Effect of Thirst-Driven Fluid Intake on 1 H Cycling Time-Trial Performance in Trained Endurance Athletes

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Preliminary Testing and Pre-Experimental Procedures
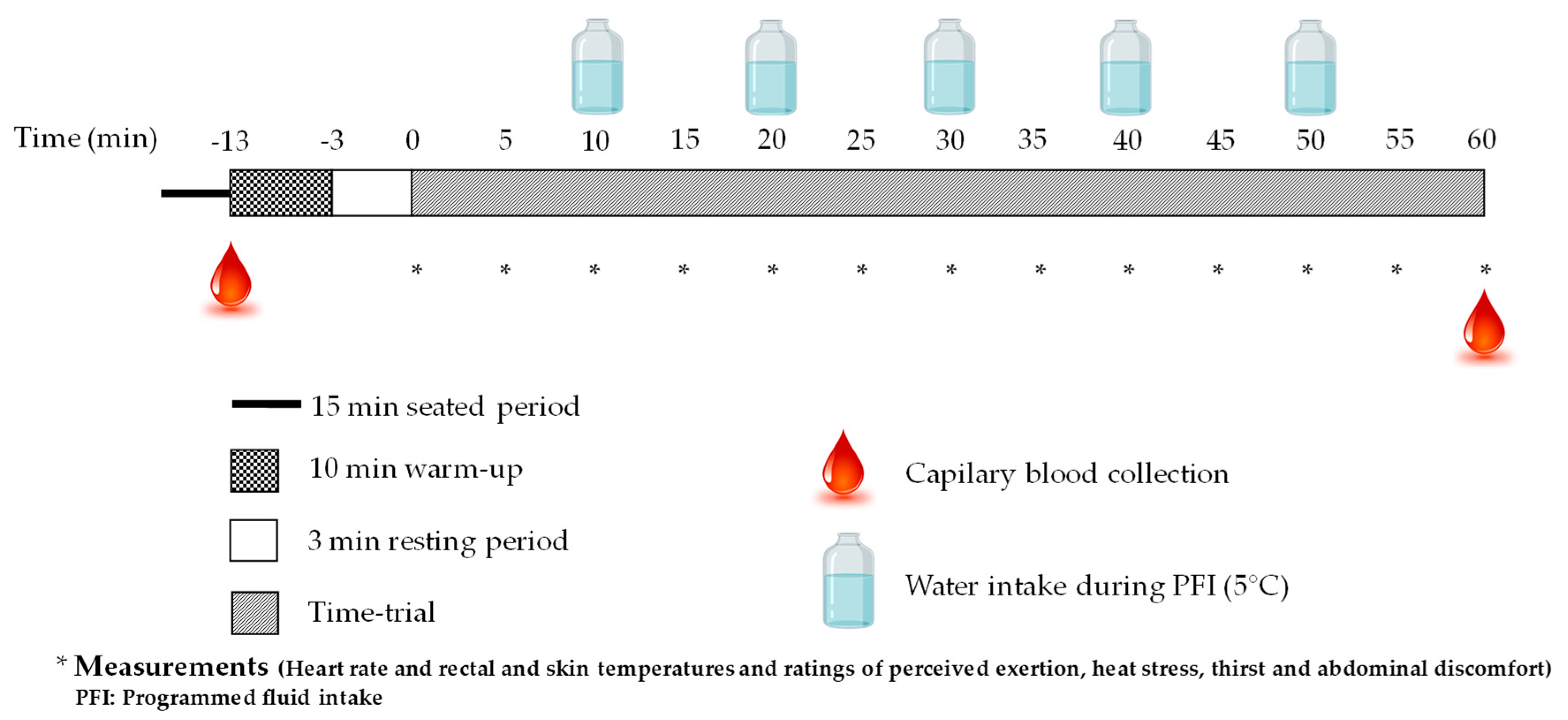
2.3. Experimental Protocol
2.4. Measurements
2.4.1. Heart rate, Rectal, Skin and Mean Skin Temperatures
2.4.2. Hemoglobin, Hematocrit and Changes in Plasma Volume and Sodium
2.4.3. Sweat Loss, Body Mass Loss, Rate of % Body Mass Loss and Urine Specific Gravity
2.5. Statistical Analyses
3. Results
3.1. Participants and Laboratory Temperature and Relative Humidity
3.2. Hydration State of Participants Prior to the Time-Trials
3.3. Fluid Balance
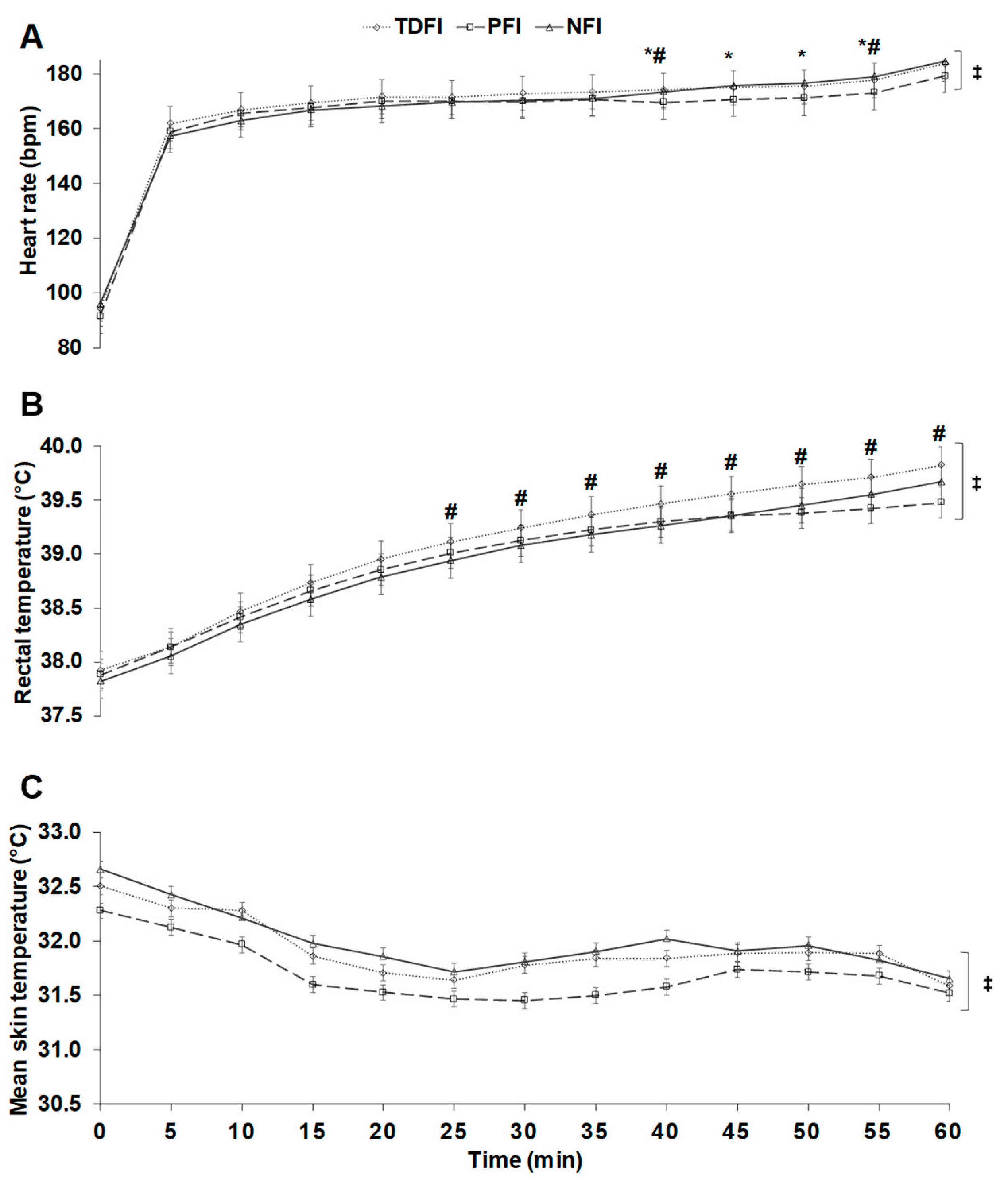
3.4. Physiological Responses during the Time-Trials
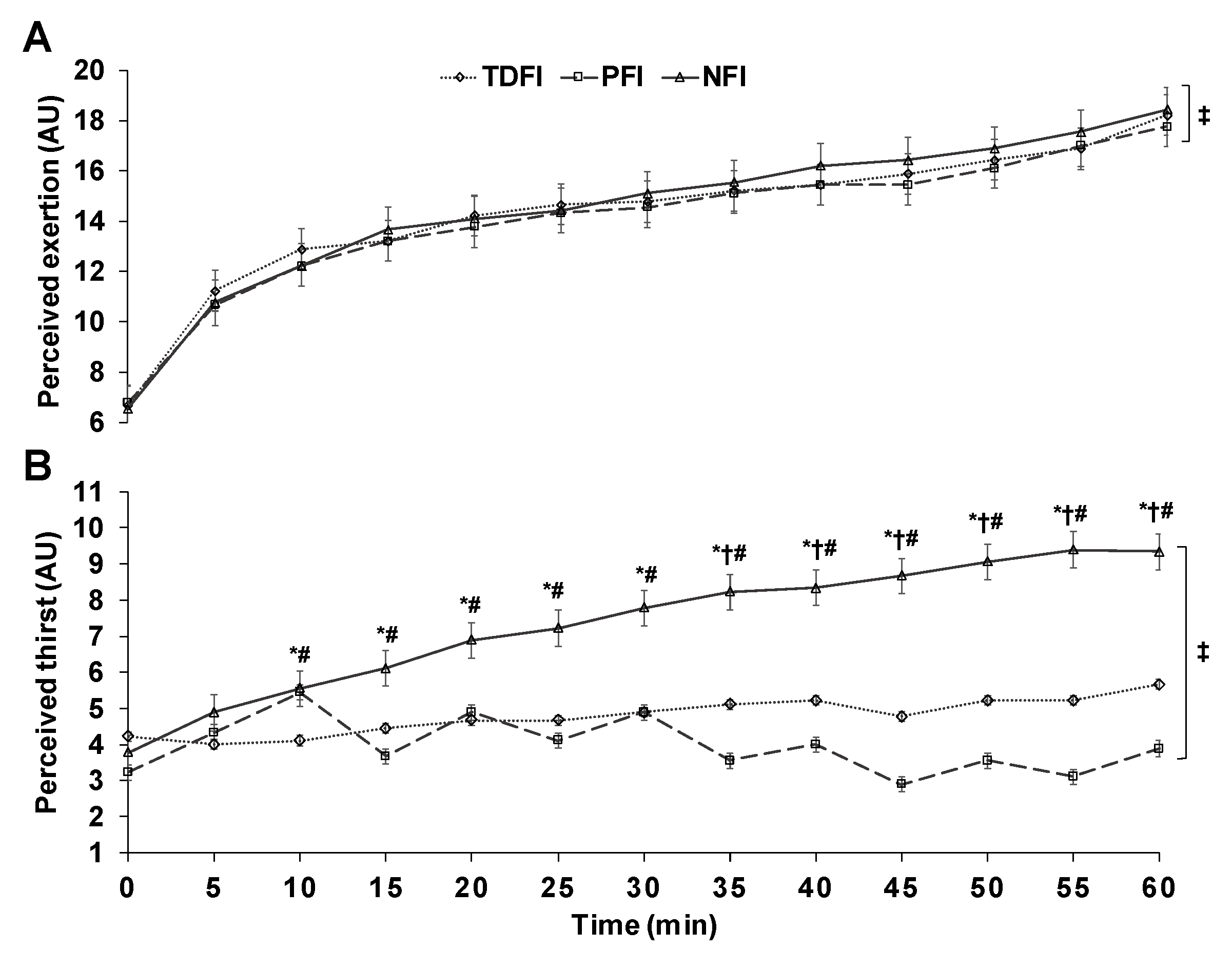
3.5. Perceptual Responses during the Time-Trials
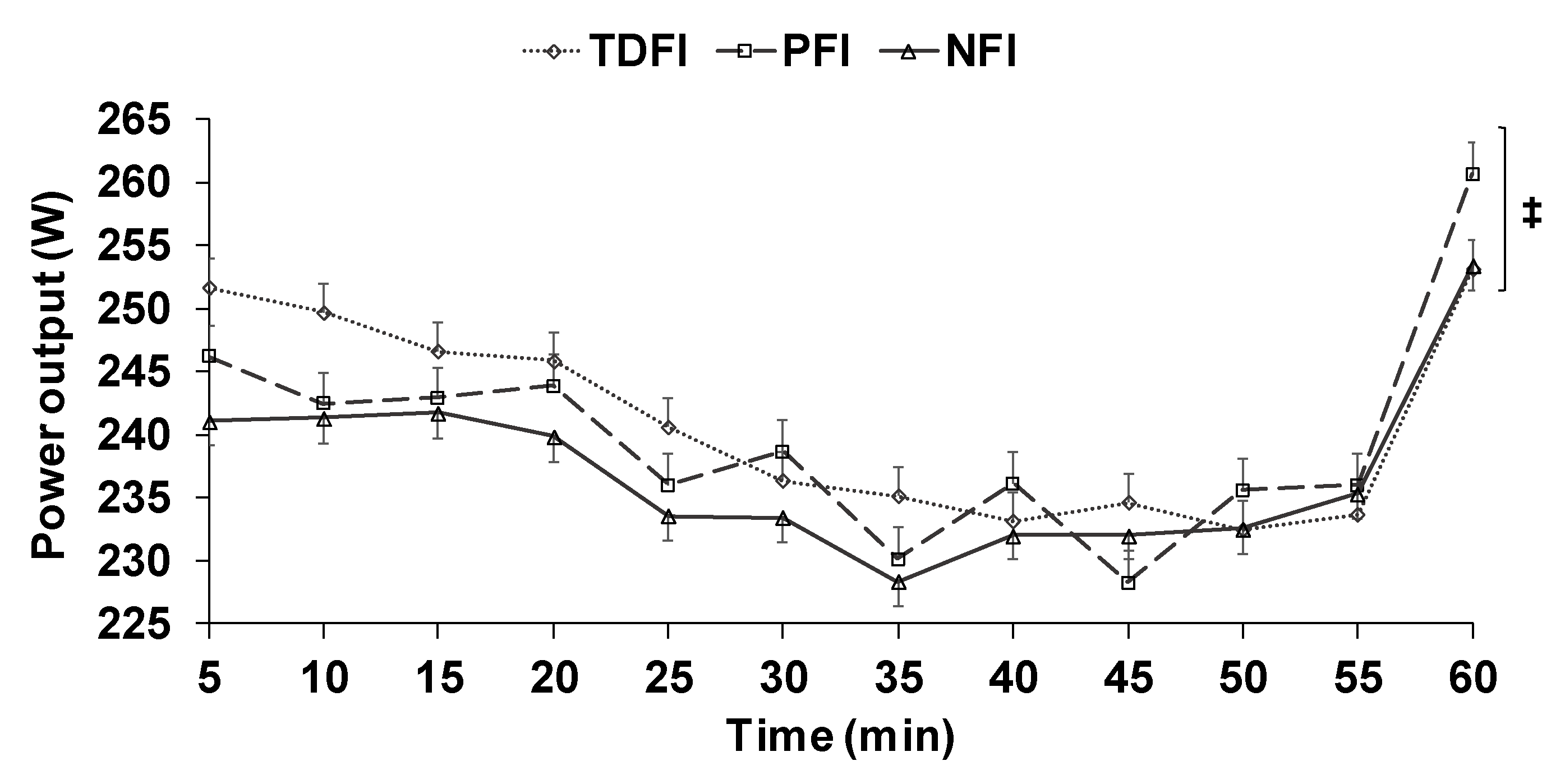
3.6. Time-Trial Performance
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cheuvront, S.N.; Kenefick, R.W.; Montain, S.J.; Sawka, M.N. Mechanisms of aerobic performance impairment with heat stress and dehydration. J. Appl. Physiol. 2010, 109, 1989–1995. [Google Scholar] [CrossRef] [Green Version]
- Montain, S.J.; Coyle, E.F. Fluid ingestion during exercise increases skin blood flow independent of increases in blood volume. J. Appl. Physiol. 1992, 73, 903–910. [Google Scholar] [CrossRef]
- Bachle, L.; Eckerson, J.; Albertson, L.; Ebersole, K.; Goodwin, T.; Petzel, D. The effect of fluid replacement on endurance performance. J. Strength Cond. Res./Natl. Strength Cond. Assoc. 2001, 15, 217–224. [Google Scholar]
