Population Health Inequalities Across and Within European Metropolitan Areas through the Lens of the EURO-HEALTHY Population Health Index


 ,
,  , , ,
, , , 

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
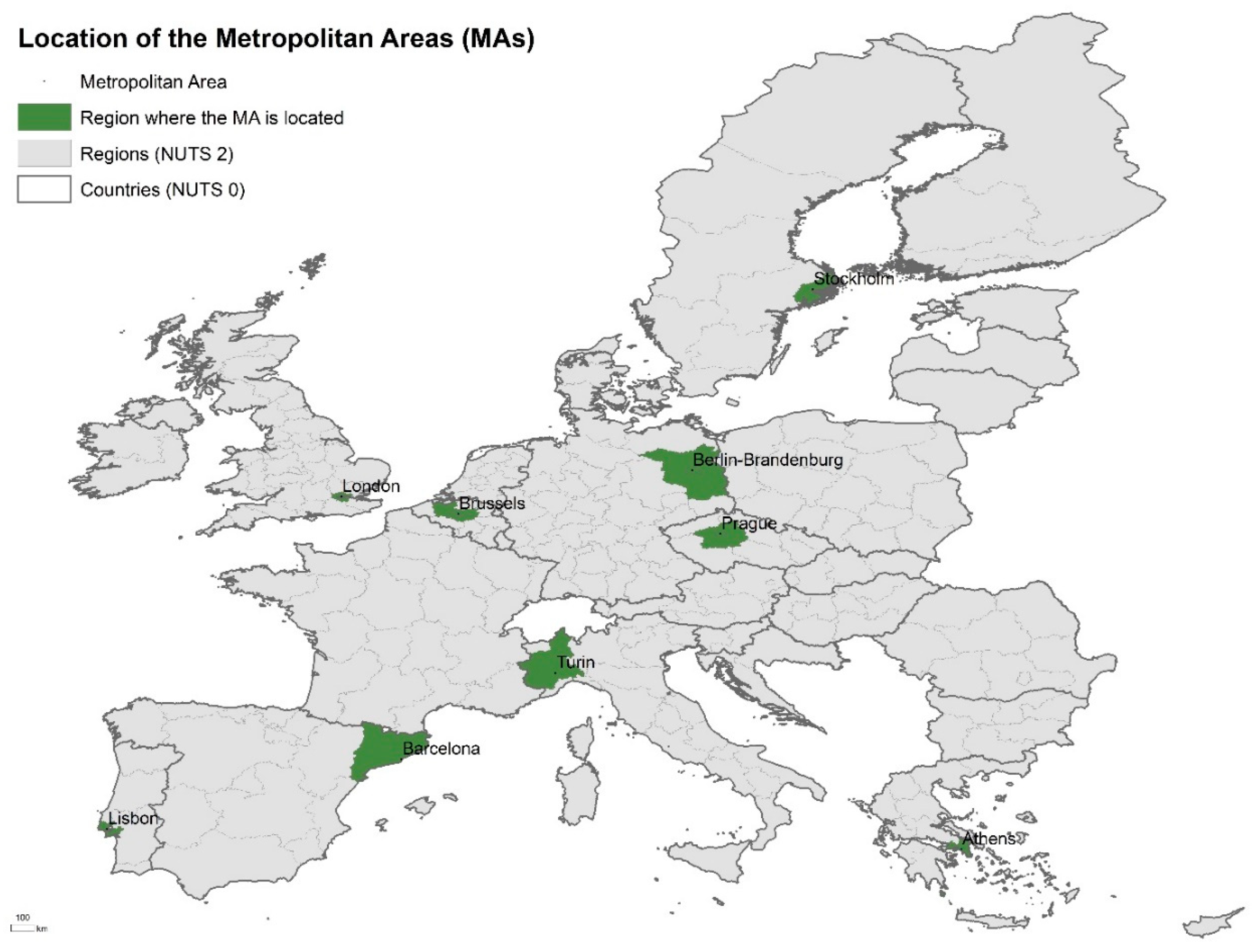
2.1. Study Area
2.2. Applying the Population Health Index
Indicators
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Prasad, A. The Urban Health Equity Assessment and Response Tool (HEART)—A Decade of Development and Implementation. J. Urban Health 2018, 95, 609. [Google Scholar] [CrossRef] [PubMed]
- Corburn, J. Urban Place and Health Equity: Critical Issues and Practices. Int. J. Environ. Res. Public Health 2017, 14, 117. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Report on Urban Health; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Giles-Corti, B.; Vernez-Moudon, A.; Reis, R.; Turrell, G.; Dannenberg, A.L.; Badland, H.; Foster, S.; Lowe, M.; Sallis, J.F.; Stevenson, M.; et al. City planning and population health: A global challenge. Lancet 2016, 388, 2912–2924. [Google Scholar] [CrossRef]
- Marmot, M.; Bell, R. The Sustainable Development Goals and Health Equity. Epidemiology 2018, 29, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Grant, M. Planning for Healthy Cities. In Integrating Human Health into Urban and Transport Planning; Springer International Publishing: Cham, Switzerland, 2019; pp. 221–250. [Google Scholar]
- Singh, S.; Beagley, J. Health and the New Urban Agenda: A mandate for action. Lancet 2017, 389, 801–802. [Google Scholar] [CrossRef]
- Takano, T.; Nakamura, K. An analysis of health levels and various indicators of urban environments for Healthy Cities projects. J. Epidemiol. Community Health 2001, 55, 263–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vardoulakis, S.; Dimitroulopoulou, S.; Mitsakou, C.; Heaviside, C.; Katsouyanni, K.; Samoli, E.; Santana, P. Developing Environmental Public Health Indicators for European Metropolitan Areas. In Proceedings of the International Conference on Urban Risks, Lisbon, Portugal, 30 June–2 July 2016. [Google Scholar]
- Lawrence, R.J. Urban Health Challenges in Europe. J. Urban Health 2013, 90, 23. [Google Scholar] [CrossRef] [PubMed]
- Harpham, T. Urban health in developing countries: What do we know and where do we go? Health Place 2009, 15, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.; Vlahov, D. URBAN HEALTH: Evidence, Challenges, and Directions. Annu. Rev. Public Health 2005, 26, 341–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borrell, C.; Pons-Vigués, M.; Morrison, J.; Díez, È. Factors and processes influencing health inequalities in urban areas. J. Epidemiol. Community Health 2013, 67, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Corburn, J. City planning as preventive medicine. Prev. Med. 2015, 77, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Ompad, D.C.; Galea, S.; Caiaffa, W.T.; Vlahov, D. Social Determinants of the Health of Urban Populations: Methodologic Considerations. J. Urban Health 2007, 84, 42–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahlgren, G.; Whitehead, M. Policies and Strategies to Promote Social Equity in Health; The Institute for Futures Studies: Stockholm, Sweden, 1991. [Google Scholar]
