
Nutritional Recommendations for Pregnant Women Receiving Dialysis: A Scoping Review

School of Medical, Indigenous and Health Sciences, University of Wollongong, Wollongong, NSW 2522, Australia
*
Author to whom correspondence should be addressed.
Kidney Dial. 2024, 4(1), 46-77; https://doi.org/10.3390/kidneydial4010005
Submission received: 15 December 2023
/
Revised: 9 February 2024
/
Accepted: 1 March 2024
/
Published: 15 March 2024
(This article belongs to the Special Issue Obstetric Nephrology—Emerging Field Both in Obstetrics and Nephrology)
Abstract
:Pregnancy in the dialysing population is an infrequent but increasing event. There is a lack of contemporary guidance regarding the nutritional management of this complex patient group. The aim of this scoping review was to identify, evaluate and summarise the evidence base describing nutritional recommendations for pregnant women receiving dialysis. A systematic search strategy of four databases and the grey literature was conducted. Eligible publications contained reference to recommendations regarding nutrition, supplements, breastfeeding, dietary patterns, and/or weight recommendations for pregnant dialysing women. A total of 136 eligible records were included for synthesis including 66 case reports/case series, 46 reviews, 15 book chapters, 5 editorials, and 4 consensus guidelines/position papers. Recommendations regarding energy, protein, dietary patterns, weight, and vitamin and mineral supplementation were common. However, significant discrepancy across these recommendations was evident. There were limited recommendations regarding other nutrients and breastfeeding. A summary of nutritional recommendations to guide clinical practice was constructed. Pregnancy planning, pre-conception dietetic counselling, interprofessional education, and the guidance synthesised in this review could be utilised by clinicians to improve clinical management and optimise outcomes in these patients. Future research should explore the experiences and perspectives of pregnant dialysing women, investigate nutrient losses during intensive dialysis, and evaluate postpartum follow-up.
1. Introduction
Pregnancy is an infrequent event in women with kidney failure (KF) [1]. The incidence in the dialysing population ranges from <1% to approximately 7% [2]. Reasons for infertility in women on dialysis include abnormalities in the hypothalamic–pituitary–ovarian axis resulting in anovulation and/or absent or irregular menses [3], decreased estrogen and progesterone levels, secondary abnormalities in endometrial morphology, and decreased kidney prolactin clearance resulting in hyperprolactinaemia [1] (see Figure 1 and Figure 2 for further details). These physical abnormalities are compounded by the emotional stress that KF and dialysis imposes on patients [4]. Furthermore, pregnancy on dialysis is associated with significant risks [1]. Foetal complications include prematurity (>80%), spontaneous abortion (40%), foetal/neonatal demise (21–33%), intrauterine growth restriction (20%), and polyhydramnios (29–67%) [5].
A nationwide survey conducted in 2014 by the Italian Study Group on ‘Kidney and Pregnancy’ found that the probability of delivering a live-born baby on dialysis was one-hundredth of the general population of the same age group [8]. Additionally, maternal complications include accelerated decline in renal function, worsened hypertension, superimposed preeclampsia, preterm labour, worsened anaemia, and abruptio placentae [5]. Evidently, pregnancy in this context remains a challenging scenario.
Despite this, the occurrence of pregnancy in people with ESKD is being increasingly reported [9]. A recent systematic review highlighted a substantial rise in the number of reported cases of pregnancy in women on dialysis (90 pregnancies in the years 2000 to 2008, compared to 584 pregnancies between 2008 and 2014) [10].
Factors contributing to this increase may include the rise in chronic conditions related to kidney disease in the child-bearing population [11], expanding knowledge about pregnancy during dialysis [12], improved fertility outcomes as a result of intensive dialysis delivery and nocturnal haemodialysis [13], as well as increased waiting time for kidney transplantation [14]. It is therefore likely that a dialysis unit will have to provide care for at least one pregnant patient [14], making it paramount that medical and allied health teams understand how to manage such cases.
Providing nutritional care for pregnant patients with KF is complex. Pregnancy itself is associated with physiologic changes that increase the body’s demand for energy and nutrients [15]. Additionally, dialysis schedules are intensified during pregnancy to reduce uraemia and mimic normal kidney function during foetal development [16], resulting in the loss of glucose, amino acids, proteins, vitamins, and trace elements from the blood [17,18]. Care under a dietitian is therefore crucial to ensure that maternal and foetal nutritional requirements are satisfied. A close interactive multidisciplinary team of nephrologists, obstetricians, dialysis nurses, neonatologists, paediatricians, and psychologists is also required to optimise pregnancy outcomes in these scenarios [19,20].
Given that the pregnant dialysing patient presents a challenging case, there remains a need for contemporary guidance for clinicians about the nutritional management of this patient group [9]. Whilst research regarding the dialysis prescription during pregnancy has grown substantially over recent years, the nutritional recommendations for this population remain largely unknown. Therefore, this scoping review aimed to synthesise nutritional recommendations for pregnant women receiving dialysis. The specific objectives of this review were as follows:
- Identify and evaluate academic and grey literature describing nutritional recommendations for pregnant women receiving dialysis.
- Synthesise existing guidance on nutritional recommendations for pregnant dialysing women to guide clinical practice.