- Backx, K.; van Someren, K.A.; Palmer, G.S. One hour cycling performance is not affected by ingested fluid volume. Int. J. Sport Nutr. Exerc. Metab. 2003, 13, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Kay, D.; Marino, F.E. Failure of fluid ingestion to improve self-paced exercise performance in moderate-to-warm humid environments. J. Biol. 2003, 28, 29–34. [Google Scholar] [CrossRef]
- McConell, G.K.; Stephens, T.J.; Canny, B.J. Fluid ingestion does not influence intense 1-h exercise performance in a mild environment. Med. Sci. Sports Exerc. 1999, 31, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.A.; Hawley, J.A.; Palmer, G.S.; Wilson, G.R.; Gray, D.A.; Noakes, T.D.; Dennis, S.C. Water ingestion does not improve 1-h cycling performance in moderate ambient temperatures. Eur. J. Appl. Physiol. Occup. Physiol. 1995, 71, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Below, P.R.; Mora-Rodriguez, R.; Gonzalez-Alonso, J.; Coyle, E.F. Fluid and carbohydrate ingestion independently improve performance during 1 h of intense exercise. Med. Sci. Sports Exerc. 1995, 27, 200–210. [Google Scholar] [CrossRef]
- Holland, J.J.; Skinner, T.L.; Irwin, C.G.; Leveritt, M.D.; Goulet, E.D.B. The influence of drinking fluid on endurance cycling performance: A meta-analysis. Sports Med. (Auckl. N. Z.) 2017, 47, 2269–2284. [Google Scholar] [CrossRef]
- Savoie, F.A.; Dion, T.; Asselin, A.; Gariepy, C.; Boucher, P.M.; Berrigan, F.; Goulet, E.D. Intestinal temperature does not reflect rectal temperature during prolonged, intense running with cold fluid ingestion. Physiol. Meas. 2015, 36, 259–272. [Google Scholar] [CrossRef]
