
Childhood Reports of Food Neglect and Impulse Control Problems and Violence in Adulthood

Abstract
:1. Introduction
The Current Study
2. Materials and Methods
2.1. Participants
2.2. Diagnostic Assessment
2.3. Measures
2.3.1. Food Neglect/Frequent Hunger
2.3.2. Interpersonal Violence
2.3.3. Impulse-Control Deficits
2.3.4. Mental and Substance Use Disorders
2.3.5. Sociodemographic Factors
2.4. Analysis
3. Results
3.1. Characteristics of Individuals Reporting Frequent Exposure to Hunger
3.2. Is Frequent Hunger During Childhood Associated with Interpersonal Violence?
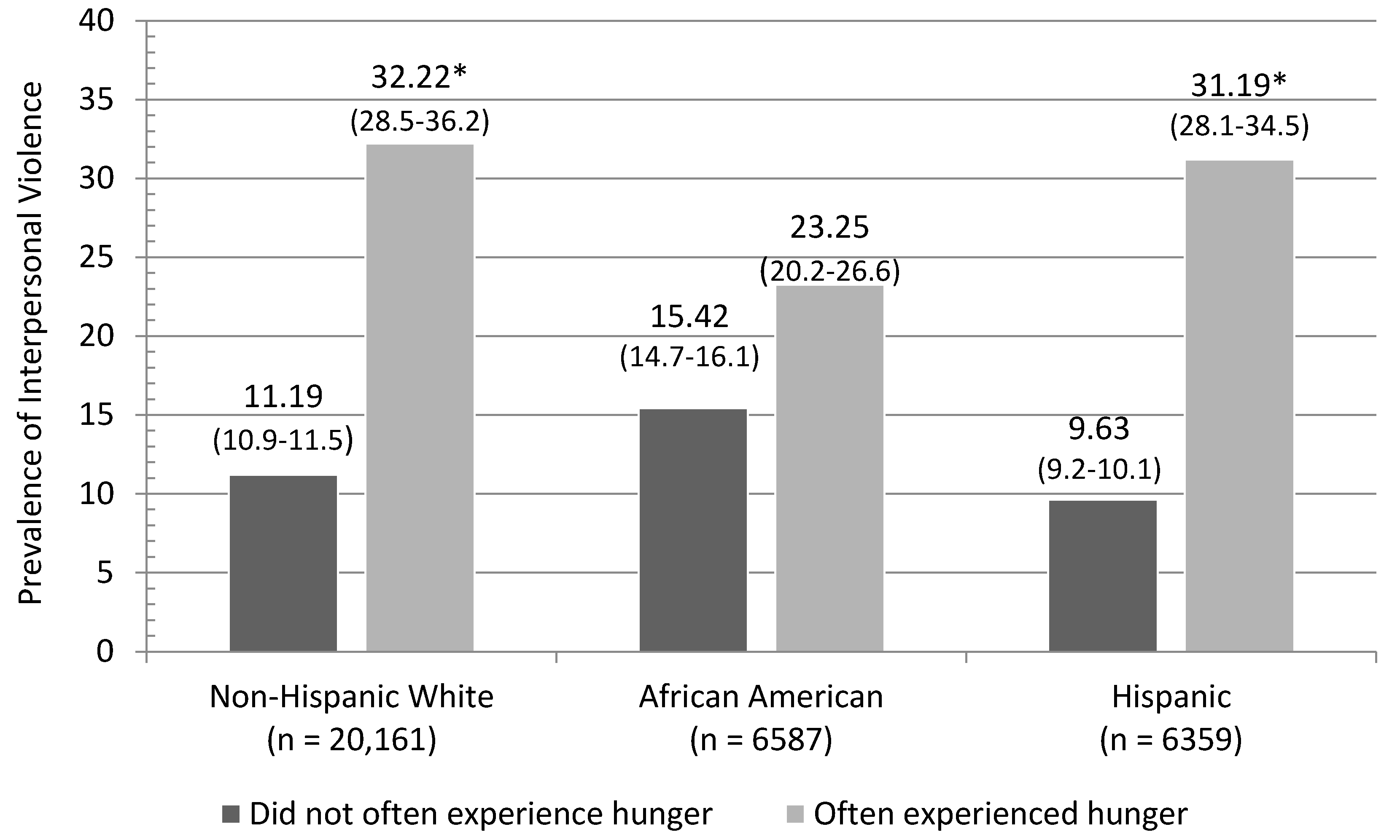
3.3. Does the Relationship Vary Across Gender and Race/Ethnicity?
3.4. Is There a Link Between Frequent Hunger and Impulse-Control Deficits?
4. Discussion
Study Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix
References
- Campbell, C.C. Food insecurity: A nutritional outcome or a predictor variable? J. Nutr. 1991, 121, 408–415. [Google Scholar] [PubMed]
- Gailliot, M. Race, crime, intellectual performance-and food: Poor nutrition con-tributes to racial differences in violence and SAT scores. Adv. Soc. Sci. Res. J. 2014, 1, 34–40. [Google Scholar]
- Georgieff, M.K. Nutrition and the developing brain: Nutrient priorities and measurement. Am. J. Clin. Nutr. 2007, 85, 614S–620S. [Google Scholar] [PubMed]
- Nord, M.; Andrews, M.; Carlson, S. Food Insecurity in the United States; United States Department of Agriculture: Washington, DC, USA, 2006. [Google Scholar]
- Timmer, C.P. Behavioral dimensions of food security. Proc. Natl. Acad. Sci. USA 2012, 109, 12315–12320. [Google Scholar] [CrossRef] [PubMed]
- Alaimo, K.; Olson, C.M.; Frongillo, E.A. Food insufficiency and American school-aged children’s cognitive, academic, and psychosocial development. Pediatrics 2001, 108, 44–53. [Google Scholar] [PubMed]
- Belsky, D.W.; Moffitt, T.E.; Arseneault, L.; Melchior, M.; Caspi, A. Context and sequelae of food insecurity in children’s development. Am. J. Epidemiol. 2010, 172, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Chilton, M.; Black, M.M.; Berkowitz, C.; Casey, P.H.; Cook, J.; Cutts, D.; Frank, D.A. Food insecurity and risk of poor health among US-born children of immigrants. Am. J. Public Health 2009, 99, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Chilton, M.; Chyatte, M.; Breaux, J. The negative effects of poverty & food insecurity on child development. Indian J. Med. Res. 2007, 126, 262–272. [Google Scholar] [PubMed]
- Cook, J.T.; Frank, D.A.; Berkowitz, C.; Black, M.M.; Casey, P.H.; Cutts, D.B.; Nord, M. Food insecurity is associated with adverse health outcomes among human infants and toddlers. J. Nutr. 2004, 134, 1432–1438. [Google Scholar] [PubMed]
- Jyoti, D.F.; Frongillo, E.A.; Jones, S.J. Food insecurity affects school children’s academic performance, weight gain, and social skills. J. Nutr. 2005, 135, 2831–2839. [Google Scholar] [PubMed]
