Short-Term Effects of the Serious Game “Fit, Food, Fun” on Nutritional Knowledge: A Pilot Study among Children and Adolescents
 , , , , and
, , , , and 
Abstract
1. Introduction
2. Materials and Methods
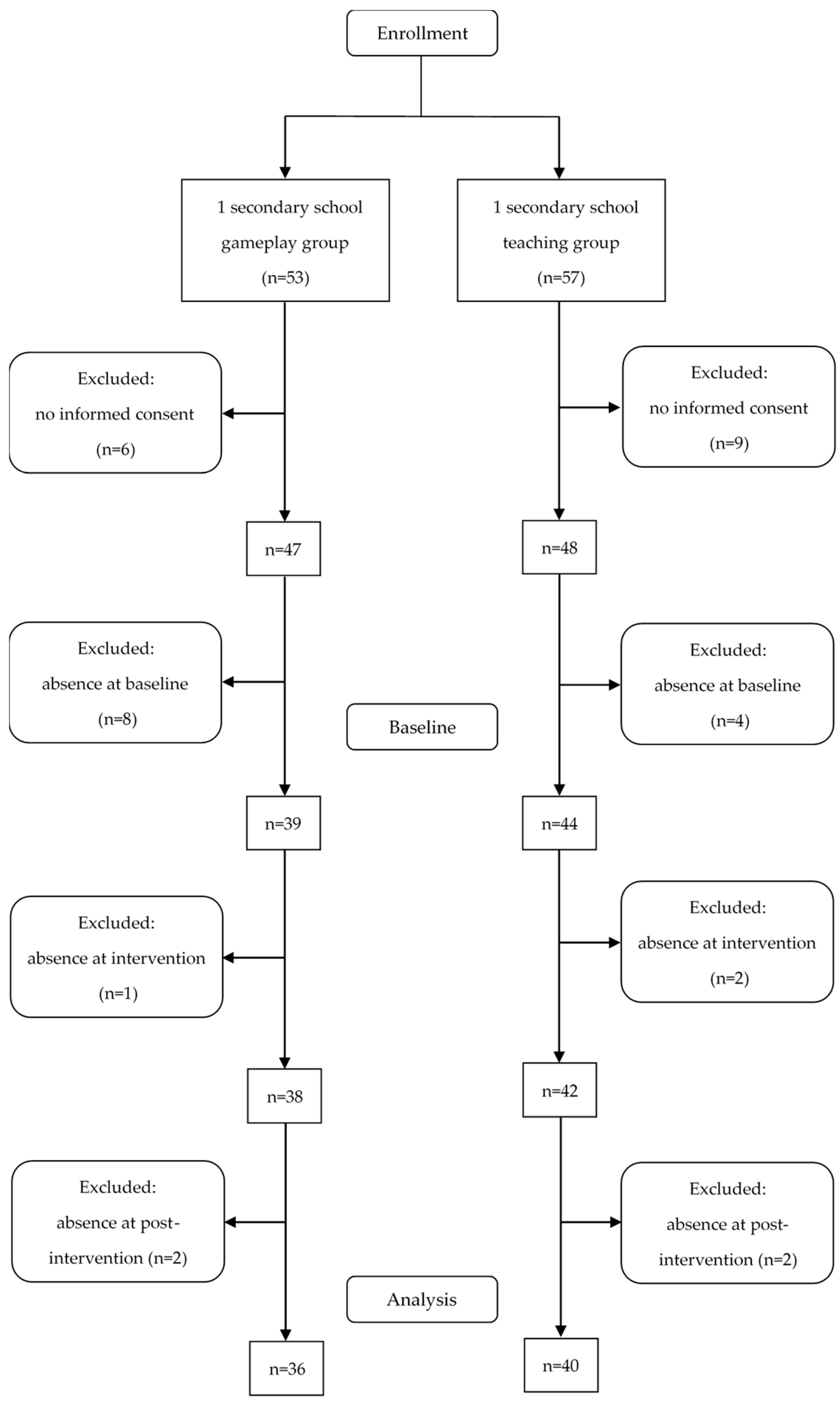
2.1. Study Participants and Design
2.2. Intervention
2.2.1. Gameplay Group
2.2.2. Teaching Group
2.3. Measures
2.3.1. Anthropometry
2.3.2. Questionnaire
