Psychological Distress, Related Work Attendance, and Productivity Loss in Small-to-Medium Enterprise Owner/Managers


Abstract
:1. Introduction
1.1. Background and Rationale for the Study
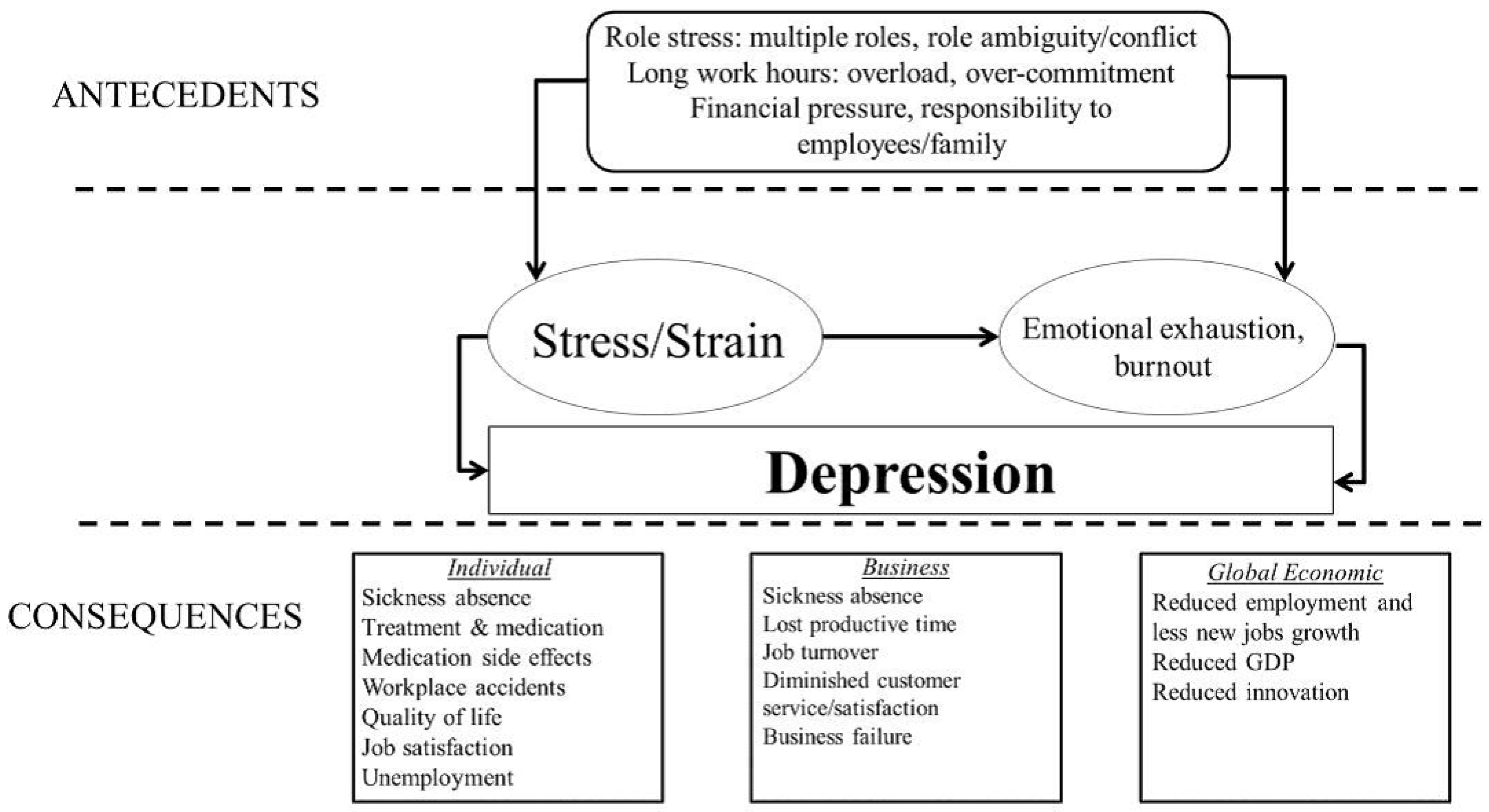
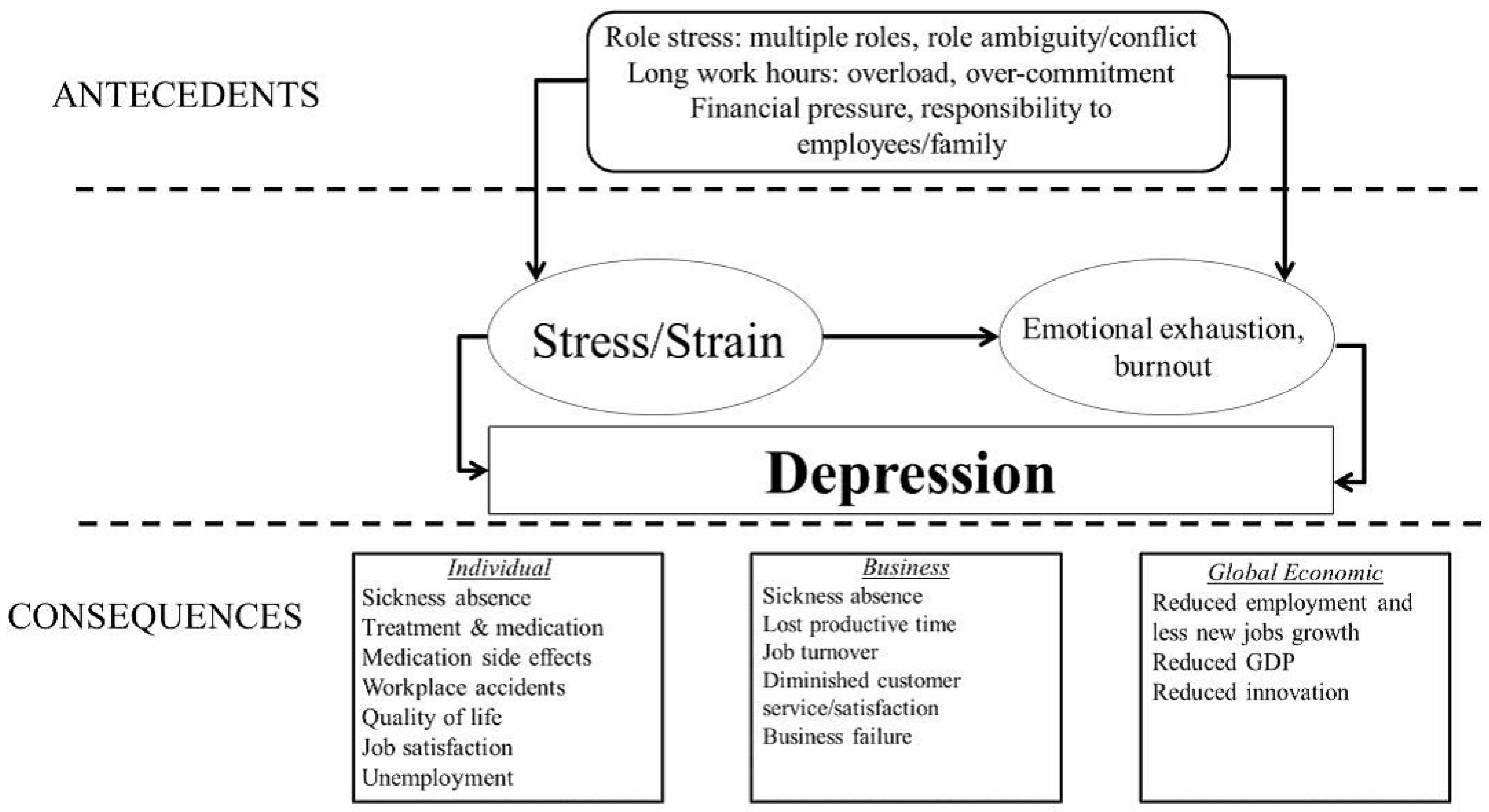
1.2. Theoretical Approach
2. Experimental Section
2.1. Participants, Sampling and Recruitment Procedures

{kind=link}
{kind=link}
| Sample Characteristics | Business in Mind | Australian Bureau of Statistics |
|---|---|---|
| Age | 33.2%—40–49 years | 28.2%—45–54 years |
| 25.8%—50–59 years | 26.8%—35–44 years | |
| 23.9%—30–39 years | 14.3%—55–59 years | |
| 9.2%—18–29 years | 12.1%—25–34 years | |
| 7.8%—60–69 years | <10%—65 and over | |
| <10%—25 and under | ||
| Gender | 56.7%—female | 31.5%—female |
| Industry | 29.5%—other | 83.1%—service |
| 20.3%—service | 10.2%—agriculture, forestry, fishing | |
| 14.3%—health | 4.1%—manufacturing | |
| 6.0%—building & construction | 0.4%—mining | |
| 7.8%—retail | ||
| 3.7%—innovation, science, tech. | ||
| 4.2%—finance | ||
| 3.7%—manufacturing | ||
| 3.7%—transport | ||
| 1.4%—agriculture | ||
| 2.8%—tourism | ||
| 2.3%—wholesale | ||
| 0.3%—mining |
2.2. Measures
2.2.1. Kessler (K10) Screening Scale for Psychological Distress
2.2.2. Absenteeism and Presenteeism Days and Related Lost Productive Time