- Dahlgren, G.; Whitehead, M. European Strategies for Tackling Social Inequities in Health: Levelling Up Part 2; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Mitsakou, C.; Dimitroulopoulou, S.; Heaviside, C.; Katsouyanni, K.; Samoli, E.; Rodopoulou, S.; Costa, C.; Almendra, R.; Santana, P.; Dell’Olmo, M.M.; et al. Environmental public health risks in European metropolitan areas within the EURO-HEALTHY project. Sci. Total Environ. 2019, 658, 1630–1639. [Google Scholar] [CrossRef] [PubMed]
- Santana, P.; Costa, C.; Cardoso, G.; Loureiro, A.; Ferrão, J. Suicide in Portugal: Spatial determinants in a context of economic crisis. Health Place 2015, 35, 85–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diez Roux, A.V. Investigating Neighborhood and Area Effects on Health. Am. J. Public Health 2001, 91, 1783–1789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santana, P.; Costa, C.; Marí-Dell’Olmo, M.; Gotsens, M.; Borrell, C. Mortality, material deprivation and urbanization: Exploring the social patterns of a metropolitan area. Int. J. Equity Health 2015, 14, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Cummins, S.; Curtis, S.; Diez-Roux, A.V.; Macintyre, S. Understanding and representing ‘place’ in health research: A relational approach. Soc. Sci. Med. 2007, 65, 1825–1838. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, S.; Ellaway, A.; Hiscock, R.; Kearns, A.; Der, G.; McKay, L. What features of the home and the area might help to explain observed relationships between housing tenure and health? Evidence from the west of Scotland. Health Place 2003, 9, 207–218. [Google Scholar] [CrossRef]
- Vlahov, D.; Freudenberg, N.; Proietti, F.; Ompad, D.; Quinn, A.; Nandi, V.; Galea, S. Urban as a determinant of health. J. Urban Health 2007, 84 (Suppl. 1), 16–26. [Google Scholar] [CrossRef] [PubMed]
- Vlahov, D.; Caiaffa, W.T. Healthy urban governance and population health. Participatory budgeting in Belo Horizonte, Brazil. In The Urban Transformation: Health, Shelter and Climate Change; Sclar, E., Volavka-Close, N., Brown, P., Eds.; Routledge: Abington-on-Thames, UK, 2013; p. 232. ISBN 9781849712163. [Google Scholar]
