | Active Severe Early Childhood Caries, n (%) |
|---|---|---|---|
| Severe thinness or thinness | 1 (0.7%) | 0 (0.0%) | 0 (0.0%) |
| Adequate | 114 (79.7%) | 97 (80.2%) | 39 (84.8%) |
| Overweight | 18 (12.5%) | 15 (12.4%) | 5 (10.9%) |
| Obesity | 10 (7.0%) | 9 (7.4%) | 2 (4.3%) |
| Total | 143 (100.0%) | 121 (100.0%) | 46 (100.0%) |
| Independent variables | OR | 95%CI | p-value |
|---|---|---|---|
| Children being overweight or obese | 1.32 | 0.70–2.50 | 0.40 |
| Children’s age [1] | 0.94 | 0.88–1.00 | 0.06 |
| Mother’s level of formal education [1] | 1.03 | 0.94–1.13 | 0.51 |
| Family income [1] | 1.22 | 1.01–1.50 | 0.04 |
4. Discussion
5. Conclusions
Acknowledgments
Conflict of Interest
References
- American Academy on Pediatric Dentistry. Policy on early childhood caries (ECC): Classifications, consequences, and preventive strategies. Pediatr. Dent. 2008, 30 (Suppl. 7), 40–43.
- Gaur, S.; Nayak, R. Underweight in low socioeconomic status preschool children with severe early childhood caries. J. Indian Soc. Pedod. Prev. Dent. 2011, 29, 305–309. [Google Scholar] [CrossRef]
- Gradella, C.M.; Bernabe, E.; Bonecker, M.; Oliveira, L.B. Caries prevalence and severity, and quality of life in Brazilian 2- to 4-year-old children. Community Dent. Oral Epidemiol. 2011, 39, 498–504. [Google Scholar] [CrossRef]
- Vania, A.; Parisella, V.; Capasso, F.; Di Tanna, G.L.; Vestri, A.; Ferrari, M.; Polimeni, A. Early childhood caries underweight or overweight, that is the question. Eur. J. Paediatr. Dent. 2011, 12, 231–235. [Google Scholar]
- Caufield, P.W.; Li, Y.; Bromage, T.G. Hypoplasia-associated severe early childhood caries—A proposed definition. J. Dent. Res. 2012, 91, 544–550. [Google Scholar]
- Kantovitz, K.R.; Pascon, F.M.; Rontani, R.M.; Gaviao, M.B. Obesity and dental caries—A systematic review. Oral Health Prev. Dent. 2006, 4, 137–144. [Google Scholar]
- Werner, S.L.; Phillips, C.; Koroluk, L.D. Association between childhood obesity and dental caries. Pediatr. Dent. 2012, 34, 23–27. [Google Scholar]
- Sheller, B.; Churchill, S.S.; Williams, B.J.; Davidson, B. Body mass index of children with severe early childhood caries. Pediatr. Dent. 2009, 31, 216–221. [Google Scholar]
- Norberg, C.; Hallstrom Stalin, U.; Matsson, L.; Thorngren-Jerneck, K.; Klingberg, G. Body mass index (BMI) and dental caries in 5-year-old children from southern Sweden. Community Dent. Oral Epidemiol. 2012, 40, 315–322. [Google Scholar] [CrossRef]
- van Gemert-Schriks, M.C.; van Amerongen, E.W.; Aartman, I.H.; Wennink, J.M.; Ten Cate, J.M.; de Soet, J.J. The influence of dental caries on body growth in prepubertal children. Clin. Oral Invest. 2011, 15, 141–149. [Google Scholar] [CrossRef]
- Subramaniam, P.; Singh, D. Association of age specific body mass index, dental caries and socioeconomic status of children and adolescents. J. Clin. Pediatr. Dent. 2011, 36, 175–179. [Google Scholar]
- Koksal, E.; Tekcicek, M.; Yalcin, S.S.; Tugrul, B.; Yalcin, S.; Pekcan, G. Association between anthropometric measurements and dental caries in Turkish school children. Cent. Eur. J. Public Health 2011, 19, 147–151. [Google Scholar] [CrossRef]
- Ngoenwiwatkul, Y.; Leela-adisorn, N. Effects of dental caries on nutritional status among first-grade primary school children. Asia Pac. J. Public Health 2009, 21, 177–183. [Google Scholar] [CrossRef]
- Floyd, B. Associations between height, body mass, and frequency of decayed, extracted, and filled deciduous teeth among two cohorts of Taiwanese first graders. Am. J. Phys. Anthropol. 2009, 140, 113–119. [Google Scholar] [CrossRef]
- Cameron, F.L.; Weaver, L.T.; Wright, C.M.; Welbury, R.R. Dietary and social characteristics of children with severe tooth decay. Scott. Med. J. 2006, 51, 26–29. [Google Scholar] [CrossRef]
