Gait Quality Assessment in Survivors from Severe Traumatic Brain Injury: An Instrumented Approach Based on Inertial Sensors


 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Clinical Assessment
- Dynamic gait index (DGI)—to assess a subject’s ability to modify gait in response to changing task demands. It consists of items rated from 0 to 3 (0 = severely impaired; 3 = normal performance), yielding a maximum score of 24 points. A score lower than 19 points has been associated with impairment of gait and fall risk [35,41].
- Berg balance scale (BBS)—to measure 14 different tasks related to balance and postural control. It is scored from 0 to 4, with 0 indicating that the subject is unable to perform the task and 4 that the subject fully meets the most difficult criteria required for the task [42].
- Community balance and mobility scale (CB&M)—to assess specific aspects of balance and mobility which are necessary for independent functioning within the community [43]. This scale includes several challenging tasks and it is based on 19 tests. Higher scores are indicative of better balance and mobility.
2.2.2. Motor Assessment
2.3. Equipment
2.4. Data Processing
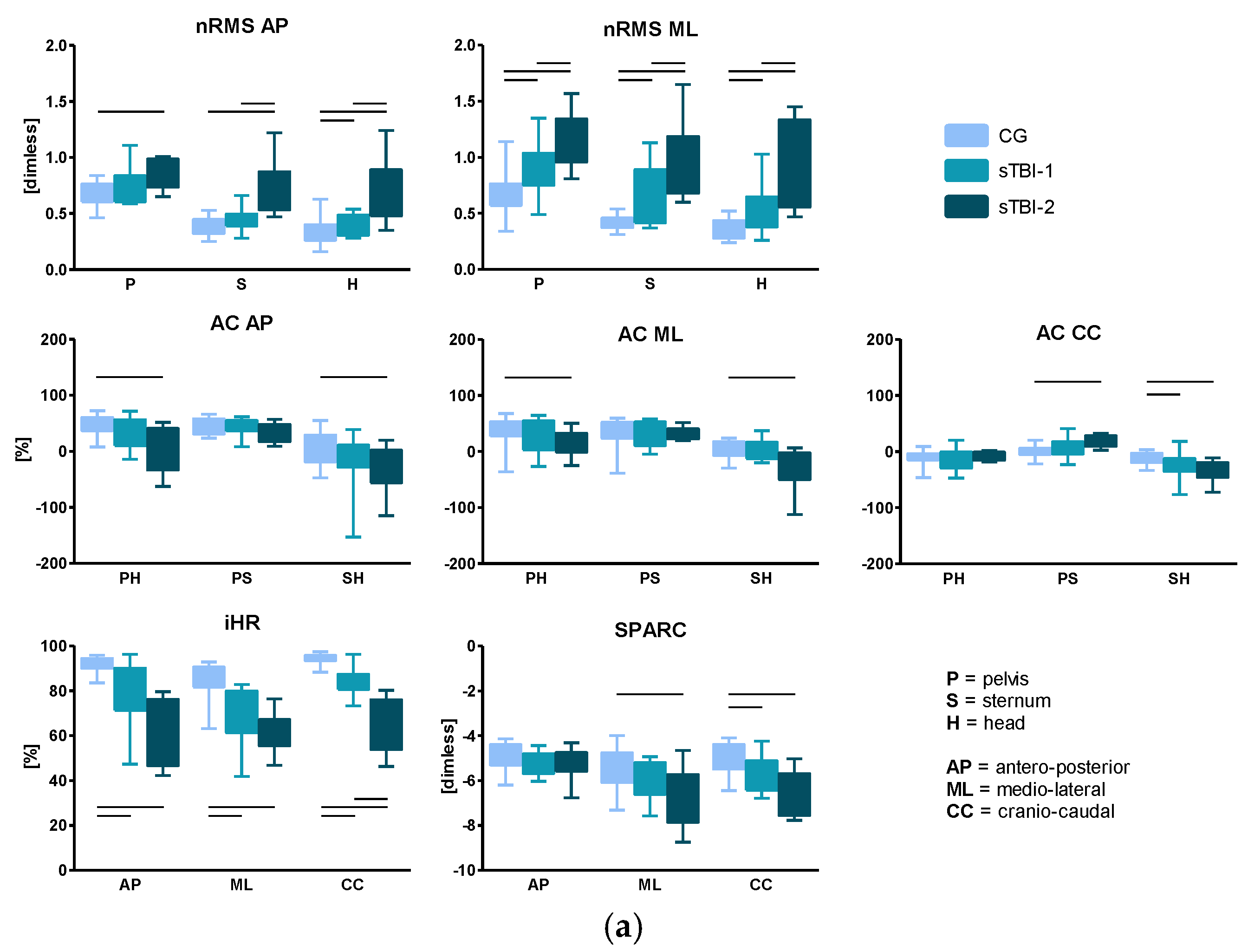
- Normalized root mean square (nRMS) values of the accelerations were calculated by dividing the RMS, AP, and ML components by the CC component, at each upper-body level (P, S, H). High RMS values have been associated with higher amount of acceleration, and hence, decreased stability, as reported in [29].