- Kirkpatrick, S.I.; McIntyre, L.; Potestio, M.L. Child hunger and long-term adverse consequences for health. Arch. Pediatr. Adolesc. Med. 2010, 164, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Rose-Jacobs, R.; Black, M.M.; Casey, P.H.; Cook, J.T.; Cutts, D.B.; Chilton, M.; Frank, D.A. Household food insecurity: Associations with at-risk infant and toddler development. Pediatrics 2008, 121, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Wilde, P.E.; Peterman, J.N. Individual weight change is associated with household food security status. J. Nutr. 2006, 136, 1395–1400. [Google Scholar] [PubMed]
- Cecil, C.A.; Barker, E.D.; Jaffee, S.R.; Viding, E. Association between maladaptive parenting and child self-control over time: Cross-lagged study using a monozygotic twin difference design. Br. J. Psychiat. 2012, 201, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.B.; Beaver, K.M. A shared pathway of antisocial risk: A path model of parent and child effects. J. Crim. Justice 2015, 43, 154–163. [Google Scholar] [CrossRef]
- Moon, B.; McCluskey, J.D.; Blurton, D.; Hwang, H.W. Parent and teacher practices as sources of low self-control evidence from Korea. Youth Violence Juv. Justice 2014, 12, 167–187. [Google Scholar] [CrossRef]
- Vazsonyi, A.T.; Huang, L. Hirschi’s reconceptualization of self-control: Is truth truly the daughter of time? Evidence from eleven cultures. J. Crim. Justice 2015, 43, 59–68. [Google Scholar] [CrossRef]
- Meldrum, R.C.; Barnes, J.C.; Hay, C. Sleep deprivation, low self-control, and delinquency: A test of the strength model of self-control. J. Youth Adolesc. 2015, 44, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, R.C.; Phillips, S.M.; Orzol, S.M. Food insecurity and the risks of depression and anxiety in mothers and behavior problems in their preschool-aged children. Pediatrics 2006, 118, e859–e868. [Google Scholar] [CrossRef] [PubMed]
- Kar, B.R.; Rao, S.L.; Chandramouli, B.A. Cognitive development in children with chronic protein energy malnutrition. Behav. Brain Funct. 2008, 4, 1186. [Google Scholar] [CrossRef] [PubMed]
- Sinn, N. Nutritional and dietary influences on attention deficit hyperactivity disorder. Nutr. Rev. 2008, 66, 558–568. [Google Scholar] [CrossRef] [PubMed]
- Lukowski, A.F.; Koss, M.; Burden, M.J.; Jonides, J.; Nelson, C.A.; Kaciroti, N.; Lozoff, B. Iron deficiency in infancy and neurocognitive functioning at 19 years: Evidence of long-term deficits in executive function and recognition memory. Nutr. Neurosci. 2010, 13, 54–70. [Google Scholar] [CrossRef] [PubMed]
- Galler, J.R.; Bryce, C.P.; Waber, D.P.; Medford, G.; Eaglesfield, G.D.; Fitzmaurice, G. Early malnutrition predicts parent reports of externalizing behaviors at ages 9–17. Nutr. Neurosci. 2011, 14, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Raine, A. The effect of childhood malnutrition on externalizing behavior. Cur. Opin. Pediatr. 2006, 18, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Raine, A.; Venables, P.H.; Mednick, S.A. Malnutrition at age 3 years and externalizing behavior problems at ages 8, 11, and 17 years. Am. J. Psychiatry 2004, 161, 2005–2013. [Google Scholar] [CrossRef] [PubMed]
