Evaluating the Risk of Epidemic Thunderstorm Asthma: Lessons from Australia

 , , ,
, , ,
Abstract
:1. Introduction
1.1. Study Location
1.2. Thunderstorms in Tasmania
1.3. Pollen in Tasmania
1.4. Natural Disaster Risk Assessment in the Tasmanian Context
1.5. Research Aim
2. Materials and Methods
2.1. Study Design
2.2. Health Outcomes
2.3. Meteorological Data
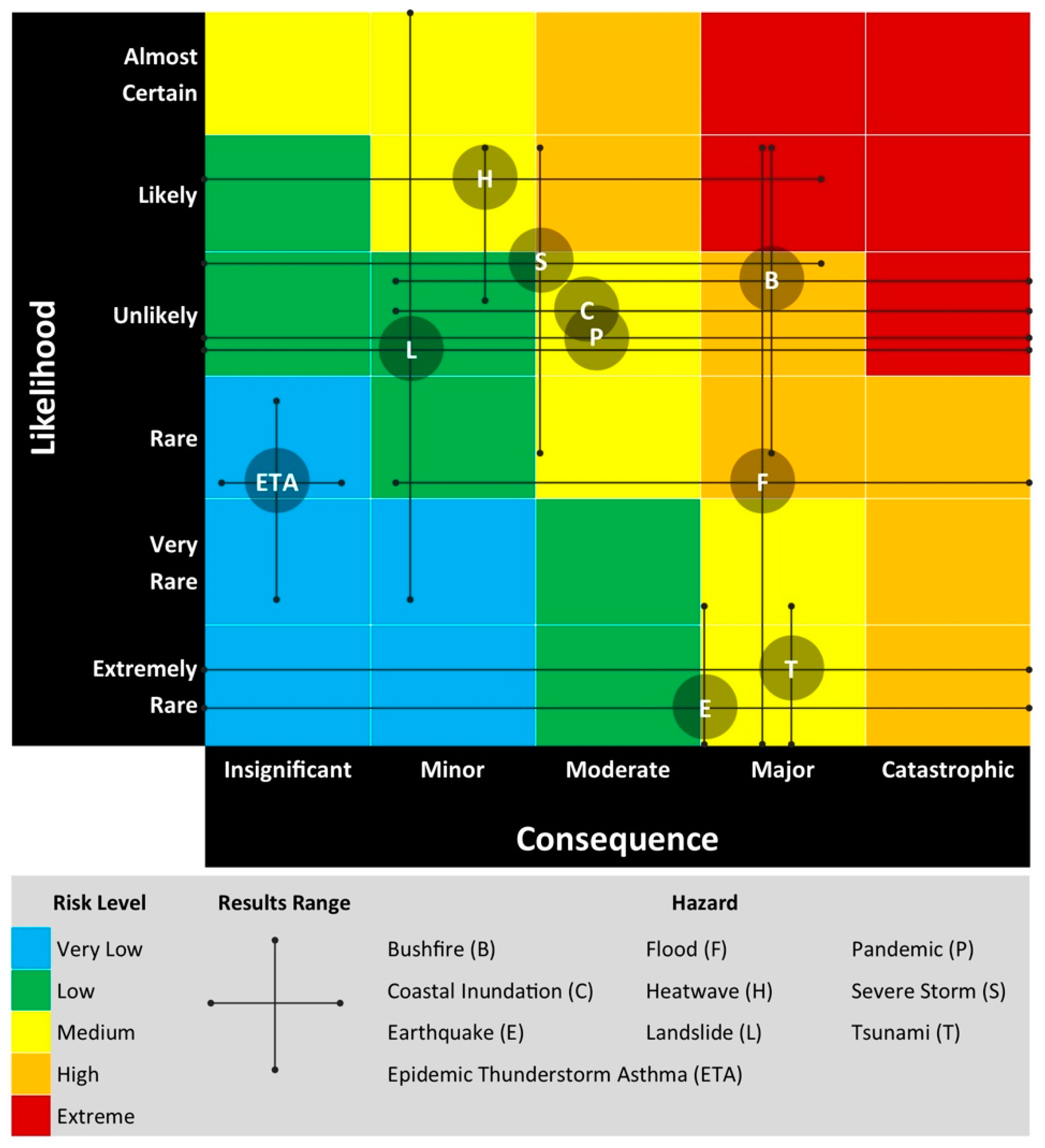
2.4. Risk Assessment
3. Results
3.1. Health Outcomes and Meteorological Data
3.2. Risk Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Victorian Government. The November 2016 Victorian Epidemic Thunderstorm Asthma Event: An Assessment of the Health Impacts; Department of Health and Human Services: Melbourne, Australia, 2017.