- Attenuation coefficients (AC) [50] between each level pair of the upper-body, for each acceleration component (j), defined as:Each coefficient represents the variation of the acceleration from lower to upper-body levels. A positive coefficient indicates an attenuation of the accelerations, while a negative coefficient indicates an amplification of the accelerations from the lower to the upper body level.
- Improved harmonic ratio (iHR), as proposed by [51], was calculated for each acceleration component (j) measured at the pelvis level. This index is based on a spectral analysis of the acceleration signals and is a measure of hemilateral symmetry when stepping (0% = total asymmetry; 100% = total symmetry). It was calculated as follows:
- SPectral ARC length (SPARC), as proposed by [52], calculated for each acceleration component (j) measured at the pelvis level. The calculation of SPARC was performed as follows:where is the Fourier magnitude spectrum of the acceleration signal a(t) and is the normalized magnitude spectrum.
2.5. Statistical Analysis
- Mann–Whitney U test to investigate if significant differences existed between sTBI-1 and sTBI-2 for the clinical scale scores;
- Kruskal–Wallis H-test on the estimated biomechanical parameters, to investigate if significant differences existed among the different levels of walking ability (‘‘group” factor: CG, sTBI-1, or sTBI-2);
- Spearman’s rank correlation coefficient (q) between gait quality indices and clinical scale scores, considering the whole sTBI group.
3. Results
3.1. Clinical Scale Score Results
3.2. Spatio-Temporal Parameters and Clinical FST Parameters
3.3. Root Mean Square, Attenuation Coefficients, Improved Harmonic Ratio, and SPARC
3.4. Association of the Gait Quality Indices with the Clinical Scale Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Teasdale, G.M. Head Injury. J. Neurol. 1995, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Jennett, B. Epidemiology of head injury. J. Neurol. Psychiatry 1996, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kraus, J.; Sullivan, C.; Bowers, S.; Knowlton, S.; Marshall, L. The incidence of acute brain injury and serious impairment in a defined population. Am. J. Epidemiol. 1984, 119, 186–201. [Google Scholar] [CrossRef] [PubMed]
- Popescu, C.; Anghelescu, A.; Daia, C.; Onose, G. Actual data on epidemiological evolution and prevention endeavours regarding traumatic brain injury. J. Med. Life 2015, 8, 272–277. [Google Scholar] [PubMed]
- Ponsford, J.L.; Spitz, G.; Cromarty, F.; Gifford, D.; Attwood, D. Costs of Care after Traumatic Brain Injury. J. Neurotrauma 2013, 30, 1498–1505. [Google Scholar] [CrossRef]
- Teasdale, G.; Maas, A.; Lecky, F.; Manley, G.; Stocchetti, N.; Murray, G. The Glasgow Coma Scale at 40 years: Standing the test of time. Lancet Neurol. 2014, 13, 844–854. [Google Scholar] [CrossRef]
- Ciurli, P.; Bivona, U.; Barba, C.; Onder, G.; Silvestro, D.; Azicnuda, E.; Rigon, J.; Formisano, R. Metacognitive unawareness correlates with executive function impairment after severe traumatic brain injury. J. Int. Neuropsychol. Soc. 2010, 16, 360–368. [Google Scholar] [CrossRef]