- World Health Organization. Unmasking and Overcoming Health in urban settings. In Unmasking and Overcoming Health in Urban Settings; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Loureiro, A.; Costa, C.; Almendra, R.; Freitas, Â.; Santana, P.; Loureiro, A.; Costa, C.; Almendra, R.; Freitas, Â.; Santana, P. The socio-spatial context as a risk factor for hospitalization due to mental illness in the metropolitan areas of Portugal. Cad. Saude Publica 2015, 31, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, R.; Borsboom, G.; Saez, M.; Dell’Olmo, M.; Burström, B.B.; Corman, D.; Costa, C.; Deboosere, P.; Domínguez-Berjón, M.F.; Dzúrová, D.; et al. Social differences in avoidable mortality between small areas of 15 European cities: An ecological study. Int. J. Health Geogr. 2014, 13, 8. [Google Scholar] [CrossRef] [PubMed]
- Gotsens, M.; Marí-Dell’Olmo, M.; Pérez, K.; Palência, L.; Martinez-Beneito, M.-A.; Rodríguez-Sanz, M.; Burstrom, B.; Costa, G.; Deboosere, P.; Domínguez-Berjón, F.; et al. Socioeconomic inequalities in injury mortality in small areas of 15 European cities. Health Place 2013, 24, 165–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolasco, A.; Moncho, J.; Quesada, J.A.; Melchor, I.; Pereyra-Zamora, P.; Tamayo-Fonseca, N.; Martínez-Beneito, M.A.; Zurriaga, O.; Ballesta, M.; Daponte, A.; et al. Trends in socioeconomic inequalities in preventable mortality in urban areas of 33 Spanish cities, 1996–2007 (MEDEA project). Int. J. Equity Health 2015, 14, 33. [Google Scholar] [CrossRef] [PubMed]
- Santana, P.; Costa, C.; Freitas, Â.; Stefanik, I.; Quintal, C.; Bana e Costa, C.; Borrell, C.; Dimitroulopoulou, C.; Ferreira, P.; Krafft, T.; et al. Atlas of Population Health in European Union Regions; Santana, P., Ed.; Imprensa da Universidade de Coimbra: Coimbra, Portugal, 2017; ISBN 978-989-26-1462-5. [Google Scholar]
- O’Reilly, G.; O’Reilly, D.; Rosato, M.; Connolly, S. Urban and rural variations in morbidity and mortality in Northern Ireland. BMC Public Health 2007, 7, 123. [Google Scholar] [CrossRef] [PubMed]
- Gartner, A.; Farewell, D.; Roach, P.; Dunstan, F. Rural/urban mortality differences in England and Wales and the effect of deprivation adjustment. Soc. Sci. Med. 2011, 72, 1685–1694. [Google Scholar] [CrossRef] [PubMed]
- Mari-Dell’Olmo, M.; Gotsens, M.; Palencia, L.; Burstrom, B.; Corman, D.; Costa, G.; Deboosere, P.; Diez, E.; Dominguez-Berjon, F.; Dzurova, D.; et al. Socioeconomic inequalities in cause-specific mortality in 15 European cities. J. Epidemiol. Community Health 2015, 69, 432–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borrell, C.; Mari-Dell’olmo, M.; Palencia, L.; Gotsens, M.; Burstrom, B.; Dominguez-Berjon, F.; Rodriguez-Sanz, M.; Dzurova, D.; Gandarillas, A.; Hoffmann, R.; et al. Socioeconomic inequalities in mortality in 16 European cities. Scand. J. Public Health 2014, 42, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Baum, F. Cracking the nut of health equity: Top down and bottom up pressure for action on the social determinants of health. Promot. Educ. 2007, 14, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Fosse, E.; Helgesen, M.K.; Hagen, S.; Torp, S. Addressing the social