- Daries, H.N.; Noakes, T.D.; Dennis, S.C. Effect of fluid intake volume on 2-h running performances in a 25 degrees C environment. Med. Sci. Sports Exerc. 2000, 32, 1783–1789. [Google Scholar] [CrossRef] [PubMed]
- Dion, T.; Savoie, F.A.; Asselin, A.; Gariepy, C.; Goulet, E.D. Half-marathon running performance is not improved by a rate of fluid intake above that dictated by thirst sensation in trained distance runners. Eur. J. Appl. Physiol. 2013, 113, 3011–3020. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.B.; Voss, K.W. The influence of volume on gastric emptying and fluid balance during prolonged exercise. Med. Sci. Sports Exerc. 1991, 23, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Goulet, E.D.B.; Hoffman, M.D. Impact of Ad Libitum Versus Programmed Drinking on Endurance Performance: A Systematic Review with Meta-Analysis. Sports Med. (Auckl. N. Z.) 2019, 49, 221–232. [Google Scholar] [CrossRef]
- Noakes, T.D. Is drinking to thirst optimum? Ann. Nutr. Metab. 2010, 57 (Suppl. 2), 9–17. [Google Scholar] [CrossRef]
- Dugas, J.P.; Oosthuizen, U.; Tucker, R.; Noakes, T.D. Rates of fluid ingestion alter pacing but not thermoregulatory responses during prolonged exercise in hot and humid conditions with appropriate convective cooling. Eur. J. Appl. Physiol. 2009, 105, 69–80. [Google Scholar] [CrossRef]
- Mundel, T.; King, J.; Collacott, E.; Jones, D.A. Drink temperature influences fluid intake and endurance capacity in men during exercise in a hot, dry environment. Exp. Physiol. 2006, 91, 925–933. [Google Scholar] [CrossRef]