- Marks, G.B.; Bush, R.K. It’s blowing in the wind: New insights into thunderstorm-related asthma. J. Allergy Clin. Immunol. 2007, 120, 530–532. [Google Scholar] [CrossRef] [PubMed]
- Marks, G.B.; Colquhoun, J.R.; Girgis, S.T.; Koski, M.H.; Treloar, A.B.A.; Hansen, P.; Downs, S.H.; Car, N.G. Thunderstorm outflows preceding epidemics of asthma during spring and summer. Thorax 2001, 56, 468–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, P.E.; Jonsson, H. Thunderstorm asthma. Curr. Allergy Asthma Rep. 2004, 4, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.M.; Erbas, B.; Simunovic, M.; Al Kouba, J.; Milic, A.; Fagan, D. Literature Review on Thunderstorm Asthma and Its Implications for Public Health Advice; Queensland University of Technology: Brisbane, Australia, 2017. [Google Scholar]
- Dabrera, G.; Murray, V.; Emberlin, J.; Ayres, J.G.; Collier, C.; Clewlow, Y.; Sachon, P. Thunderstorm asthma: An overview of the evidence base and implications for public health advice. QJM Int. J. Med. 2013, 106, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Thien, F.; Beggs, P.J.; Csutoros, D.; Darvall, J.; Hew, M.; Davies, J.M.; Bardin, P.G.; Bannister, T.; Barnes, S.; Bellomo, R.; et al. The Melbourne epidemic thunderstorm asthma event 2016: An investigation of environmental triggers, effect on health services, and patient risk factors. Lancet Planet. Health 2018, 2, e255–e263. [Google Scholar] [CrossRef]
- Wood, S. Thunderstorm Asthma: The Night a Deadly Storm Took Melbourne’s Breath Away. 2017. Available online: www.smh.com.au/lifestyle/thunderstorm-asthma-the-night-a-deadly-storm-took-melbournes-breath-away-20170308-gut8ur.html (accessed on 10 March 2017).
- Davey, M. Thunderstorm Asthma: ‘You’re Talking an Event Equivalent to a Terrorist Attack’. 2016. Available online: https://www.theguardian.com/australia-news/2016/nov/27/thunderstorm-asthma-oure-talking-an-event-equivalent-to-a-terrorist-attack (accessed on 29 November 2016).
- Marks, G.B. It’s Not Just about Melbourne: Why We Need a National Approach to ‘Thunderstorm Asthma’. 2016. Available online: https://theconversation.com/its-not-just-about-melbourne-why-we-need-a-national-approach-to-thunderstorm-asthma-69426 (accessed on 27 November 2016).
- Victorian Government. Department of Health and Human Services Policy and Funding Guidelines; Department of Health and Human Services: Melbourne, Australia, 2017.
- Grundstein, A.; Shepherd, M.; Miller, P. The Role of Mesoscale-Convective Processes in Explaining the 21 November 2016 Epidemic Thunderstorm Asthma Event in Melbourne, Australia. J. Appl. Meteorol. Climatol. 2017, 56, 1337. [Google Scholar] [CrossRef]
- Department of Premier and Cabinet. TasALERT—Thunderstorm Asthma. Available online: https://www.facebook.com/tasalert/posts/1733972686615172 (accessed on 25 March 2018).
- Billings, P. High Pollen Count and Forecast Thunderstorm Combine to Create Severe Asthma Risk in Southern Tasmania. 2017. Available online: www.themercury.com.au/news/tasmania/high-pollen-count-and-forecast-thunderstorm-combine-to-create-severe-asthma-risk-in-southern-tasmania/news-story/21be2d1cd7a5212d7b90e0b5090b03c5 (accessed on 15 November 2017).
- Monery, H. Tasmania Issued Thunderstorm Asthma Warning. 2017. Available online: http://www.examiner.com.au/story/5057451/thunderstorm-asthma-warning-issued-for-people-across-tasmania (accessed on 15 November 2017).
- Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS): Volume 5—Remoteness Structure Commonwealth Government; Australian Bureau of Statistics: Canberra, Australia, 2011; Volume 1270.0.55.005.
- Australian Bureau of Statistics. 2016 Census; Commonwealth Government: Canberra, Australia, 2017.