2.4. Statistical Analyses
3. Results
3.1. Participant Characteristics
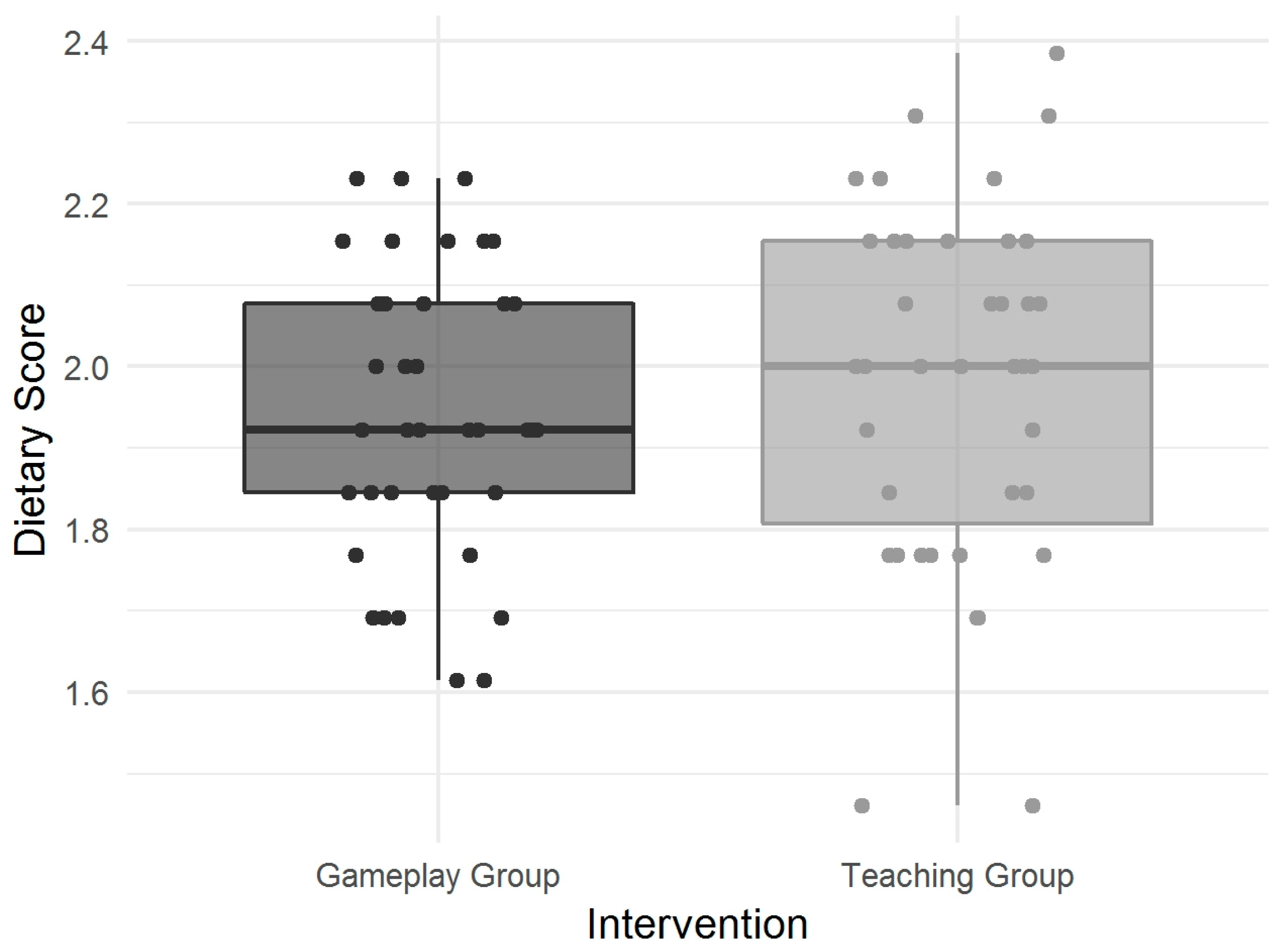
3.2. Nutritional Knowledge
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. New Global Estimates of Child and Adolescent Obesity Released on World Obesity Day. Available online: http://www.who.int/end-childhood-obesity/news/new-estimate-child-adolescent-obesity/en/ (accessed on 11 September 2018).