- Lee, J.K.; Shirreffs, S.M.; Maughan, R.J. Cold drink ingestion improves exercise endurance capacity in the heat. Med. Sci. Sports Exerc. 2008, 40, 1637–1644. [Google Scholar] [CrossRef]
- Ramanathan, N.L. A new weighting system for mean surface temperature of the body. J. Appl. Physiol. 1964, 19, 531–533. [Google Scholar] [CrossRef]
- WHO Guidelines Approved by the Guidelines Review Committee. WHO Guidelines on Drawing Blood: Best Practices in Phlebotomy; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Goulet, E.D.B.; De La Flore, A.; Savoie, F.A.; Gosselin, J. Salt + Glycerol-Induced Hyperhydration Enhances Fluid Retention More Than Salt- or Glycerol-Induced Hyperhydration. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 246–252. [Google Scholar] [CrossRef]
- Dill, D.B.; Costill, D.L. Calculation of percentage changes in volumes of blood, plasma, and red cells in dehydration. J. Appl. Physiol. 1974, 37, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Marino, F.E.; Kay, D.; Cannon, J.; Serwach, N.; Hilder, M. A reproducible and variable intensity cycling performance protocol for warm conditions. J. Sci. Med. Sport 2002, 5, 95–107. [Google Scholar] [CrossRef]
- Palmer, G.S.; Dennis, S.C.; Noakes, T.D.; Hawley, J.A. Assessment of the reproducibility of performance testing on an air-braked cycle ergometer. Int. J. Sports Med. 1996, 17, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Kruschke, J.K.; Liddell, T.M. The Bayesian New Statistics: Hypothesis testing, estimation, meta-analysis, and power analysis from a Bayesian perspective. Psychon. Bull. Rev. 2018, 25, 178–206. [Google Scholar] [CrossRef] [PubMed]