- Oddy, W.H.; Robinson, M.; Ambrosini, G.L.; de Klerk, N.H.; Beilin, L.J.; Silburn, S.R.; Stanley, F.J. The association between dietary patterns and mental health in early adolescence. Prev. Med. 2009, 49, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Raine, A. The Anatomy of Violence: The Biological Roots of Crime; Pantheon: New York, NY, USA, 2013. [Google Scholar]
- Schoenthaler, S.J.; Bier, I.D. Diet and delinquency: Empirical testing of seven theories. Int. J. Neurosci. J. 1985, 7, 108–131. [Google Scholar] [CrossRef]
- Chilton, M.M.; Rabinowich, J.R.; Woolf, N.H. Very low food security in the USA is linked with exposure to violence. Public Health Nutr. 2014, 17, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Melchoir, M.; Caspi, A.; Howard, L.M.; Ambler, A.P.; Bolton, H.; Mountain, N.; Moffitt, T.E. Mental health context of food insecurity: A representative cohort of families with young children. Pediatrics 2009, 124, e564–e572. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, R.I.M. The social brain hypothesis. Evol. Anthropol. 1998, 6, 178–190. [Google Scholar] [CrossRef]
- Calkins, S.D.; Fox, N.A. Self-regulatory processes in early personality development: A multilevel approach to the study of childhood social withdrawal and aggression. Dev. Psychopathol. 2002, 14, 477–498. [Google Scholar] [CrossRef] [PubMed]
- DeLisi, M.; Vaughn, M.G. Foundation for a temperament-based theory of antisocial behavior and criminal justice system involvement. J. Crim. Justice 2014, 42, 10–25. [Google Scholar] [CrossRef]
- Gottfredson, M.; Hirschi, T. A General Theory of Crime; Stanford University Press: Stanford, CA, USA, 1990. [Google Scholar]
- Keenan, K. Emotion dysregulation as a risk factor for child psychopathology. Clin. Psychol. Sci. Pract. 2000, 7, 418–434. [Google Scholar] [CrossRef]
- Moffitt, T.E. Adolescence-limited and life-course-persistent antisocial behavior: A developmental taxonomy. Psychol. Rev. 1993, 100, 674–701. [Google Scholar] [CrossRef] [PubMed]
- Posner, M.I.; Rothbart, M.K. Developing mechanisms of self-regulation. Dev. Psycopathol. 2000, 12, 427–441. [Google Scholar] [CrossRef]
- Vaughn, M.G.; Beaver, K.M.; DeLisi, M.; Wright, J.P. Identifying latent classes of behavioral risk based on early childhood manifestations of self-control. Youth Violence Juv. Justice 2009, 7, 16–31. [Google Scholar] [CrossRef]
- Seligman, H.K.; Davis, T.C.; Schillinger, D.; Wolf, M.S. Food insecurity is associated with hypoglycemia and poor diabetes self-management in a low-income sample with diabetes. J. Health Care Poor Underserved 2010, 21, 1227–1233. [Google Scholar] [PubMed]