- Bivona, U.; Costa, A.; Contrada, M.; Silvestro, D.; Azicnuda, E.; Aloisi, M.; Catania, G.; Ciurli, P.; Guariglia, C.; Caltagirone, C.; et al. Depression, apathy and impaired self-awareness following severe traumatic brain injury: A preliminary investigation. Brain Inj. 2019, 33, 1245–1256. [Google Scholar] [CrossRef]
- Bivona, U.; Formisano, R.; De Laurentiis, S.; Accetta, N.; Rita Di Cosimo, M.; Massicci, R.; Ciurli, P.; Azicnuda, E.; Silvestro, D.; Sabatini, U.; et al. Theory of mind impairment after severe traumatic brain injury and its relationship with caregivers’ quality of life. Restor. Neurol. Neurosci. 2015, 33, 335–345. [Google Scholar] [CrossRef]
- Mathias, J.L.; Wheaton, P. Changes in attention and information-processing speed following severe traumatic brain injury: A meta-analytic review. Neuropsychology 2007, 21, 212–223. [Google Scholar] [CrossRef]
- Miotto, E.C.; Cinalli, F.Z.; Serrao, V.T.; Benute, G.G.; Lucia, M.C.S.; Scaff, M. Cognitive deficits in patients with mild to moderate traumatic brain injury. Arq. Neuropsiquiatr. 2010, 68, 862–868. [Google Scholar] [CrossRef]
- Fleminger, S. Long-term psychiatric disorders after traumatic brain injury. Eur. J. Anaesthesiol. 2008, 25, 123–130. [Google Scholar] [CrossRef]
- Bergamini, E.; Iosa, M.; Belluscio, V.; Morone, G.; Tramontano, M.; Vannozzi, G. Multi-sensor assessment of dynamic balance during gait in patients with subacute stroke. J. Biomech. 2017, 61, 208–215. [Google Scholar] [CrossRef]
- Chen, G.; Patten, C.; Kothari, D.H.; Zajac, F.E. Gait differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds. Gait Posture 2005, 22, 51–56. [Google Scholar] [CrossRef]
- Iosa, M.; Fusco, A.; Morone, G.; Pratesi, L.; Coiro, P.; Venturiero, V.; De Angelis, D.; Bragoni, M.; Paolucci, S. Assessment of upper-body dynamic stability during walking in patients with subacute stroke. J. Rehabil. Res. Dev. 2012, 49, 439. [Google Scholar] [CrossRef]
- Mancini, M.; King, L.A.; Salarian, A.; Holmstrom, L.; McNames, J.; Horak, F.B. Mobility Lab to Assess Balance and Gait with Synchronized Body-worn Sensors. J. Bioeng. Biomed. Sci. 2014, 1–15. [Google Scholar] [CrossRef]
- Patterson, K.K.; Parafianowicz, I.; Danells, C.J.; Closson, V.; Verrier, M.C.; Staines, W.R.; Black, S.E.; McIlroy, W.E. Gait Asymmetry in Community-Ambulating Stroke Survivors. Arch. Phys. Med. Rehabil. 2008, 89, 304–310. [Google Scholar] [CrossRef]
- Schlachetzki, J.C.M.; Aminian, K.; Klucken, J.; Kohl, Z.; Marxreiter, F.; Barth, J.; Reinfelder, S.; Gassner, H.; Eskofier, B.M.; Winkler, J.; et al. Wearable sensors objectively measure gait parameters in Parkinson’s disease. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Rinne, M.B.; Pasanen, M.E.; Vartiainen, M.V.; Lehto, T.M.; Sarajuuri, J.M.; Alaranta, H.T. Motor performance in physically well-recovered men with traumatic brain injury. J. Rehabil. Med. 2006, 38, 224–229. [Google Scholar] [CrossRef]
- Williams, G.; Galna, B.; Morris, M.E.; John, O. Spatio-Temporal Deficits and Kinematic Classification of Gait following a Traumatic Brain Injury: A systematic review. J. Head Trauma Rehabil. 2010, 25, 366–374. [Google Scholar] [CrossRef]