2.2.3. Socio-Demographic Factors
2.2.4. Individual Characteristics
2.2.5. Business Characteristics
2.2.6. Work-Related Wellbeing Factors
2.2.7. Health-Related Factors
2.3. Statistical Methods
3. Results and Discussion
| All Owner/Managers (N = 217) | Owner/Managers with Low/Moderate Psychological Distress (N = 137) | Owner/Managers with High/Very High Psychological Distress (N = 80) | |||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | p | |
| Absenteeism | |||||||
| Yes | 58 | 26.7 | 27 | 19.7 | 31 | 38.8 | 0.002 |
| No | 159 | 73.3 | 110 | 80.3 | 49 | 61.2 | |
| Presenteeism | |||||||
| Yes | 144 | 66.4 | 78 | 56.9 | 66 | 82.5 | 0.0001 |
| No | 73 | 33.6 | 59 | 43.1 | 14 | 17.5 | |
| Mean | S.D. | ||||||
| Absenteeism Days | 1.3 | 0.4 | 0.4 | 0.1 | 2.8 | 1.1 | 0.004 |
| Presenteeism Days | 6.2 | 0.5 | 3.2 | 0.5 | 11.2 | 1.0 | <0.00001 |

3.1. Psychological Distress
3.1.1. Past Month Sickness Absenteeism and Presenteeism by Psychological Distress
3.1.2. Total Absenteeism and Presenteeism by Psychological Distress
| Variable | Total Absenteeism Days | Total Presenteeism Days |
|---|---|---|
| β | β | |
| Age | −0.09 | −0.07 |
| Gender | 0.99 * | 0.26 |
| Education | 1.29 ** | 0.27 |
| Employees supervised | 0.03 | −0.12 |
| Firm size | 0.20 | −0.11 |
| Work hours | −0.13 | −0.35 |
| Treatment | 1.42 *** | 0.57 ** |