- Gailliot, M.T. Unlocking the energy dynamics of executive functioning: Linking executive functioning to brain glycogen. Perspect. Psychol. Sci. 2008, 3, 245–263. [Google Scholar] [CrossRef] [PubMed]
- Gailliot, M.T.; Baumeister, R.F. The physiology of willpower: Linking blood glucose to self-control. Personal. Soc. Psychol. Rev. 2007, 11, 303–327. [Google Scholar] [CrossRef] [PubMed]
- Muraven, M.; Baumeister, R.F. Self-regulation and depletion of limited resources: Does self-control resemble a muscle? Psychol. Bull. 2000, 126, 247–259. [Google Scholar] [CrossRef] [PubMed]
- DeWall, C.N.; Deckman, T.; Gailliot, M.T.; Bushman, B.J. Sweetened blood cools hot tempers: Physiological self-control and aggression. Aggress. Behav. 2011, 37, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Miller, G.E.; Chen, E.; Parker, K.J. Psychological stress in childhood and susceptibility to the chronic diseases of aging: Moving toward a model of behavioral and biological mechanisms. Psychol. Bull. 2011, 137, 959–997. [Google Scholar] [CrossRef] [PubMed]
- Gailliot, M.T.; Baumeister, R.F.; DeWall, C.N.; Maner, J.K.; Plant, E.A.; Tice, D.M.; Brewer, L.E.; Schmeichel, B.J. Self-control relies on glucose as a limited energy source: Willpower is more than a metaphor. J. Pers. Soc. Psychol. 2007, 92, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Bjorkqvist, K.; Lagerspetz, K.M.J.; Kaukiainen, A. Do girls manipulate and boys fight? Developmental trends in regard to direct and indirect aggression. Aggress. Behav. 1992, 18, 117–127. [Google Scholar] [CrossRef]
- Hasin, D.S.; Grant, B.F. The National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) Waves 1 and 2: Review and summary of findings. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1609–1640. [Google Scholar] [CrossRef] [PubMed]
- Salas-Wright, C.P.; Vaughn, M.G. Size matters: Are physically large people more likely to be violent? J. Interpers. Violence 2014. [Google Scholar] [CrossRef] [PubMed]
- Grant, B.F.; Dawson, D.A. Introduction to the national epidemiologic survey on alcohol and related conditions. Alcohol Res. Health 2006, 29, 74. [Google Scholar]
- Vaughn, M.G.; Fu, Q.; DeLisi, M.; Beaver, K.M.; Perron, B.E.; Howard, M.O. Criminal victimization and comorbid substance use and psychiatric disorders in the United States: Results from the NESARC. Ann. Epidemiol. 2010, 20, 281–288. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR Fourth Edition (Text Revision); American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Grant, B.F.; Harford, T.; Dawson, D.A.; Chou, P.S.; Pickering, R.P. The Alcohol Use Disorder and Associated Disabilities Interview schedule (AUDADIS): Reliability of alcohol and drug modules in a general population sample. Drug Alcohol Depend. 1995, 39, 37–44. [Google Scholar] [CrossRef]
- Grant, B.F.; Dawson, D.A.; Stinson, F.S.; Chou, P.S.; Kay, W.; Pickering, R.P. The Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV (AUDADIS-IV): Reliability of alcohol consumption, tobacco use, family history of depression and psychiatric diagnostic modules in a general population sample. Drug Alcohol Depend. 2003, 71, 7–16. [Google Scholar] [CrossRef]