- Formisano, R.; Lucia, F.S.; Birbamer, G.; Gerstenbrand, F. Post-Traumatic Cerebellar Syndrome. New Trends Clin. Neuropharmacol. 1987, 1, 115–118. [Google Scholar]
- Formisano, R.; Zasler, N.D. Posttraumatic parkinsonism. J. Head Trauma Rehabil. 2014, 29, 387–390. [Google Scholar] [CrossRef]
- Lehmann, J.; Sherlyn, B.; Price, R.; Burleigh, A.; Hertling, D. Quantitative Evaluation of Sway as an Indicator of Functional Balance in Post-Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 1990, 93, 2012–2013. [Google Scholar]
- Wade, L.D.; Canning, C.G.; Fowler, V.; Felmingham, K.L.; Baguley, I.J. Changes in postural sway and performance of functional tasks during rehabilitation after traumatic brain injury. Arch. Phys. Med. Rehabil. 1997, 78, 1107–1111. [Google Scholar] [CrossRef]
- Geurts, A.C.H.; Ribbers, G.M.; Knoop, J.A.; Van Limbeek, J. Identification of static and dynamic postural instability following traumatic brain injury. Arch. Phys. Med. Rehabil. 1996, 77, 639–644. [Google Scholar] [CrossRef]
- Chou, L.S.; Kaufman, K.R.; Walker-Rabatin, A.E.; Brey, R.H.; Basford, J.R. Dynamic instability during obstacle crossing following traumatic brain injury. Gait Posture 2004, 20, 245–254. [Google Scholar] [CrossRef]
- Ochi, F. Temporal-Spatial Feature of Gait after Traumatic Brain Injury. J. Head Trauma Rehabil. 1999, 14, 105–115. [Google Scholar] [CrossRef]
- Basford, J.R.; Chou, L.S.; Kaufman, K.R.; Brey, R.H.; Walker, A.; Malec, J.F.; Moessner, A.M.; Brown, A.W. An assessment of gait and balance deficits after traumatic brain injury. Arch. Phys. Med. Rehabil. 2003, 84, 343–349. [Google Scholar] [CrossRef]
- Kavanagh, J.J.; Menz, H.B. Accelerometry: A technique for quantifying movement patterns during walking. Gait Posture 2008, 28, 1–15. [Google Scholar] [CrossRef]
- Buckley, C.; Galna, B.; Rochester, L.; Mazzà, C. Upper body accelerations as a biomarker of gait impairment in the early stages of Parkinson’s disease. Gait Posture 2019, 71, 289–295. [Google Scholar] [CrossRef]
- Shany, T.; Redmond, S.J.; Marschollek, M.; Lovell, N.H. Assessing fall risk using wearable sensors: A practical discussion. Z. Gerontol. Geriatr. 2012, 45, 694–706. [Google Scholar] [CrossRef]
- Buckley, C.; Brook, G.; Lynn, R.; Claudia, M. Attenuation of Upper Body Accelerations during Gait: Piloting an Innovative Assessment Tool for Parkinson’s Disease. Biomed Res. Int. 2015, 2015. [Google Scholar] [CrossRef]
- Belluscio, V.; Bergamini, E.; Salatino, G.; Marro, T.; Gentili, P.; Iosa, M.; Morelli, D.; Vannozzi, G. Dynamic balance assessment during gait in children with Down and Prader-Willi syndromes using inertial sensors. Hum. Mov. Sci. 2019, 63, 53–61. [Google Scholar] [CrossRef]
- Summa, A.; Vannozzi, G.; Bergamini, E.; Iosa, M.; Morelli, D.; Cappozzo, A. Multilevel upper body movement control during gait in children with cerebral palsy. PLoS ONE 2016, 11, 1–13. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Baldwin, M.; Polissar, N.L.; Gruber, W. Predicting the probability for falls in community-dwelling older adults. Phys. Ther. 1997, 77, 812–819. [Google Scholar] [CrossRef]