determinants of health at the local level: Opportunities and challenges. Scand. J. Public Health 2018, 46, 47–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bambra, C.; Gibson, M.; Sowden, A.; Wright, K.; Whitehead, M.; Petticrew, M. Tackling the wider social determinants of health and health inequalities: Evidence from systematic reviews. J. Epidemiol. Community Health 2010, 64, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Tallarek née Grimm, M.J.; Helgesen, M.K.; Fosse, E. Reducing social inequities in health in Norway: Concerted action at state and local levels? Health Policy 2013, 113, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Morrison, J.; Pons-Vigués, M.; Bécares, L.; Burström, B.; Gandarillas, A.; Domínguez-Berjón, F.; Diez, E.; Costa, G.; Ruiz, M.; Pikhart, H.; et al. Health inequalities in European cities: Perceptions and beliefs among local policymakers. BMJ Open 2014, 4, e004454. [Google Scholar] [CrossRef] [PubMed]
- Newman, L.; Baum, F.; Javanparast, S.; O’Rourke, K.; Carlon, L. Addressing social determinants of health inequities through settings: A rapid review. Health Promot. Int. 2015, 30, ii126–ii143. [Google Scholar] [CrossRef] [PubMed]
- Vlahov, D. Urban Health: Global Perspectives; Jossey-Bass: San Francisco, CA, USA, 2010; ISBN 9780470422069. [Google Scholar]
- Prasad, A.; Gray, C.B.; Ross, A.; Kano, M. Metrics in Urban Health: Current Developments and Future Prospects. Annu. Rev. Public Health 2016, 37, 113–133. [Google Scholar] [CrossRef] [PubMed]
- Rothenberg, R.; Weaver, S.R.; Dai, D.; Stauber, C.; Prasad, A.; Kano, M. A Flexible Urban Health Index for Small Area Disparities. J. Urban Health 2014, 91, 823–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitas, Â.; Santana, P.; Oliveira, M.D.; Almendra, R.; Bana e Costa, J.C.; Bana e Costa, C.A. Indicators for evaluating European population health: A Delphi selection process. BMC Public Health 2018, 18, 557. [Google Scholar] [CrossRef] [PubMed]
- Bana e Costa, C.; Freitas, L.; Oliveira, M.; Rodrigues, T.; Vieira, A. Using the MACBETH socio-technical methodological approach to build the EURO-HEALTHY PHI. In Promoting Population Health and Equity in Europe: From Evidence to Policy; Coimbra University Press: Coimbra, Portugal, 2017. [Google Scholar]
- Sohn, C.; Stambolic, N. The urban development of European border regions: A spatial typology. Eur. Reg. 2013, 21, 177–189. [Google Scholar]
- Bana e Costa, C.; De Corte, J.-M.; Vansnick, J.-C. MACBETH. Int. J. Inf. Technol. Decis. Mak. 2012, 11, 359–387. [Google Scholar] [CrossRef]
- Stefanik, I.; Freitas, Â.; Doetsch, J.; Santana, P. Involving key stakeholders in the EURO-HEALTH. In Promoting Population Health and Equity in Europe: From Evidence to Policy; Coimbra University Press: Coimbra, Portugal, 2017. [Google Scholar]