| Self-rated health | 0.29 | 0.77 ** |
| Business confidence | 0.03 | −0.09 |
| Job tension | −1.01 * | 0.35 |
| Job satisfaction | −1.81 ** | −0.46 |
| Work/life balance | 0.86 | −0.23 |
| Conscientiousness | −0.73 | −0.23 |
| Neuroticism | 1.54 *** | 0.14 |
3.1.3. Correlates of Absenteeism and Presenteeism
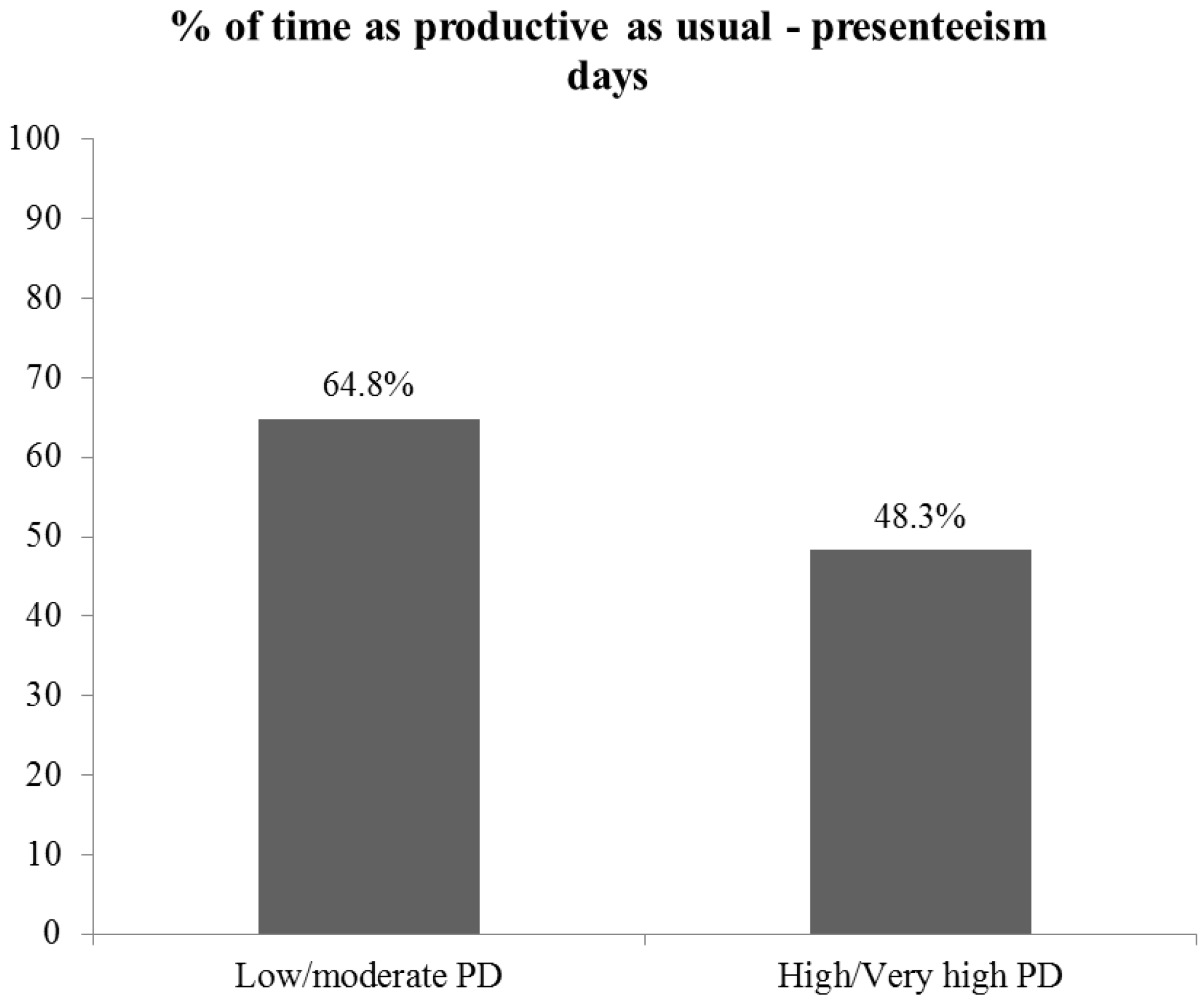
3.1.4. Inefficiency due to Presenteeism by Psychological Distress
3.2. Discussion
3.2.1. Limitations
3.2.2. Strengths
4. Conclusions
Acknowledgments
Conflicts of Interest
References
- Andrews, G.; Slade, T. Interpreting scores on the kessler psychological distress scale (k10). Aust. N. Z. J. Publ. Health 2001, 25, 494–497. [Google Scholar] [CrossRef]
- Oakley-Browne, M.A.; Wells, J.E.; Scott, K.M.; McGee, M.A. The kessler psychological distress scale in Te Rau Hinengaro: The New Zealand mental health survey. Aust. N. Z. J. Psychiat. 2010, 44, 314–322. [Google Scholar] [CrossRef]
- Kessler, R.C.; Akiskal, H.S.; Ames, M.; Birnbaum, H.; Greenberg, P.; Hirschfield, R.M.A.; Jin, R.; Merikangas, K.R.; Simon, G.E.; Wang, P.S. Prevalence and effects of mood disorders on work performance in a nationally representative sample of U.S. Workers. Amer. J. Psychiat. 2006, 163, 1561–1568. [Google Scholar] [CrossRef]