- Schienkiewitz, A.; Brettschneider, A.K.; Damerow, S.; Schaffrath Rosario, A. Übergewicht und Adipositas im Kindes- und Jugendalter in Deutschland—Querschnittergebnisse aus KiGGS Welle 2 und Trends. J. Health Monitoring 2018, 3, 16–23. [Google Scholar] [CrossRef]
- Deterding, S. Proceedings of the 15th International Academic MindTrek Conference Envisioning Future Media Environments; ACM: New York, NY, USA, 2011; ISBN 9781450308168. [Google Scholar]
- DeSmet, A.; van Ryckeghem, D.; Compernolle, S.; Baranowski, T.; Thompson, D.; Crombez, G.; Poels, K.; van Lippevelde, W.; Bastiaensens, S.; van Cleemput, K.; et al. A meta-analysis of serious digital games for healthy lifestyle promotion. Prev. Med. 2014, 69, 95–107. [Google Scholar] [CrossRef]
- Sailer, M.; Hense, J.U.; Mayr, S.K.; Mandl, H. How gamification motivates: An experimental study of the effects of specific game design elements on psychological need satisfaction. Comput. Hum. Behav. 2017, 69, 371–380. [Google Scholar] [CrossRef]
- Blakely, G.; Skirton, H.; Cooper, S.; Allum, P.; Nelmes, P. Educational gaming in the health sciences: Systematic review. J. Adv. Nurs. 2009, 65, 259–269. [Google Scholar] [CrossRef]
- Read, J.L.; Shortell, S.M. Interactive games to promote behavior change in prevention and treatment. JAMA 2011, 305, 1704–1705. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T.; Baranowski, J.; Chen, T.-A.; Buday, R.; Beltran, A.; Dadabhoy, H.; Ryan, C.; Lu, A.S. Videogames that Encourage Healthy Behavior did not Alter Fasting Insulin or other Diabetes Risks in Children: Randomized Clinical Trial. Games Health J. 2019. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T.; Blumberg, F.; Buday, R.; DeSmet, A.; Fiellin, L.E.; Green, C.S.; Kato, P.M.; Lu, A.S.; Maloney, A.E.; Mellecker, R.; et al. Games for Health for Children-Current Status and Needed Research. Games Health J. 2016, 5, 1–12. [Google Scholar] [CrossRef]
- Baranowski, T.; Buday, R.; Thompson, D.; Lyons, E.J.; Lu, A.S.; Baranowski, J. Developing Games for Health Behavior Change: Getting Started. Games Health J. 2013, 2, 183–190. [Google Scholar] [CrossRef]
- Primack, B.A.; Carroll, M.V.; McNamara, M.; Klem, M.L.; King, B.; Rich, M.; Chan, C.W.; Nayak, S. Role of video games in improving health-related outcomes: A systematic review. Am. J. Prev. Med. 2012, 42, 630–638. [Google Scholar] [CrossRef]
- Lewis, Z.H.; Swartz, M.C.; Lyons, E.J. What’s the Point?: A Review of Reward Systems Implemented in Gamification Interventions. Games Health J. 2016, 5, 93–99. [Google Scholar] [CrossRef]
- Baranowski, T.; Ryan, C.; Hoyos-Cespedes, A.; Lu, A.S. Nutrition Education and Dietary Behavior Change Games: A Scoping Review. Games Health J. 2019, 8, 153–176. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Noguera, M.; Tort, S.; Martínez-Zapata, M.J.; Bonfill, X. Primary school interventions to promote fruit and vegetable consumption: A systematic review and meta-analysis. Prev. Med. 2011, 53, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T.; Buday, R.; Thompson, D.I.; Baranowski, J. Playing for real: Video games and stories for health-related behavior change. Am. J. Prev. Med. 2008, 34, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Turnin, M.C.; Tauber, M.T.; Couvaras, O.; Jouret, B.; Bolzonella, C.; Bourgeois, O.; Buisson, J.C.; Fabre, D.; Cance-Rouzaud, A.; Tauber, J.P.; et al. Evaluation of microcomputer nutritional teaching games in 1876 children at school. Diabetes Metab. 2001, 27, 459–464. [Google Scholar] [PubMed]