- McIntyre, L.; Connor, S.K.; Warren, J. Child hunger in Canada: Results of the 1994 National Longitudinal Survey of Children and Youth. Can. Med. Assoc. J. 2000, 163, 961–965. [Google Scholar]
- Cumming, G.; Finch, S. Inference by eye: Confidence intervals and how to read pictures of data. Am. Psychol. 2005, 60, 170. [Google Scholar] [CrossRef] [PubMed]
- Allison, P.D. Comparing logit and probit coefficients across groups. Sociol. Methods Res. 1999, 28, 186–208. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 13; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- NESARC Wave I and II Data. Available online: http://www.psc.isr.umich.edu/dis/data/catalog/detail/1179 (accessed on 29 March 2016).
- Flexon, J.L. Callous-unemotional traits and differently motivated aggression: An examination of variants in a noninstitutionalized sample. Youth Violence Juv. Justice 2015, 13, 18–40. [Google Scholar] [CrossRef]
- Vaughn, M.G.; DeLisi, M.; Salas-Wright, C.; Maynard, B.R. Examining violence and externalizing behavior among youth in the United States: Is there a severe 5%? Youth Violence Juv. Justice 2014, 12, 3–21. [Google Scholar] [CrossRef]
- Vaughn, M.G.; Fu, Q.; Wernet, S.J.; DeLisi, M.; Beaver, K.M.; Perron, B.E.; Howard, M.O. Characteristics of abstainers from substance use and antisocial behavior in the United States. J. Crim. Justice 2011, 39, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Walters, G.D. Pathways to early delinquency: Exploring the individual and collective contributions of difficult temperament, low maternal involvement, and externalizing behavior. J. Crim. Justice 2014, 42, 321–326. [Google Scholar] [CrossRef]
- Walters, G.D. Early childhood temperament, maternal monitoring, reactive criminal thinking, and the origin(s) of low self-control. J. Crim. Justice 2015, 43, 369–376. [Google Scholar] [CrossRef]
- Benton, D. The impact of diet on anti-social, violent and criminal behaviour. Neurosci. Biobehav. Rev. 2007, 31, 752–774. [Google Scholar] [CrossRef] [PubMed]
- Bjork, J.M.; Dougherty, D.M.; Moeller, F.G.; Cherek, D.R.; Swann, A.C. The effects of tryptophan depletion and loading on laboratory aggression in men: Time course and a food-restricted control. Psychopharmacol. Ser. 1999, 142, 24–30. [Google Scholar] [CrossRef]
- Gray, G.E. Diet, crime and delinquency: A critique. Nutr. Rev. 1986, 44, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Virkkunen, M. Reactive hypoglycemic tendency among habitually violent offenders. Nutr. Rev. 1986, 44, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Zaalberg, A.; Nijman, H.; Bulten, E.; Stroosma, L.; van der Staak, C. Effects of nutritional supplements on aggression, rule-breaking, and psychopathology among young adult prisoners. Aggress. Behav. 