- Blume, J.D.; D’Agostino McGowan, L.; Dupont, W.D.; Greevy, R.A., Jr. Second-generation p-values: Improved rigor, reproducibility, & transparency in statistical analyses. PLoS ONE 2018, 13, e0188299. [Google Scholar] [CrossRef]
- Hopkins, W.G. How to interpret changes in an athletic performance test. Sportscience 2004, 8, 1–7. [Google Scholar]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef]
- Goulet, E.D.; Aubertin-Leheudre, M.; Plante, G.E.; Dionne, I.J. A meta-analysis of the effects of glycerol-induced hyperhydration on fluid retention and endurance performance. Int. J. Sport Nutr. Exerc. Metab. 2007, 17, 391–410. [Google Scholar] [CrossRef]
- Noakes, T.D. Fluid replacement during exercise. Exerc. Sport Sci. Rev. 1993, 21, 297–330. [Google Scholar] [CrossRef]
- Goulet, E.D. Effect of exercise-induced dehydration on endurance performance: Evaluating the impact of exercise protocols on outcomes using a meta-analytic procedure. Br. J. Sports Med. 2013, 47, 679–686. [Google Scholar] [CrossRef]
- Burke, L.M.; Wood, C.; Pyne, D.B.; Telford, D.R.; Saunders, P.U. Effect of carbohydrate intake on half-marathon performance of well-trained runners. Int. J. Sport Nutr. Exerc. Metab. 2005, 15, 573–589. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.N.; Noakes, T.D. Does dehydration impair exercise performance? Med. Sci. Sports Exerc. 2007, 39, 1209–1217. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.N.; Burke, L.M.; Eichner, E.R.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. American College of Sports Medicine position stand. Exercise and fluid replacement. Med. Sci. Sports Exerc. 2007, 39, 377–390. [Google Scholar] [CrossRef] [PubMed]