- Esser, P.; Dawes, H.; Collett, J.; Feltham, M.G.; Howells, K. Assessment of spatio-temporal gait parameters using inertial measurement units in neurological populations. Gait Posture 2011, 34, 558–560. [Google Scholar] [CrossRef]
- Haggard, P.; Cockburn, J.; Cock, J.; Fordham, C.; Wade, D. Interference between gait and cognitive tasks in a rehabilitating neurological population. J. Neurol. Neurosurg. Psychiatry 2000, 69, 479–486. [Google Scholar] [CrossRef]
- Iosa, M.; De Sanctis, M.; Summa, A.; Bergamini, E.; Morelli, D.; Vannozzi, G. Usefulness of magnetoinertial wearable devices in neurorehabilitation of children with cerebral palsy. Appl. Bionics Biomech. 2018, 2018. [Google Scholar] [CrossRef]
- Cohen, J. Statistical power analysis. Int. Encycl. Educ. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Levin, H.S.; O′Donnel, V.M.; Grossaman, R.G. The Galveston Orientation and Amnesia Test. J. Nerv. Ment. Dis. 1979, 167, 675–684. [Google Scholar] [CrossRef]
- Herman, T.; Inbar-borovsky, N.; Brozgol, M.; Giladi, N.; Hausdorff, J.M. The Dynamic Gait Index in Healthy Older Adults: The Role of StairClimbing, Fear of Falling and Gender. Gait Posture 2009, 29, 237–241. [Google Scholar] [CrossRef]
- Berg, W.P.; Alessio, H.M.; Mills, E.M.; Tong, C. Circumstances and consequences of falls in independent community-dwelling older adults. Age Ageing 1997, 26, 261–268. [Google Scholar] [CrossRef]
- Howe, J.A.; Inness, E.L.; Venturini, A.; Williams, J.I.; Verrier, M.C. The Community Balance and Mobility Scale—A balance measure for individuals with traumatic brain injury. Clin. Rehabil. 2006, 20, 885–895. [Google Scholar] [CrossRef]
- Van Hedel, H.J.; Wirz, M.; Dietz, V. Assessing walking ability in subjects with spinal cord injury: Validity and reliability of 3 walking tests. Arch. Phys. Med. Rehabil. 2005, 86, 190–196. [Google Scholar] [CrossRef]
- Duncan, P.W.; Studenski, S.; Richards, L.; Gollub, S.; Lai, S.M.; Reker, D.; Perera, S.; Yates, J.; Koch, V.; Rigler, S.; et al. Randomized clinical trial of therapeutic exercise in subacute stroke. Stroke 2003, 34, 2173–2180. [Google Scholar] [CrossRef]
- Turcato, A.M.; Godi, M.; Giardini, M.; Arcolin, I.; Nardone, A.; Giordano, A.; Schieppati, M. Abnormal gait pattern emerges during curved trajectories in high-functioning Parkinsonian patients walking in line at normal speed. PLoS ONE 2018, 13, 1–26. [Google Scholar] [CrossRef]
- Zhang, Y.B.; Wang, W.Q. Reliability of the Fukuda stepping test to determine the side of vestibular dysfunction. J. Int. Med. Res. 2011, 39, 1432–1437. [Google Scholar] [CrossRef]
- Belluscio, V.; Bergamini, E.; Iosa, M.; Tramontano, M.; Morone, G.; Vannozzi, G. The iFST: An instrumented version of the Fukuda Stepping Test for balance assessment. Gait Posture 2018, 60, 203–208. [Google Scholar] [CrossRef]
- Bergamini, E.; Ligorio, G.; Summa, A.; Vannozzi, G.; Cappozzo, A.; Sabatini, A.M. Estimating orientation using magnetic and inertial sensors and different sensor fusion approaches: Accuracy assessment in manual and locomotion tasks. Sensors (Switzerland) 2014, 14, 18625–18649. [Google Scholar] [CrossRef]