2010, 36, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Cross, C.P.; Copping, L.T.; Campbell, A. Sex differences in impulsivity: A meta-analysis. Psychol. Bull. 2011, 137, 97–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flegal, K.M.; Carroll, M.D.; Ogden, C.L.; Curtin, L.R. Prevalence and trends in obesity among US adults, 1999–2008. J. Am. Med. Assoc. 2010, 303, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Mischel, W. The Marshmallow Test: Mastering Self-Control; Little, Brown: New York, NY, USA, 2014. [Google Scholar]
- Moffitt, T.E.; Arseneault, L.; Belsky, D.; Dickson, N.; Hancox, R.J.; Harrington, H.; Caspi, A. A gradient of childhood selfcontrol predicts health, wealth, and public safety. Proc. Natl. Acad. Sci. USA 2011, 108, 2693–2698. [Google Scholar] [CrossRef] [PubMed]
- Piquero, A.R.; Jennings, W.; Farrington, D.P. On the malleability of self-control: Theoretical and policy implications regarding a general theory of crime. Justice Q. 2010, 27, 803–834. [Google Scholar] [CrossRef]
- Walker, R.E.; Keane, C.R.; Burke, J.G. Disparities and access to health food in the United States: A review of food deserts literature. Health Place 2010, 16, 876–884. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Often Experienced Frequent Hunger? (“How Often Did a Parent or Other Adult Living in Your Home Make You Go Hungry or Not Prepare You Regular Meals?”) | Unadjusted | Adjusted | ||||||
|---|---|---|---|---|---|---|---|---|
| Sociodemographic Factors | No (n = 33,991, 98.4%) | Yes (n = 436, 1.16%) | ||||||
| % | 95% CI | % | 95% CI | OR | (95% CI) | OR | (95% CI) | |
| Age | ||||||||
| 18–34 years | 25.47 | (25.11–25.83) | 24.45 | (22.24–26.80) | 1.13 | (0.93–1.37) | 1.53 | (1.25–1.88) |
| 35–49 years | 31.11 | (30.79–31.44) | 31.33 | (29.18–33.57) | 1.18 | (0.99–1.42) | 1.80 | (1.49–2.17) |
| 50–64 years | 24.13 | (23.82–24.45) | 27.80 | (25.67–30.05) | 1.35 | (1.12–1.64) | 1.96 | (1.61–2.38) |
| 65 and older | 19.29 | (19.05–19.53) | 16.41 | (14.18–18.91) | 1.00 | 1.00 | ||
| Gender | ||||||||
| Female | 51.94 | (51.61–52.27) | 63.30 | (60.73–65.79) | 1.00 | 1.00 | ||
| Male | 48.06 | (47.73–48.39) | 36.70 | (34.21–39.27) | 0.63 | (0.56–0.70) | 0.64 | (0.58–0.72) |
| Race/Ethnicity | ||||||||
| Non-Hispanic White | 70.67 | (72.19–73.14) | 65.09 | (62.75–67.37) | 1.00 | 1.00 | ||
| African American | 11.29 | (10.89–11.71) | 9.88 | (8.63–11.28) | 0.98 | (0.84–1.13) | 0.72 | (0.62–0.84) |
| Hispanic | 4.31 | (4.19–4.44) | 5.21 | (4.90–5.53) | 1.89 | (1.67–2.13) | 1.31 | (0.12–1.54) |
| Other | 11.37 | (11.53–11.93) | 19.82 | (18.13–21.63) | 2.10 | (1.82–2.43) | 1.94 | (1.68–2.24) |
| Household Income | ||||||||
| <$20,000 | 19.37 | (19.10–19.65) | 31.16 | (28.55–33.88) | 2.81 | (2.49–3.18) | 2.27 | (2.02–2.55) |
| $20,000–$34,999 | 18.77 | (18.46–19.08) | 27.80 | (25.19–30.58) | 2.59 | (2.24–3.00) | 2.22 | (1.95–2.54) |
| $35,000–$69,999 | 32.37 | (32.07–32.67) | 24.19 | (21.66–26.91) | 1.31 | (1.13–1.52) | 1.20 | (1.03–1.39) |