- Baranowski, T.; Baranowski, J.; Cullen, K.W.; Marsh, T.; Islam, N.; Zakeri, I.; Honess-Morreale, L.; deMoor, C. Squire’s Quest! Am. J. Prev. Med. 2003, 24, 52–61. [Google Scholar] [CrossRef]
- Evans, C.E.L.; Christian, M.S.; Cleghorn, C.L.; Greenwood, D.C.; Cade, J.E. Systematic review and meta-analysis of school-based interventions to improve daily fruit and vegetable intake in children aged 5 to 12 y. Am. J. Clin. Nutr. 2012, 96, 889–901. [Google Scholar] [CrossRef] [PubMed]
- Vézina-Im, L.-A.; Beaulieu, D.; Bélanger-Gravel, A.; Boucher, D.; Sirois, C.; Dugas, M.; Provencher, V. Efficacy of school-based interventions aimed at decreasing sugar-sweetened beverage consumption among adolescents: A systematic review. Public Health Nutr. 2017, 20, 2416–2431. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.V.; Shegog, R.; Chow, J.; Finley, C.; Pomeroy, M.; Smith, C.; Hoelscher, D.M. Effects of the Quest to Lava Mountain Computer Game on Dietary and Physical Activity Behaviors of Elementary School Children: A Pilot Group-Randomized Controlled Trial. J. Acad. Nutr. Diet. 2015, 115, 1260–1271. [Google Scholar] [CrossRef]
- Baranowski, T.; Baranowski, J.; Thompson, D.; Buday, R.; Jago, R.; Griffith, M.J.; Islam, N.; Nguyen, N.; Watson, K.B. Video game play, child diet, and physical activity behavior change a randomized clinical trial. Am. J. Prev. Med. 2011, 40, 33–38. [Google Scholar] [CrossRef]
- Holzmann, S.L.; Dischl, F.; Schäfer, H.; Groh, G.; Hauner, H.; Holzapfel, C. Digital Gaming for Nutritional Education: A Survey on Preferences, Motives, and Needs of Children and Adolescents. JMIR Form. Res. 2019, 3, e10284. [Google Scholar] [CrossRef]
- Schäfer, H.; Plecher, D.A.; Holzmann, S.L.; Groh, G.; Klinker, G.; Holzapfel, C.; Hauner, H. NUDGE—NUtritional, Digital Games in Enable; Positive Gaming: Workshop on Gamification and Games for Wellbeing; A CHI PLAY ’17 Workshop: Amsterdam, The Netherlands, 15 October 2017. [Google Scholar]
- Keller, J.M. Motivational Design for Learning and Performance: The ARCS Model Approach; Springer: Boston, MA, USA, 2010; ISBN 1441912509. [Google Scholar]
- Städeli, C. Kompetenzorientiert unterrichten—das AVIVA-Modell. Fünf Phasen guten Unterrichts; hep Verlag: Bern, Switzerland, 2013; ISBN 978-3-03905-900-3. [Google Scholar]
- Kromeyer-Hauschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.C.; Hesse, V.; von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Perzentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben. Monatsschr Kinderheilkd 2001, 149, 807–818. [Google Scholar] [CrossRef]
- Beckert-Zieglschmid, C.; Brähler, E. Der Leipziger Lebensstilfragebogen für Jugendliche (LLfJ). Ein Instrument zur Arbeit mit Jugendlichen; das Handbuch; mit zahlreichen Tabellen; Vandenhoeck & Ruprecht: Göttingen, Germany, 2007; ISBN 9783525491072. [Google Scholar]