- McDermott, B.P.; Anderson, S.A.; Armstrong, L.E.; Casa, D.J.; Cheuvront, S.N.; Cooper, L.; Kenney, W.L.; O’Connor, F.G.; Roberts, W.O. National Athletic Trainers’ Association Position Statement: Fluid Replacement for the Physically Active. J. Athl. Train. 2017, 52, 877–895. [Google Scholar] [CrossRef]
- Merry, T.L.; Ainslie, P.N.; Cotter, J.D. Effects of aerobic fitness on hypohydration-induced physiological strain and exercise impairment. Acta Physiol. (Oxf. Engl.) 2010, 198, 179–190. [Google Scholar] [CrossRef]
- Periard, J.D.; Racinais, S.; Sawka, M.N. Adaptations and mechanisms of human heat acclimation: Applications for competitive athletes and sports. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. 1), 20–38. [Google Scholar] [CrossRef]
- Saunders, A.G.; Dugas, J.P.; Tucker, R.; Lambert, M.I.; Noakes, T.D. The effects of different air velocities on heat storage and body temperature in humans cycling in a hot, humid environment. Acta Physiol. Scand. 2005, 183, 241–255. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean ± SD |
|---|---|
| Age (years) | 30 ± 9 |
| Height (cm) | 175 ± 4 |
| Body mass (kg) | 71 ± 7 |
| Fat mass (%) | 11 ± 8 |
| Fat-free mass (%) | 86 ± 8 |
| Resting heart rate (beats·min−1) | 60 ± 10 |
| Maximal heart rate (beats·min−1) | 192 ± 8 |
| Peak oxygen consumption (mL·kg−1·min−1) | 59 ± 8 |
| Peak power output (W) | 391 ± 51 |
| Relative peak power output (W·kg−1) | 5.5 ± 0.7 |
| Parameters | NFI | TDFI | PFI | p |
|---|---|---|---|---|
| USG (g·mL−1) | 1.008 ± 0.007 | 1.008 ± 0.007 | 1.006 ± 0.004 | 0.97 |
| Hematocrit (%) | 46 ± 2 | 46 ± 2 | 45 ± 3 | 0.44 |
| Body mass (kg) | 72.2 ± 7.3 | 71.9 ± 7.4 | 72.1 ± 7.5 | 0.49 |