- Diz, P.; Meleti, M.; Diniz-Freitas, M.; Vescovi, P.; Warnakulasuriya, S.; Johnson, N.W.; Kerr, A.R. Oral and pharyngeal cancer in Europe. Transl. Res. Oral Oncol. 2017. [Google Scholar] [CrossRef]
- Pons-Vigués, M.; Diez, E.; Morrison, J.; Salas-Nicás, S.; Hoffmann, R.; Burstrom, B.; van Dijk, J.P.; Borrell, C. Social and health policies or interventions to tackle health inequalities in European cities: A scoping review. BMC Public Health 2014, 14, 198. [Google Scholar] [CrossRef] [PubMed]
- Dragano, N.; Bobak, M.; Wege, N.; Peasey, A.; Verde, P.E.; Kubinova, R.; Weyers, S.; Moebus, S.; Möhlenkamp, S.; Stang, A.; et al. Neighbourhood socioeconomic status and cardiovascular risk factors: A multilevel analysis of nine cities in the Czech Republic and Germany. BMC Public Health 2007, 7, 255. [Google Scholar] [CrossRef] [PubMed]
- Bosakova, L.; Rosicova, K.; Filakovska Bobakova, D.; Rosic, M.; Dzurova, D.; Pikhart, H.; Lustigova, M.; Santana, P. Mortality in the Visegrad countries from the perspective of socioeconomic inequalities. Int. J. Public Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Samoli, E.; Stergiopoulou, A.; Santana, P.; Rodopoulou, S.; Mitsakou, C.; Dimitroulopoulou, C.; Bauwelinck, M.; de Hoogh, K.; Costa, C.; Marí-Dell’Olmo, M.; et al. Spatial variability in air pollution exposure in relation to socioeconomic indicators in nine European metropolitan areas: A study on environmental inequality. Environ. Pollut. 2019. under review. [Google Scholar]
- Deboosere, P.; Eggerickx, T.; Van Hecke, E.; Wayens, B. The population of Brussels: A demographic overview. Brussels Stud. 2009, 3. [Google Scholar] [CrossRef]
- Schuurman, N.; Bell, N.; Dunn, J.R.; Oliver, L. Deprivation Indices, Population Health and Geography: An Evaluation of the Spatial Effectiveness of Indices at Multiple Scales. J. Urban Health 2007, 84, 591–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stauber, C.; Adams, E.A.; Rothenberg, R.; Dai, D.; Luo, R.; Weaver, S.R.; Prasad, A.; Kano, M.; Heath, J. Measuring the Impact of Environment on the Health of Large Cities. Int. J. Environ. Res. Public Health 2018, 15, 1216. [Google Scholar] [CrossRef] [PubMed]
- Jollands, N.; Lermit, J.; Patterson, M. The Usefulness of Aggregate Indicators in Policy Making and Evaluation: A Discussion with Application to Eco-Efficiency Indicators in New Zealand; Australian National University Digital Collections: Palmerston North, New Zealand, 2003. [Google Scholar]
- Openshaw, S. The Modifiable Areal Unit Problem. Concepts and Techniques in Modern Geography; Geobooks: Norwich, UK, 1984. [Google Scholar]
- Corburn, J.; Cohen, A.K. Why We Need Urban Health Equity Indicators: Integrating Science, Policy, and Community. PLoS Med. 2012, 9, e1001285. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Closing the Gap: Policy into Practice on Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2011; ISBN 978 92 4 150240 5.