- Mazzà, C.; Iosa, M.; Pecoraro, F.; Cappozzo, A. Control of the upper body accelerations in young and elderly women during level walking. J. Neuroeng. Rehabil. 2008, 5, 30. [Google Scholar] [CrossRef]
- Pasciuto, I.; Bergamini, E.; Iosa, M.; Vannozzi, G.; Cappozzo, A. Overcoming the limitations of the Harmonic Ratio for the reliable assessment of gait symmetry. J. Biomech. 2017, 53, 84–89. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Melendez-Calderon, A.; Roby-Brami, A.; Burdet, E. On the analysis of movement smoothness. J. Neuroeng. Rehabil. 2015, 12, 1–11. [Google Scholar] [CrossRef]
- Fang, X.; Liu, C.; Jiang, Z. Reference values of gait using APDM movement monitoring inertial sensor system. R. Soc. Open Sci. 2018, 5. [Google Scholar] [CrossRef]
- Peppe, A.; Stanzione, P.; Pierantozzi, M.; Semprini, R.; Bassi, A.; Santilli, A.M.; Formisano, R.; Piccolino, M.; Bernardi, G. Does pattern electroretinogram spatial tuning alteration in Parkinson’s disease depend on motor disturbances or retinal dopaminergic loss? Electroencephalogr. Clin. Neurophysiol. 1998, 106, 374–382. [Google Scholar] [CrossRef]
- Formisano, R.; D’Ippolito, M.; Risetti, M.; Riccio, A.; Caravasso, C.F.; Catani, S.; Rizza, F.; Forcina, A.; Buzzi, M.G. Vegetative state, minimally conscious state, akinetic mutism and parkinsonism as a continuum of recovery from disorders of consciousness: An exploratory and preliminary study. Funct. Neurol. 2011, 26, 15–24. [Google Scholar]
- Tramontano, M.; Morone, G.; Curcio, A.; Temperoni, G.; Medici, A.; Morelli, D.; Caltagirone, C.; Paolucci, S.; Iosa, M. Maintaining gait stability during dual walking task: Effects of age and neurological disorders. Eur. J. Phys. Rehabil. Med. 2017, 53, 7–13. [Google Scholar]
- Galna, B.; Barry, G.; Jackson, D.; Mhiripiri, D.; Olivier, P.; Rochester, L. Accuracy of the Microsoft Kinect sensor for measuring movement in people with Parkinson’s disease. Gait Posture 2014, 39, 1062–1068. [Google Scholar] [CrossRef]
- Boonstra, A.M.; Schiphorst, H.R.; Reneman, M.F.; Posthumus, J.B.; Stewart, R.E. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int. J. Rehabil. Res. 2008, 31, 165–169. [Google Scholar] [CrossRef]
- Iosa, M.; Marro, T.; Paolucci, S.; Morelli, D. Stability and harmony of gait in children with cerebral palsy. Res. Dev. Disabil. 2012, 33, 129–135. [Google Scholar] [CrossRef]
- Doi, T.; Hirata, S.; Ono, R.; Tsutsumimoto, K.; Misu, S.; Ando, H. The harmonic ratio of trunk acceleration predicts falling among older people: Results of a 1-year prospective study. J. Neuroeng. Rehabil. 2013, 10, 7. [Google Scholar] [CrossRef]
- Menz, H.B.; Lord, S.R.; Fitzpatrick, R.C. Acceleration patterns of the head and pelvis when walking on level and irregular surfaces. Gait Posture 2003, 18, 35–46. [Google Scholar] [CrossRef]
- Wong, S.S.T.; Yam, M.S.; Ng, S.S.M. The Figure-of-Eight Walk test: Reliability and associations with stroke-specific impairments. Disabil. Rehabil. 2013, 35, 1896–1902. [Google Scholar] [CrossRef] [PubMed]