- Strobl, R.; Müller, M.; Thorand, B.; Linkohr, B.; Autenrieth, C.S.; Peters, A.; Grill, E. Men benefit more from midlife leisure-time physical activity than women regarding the development of late-life disability—Results of the KORA-Age study. Prev. Med. 2014, 62, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Dudley, D.A.; Cotton, W.G.; Peralta, L.R. Teaching approaches and strategies that promote healthy eating in primary school children: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 28. [Google Scholar] [CrossRef] [PubMed]
- Amaro, S.; Viggiano, A.; Di Costanzo, A.; Madeo, I.; Viggiano, A.; Baccari, M.E.; Marchitelli, E.; Raia, M.; Viggiano, E.; Deepak, S.; et al. Kalèdo, a new educational board-game, gives nutritional rudiments and encourages healthy eating in children: A pilot cluster randomized trial. Eur. J. Pediatr. 2006, 165, 630–635. [Google Scholar] [CrossRef] [PubMed]
- Viggiano, A.; Viggiano, E.; Di Costanzo, A.; Viggiano, A.; Andreozzi, E.; Romano, V.; Rianna, I.; Vicidomini, C.; Gargano, G.; Incarnato, L.; et al. Kaledo, a board game for nutrition education of children and adolescents at school: Cluster randomized controlled trial of healthy lifestyle promotion. Eur. J. Pediatr. 2015, 174, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Hermans, R.C.J.; van den Broek, N.; Nederkoorn, C.; Otten, R.; Ruiter, E.L.M.; Johnson-Glenberg, M.C. Feed the Alien! The Effects of a Nutrition Instruction Game on Children’s Nutritional Knowledge and Food Intake. Games Health J. 2018, 7, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Könnölä, K.; Ranti, T.; Liukkonen, T.N.; Mäkilä, T. Food-Related Gamification: Literature Review. In Proceedings of the GAME-ON 2016, Universidade Nova de Lisboa, Lisbon, Portugal, 13–15 September 2016. [Google Scholar]
- Howe, K.B.; Suharlim, C.; Ueda, P.; Howe, D.; Kawachi, I.; Rimm, E.B. Gotta catch’em all! Pokémon GO and physical activity among young adults: Difference in differences study. BMJ 2016, 355, i6270. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T. Pokémon Go, go, go, gone? Games Health J. 2016, 5, 293–294. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Nr | Parameter | Question |
|---|---|---|
| Selected Rules of the German Nutrition Society | ||
| 1 | Select (whole grain)1: For cereal products such as bread, pasta, rice, and flour, the (whole grain) choice is the best choice for your health. Foods made from (whole grain) satiate longer and contain (more) nutrients than white flour products. | Cloze |
| 2 | Reduce (sugar) and salt intake: Food and beverages sweetened with (sugar) are (not) recommended. Avoid them as much as possible and use (sugar) sparingly. Reduce salt and reduce the amount of salty food. | Cloze |
| 3 | Choose health-promoting fats: Prefer (vegetable) oils such as rapeseed oil and spreadable fats made from it. Avoid (hidden) fats. Fat is often “invisible” in processed foods such as (sausage), pastries, sweets, fast food, and (convenience products). | Cloze |
| 4 | Pay attention to body weight and stay (active): A wholesome (diet) and physical (activity) belong together. Not only regular sport is important, but also an active daily life. Per day, 30 to (60) min of moderate physical activity promotes your health. | Cloze |
| 5 | Choose (water) as your drink of choice: Drink around (1.5) liters every day. Ideally (water) or other non-caloric drinks such as unsweetened tea. Sugar-sweetened and alcoholic beverages are (not) recommendable. | Cloze |