- Goetzel, R.Z.; Long, S.R.; Ozminkowski, R.J.; Hawkins, K.; Wang, S.; Lynch, W. Health, absence, disability, and presenteeism cost estimates of certain physical and mental health conditions. J. Occup. Environ. Med. 2004, 46, 398–412. [Google Scholar] [CrossRef]
- Lerner, D.; Adler, D.A.; Chang, H.; Lapitsky, L.; Hood, M.Y.; Perissinotto, C.; Reed, J.; McLaughlin, T.J.; Berndt, E.R.; Rogers, W.H. Unemployment, job retention, and productivity loss among employees with depression. Psychiatr. Services 2004, 55, 1371–1378. [Google Scholar]
- Stewart, W.F.; Ricci, J.A.; Chee, E.; Hahn, S.R.; Morganstein, D. Cost of lost productive work time among us workers with depression. JAMA 2003, 289, 3135–3144. [Google Scholar] [CrossRef]
- Sanderson, K.; Tilse, E.; Nicholson, J.; Oldenburg, B.; Graves, N. Which presenteeism measures are more sensitive to depression and anxiety? J. Affect. Disorders 2007, 101, 65–74. [Google Scholar] [CrossRef]
- Bender, A.; Farvolden, P. Depression and the workplace: A progress report. Curr. Psychiat. Rep. 2008, 10, 73–79. [Google Scholar] [CrossRef]
- LaMontagne, A.; Sanderson, K.; Cocker, F. Estimating the Economic Benefits of Eliminating Job Strain as a Risk Factor for Depression; Victorian Health Promotion Foundation (VicHealth): Melbourne, Australia, 2010. [Google Scholar]
- Bureau of Labor Statistics. Occupational Employment and Wages; U.S. Bureau of Labor Statistics: Washington, DC, USA, 2009.