- Kuleshov, Y.; de Hoedt, G.; Wright, W.; Brewster, A. Thunderstorm distribution and frequency in Australia. Aust. Meteorol. Mag. 2002, 51, 145. [Google Scholar]
- Allen, J.T.; Karoly, D.J. A climatology of Australian severe thunderstorm environments 1979–2011: Inter-annual variability and ENSO influence. Int. J. Climatol. 2014, 34, 81–97. [Google Scholar] [CrossRef]
- Jones, M. Tornadoes and waterspouts in northern Tasmania. Meteorol. Note 1990, 192, 1–28. [Google Scholar]
- Bellomo, R.; Gigliotti, P.; Treloar, A.; Holmes, P.; Suphioglu, C.; Singh, M.B.; Knox, B. Two consecutive thunderstorm associated epidemics of asthma in the City of Melbourne. The possible role of ryegrass pollen. Med. J. Aust. 1992, 156, 834–837. [Google Scholar] [PubMed]
- Haberle, S.; Bowman, D.; Newnham, R.; Johnston, F.; Beggs, P.; Buters, J.; Campbell, B.; Erbas, B.; Godwin, I.; Green, B.J.; et al. The macroecology of airborne pollen in Australian and New Zealand urban areas. PLoS ONE 2014, 9, e97925. [Google Scholar] [CrossRef] [PubMed]
- Tng, D.Y.P.; Hopf, F.; Haberle, S.G.; Bowman, D.M.J.S. Seasonal pollen distribution in the atmosphere of Hobart, Tasmania: Preliminary observations and congruence with flowering phenology. Aust. J. Bot. 2010, 58, 440–452. [Google Scholar] [CrossRef]
- Johnston, F.H.; Wheeler, A.J.; Williamson, G.J.; Campbell, S.L.; Jones, P.J.; Koolhof, I.S.; Lucani, C.; Cooling, N.B.; Bowman, D.M.J.S. Using smartphone technology to reduce health impacts from atmospheric environmental hazards. Environ. Res. Lett. 2018, 13, 044019. [Google Scholar] [CrossRef] [Green Version]
- Lane, P.; Morris, D.; Bridle, K.; Eyles, A. Common Grasses: An Agriculturalists’ Guide; Cradle Coast NRM, NRM North, NRM South and the University of Tasmania: Hobart, Australia, 2015. [Google Scholar]
- White, C.; Remenyi, T.; McEvoy, D.; Trundle, A.; Corney, S. 2016 Tasmanian State Natural Disaster Risk Assessment; University of Tasmania: Tasmania, Australia, 2016. [Google Scholar]
- Commonwealth of Australia. National Emergency Risk Assessment Guidelines—Handbook 10; Australian Institute for Disaster Resilience, Attorney General’s Department: Canberra, Australia, 2015.
- Organisation for Economic Cooperation and Development. National Risk Assessments: A Cross Country Perspective; OECD Publishing: Paris, France, 2018. [Google Scholar] [CrossRef]
- Federal Office for Civil Protection. Disasters and Emergencies in Switzerland 2015; Federal Office for Civil Protection: Bern, Switzerland, 2015. [Google Scholar]
- Noji, E.K. The Public Health Consequences of Disasters. Prehospit. Disaster Med. 2000, 15, 21–31. [Google Scholar] [CrossRef]
- Commonwealth of Australia. Australian Disaster Resilience Handbook 1: Disaster Health; Australian Institute for Disaster Resilience, Attorney General’s Department: Canberra, Australia, 2011. [Google Scholar]
- Thornley, L.; Ball, J.; Signal, L.; Lawson-Te Aho, K.; Rawson, E. Building community resilience: Learning from the Canterbury earthquakes. Kōtuitui N. Z. J. Soc. Sci. Online 2015, 10, 23–35. [Google Scholar] [CrossRef]
- Silverman, R.A.; Stevenson, L.; Hastings, H.M. Age-related seasonal patterns of emergency department visits for acute asthma in an urban environment. Ann. Emerg. Med. 2003, 42, 577–586. [Google Scholar] [CrossRef]
- Lincoln, D.; Morgan, G.; Sheppeard, V.; Jalaludin, B.; Corbett, S.; Beard, J. Childhood asthma and return to school in Sydney, Australia. Public Health 2006, 120, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-H.; Xirasagar, S.; Lin, H.-C. Seasonality in Adult Asthma Admissions, Air Pollutant Levels, and Climate: A Population-based Study. J. Asthma 2006, 43, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Silver, J.; Sutherland, M.; Johnston, F.; Lampugnani, E.; McCarthy, M.; Jacobs, S.; Pezza, A.; Newbigin, E. Seasonal asthma in Melbourne, Australia, and some observations on the occurrence of thunderstorm asthma and its predictability. PLoS ONE 2018, 13, e0194929. [Google Scholar] [CrossRef] [PubMed]
- Norwegian Directorate for Civil Protection. National Risk Analysis; Norwegian Government: Tønsberg, Norway, 2014.