| 6 | Vegetables and (fruits)—choose “5 a day”: Enjoy at least (3) portions of vegetables and (2) portions of (fruits) each day. | Cloze |
| Miscellaneous—Nutrition | ||
| 7 | What is the meaning of the term “calories” and what is a different term for calories? | Single choice |
| 8 | What is another word for protein? | Open |
| 9 | Is sugar a carbohydrate? | Single choice |
| 10 | How many servings of fruits and vegetables should you eat daily (one serving = handful)? | Single choice |
| 11 | Which of the following statements is correct? In daily nutrition you should... Reduce sugar, but you can eat as much salt as you like OR Use salt sparingly, but you can eat as much sugar as you like OR Reduce neither salt nor sugar OR Reduce sugar and salt OR Don’t know | Single choice |
| 12 | Which of the following statements is correct? Whole grain bread contains more nutrients (e.g., fiber) than white bread AND Satiates more than white bread OR White bread contains more nutrients (e.g., fiber) than whole grain bread OR White bread and whole grain bread do not differ in terms of nutrients (e.g., fiber) AND Satiety OR Don’t know | Single choice |
| 13 | Which of the following foods has the highest fat content for the same amount? Chocolate OR Hard caramels/sweets OR Jelly Bears OR Cereal bar OR Marshmallows OR Don’t know | Single choice |
| 14 | Which of the following statements is correct? Fruits and vegetables contain the same amount of sugar OR Vegetables contain less sugar than fruits for the same amount OR Fruits contain less sugar than vegetables for the same amount OR Don’t know | Single choice |
| 15 | Which of the following foods has the highest sugar content for the same amount? Soft drinks (e.g., lemonade, cola) OR Water OR Cow’s milk OR Juice spritzer OR Tomato juice OR Don’t know | Single choice |
| 16 | Which of the following statements is correct? Protein is particularly high in...Clarified butter OR Cucumber OR Pizza OR Licorice OR Tuna fish OR Don’t know | Single choice |
| 17 | What does the abbreviation DGE stand for? German Cooperative for Nutrition OR German Society for Global Warming OR German Society for Nutritional Habits OR German Nutrition Society OR Don’t know | Single choice |
| Miscellaneous—Physical Activity | ||
| 18 | How many calories (kcal) do you expend approximately if you ride a bike at medium effort for 2 h? Less than 200 kcal OR 600–1000 kcal OR More than 1000 kcal OR Don’t know | Single choice |
| 19 | In which of the following three sports do you expend the most energy during the same performance (e.g., duration, distance)? Cycling OR Running/Jogging OR Swimming OR Don’t know | Single choice |
| Parameter | Gameplay Group (GG) | Teaching Group (TG) | Difference | ||||
|---|---|---|---|---|---|---|---|
| Total N (%) or mean ± SD | Female N (%) or mean ± SD | Male N (%) or mean ± SD | Total N (%) or mean ± SD | Female N (%) or mean ± SD | Male N (%) or mean ± SD | p | |
| Total | 39 | 13 | 26 | 44 | 12 | 32 | |
| 7th grade | 27 | 10 | 17 | 28 | 8 | 20 | |
| 8th grade | 12 | 3 | 9 | 16 | 4 | 12 | |
| Age (y) | 13.5 ± 0.7 | 13.4 ± 0.8 | 13.6 ± 0.8 | 12.8 ± 0.9 | 12.5 ± 0.9 | 12.9 ± 0.9 | 0.0003 |