- Department of Business Innovation and Skills. Small and Medium-sized Enterprise (SME) Statistics for the UK and Regions 2009; Government of the United Kingdom: London, UK, 2010.
- Shepherd, C.D. Entrepreneurial burnout: Exploring antecedents, dimensions and outcomes. J. Res. Mark. Entrep. 2010, 12, 71–79. [Google Scholar]
- Caspi, A.; Sugden, K.; Moffitt, T.E.; Taylor, A.; Craig, I.W.; Harrington, H.; McClay, J.; Mill, J.; Martin, J.; Braithwaite, A.; et al. Influence of life stress on depression: Moderation by a polymorphism in the 5-HTT gene. Science 2003, 301, 386–389. [Google Scholar] [CrossRef]
- Melchior, M.; Caspi, A.; Milne, B.J.; Danese, A.; Poulton, R.; Moffitt, T.E. Work stress precipitates depression and anxiety in young, working women and men. Psychol. Med. 2007, 37, 1119–1129. [Google Scholar] [CrossRef]
- LaMontagne, A.; Keegel, T.; Louie, A.M.; Ostry, A. Job stress as a preventable upstream determinant of common mental disorders: A review for practitioners and policy-makers. Adv. Ment. Health 2010, 9, 17–35. [Google Scholar] [CrossRef]
- Nestler, E.J.; Gould, E.; Manji, H. Preclinical models: Status of basic research in depression. Biol. Psychiat. 2002, 52, 503–528. [Google Scholar] [CrossRef]
- Stansfeld, S.; Fuhrer, R.; Shipley, M.; Marmot, M. Work characteristics predict psychiatric disorder: Prospective results from the whitehall II study. Occup. Environ. Med. 1999, 56, 302–307. [Google Scholar] [CrossRef]
- Heywood, J.S.; Jirjahn, U. Teams, teamwork and absence. Scand. J. Econ. 2004, 106, 765–782. [Google Scholar] [CrossRef]
- Barmby, T.; Stephan, G. Worker absenteeism: Why firm size may matter. Manch. Sch. 2000, 68, 568–577. [Google Scholar]
- Boon, M. Determinants of Days Lost From Work due to Illness: A Micro-Analysis on Firm-Level Data; Netherlands Official Statistics: Den Haag, The Netherlands, 2000; pp. 17–22. [Google Scholar]
- de Kok, J.M.P. Precautionary actions within small and medium-sized enterprises. J. Small Bus. Management 2005, 43, 498–535. [Google Scholar]
- Benavides, F.G.; Benach, J.; Diez-Roux, A.V.; Roman, C. How do types of employment relate to health indicators? Findings from the second european survey on working conditions. J. Epidemiol. Community Health 2000, 54, 494–501. [Google Scholar] [CrossRef]
- Dionne, G.; Dostie, B. Evidence of the determinants of absenteeism using linked employer-employee data. Ind. Labor Relat. Rev. 2007, 61, 108–120. [Google Scholar]
- Etzion, D. Moderating effect of social support on the stress burnout relationship. J. Appl. Psychol. 1984, 69, 615–622. [Google Scholar] [CrossRef]
- Koopmans, P.; Roelen, C.; Groothoff, J. Sickness absence due to depressive symptoms. Int. Arch. Occup. Environ. Health 2008, 81, 711–719. [Google Scholar] [CrossRef]
- Rodwell, J.J.; Noblet, A.J.; Allisey, A.F. Improving employee outcomes in the public sector: The beneficial effects of social support at work and job control. Pers. Rev. 2011, 40, 383–397. [Google Scholar] [CrossRef]
- Vistness, J.P. Gender differences in days lost from work due to illness. Ind. Labor Relat. Rev. 1997, 50, 304–323. [Google Scholar]
- Pauly, M.; Nicholson, S.; Polsky, D.; Berger, M.L.; Sharda, C. Valuing reductions in on-the-job illness: ‘Presenteeism’ from managerial and economic perspectives. Health Economics 2008, 17, 469–485. [Google Scholar] [CrossRef]
- Pauly, M.V.; Nicholson, S.; Xu, J.; Polsky, D.; Danzon, P.M.; Murray, J.F.; Berger, M.L. A general model of the impact of absenteeism on employers and employees. Health Economics 2002, 11, 221–231. [Google Scholar] [CrossRef]
- Cocker, F.; Martin, A.; Scott, J.; Venn, A.; Sanderson, K. Psychological distress and related work attendance among small-to-medium enterprise owner/managers: Literature review and research agenda. Int. J. Ment. Health Promot. 2013, 14, 1–18. [Google Scholar]
- Johns, G. Attendance dynamics at work: The antecedents and correlates of presenteeism, absenteeism, and productivity loss. J. Occup. Health Psychol. 2011, 16, 483–500. [Google Scholar] [CrossRef]