- Oliveira, L.B.; Sheiham, A.; Bonecker, M. Exploring the association of dental caries with social factors and nutritional status in Brazilian preschool children. Eur. J. Oral Sci. 2008, 116, 37–43. [Google Scholar] [CrossRef]
- Trikaliotis, A.; Boka, V.; Kotsanos, N.; Karagiannis, V.; Hassapidou, M. Short communication: Dmfs and BMI in preschool Greek children. An epidemiological study. Eur. Arch. Paediatr. Dent. 2011, 12, 176–178. [Google Scholar]
- Mojarad, F.; Maybodi, M.H. Association between dental caries and body mass index among hamedan elementary school children in 2009. J. Dent. (Tehran) 2011, 8, 170–177. [Google Scholar]
- D’Mello, G.; Chia, L.; Hamilton, S.D.; Thomson, W.M.; Drummon, B.K. Childhood obesity and dental caries among paediatric dental clinic attenders. Int. J. Paediatr. Dent. 2011, 21, 217–222. [Google Scholar] [CrossRef]
- Costacurta, M.; Di Renzo, L.; Bianchi, A.; Fabiocchi, F.; De Lorenzo, A.; Docimo, R. Obesity and dental caries in paediatric patients. A cross-sectional study. Eur. J. Paediatr. Dent. 2011, 12, 112–116. [Google Scholar]
- Vazquez-Nava, F.; Vazquez-Rodriguez, E.M.; Saldivar-Gonzalez, A.H.; Lin-Ochoa, D.; Martinez-Perales, G.M.; Joffre-Velazquez, V.M. Association between obesity and dental caries in a group of preschool children in Mexico. J. Public Health Dent. 2010, 70, 124–130. [Google Scholar]
- Juarez-Lopez, M.L.; Villa-Ramos, A. Caries prevalence in preschool children with overweight and obesity. Rev. Invest. Clin. 2010, 62, 115–120. [Google Scholar]
- Hong, L.; Ahmed, A.; McCunniff, M.; Overman, P.; Mathew, M. Obesity and dental caries in children aged 2–6 years in the United States: National Health and Nutrition Examination Survey 1999–2002. J. Public Health Dent. 2008, 68, 227–233. [Google Scholar] [CrossRef]
- Willershausen, B.; Moschos, D.; Azrak, B.; Blettner, M. Correlation between oral health and body mass index (BMI) in 2071 primary school pupils. Eur. J. Med. Res. 2007, 12, 295–299. [Google Scholar]
- Marshall, T.A.; Eichenberger-Gilmore, J.M.; Broffitt, B.A.; Warren, J.J.; Levy, S.M. Dental caries and childhood obesity: Roles of diet and socioeconomic status. Community Dent. Oral Epidemiol. 2007, 35, 449–458. [Google Scholar] [CrossRef]
- Gerdin, E.W.; Angbratt, M.; Aronsson, K.; Eriksson, E.; Johansson, I. Dental caries and body mass index by socio-economic status in Swedish children. Community Dent. Oral Epidemiol. 2008, 36, 459–465. [Google Scholar] [CrossRef]
- Malek Mohammadi, T.; Wright, C.M.; Kay, E.J. Childhood growth and dental caries. Community Dent. Health 2009, 26, 38–42. [Google Scholar]
- Clarke, M.; Locker, D.; Berall, G.; Pencharz, P.; Kenny, D.J.; Judd, P. Malnourishment in a population of young children with severe early childhood caries. Pediatr. Dent. 2006, 28, 254–259. [Google Scholar]
- Alm, A.; Isaksson, H.; Fahraeus, C.; Koch, G.; Andersson-Gare, B.; Nilsson, M.; Birkhed, D.; Wendts, L.K. BMI status in Swedish children and young adults in relation to caries prevalence. Swed. Dent. J. 2011, 35, 1–8. [Google Scholar]
- Kopycka-Kedzierawski, D.T.; Auinger, P.; Billings, R.J.; Weitzman, M. Caries status and overweight in 2- to 18-year-old US children: Findings from national surveys. Community Dent. Oral Epidemiol. 2008, 36, 157–67. [Google Scholar] [CrossRef]
- Bonecker, M.; Ardenghi, T.M.; Oliveira, L.B.; Sheiham, A.; Marcenes, W. Trends in dental caries in 1- to 4-year-old children in a Brazilian city between 1997 and 2008. Int. J. Paediatr. Dent. 2010, 20, 125–131. [Google Scholar] [CrossRef]
- Projeto SB Brasil 2003: Condições de Saúde Bucal da População Brasileira 2002–2003: Resultados Principais; Ministério da Saúde: Brasília, Brasil, 2004.