| >$70,000 | 29.49 | (29.22–29.76) | 16.86 | (15.47–18.33) | 1.00 | 1.00 | ||
| Education Level | ||||||||
| Less than H.S. | 13.78 | (13.52–14.05) | 28.82 | (25.61–32.25) | 3.16 | (2.63–3.79) | 2.32 | (1.91–2.82) |
| H.S. Graduate | 27.43 | (27.06–27.81) | 30.34 | (27.34–33.53) | 1.67 | (1.45–1.93) | 1.42 | (1.23–1.64) |
| Some College | 21.77 | (21.47–22.07) | 16.35 | (14.75–18.08) | 1.13 | (0.97–1.33) | 1.01 | (0.86–1.18) |
| Completed AA, BA, or Technical Degree | 37.01 | (36.64–37.38) | 24.49 | (22.29–26.83) | 1.00 | 1.00 | ||
| Region of U.S. | ||||||||
| West | 17.75 | (17.33–18.18) | 22.44 | (20.26–24.77) | 1.00 | 1.00 | ||
| Northeast | 18.53 | (18.19–18.88) | 16.61 | (14.71–18.70) | 1.18 | (1.01–1.39) | 1.21 | (1.03–1.42) |
| Midwest | 38.42 | (37.97–38.87) | 33.87 | (30.60–37.31) | 0.84 | (0.72–0.97) | 0.81 | (0.69–0.94) |
| South | 25.30 | (24.95–25.65) | 27.08 | (24.63–29.67) | 0.82 | (0.69–0.98) | 0.83 | (0.70–0.98) |
| Urbanicity | ||||||||
| Rural | 67.27 | (66.77–67.77) | 64.47 | (61.14–67.68) | 1.00 | 1.00 | ||
| Urban | 32.73 | (32.23–33.23) | 35.53 | (32.32–38.86) | 1.13 | (0.99–1.30) | 1.09 | (0.96–1.25) |
| Often Experienced Frequent Hunger? (“How Often Did a Parent or Other Adult Living in Your Home Make You Go Hungry or Not Prepare You Regular Meals?”) | ||||||||
|---|---|---|---|---|---|---|---|---|
| No (Never/Almost Never/Sometimes) | Yes (Fairly Often/Often) | Unadjusted | Adjusted | |||||
| (n = 33,991, 98.84%) | (n = 436, 1.16%) | |||||||
| % | 95% CI | % | 95% CI | OR | 95% CI | AOR | 95% CI | |
| Violent Antisocial Behavior | ||||||||
| Any violence | ||||||||
| No | 85.41 | (85.12–85.69) | 63.02 | (60.44–65.54) | 1.00 | 1.00 | ||
| Yes | 14.59 | (14.31–14.88) | 36.98 | 34.46–39.56) | 3.62 | (3.20–4.10) | 2.08 | (1.81–2.38) |
| Get into a lot of fights that you started? | ||||||||
| No | 97.11 | (96.99–97.22) | 85.82 | (83.31–88.01) | 1.00 | |||
| Yes | 2.89 | (2.78–3.01) | 14.14 | (11.99–16.69) | 5.55 | (4.56–6.75) | 2.18 | (1.77–2.68) |
| Hit someone so hard that you injure them or they had to see a doctor? | ||||||||
| No | 93.79 | (93.60–93.98) | 80.16 | (77.67–82.44) | 1.00 | |||
| Yes | 6.21 | (6.02–6.40) | 19.84 | (17.56–22.33) | 3.74 | (3.19–4.38) | 2.21 | (1.85–2.64) |
| Use a weapon like a stick, knife, or gun in a fight? | ||||||||
| No | 97.27 | (97.17–97.37) | 86.85 | (84.57–88.84) | 1.00 | |||
| Yes | 2.73 | (2.63–2.83) | 13.15 | (11.16–15.43) | 5.40 | (4.48–6.50) | 2.34 | (1.90–2.88) |
| Physically hurt another person in any way on purpose? | ||||||||
| No | 94.69 | (94.51–94.87) | 82.94 | (80.90–84.80) | 1.00 | |||
| Yes | 5.31 | (5.13–5.49) | 17.06 | (15.20–19.10) | 3.67 | (3.18–4.24) | 2.06 | (1.79–2.38) |
| Female | Male | |||
|---|---|---|---|---|
| AOR | 95% CI | AOR | 95% CI | |
| Violent Antisocial Behavior | ||||
| Any violence? | 1.63 | (1.36–1.96) | 2.73 | (2.15–3.45) |