- Aronsson, G.; Gustafsson, K. Sickness presenteeism: Prevalence, attendance-pressure factors, and an outline of a model for research. J. Occup. Environ. Med. 2005, 47, 958–966. [Google Scholar] [CrossRef]
- Hansen, C.D.; Andersen, J.H. Going ill to work: What personal circumstances, attitudes and work-related factors are associated with sickness presenteeism? Soc. Sci. Med. 2008, 67, 956–965. [Google Scholar] [CrossRef]
- Johns, G. Presenteeism in the workplace: A review and research agenda. J. Organ. Behav. 2009, 31, 519–542. [Google Scholar] [CrossRef]
- Carland, J.W.; Hoy, F.; Boulton, W.R.; Carland, J.A.C. Differentiating entrepreneurs from small business owners: A conceptualisation. Acad. Manage. Rev. 1984, 9, 354–359. [Google Scholar]
- Wagener, S.; Gorgievski, M.; Rijsdijk, S.A. Businessman or host? Individual differences between entrepreneurs and small business owners in the hospitality industry. Serv. Ind.J. 2010, 30, 1513–1527. [Google Scholar] [CrossRef]
- Stewart, W.H.; Watson, W.E.; Carland, J.C.; Carland, J.W. A proclivity for entrepreneurship: A comparison of entrepreneurs, small business owners, and corporate managers. J. Bus. Venturing 1999, 14, 189–214. [Google Scholar] [CrossRef]
- Sunderland, M.; Slade, T.; Stewart, G.; Andrews, G. Estimating the prevalence of DSM-IV mental illness in the australian general population using the kessler psychological distress scale. Aust. N. Z. J. Psychiat. 2011, 45, 880–889. [Google Scholar] [CrossRef]
- Phongsavan, P.; Chey, T.; Bauman, A.; Brooks, R.; Silove, D. Social capital, socio-economic status and psychological distress among australian adults. Soc. Sci. Med. 2006, 63, 2546–2561. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.T.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kessler, R.C.; Slade, T.; Andrews, F. The performance of the k6 and k10 screening scales for psychological distress in the australian national survey of mental health and wellbeing. Psychol. Med. 2003, 33, 357–362. [Google Scholar] [CrossRef]
- Kessler, R.C.; Ames, M.; Hymel, P.A.; Loeppke, R.; McKenas, D.; Richling, D.E.; Stang, P.; Ustun, T.B. Using the world health organisation health and work performance questionnaire (HPQ) to evaluate the indirect workplace cost of illness. J. Occup. Environ. Med. 2004, 46, S23–S37. [Google Scholar] [CrossRef]
- Kessler, R.C.; Barber, C.; Beck, A.; Berglund, P.A.; Cleary, P.D.; McKenas, D.; Pronk, N.; Simon, G.; Stang, P.; Ustun, T.B.; et al. The world health organisation health and work performance questionnaire (hpq). J. Occup. Environ. Med. 2003, 45, 156–174. [Google Scholar] [CrossRef]
- Wang, P.S.; Beck, A.; Berglund, P.A.; Leutzinger, J.A.; Pronk, N.; Richling, D.E.; Schenk, T.W.; Simon, G.; Stang, P.; Ustun, T.B.; et al. Chronic medical conditions and work performance in the health and work performance questionnaire calibration surveys. J. Occup. Environ. Med. 2003, 45, 1303–1311. [Google Scholar] [CrossRef]
- Hilton, M.F.; Sheridan, J.S.; Cleary, C.M.; Whiteford, H. Employee absenteeism measures reflecting current work practices may be instrumental in a re-evaluation of the relationship between psychological distress/mental health and absenteeism. Int. J. Meth. Psychiatr. Res. 2009, 18, 37–47. [Google Scholar] [CrossRef]
- Aronsson, G.; Gustafsson, K.; Dallner, M. Sick but yet at work. An empirical study of sickness presenteeism. J. Epidemiol. Community Health 2000, 54, 502–509. [Google Scholar] [CrossRef]
- Koopman, C.; Pelletier, K.R.; Murray, J.F.; Sharda, C.E.; Berger, M.L.; Turpin, R.S.; Hackleman, P.; Gibson, P.; Holmes, D.M.; Bendel, T. Stanford presenteeism scale: Health status and employee productivity. J. Occup. Environ. Med. 2002, 44, 14–20. [Google Scholar] [CrossRef]
- Brouwer, W.B.F.; Koopmanschap, M.A.; Rutten, F.F.H. Productivity losses without absence: Measurement validation and empirical evidence. Health Policy 1999, 48, 13–27. [Google Scholar]