| Height (m) | 1.66 ± 0.1 | 1.60 ± 0.06 | 1.69 ± 0.09 | 1.61 ± 0.08 | 1.60 ± 0.06 | 1.61 ± 0.09 | 0.006 |
| Weight (kg) | 70.0 ± 18.6 | 70.3 ± 22.8 | 69.8 ± 16.6 | 57.8 ± 14.7 | 60.7 ± 15.9 | 56.7 ± 14.3 | 0.001 |
| BMI percentiles | 0.5 | ||||||
| Underweight | 1 (3%) | 1 (8%) | 0 (0%) | 1 (2%) | 0 (0%) | 1 (3%) | |
| Normal weight | 19 (49%) | 5 (38%) | 14 (54%) | 27 (61%) | 7 (58%) | 20 (62%) | |
| Overweight | 6 (15%) | 1 (8%) | 5 (19%) | 8 (18%) | 2 (17%) | 6 (19%) | |
| Obesity | 5 (13%) | 0 (0%) | 5 (19%) | 5 (11%) | 1 (8%) | 4 (12%) | |
| Severe Obesity | 8 (21%) | 6 (46%) | 2 (8%) | 3 (7%) | 2 (17%) | 1 (3%) | |
| Parameter | Gameplay Group (GG) | Teaching Group (TG) | Difference | ||
|---|---|---|---|---|---|
| n/N | % | n/N | % | p | |
| Healthy diet “importance” | 26/39 | 67 | 37/44 | 84 | 0.1 |
| Healthy diet “attention” | 23/37 | 62 | 32/44 | 73 | 0.4 |
| Physical activity | 0.08 | ||||
| High | 8/38 | 21 | 13/42 | 31 | |
| Moderate | 22/38 | 58 | 27/42 | 64 | |
| Low | 8/38 | 21 | 2/42 | 5 | |
| Knowledge | Gameplay Group (GG) | Teaching Group (TG) | Difference | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Category | N | Pre | Post | p | N | Pre | Post | p | p |
| Rules | 25 | 40 | |||||||
| (Whole) grain | 0.08 | 0.16 | 0.14 | 0.23 | |||||
| Sugar & salt | 0.26 | 0.35 | 0.35 | 0.48 | |||||
| Fats & oils | 0.12 | 0.10 | 0.03 | 0.08 | |||||
| Lifestyle | 0.21 | 0.22 | 0.15 | 0.31 | |||||
| Water & beverages | 0.47 | 0.63 | 0.38 | 0.62 | |||||
| Vegetables & fruits | 0.52 | 0.53 | 0.42 | 0.65 | |||||
| Total knowledge | 0.25 | 0.33 | 0.02 | 0.24 | 0.39 | <0.0001 | 0.02 | ||
| Miscellaneous | 35 | 40 | |||||||
| Nutrition | 0.44 | 0.58 | 0.40 | 0.58 | |||||
| Physical activity | 0.39 | 0.53 | 0.31 | 0.50 | |||||
| Total knowledge | 0.43 | 0.57 | <0.0001 | 0.39 | 0.56 | <0.0001 | 0.3 | ||
| Overall knowledge | 24 | 0.31 | 0.42 | 0.001 | 40 | 0.29 | 0.45 | <0.0001 | 0.01 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holzmann, S.L.; Schäfer, H.; Groh, G.; Plecher, D.A.; Klinker, G.; Schauberger, G.; Hauner, H.; Holzapfel, C. Short-Term Effects of the Serious Game “Fit, Food, Fun” on Nutritional Knowledge: A Pilot Study among Children and Adolescents. Nutrients 2019, 11, 2031. https://doi.org/10.3390/nu11092031
Holzmann SL, Schäfer H, Groh G, Plecher DA, Klinker G, Schauberger G, Hauner H, Holzapfel C. Short-Term Effects of the Serious Game “Fit, Food, Fun” on Nutritional Knowledge: A Pilot Study among Children and Adolescents. Nutrients. 2019; 11(9):2031. https://doi.org/10.3390/nu11092031
Chicago/Turabian StyleHolzmann, Sophie Laura, Hanna Schäfer, Georg Groh, David Alexander Plecher, Gudrun Klinker, Gunther Schauberger, Hans Hauner, and Christina Holzapfel. 2019. "Short-Term Effects of the Serious Game “Fit, Food, Fun” on Nutritional Knowledge: A Pilot Study among Children and Adolescents" Nutrients 11, no. 9: 2031. https://doi.org/10.3390/nu11092031
APA StyleHolzmann, S. L., Schäfer, H., Groh, G., Plecher, D. A., Klinker, G., Schauberger, G., Hauner, H., & Holzapfel, C. (2019). Short-Term Effects of the Serious Game “Fit, Food, Fun” on Nutritional Knowledge: A Pilot Study among Children and Adolescents. Nutrients, 11(9), 2031. https://doi.org/10.3390/nu11092031