- Marmot, M.; Friel, S.; Bell, R.; Houweling, T.A.; Taylor, S.; CSDH; Marmot, M.; World Health Organization. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; Elsevier: Geneva, Switzerland, 2008; Volume 372. [Google Scholar]
- Costa, C.; Freitas, Â.; Stefanik, I.; Krafft, T.; Pilot, E.; Morrison, J.; Santana, P. Evaluation of data availability on population health indicators at regional level across the European Union. Popul. Health Metr. 2019. under review. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metropolitan Area | Area (km2) | Density (Inhabitants/km2) | Population (Inhabitants) | Population +65 (%) | Population Range (Inhabitants) |
|---|---|---|---|---|---|
| Athens | 403 | 7669 | 3,090,508 | 17.8 | 25,389–664,046 |
| Barcelona | 420 | 7590 | 3,103,973 | 18.9 | 13,531–1,611,822 |
| Berlin—Brandenburg | 16,669 | 352 | 5,871,022 | 20.7 | 58,018–371,438 |
| Brussels | 3591 | 698 | 2,504,715 | 16.1 | 2160–176,545 |
| Prague | 315 | 3737 | 1,177,141 | 18.5 | 6021–128,063 |
| Lisbon | 2917 | 966 | 2,821,876 | 18.2 | 17,569–547,733 |
| London | 1468 | 5733 | 8,416,543 | 11.4 | 7648–372,752 |
| Stockholm | 6011 | 348 | 2,091,449 | 15.2 | 9331–864,315 |
| Turin | 1000 | 1620 | 1,619,478 | 24.8 | 1200–886,837 |
| Component: Health Determinants | ||
|---|---|---|
| Area of Concern | Dimension | Indicator |
| Economic conditions, social protection and security | Employment | Unemployment rate (%) |
| Long-term unemployment rate (%) | ||
| Income and Living conditions | Disposable income of private households per capita (Euro per inhabitant) | |
| People at risk of poverty or social exclusion (%) | ||
| Disposable income ratio—S80/S20 | ||
| Social protection | Expenditure on care for the elderly (% of GDP) | |
| Security | Crimes recorded by the police (per 100,000 inhabitants) | |
| Education | Education | Population aged 25–64 with upper secondary or tertiary education attainment (%) |
| Early leavers from education and training (%) | ||
| Demographic change | Ageing | At risk of poverty rate of older people (%) |
| Ageing index (ratio) | ||
| Lifestyle and health behaviours | Lifestyle and health behaviours | Adults who are obese (%) |
| Daily smokers—aged 15 and over (%) | ||
| Pure alcohol consumption—aged 15 and over (Litres per capita) | ||
| Live births by mothers under age of 20 (%) | ||
| Physical environment | Pollution | Annual mean of daily PM2.5 concentrations (ug/m3) |
| Annual mean of daily PM10 concentrations (ug/m3) | ||
| Greenhouse Gas (total tonnes of CO2 eq. emissions per capita) | ||
| Built environment | Housing conditions | Average number of rooms per person |
| Households without indoor flushing toilet (%) | ||
| Households without central heating (%) | ||
| Water and sanitation | Population connected to public water supply (%) | |
| Population connected to wastewater treatment plants (%) | ||
| Recycling | Recycling rate of municipal waste (%) | |
| Road safety | Road safety | Victims of road accidents—injured and killed (per 100,000 inhabitants) |
| Fatality rate due to road traffic accidents (per 1000 victims) | ||
| Healthcare resources and expenditure | Healthcare resources | Medical doctors (per 100,000 inhabitants) |
| Health personnel—nurses and midwives, dentists, pharmacists and physiotherapists (per 100,000 inhabitants) | ||
| Healthcare expenditure | Total health expenditure (Purchasing Power Parity per capita) | |
| Private households’ out-of-pocket expenses on health (% total health expenditure) | ||
| Total health expenditure (Purchasing Power Parity per capita) | ||
| Healthcare performance | Healthcare performance | Hospital discharges due to diabetes, hypertension and asthma (per 100,000 inhabitants) |