| Get into a lot of fights that you started? | 1.41 | (1.07–1.85) | 3.07 | (2.16–4.34) |
| Hit someone so hard that you injure them or they had to see a doctor? | 1.92 | (1.51–2.43) | 2.63 | (2.01–3.44) |
| Use a weapon like a stick, knife, or gun in a fight? | 1.85 | (1.44–2.37) | 2.88 | (2.01–4.13) |
| Physically hurt another person in any way on purpose? | 2.09 | (1.72–2.54) | 2.09 | (1.60–2.73) |
| Often Experienced Frequent Hunger? (“How Often did a Parent or other Adult Living in Your Home Make You Go Hungry or not Prepare You Regular Meals?”) | ||||||||
|---|---|---|---|---|---|---|---|---|
| No (Never/Almost Never/Sometimes) | Yes (Fairly Often/Often) | Unadjusted | Adjusted | |||||
| (n = 33,991, 98.84%) | (n = 436, 1.16%) | |||||||
| % | 95% CI | % | 95% CI | OR | 95% CI | AOR | 95% CI | |
| Impulse-Control Deficits | ||||||||
| Any self-control deficit | ||||||||
| No | 74.24 | (73.93–74.55) | 48.82 | (45.60–52.05) | 1.00 | 1.00 | ||
| Yes | 25.76 | (25.45–26.07) | 51.18 | (47.95–54.40) | 3.02 | (2.65–3.45) | 1.97 | (1.70–2.29) |
| Have you often done things impulsively? | ||||||||
| No | 83.12 | (82.84–83.40) | 65.21 | (61.89–68.38) | 1.00 | 1.00 | ||
| Yes | 16.88 | (16.60–17.16) | 34.79 | (31.62–38.11) | 2.63 | (2.27–3.04) | 1.70 | (1.45–2.00) |
| Have even little things made you angry or have you had difficulty controlling your anger? | ||||||||
| No | 92.69 | (92.53–92.84) | 83.77 | (82.15–85.27) | 1.00 | 1.00 | ||
| Yes | 7.31 | (7.16–7.47) | 16.23 | (14.73–17.85) | 2.45 | (2.17–2.77) | 1.19 | (1.04–1.36) |
| Have you often had temper outbursts or gotten so angry that you lose control? | ||||||||
| No | 93.23 | (93.06–93.39) | 78.57 | (76.91–80.14) | 1.00 | 1.00 | ||
| Yes | 6.77 | (6.61–6.94) | 21.43 | (19.86–23.09) | 3.75 | (3.40–4.14) | 1.81 | (1.61–2.03) |
| Have you hit people or thrown things when you got angry? | ||||||||
| No | 91.28 | (91.11–91.45) | 76.96 | (74.23–79.49) | 1.00 | 1.00 | ||
| Yes | 8.72 | (8.55–8.89) | 23.01 | (20.51–25.77) | 3.13 | (2.70–3.64) | 1.66 | (1.39–1.98) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaughn, M.G.; Salas-Wright, C.P.; Naeger, S.; Huang, J.; Piquero, A.R. Childhood Reports of Food Neglect and Impulse Control Problems and Violence in Adulthood. Int. J. Environ. Res. Public Health 2016, 13, 389. https://doi.org/10.3390/ijerph13040389
Vaughn MG, Salas-Wright CP, Naeger S, Huang J, Piquero AR. Childhood Reports of Food Neglect and Impulse Control Problems and Violence in Adulthood. International Journal of Environmental Research and Public Health. 2016; 13(4):389. https://doi.org/10.3390/ijerph13040389
Chicago/Turabian StyleVaughn, Michael G., Christopher P. Salas-Wright, Sandra Naeger, Jin Huang, and Alex R. Piquero. 2016. "Childhood Reports of Food Neglect and Impulse Control Problems and Violence in Adulthood" International Journal of Environmental Research and Public Health 13, no. 4: 389. https://doi.org/10.3390/ijerph13040389