- Ilias, I. Eight year retrospective study of thunderstorm-associated asthma attacks in Athens Greece. Int. J. Environ. Health Res. 1998, 8, 335–337. [Google Scholar] [CrossRef]
- Higham, J.; Venables, K.; Kupek, E.; Bajekal, M.; Kopek, E. Asthma and thunderstorms: Description of an epidemic in general practice in Britain using data from a doctors’ deputising service in the UK. J. Epidemiol. Community Health 1997, 51, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. National Health Survey 2014–15; Commonwealth Government: Canberra, Australia, 2015.
- Department of Health and Human Services. Report on the Tasmanian Population Health Survey 2016; Tasmanian Government: Hobart, Australia, 2017.
- Australian Bureau of Statistics. ABS 3303.0 Causes of Death, Tasmania; Australian Government, 2016.
- Lake, I.R.; Jones, N.R.; Agnew, M.; Goodess, C.M.; Giorgi, F.; Hamaoui-Laguel, L.; Semenov, M.A.; Solomon, F.; Storkey, J.; Vautard, R.; et al. Climate Change and Future Pollen Allergy in Europe. Environ. Health Perspect. 2017, 125, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Anenberg, S.; Weinberger, K.R.; Roman, H.; Neumann, J.E.; Crimmins, A.; Fann, N.; Martinich, J.; Kinney, P.L. Impacts of oak pollen on allergic asthma in the USA and potential effect of future climate change: A modelling analysis. Lancet 2017, 389, S2. [Google Scholar] [CrossRef]
- Walsh, K.J.E.; White, C.J.; McInnes, K.L.; Holmes, J.; Schuster, S.; Richter, H.; Evans, J.P.; Di Luca, A.; Warren, R.A. Natural hazards in Australia: Storms, wind and hail. Clim. Chang. 2016, 139, 55–67. [Google Scholar] [CrossRef]
- Hoogewind, K.A.; Baldwin, M.E.; Trapp, R.J. The Impact of Climate Change on Hazardous Convective Weather in the United States: Insight from High-Resolution Dynamical Downscaling. J. Clim. 2017, 30, 10081–10100. [Google Scholar] [CrossRef]
- Romps, D.M.; Seeley, J.T.; Vollaro, D.; Molinari, J. Projected increase in lightning strikes in the United States due to global warming. Science 2014, 346, 851–854. [Google Scholar] [CrossRef]
- Press, A. Tasmanian Wilderness World Heritage Area Bushfire and Climate Change Research Project; Tasmanian Government: Hobart, Australia, 2016.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hospital | Total Presentations | Daily Mean 1 | Daily Maximum | No. of Case Days | No. of Control Days |
|---|---|---|---|---|---|
| Royal Hobart | 7268 | 1.37 | 7 | 10 | 40 |
| Launceston General | 5807 | 1.09 | 8 | 16 | 64 |
| MCH/NWRH 2 combined | 6904 | 1.30 | 11 | 11 | 44 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campbell, S.L.; Fox-Hughes, P.D.; Jones, P.J.; Remenyi, T.A.; Chappell, K.; White, C.J.; Johnston, F.H. Evaluating the Risk of Epidemic Thunderstorm Asthma: Lessons from Australia. Int. J. Environ. Res. Public Health 2019, 16, 837. https://doi.org/10.3390/ijerph16050837
Campbell SL, Fox-Hughes PD, Jones PJ, Remenyi TA, Chappell K, White CJ, Johnston FH. Evaluating the Risk of Epidemic Thunderstorm Asthma: Lessons from Australia. International Journal of Environmental Research and Public Health. 2019; 16(5):837. https://doi.org/10.3390/ijerph16050837
Chicago/Turabian StyleCampbell, Sharon L., Paul D. Fox-Hughes, Penelope J. Jones, Tomas A. Remenyi, Kate Chappell, Christopher J. White, and Fay H. Johnston. 2019. "Evaluating the Risk of Epidemic Thunderstorm Asthma: Lessons from Australia" International Journal of Environmental Research and Public Health 16, no. 5: 837. https://doi.org/10.3390/ijerph16050837