- Di Russo, F.; Incoccia, C.; Formisano, R.; Sabatini, U.; Zoccolotti, P. Abnormal motor preparation in severe traumatic brain injury with good recovery. J. Neurotrauma 2005, 22, 297–312. [Google Scholar] [CrossRef] [PubMed]
- Foley, J.A.; Cantagallo, A.; Della Sala, S.; Logie, R.H. Dual task performance and post traumatic brain injury. Brain Inj. 2010, 24, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Baker, K.; Rochester, L.; Nieuwboer, A. The Immediate Effect of Attentional, Auditory, and a Combined Cue Strategy on Gait During Single and Dual Tasks in Parkinson’s Disease. Arch. Phys. Med. Rehabil. 2007, 88, 1593–1600. [Google Scholar] [CrossRef] [PubMed]
- Paquet, N.; Taillon-Hobson, A.; Lajoie, Y. Fukuda and Babinski-Weil tests: Within-subject variability and test-retest reliability in nondisabled adults. J. Rehabil. Res. Dev. 2014, 51, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Akin, F.W.; Murnane, O.D.; Hall, C.D.; Riska, K.M. Vestibular consequences of mild traumatic brain injury and blast exposure: A review. Brain Inj. 2017, 31, 1188–1194. [Google Scholar] [CrossRef]
- Mancini, M.; Horak, F.B. The relevance of clinical balance assessment tools to differentiate balance deficits. Eur. J. Phys. Rehabil. Med. 2010, 46, 239–248. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| CG | sTBI-1 | sTBI-2 | |
|---|---|---|---|
| Nr. of Participants | 20 | 10 | 10 |
| Nr. of Males | 15 | 8 | 7 |
| Age [Years] | 33.9 ± 9.5 | 33.2 ± 9.6 | 36.1 ± 13.1 |
| Body Mass [kg] | 78.3 ± 14.9 | 75.9 ± 16.2 | 71.0 ± 14.7 |
| Body Height [m] | 1.78 ± 0.09 | 1.73 ± 0.11 | 1.70 ± 0.11 |
| Time Since Trauma [days] | - | 308 ± 182 | 512 ± 476 |
| sTBI-1 | sTBI-2 | p-Value | |
|---|---|---|---|
| Dynamic gait index (DGI) | 22.1 ± 1.7 * | 15.0 ± 3.0 * | 0.000 |
| Berg balance scale (BBS) | 49.8 ± 2.1 * | 42.4 ± 3.9 * | 0.000 |
| Community balance and mobility scale (CB&M) | 42.0 ± 14.0 * | 15.5 ± 8.9 * | 0.000 |
| Stride Frequency | Stride Duration | Rotation | Side | Displacement | |||
|---|---|---|---|---|---|---|---|
| AP | ML | ||||||
| [Stridesxs−1] | [s] | [Degrees] | [% Right] | [cm] | [cm] | ||
| 10mWT | CG | 0.9 ± 0.0 * | 1.1 ± 0.1 * | - | - | - | - |
| sTBI-1 | 0.8 ± 0.1 § | 1.2 ± 0.1 § | - | - | - | - | |
| sTBI-2 | 0.7 ± 0.1 *,§ | 1.4 ± 0.2 *,§ | - | - | - | - | |
| F8WT | CG | 0.8 ± 0.1 * | 1.2 ± 0.1 * | - | - | - | - |
| sTBI-1 | 0.8 ± 0.1 § | 1.2 ± 0.2 § | - | - | - | - | |
| sTBI-2 | 0.7 ± 0.1 *,§ | 1.5 ± 0.2 *,§ | - | - | - | - | |
| FST | CG | 0.8 ± 0.1 *,# | 1.2 ± 0.2 # | 66 ± 66 | 30 | 146 ± 71 | 44 ± 33 |
| sTBI-1 | 0.6 ± 0.2 §,# | 1.8 ± 0.9 # | 27 ± 17 | 40 | 141 ± 38 | 45 ± 46 | |
| sTBI-2 | 0.5 ± 0.2 *,§ | 2.0 ± 1.4 | 28 ± 23 | 50 | 101 ± 60 | 27 ± 31 | |
| 10mWT | F8WT | FST | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| BBS | DGI | CB&M | BBS | DGI | CB&M | BBS | DGI | CB&M | ||
| RMS_P | AP | −0.243 | −0.309 | −0.254 | −0.337 | −0.335 | −0.398 | 0.043 | 0.103 | 0.118 |
| ML | −0.656 ** | −0.467 * | −0.605 ** | −0.730 ** | −0.666 ** | −0.819 ** | −0.404 | −0.445 | −0.500 * | |