- McCrae, R.R.; Kurtz, J.E.; Yamagata, S.; Terracciano, A. Internal consistency, retest reliability, and their implications for personality scale validity. Pers. Soc. Psychol. Rev. 2011, 15, 28–50. [Google Scholar]
- Bockerman, P.; Laukkanen, E. Presenteeism in finland: Determinants by gender and the sector of economy. Ege Acad. Rev. 2009, 9, 1007–1016. [Google Scholar]
- Cocker, F.; Martin, A.; Scott, J.; Venn, A.; Otahal, P.; Sanderson, K. Factors associated with presenteeism among employed australian adults reporting lifetime major depression with 12-month symptoms. J. Affect. Disorders 2011, 135, 231–240. [Google Scholar] [CrossRef]
- Conte, J.M.; Jacobs, R.R. Validity evidence linking polychronicity and big five personality dimensions to absence, lateness, and supervisory performance ratings. Hum. Perform. 2003, 16, 107–129. [Google Scholar] [CrossRef]
- Iverson, R.D.; Deery, S.J. Understanding the “personological” basis of employee withdrawal: The influence of affective disposition on employee tardiness, early departure, and absenteeism. J. Appl. Psychol. 2001, 86, 856–866. [Google Scholar] [CrossRef]
- Hattrup, K.; O’Connell, M.S.; Wingate, P.H. Prediction of multidimensional criteria: Distinguishing task and contextual performance. Hum. Perform. 1998, 11, 305–319. [Google Scholar] [CrossRef]
- Judge, T.A.; Heller, D.; Mount, M.K. Five-factor model of personality and job satisfaction: A meta-analysis. J. Appl. Psychol. 2002, 87, 530–541. [Google Scholar] [CrossRef]
- Zhao, H.; Seibert, S.E. The big five personality dimensions and entrepreneurial status: A meta-analytical review. J. Appl. Psychol. 2006, 91, 259–271. [Google Scholar] [CrossRef]
- Rauch, A.; Frese, M. Let’s put the person back into entrepreneurship research: A meta-analysis on the relationship between business owners’ personality traits, business creation, and success. Eur. J. Work Organ. Psychol. 2007, 16, 353–385. [Google Scholar] [CrossRef]
- Costa, P.T. Work and personality: Use of the NEO-PI-R in industrial/organisational psychology. Appl. Psychol. 1996, 45, 225–241. [Google Scholar] [CrossRef]
- Blanch, A.; Aluja, A.; Gallart, S.; Dolcet, J.M. A review on the use of neo-pi-r validity scales in normative, job selection, and clinical samples. Eur. J. Psychiat. 2009, 23, 121–129. [Google Scholar]
- Nicholson, S.; Pauly, M.V.; Polsky, D.; Sharda, C.; Szrek, H.; Berger, M.L. Measuring the effects of work loss on productivity with team production. Health Economics 2006, 15, 111–123. [Google Scholar] [CrossRef]
- Ahola, K.; Kivimaki, M.; Honkonen, T.; Virtanen, M.; Koskinen, S.; Vahtera, J.; Lonnqvist, J. Occupational burnout and medically certified sickness absence: A population-based study of finnish employees. J. Psychosom. Res. 2008, 64, 185–193. [Google Scholar]
- Rantanen, I.; Tuominen, R. Relative magnitude of presenteeism and absenteeism and work-related factors affecting them among health care professionals. Int. Arch. Occup. Envir. Health 2011, 84, 225–230. [Google Scholar] [CrossRef]
- Musich, S.; Hook, D.; Baaner, S.; Spooner, M.; Edington, D.W. The association of corporate work environment factors, health risks, and medical conditions with presenteeism among australian employees. Amer. J. Health Promotion 2006, 21, 127–136. [Google Scholar] [CrossRef]
- Beutell, N. Self-employment, work-family conflict and work-family synergy: Antecedents and consequences. J. Small Bus. Entrep. 2007, 20, 325–334. [Google Scholar] [CrossRef]
- Cegarra-Leiva, D.; Sanchez-Vidal, M.E.; Cegarra-Navarro, J.G. Work life balance and the retention of managers in spanish smes. Int. J. Hum. Res. Manag. 2012, 23, 91–108. [Google Scholar] [CrossRef]
- Jamal, M. Job stress, satisfaction, and mental health: An empirical examination of self-employed and non-self-employed canadians. J. Small Bus. Manag. 1997, 35, 48–57. [Google Scholar]
- Jamal, M. Self-employment and quality of work and nonwork life: A study in cross-cultural management. J. Small Bus. Entrepr. 2009, 22. [Google Scholar] [CrossRef]