| Amenable deaths due to healthcare (standardized death rate per 100,000 inhabitants) | ||
| Component: Health Outcomes | ||
| Health Outcomes | Morbidity | Self-perceived health less than good (%) |
| Age-standardised Disability-Adjusted Life Year (DALY) rate (per 100,000 inhabitants) | ||
| Low birth weight (%) | ||
| Mortality | Preventable deaths (standardised death rate per 100,000 inhabitants) | |
| Life expectancy at birth (years) | ||
| Infant mortality (per 1000 live births) | ||
| Group | MA | Stockholm | Athens | Barcelona | Lisbon | Berlin-Brand. | Brussels | London | Prague | Turin |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Stockholm |  | | | | | | | | |
| 2 | Athens |  |  | | | | | | | |
| Barcelona | |  | | | | | | | ||
| Lisbon | | | | | | | | | ||
| NA | Berlin-Brand. | | | | | | | | | |
| Brussels | | | | | | | | | ||
| London | | | | | | | | | ||
| Prague | | | | | | | | | ||
| Turin | | | | | | | | | ||
| Mean scores | 87.8 | 58.6 | 61.1 | 62.7 | 77.2 | 76.8 | 70.4 | 73.9 | 73.1 | |
and identify the metropolitan areas where scores were found to be statistically different. By way of example: Brussels presents mean scores that are statistically different from Athens, Barcelona, and Lisbon, London and Turin (with higher scores: ) and from Stockholm (with lower scores: ). The symbols and only display lower or higher differences (respectively), although not statistically significant. NA = No group was found.| Group | MA | Stockholm | Barcelona | Turin | Lisbon | Prague | Athens | Berlin-Brand. | Brussels | London |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Stockholm | | | | | | | | | |
| 2 | Barcelona | | | | | | | | | |
| Turin | | | | | | | | | ||
| 3 | Lisbon | | | | | | | | | |
| Prague | | | | | | | | | ||
| NA | Athens | | | | | | | | | |
| Berlin-Brand. | | | | | | | | | ||
| Brussels | | | | | | | | | ||
| London | | | | | | | | | ||
| Mean scores | 94.2 | 82.8 | 83.6 | 66.7 | 66.5 | 74.4 | 72.8 | 76.3 | 76.6 | |
and identify the metropolitan areas where scores were found to be statistically different. By way of example: Brussels presents mean scores that are statistically different from Stockholm, Turin, Lisbon, Prague and Berlin-Brandenburg (with higher scores: ) and from Barcelona (with lower scores: ). The symbols and only display lower or higher differences (respectively), although not statistically significant. NA = No group was found.© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, C.; Santana, P.; Dimitroulopoulou, S.; Burstrom, B.; Borrell, C.; Schweikart, J.; Dzurova, D.; Zangarini, N.; Katsouyanni, K.; Deboseree, P.; et al. Population Health Inequalities Across and Within European Metropolitan Areas through the Lens of the EURO-HEALTHY Population Health Index. Int. J. Environ. Res. Public Health 2019, 16, 836. https://doi.org/10.3390/ijerph16050836
Costa C, Santana P, Dimitroulopoulou S, Burstrom B, Borrell C, Schweikart J, Dzurova D, Zangarini N, Katsouyanni K, Deboseree P, et al. Population Health Inequalities Across and Within European Metropolitan Areas through the Lens of the EURO-HEALTHY Population Health Index. International Journal of Environmental Research and Public Health. 2019; 16(5):836. https://doi.org/10.3390/ijerph16050836
Chicago/Turabian StyleCosta, Claudia, Paula Santana, Sani Dimitroulopoulou, Bo Burstrom, Carme Borrell, Jürgen Schweikart, Dagmar Dzurova, Nicolás Zangarini, Klea Katsouyanni, Patrick Deboseree, and et al. 2019. "Population Health Inequalities Across and Within European Metropolitan Areas through the Lens of the EURO-HEALTHY Population Health Index" International Journal of Environmental Research and Public Health 16, no. 5: 836. https://doi.org/10.3390/ijerph16050836