| RMS_S | AP | −0.555 * | −0.585 ** | −0.679 ** | −0.491 * | −0.484 * | −0.600 ** | −0.495 * | −0.655 ** | −0.500 * |
| ML | −0.583 ** | −0.503 * | −0.733 ** | −0.571 * | −0.463 * | −0.749 ** | −0.460 * | −0.516 * | −0.695 ** | |
| RMS_H | AP | −0.674 ** | −0.641 ** | −0.712 ** | −0.594 ** | −0.611 ** | −0.665 ** | −0.353 | −0.309 | −0.246 |
| ML | −0.781 ** | −0.705 ** | −0.821 ** | −0.796 ** | −0.708 ** | −0.839 ** | −0.618 ** | −0.506 * | −0.660 ** | |
| ACPH | AP | 0.535 * | 0.577 ** | 0.451 | 0.481 * | 0.349 | 0.418 | 0.608 ** | 0.550 * | 0.512 * |
| ML | 0.493 * | 0.491 * | 0.595 ** | 0.631 ** | 0.598 ** | 0.637 ** | 0.630 ** | 0.481 * | 0.623 ** | |
| CC | −0.061 | −0.076 | 0.004 | 0.057 | 0.059 | 0.182 | 0.544 * | 0.551 * | 0.567 * | |
| ACPS | AP | 0.495 * | 0.443 | 0.588 ** | 0.477 * | 0.453 | 0.454 | 0.627 ** | 0.699 ** | 0.539 * |
| ML | 0.126 | 0.159 | 0.309 | 0.181 | 0.090 | 0.279 | 0.254 | 0.122 | 0.391 | |
| CC | −0.247 | −0.286 | −0.367 | −0.251 | −0.190 | −0.368 | 0.093 | −0.129 | −0.072 | |
| ACSH | AP | 0.287 | 0.197 | 0.242 | 0.395 | 0.302 | 0.402 | 0.368 | 0.207 | 0.330 |
| ML | 0.663 ** | 0.516 * | 0.612 ** | 0.599 ** | 0.497 * | 0.486 * | 0.553 * | 0.466 * | 0.372 | |
| CC | 0.172 | 0.094 | 0.337 | 0.346 | 0.224 | 0.451 | 0.431 | 0.506 * | 0.530 * | |
| iHR | AP | 0.423 | 0.507 * | 0.605 ** | 0.196 | 0.221 | 0.361 | 0.365 | 0.433 | 0.391 |
| ML | 0.149 | 0.319 | 0.356 | −0.143 | −0.127 | −0.019 | 0.109 | 0.188 | 0.012 | |
| CC | 0.734 ** | 0.733 ** | 0.677 ** | 0.693 ** | 0.667 ** | 0.658 ** | 0.016 | 0.272 | 0.023 | |
| SPARC | AP | 0.205 | 0.051 | 0.170 | 0.384 | 0.308 | 0.411 | −0.056 | 0.011 | −0.061 |
| ML | 0.285 | 0.390 | 0.456 * | 0.195 | 0.192 | 0.160 | 0.086 | 0.092 | −0.056 | |
| CC | 0.390 | 0.512 * | 0.251 | 0.525 * | 0.601 ** | 0.547 * | 0.217 | 0.211 | 0.114 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belluscio, V.; Bergamini, E.; Tramontano, M.; Orejel Bustos, A.; Allevi, G.; Formisano, R.; Vannozzi, G.; Buzzi, M.G. Gait Quality Assessment in Survivors from Severe Traumatic Brain Injury: An Instrumented Approach Based on Inertial Sensors. Sensors 2019, 19, 5315. https://doi.org/10.3390/s19235315
Belluscio V, Bergamini E, Tramontano M, Orejel Bustos A, Allevi G, Formisano R, Vannozzi G, Buzzi MG. Gait Quality Assessment in Survivors from Severe Traumatic Brain Injury: An Instrumented Approach Based on Inertial Sensors. Sensors. 2019; 19(23):5315. https://doi.org/10.3390/s19235315
Chicago/Turabian StyleBelluscio, Valeria, Elena Bergamini, Marco Tramontano, Amaranta Orejel Bustos, Giulia Allevi, Rita Formisano, Giuseppe Vannozzi, and Maria Gabriella Buzzi. 2019. "Gait Quality Assessment in Survivors from Severe Traumatic Brain Injury: An Instrumented Approach Based on Inertial Sensors" Sensors 19, no. 23: 5315. https://doi.org/10.3390/s19235315
APA StyleBelluscio, V., Bergamini, E., Tramontano, M., Orejel Bustos, A., Allevi, G., Formisano, R., Vannozzi, G., & Buzzi, M. G. (2019). Gait Quality Assessment in Survivors from Severe Traumatic Brain Injury: An Instrumented Approach Based on Inertial Sensors. Sensors, 19(23), 5315. https://doi.org/10.3390/s19235315