| Heart rate (beats·min−1) | 76 ± 12 | 80 ± 14 | 77 ± 18 | 0.83 |
| Parameters | NFI | TDFI | PFI |
|---|---|---|---|
| Total water consumption (mL) | 0 | 565 ± 178 * | 1606 ± 125 *# |
| Total water consumption (mL·kg−1) | 0 | 8.0 ± 2.9 * | 22.5 ± 3.3 *# |
| Total water consumption (mL·km−1) | 0 | 15.8 ± 4.9 * | 45.0 ± 3.7 *# |
| Sweat loss (mL) | 2102 ± 159 | 2118 ± 129 | 2010 ± 191 |
| Post-exercise USG (g·mL−1) | 1.010 ± 0.008 | 1.011 ± 0.007 | 1.010 ± 0.005 |
| Exercise-induced BM loss (% BM) | 2.9 ± 0.4 | 2.2 ± 0.3 * | 0.6 ± 0.2 *# |
| Rate of BM loss (% BM·min−1) | 0.049 ± 0.006 | 0.036 ± 0.005 * | 0.009 ± 0.004 *# |
| Time to reach 2% BM loss (min) | 41.4 ± 5.1 | 55.9 ± 7.0 * | 236.7 ± 80.3 *# |
| Post-exercise urine production (mL) | 199 ± 110 | 152 ± 103 | 187 ± 145 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perreault-Briere, M.; Beliveau, J.; Jeker, D.; Deshayes, T.A.; Duran, A.; Goulet, E.D.B. Effect of Thirst-Driven Fluid Intake on 1 H Cycling Time-Trial Performance in Trained Endurance Athletes. Sports 2019, 7, 223. https://doi.org/10.3390/sports7100223
Perreault-Briere M, Beliveau J, Jeker D, Deshayes TA, Duran A, Goulet EDB. Effect of Thirst-Driven Fluid Intake on 1 H Cycling Time-Trial Performance in Trained Endurance Athletes. Sports. 2019; 7(10):223. https://doi.org/10.3390/sports7100223
Chicago/Turabian StylePerreault-Briere, Maxime, Jeff Beliveau, David Jeker, Thomas A. Deshayes, Ana Duran, and Eric D. B. Goulet. 2019. "Effect of Thirst-Driven Fluid Intake on 1 H Cycling Time-Trial Performance in Trained Endurance Athletes" Sports 7, no. 10: 223. https://doi.org/10.3390/sports7100223