- Caverley, N.; Cunningham, J.B.; MacGregor, J.N. Sickness presenteeism, sickness absenteeism, and health following restructuring in a public service organisation. J. Manage. Stud-Oxford. 2007, 44, 304–319. [Google Scholar] [CrossRef]
- Warr, P.; Cook, J.; Wall, T. Scales of the measurement of some work attitudes and aspects of psycholofical wellbeing. J. Occup. Psychol. 1979, 52, 129–148. [Google Scholar] [CrossRef]
- House, R.; Rizzo, J. Role conflict and ambiguity as critical variables in a model of organisational behaviour. Organ. Behav. Hum. Perform. 1972, 7, 467–505. [Google Scholar] [CrossRef]
- Kalliath, T.; Brough, P. Work-life balance: A review of the meaning of the balance construct. J. Manag. Organ. 2008, 14, 323–327. [Google Scholar] [CrossRef]
- Ware, J.; Kosinski, M.; Keller, S. A 12-item short form health survey (SF-12). Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- Haddock, C.K.; Poston, W.S.C.; Pyle, S.A.; Klesges, R.C.; van der Weg, M.W.; Peterson, A.; Debon, M. The validity of self-rated health as a measure of health status among young military personnel: Evidence from a cross-sectional survey. Health Qual. Life Outcomes 2006, 4. [Google Scholar] [CrossRef]
- Krause, N.; Jay, G. What do global self-rated health items measure? Med. Care 1994, 32, 930–942. [Google Scholar] [CrossRef]
- de Salvo, K.B.; Fisher, W.P.; Tran, K.; Bloser, N.; Merrill, W.; Peabody, J. Assessing measurement properties of two single-item general health measures. Qual. Life Res. 2006, 15, 191–201. [Google Scholar] [CrossRef]
- Bockerman, P.; Laukkanen, E. Predictors of sickness absence and presenteeism: Does the pattern differ by a respondents health? J. Occup. Environ. Med. 2010, 52, 332–335. [Google Scholar] [CrossRef]
- Smulders, P.G.W.; Nijhuis, F.J.N. The job demands-job control model and absence behaviour: Results of a 3-year longitudinal study. Work Stress 1999, 13, 115–131. [Google Scholar] [CrossRef]
- Labriola, M.; Christensen, K.B.; Lund, T.; Nielsen, M.; Lindhardt, M.; Diderichsen, F. Multilevel analysis of workplace and individual risk factors for long-term sickness absence. J. Occup. Environ. Med. 2006, 48, 923–929. [Google Scholar] [CrossRef]
- Siegrist, J. Adverse health effects of high-effort/low reward conditions. J. Occup. Health Psychol. 1996, 1, 27–41. [Google Scholar] [CrossRef]
- Burgess, P.M.; Pirkis, J.E.; Slade, T.N.; Johnston, A.K.; Meadows, G.N.; Gunn, J.M. Service use for mental health problems: Findings from the 2007 national survey of mental health and wellbeing. Aust.N.Z.J. Psychiat. 2009, 43, 615–623. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Jorm, A.F.; Korten, A.E.; Jacomb, P.A.; Christensen, H.; Rodgers, B.; Pollitt, P. “Mental health literacy”: A survey of the public’s ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Med. J. Australia 1997, 166, 182–186. [Google Scholar]
- Martin, A. Individual and contextual correlates of managers’ attitudes toward depressed employees. Hum. Resour. Manage. 2010, 49, 647–668. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Cocker, F.; Martin, A.; Scott, J.; Venn, A.; Sanderson, K. Psychological Distress, Related Work Attendance, and Productivity Loss in Small-to-Medium Enterprise Owner/Managers. Int. J. Environ. Res. Public Health 2013, 10, 5062-5082. https://doi.org/10.3390/ijerph10105062
Cocker F, Martin A, Scott J, Venn A, Sanderson K. Psychological Distress, Related Work Attendance, and Productivity Loss in Small-to-Medium Enterprise Owner/Managers. International Journal of Environmental Research and Public Health. 2013; 10(10):5062-5082. https://doi.org/10.3390/ijerph10105062
Chicago/Turabian StyleCocker, Fiona, Angela Martin, Jenn Scott, Alison Venn, and Kristy Sanderson. 2013. "Psychological Distress, Related Work Attendance, and Productivity Loss in Small-to-Medium Enterprise Owner/Managers" International Journal of Environmental Research and Public Health 10, no. 10: 5062-5082. https://doi.org/10.3390/ijerph10105062