- World Health Organization, Expert Committee on Physical Status. In Physical Status: The Use and Interpretation of Anthropometry; World Health Organization: Geneva, Switzerland, 1995; WHO Technical Report Series, No. 854.
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- World Health Organization, Oral Health Surveys: Basic Methods, 4th ed; World Health Organization: Geneva, Switzerland, 1997.
- Bratthall, D. Introducing the Significant Caries Index together with a proposal for a new global oral health goal for 12-year-olds. Int. Dent. J. 2000, 50, 378–384. [Google Scholar] [CrossRef]
- Cicchetti, D.V.; Sparrow, S.A. Developing criteria for establishing interrater reliability of specific items: Applications to assessment of adaptive behavior. Am. J. Ment. Defic. 1981, 86, 127–137. [Google Scholar]
- Kim Seow, W. Environmental, maternal, and child factors which contribute to early childhood caries: A unifying conceptual model. Int. J. Paediatr. Dent. 2012, 22, 157–168. [Google Scholar] [CrossRef]
- Hooley, M.; Skouteris, H.; Boganin, C.; Satur, J.; Kilpatrick, N. Parental influence and the development of dental caries in children aged 0–6 years: A systematic review of the literature. J. Dent. 2012, 40, 873–885. [Google Scholar] [CrossRef]
- Sales-Peres, S.H.; Goya, S.; Sant’Anna, R.M.; Silva, H.M.; Sales-Peres Ade, C.; Silva, R.P.; Lauris, J.R.; Bastos, J.R. [Prevalence of overweight and obesity, and associated factors in adolescents, at the central west area of the state Sao Paulo (SP, Brazil)]. Cien. Saude Colet. 2010, 15 (Suppl. 2), 3175–3184. [Google Scholar]
- Peres, M.A.; Latorre, M.R.; Sheiham, A.; Peres, K.G.; Barros, F.C.; Hernandez, P.G.; Maas, A.M.N.; Romano, A.R.; Victora, C.G. Effects of social and biological factors on dental caries in 6-year-old children: A cross sectional study nested in a birth cohort in Southern Brazil. Rev. Bras. Epidemiol. 2003, 6, 293–306. [Google Scholar]
- Melo, M.M.; Souza, W.V.; Lima, M.L.; Braga, C. Factors associated with dental caries in preschoolers in Recife, Pernambuco State, Brazil. Cad. Saude Publica 2011, 27, 471–485. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Vieira, A.J.; Garret, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar]
- Moss, B.G.; Yeaton, W.H. U.S. children’s preschool weight status trajectories: Patterns from 9-month, 2-year, and 4-year Early Childhood Longitudinal Study—Birth cohort data. Am. J. Health Promot. 2012, 26, 172–175. [Google Scholar] [CrossRef]
- Benzian, H.; Monse, B.; Heinrich-Weltzien, R.; Hobdell, M.; Mulder, J.; van Palenstein Helderman, W. Untreated severe dental decay: A neglected determinant of low Body Mass Index in 12-year-old Filipino children. BMC Public Health 2011, 11. [Google Scholar] [CrossRef]
- Victora, C.G.; Aquino, E.M.; do Carmo Leal, M.; Monteiro, C.A.; Barros, F.C.; Szwarcwald, C.L. Maternal and child health in Brazil: Progress and challenges. Lancet 2011, 377, 1863–1876. [Google Scholar]
- Feldens, C.A.; Giugliani, E.R.; Duncan, B.B.; Drachler Mde, L.; Vitolo, M.R. Long-term effectiveness of a nutritional program in reducing early childhood caries: A randomized trial. Community Dent. Oral Epidemiol. 2010, 38, 324–332. [Google Scholar] [CrossRef]
- Campos, J.A.; Melanda, E.A.; Antunes Jda, S.; Foschini, A.L. Dental caries and the nutritional status of preschool children: A spatial analysis. Cien. Saude Colet. 2011, 16, 4161–4168. [Google Scholar]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Costa, L.R.; Daher, A.; Queiroz, M.G. Early Childhood Caries and Body Mass Index in Young Children from Low Income Families. Int. J. Environ. Res. Public Health 2013, 10, 867-878. https://doi.org/10.3390/ijerph10030867
Costa LR, Daher A, Queiroz MG. Early Childhood Caries and Body Mass Index in Young Children from Low Income Families. International Journal of Environmental Research and Public Health. 2013; 10(3):867-878. https://doi.org/10.3390/ijerph10030867
Chicago/Turabian StyleCosta, Luciane Rezende, Anelise Daher, and Maria Goretti Queiroz. 2013. "Early Childhood Caries and Body Mass Index in Young Children from Low Income Families" International Journal of Environmental Research and Public Health 10, no. 3: 867-878. https://doi.org/10.3390/ijerph10030867