2. Materials and Methods
This scoping review followed the five-stage framework as outlined by Arksey and O’Malley [21], and was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines [22]. The protocol was registered on the Open Science Framework on 4 March 2023 (Registered form osf.io/8g6tx, Registration DOI: 10.17605/OSF.IO/8G6TX).
2.1. Stage One: Identifying the Research Question
The scoping review study design is appropriate for this study as it intends to map and describe the existing body of literature on an evolving topic [21,23]. It is also useful for conducting research in areas that have not been comprehensively reviewed [21]. The specific research question was: What are the nutritional recommendations for pregnant women receiving dialysis?
2.2. Stage Two: Identifying Relevant Studies
An exhaustive search of five bibliographic databases was conducted (2 May 2023) to ensure an extensive review of the published literature. These databases included Scopus, Web of Science, MEDLINE, CINAHL, and PubMed. The key search terms used for each database search included (pregnant OR pregnancy OR “pregnant woman” OR “pregnant women” OR “expect* mothers” OR “pregnant people” OR “pregnant person”) AND (dialysis OR hemodialysis OR haemodialysis OR “peritoneal dialysis” OR “renal replacement therapy” OR “kidney replacement therapy” OR “renal dialysis” OR “kidney dialysis” OR “chronic renal failure” OR “chronic kidney failure” OR “kidney failure” OR “end-stage renal failure” OR “end stage renal failure” OR “ESRF” OR “end-stage renal disease” OR “end stage renal disease” OR “ESRD” OR “end-stage kidney failure” OR “end stage kidney failure” OR “ESKF” OR “end-stage kidney disease” OR “end stage kidney disease” OR “ESKD”) AND (nutrition* OR nutrient* OR “nutrition* therapy” OR “diet* therapy” OR “nutrition* recommendation*” OR “nutrition* requirement*” OR “nutrition* intervention” OR “nutrition* management” OR “medical nutrition therapy” OR “nutrition* assessment” OR diet* OR vitamin* OR mineral*). This search strategy was informed by Levey and colleagues [24], similar work in the field of pregnancy and renal disease [25,26], and guidance from an experienced clinician (KL) and librarians.
A search of the grey literature was also conducted (3–9 May 2023) to obtain any relevant literature that may have been missed by the bibliographic database searches. Grey literature searching comprised four search strategies: (1) the first 300 search results in Google Scholar [27] using the terms (pregnancy) AND (dialysis) AND (nutrition) were retrieved, (2) the advanced search function in Open Grey was used to identify relevant grey literature using the terms (pregnancy) AND (dialysis) AND (nutrition), (3) the home page search function of all relevant quartile 1 and quartile 2 journals listed on SCImago under ‘Nephrology’, ‘Nutrition and Dietetics’ and ‘Obstetrics and Gynecology’ were searched using the terms ‘pregnancy and dialysis’, (4) the home pages of key societies and associations in the fields of ‘Nephrology’, ‘Nutrition and Dietetics’ and ‘Obstetrics and Gynecology’ were searched using the terms ‘pregnancy and dialysis’. A complete list of these grey literature search strategies is shown in Supplementary Table S1. Search restrictions were not applied to database or grey literature searches to ensure that all relevant sources of evidence were retrieved.
2.3. Stage Three: Selecting Studies
All records from database searches and relevant documents from grey literature searches were downloaded into EndNote (Thomson Reuters, Toronto, ON, Canada; Version 20, 2020). These citations were then uploaded to the Covidence online systematic review management tool (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org, accessed on 9 May 2023) for automatic removal of duplicates and screening by the research team. Two reviewers (EC and KL) screened the title and abstracts of all citations according to the inclusion criteria. Any disagreements during this process were resolved by discussion between the reviewers. For studies that passed initial screening, full text articles were retrieved. Two reviewers (EC and KL) examined the full text of 17 (5%) articles to ensure consistency in the application of inclusion criteria. One reviewer (EC) then screened the remaining full text articles to determine inclusion. The reference lists of each included study were also reviewed to ensure a comprehensive scope of the literature.
Sources of evidence considered eligible for inclusion were case reports, case series, reviews, observational studies, editorials, conference abstracts, consensus guidelines, position papers, and book chapters. Each source of evidence had to include nutritional, supplement, breastfeeding, dietary pattern, and/or weight recommendations for pregnant dialysing women. Documents from the grey literature were included only if they were in English, and non-English studies from database searches were included only if they could be translated by the research team. Documents without full text availability, non-human studies, and ‘Biology’, ‘Molecular’, and ‘Exercise and Sports Science’ journals in the grey literature were excluded from the review. Details of eligibility criteria can be found in Supplementary Table S2.
2.4. Stage Four: Charting the Data
Data charting forms were developed in Excel (Microsoft Corporation, Redmond, WA, USA, 2023) by one reviewer (EC). In the initial phases of the data charting process, the research team met regularly to determine whether the approach to data extraction was consistent with the research question and purpose. Once the approach was agreed upon, one reviewer (EC) independently extracted information from the included literature and populated it in the data charting forms.
Sources of evidence were grouped according to their type, i.e., consensus guidelines/position papers, reviews, case reports/case series, editorials, and book chapters. The completed data charting forms were then transferred from Excel to Word (Microsoft Corporation, 2023) by one reviewer (EC). Data charting included authors, year of publication, country of origin, aetiology of kidney disease, number of subjects in the study, maternal age at pregnancy diagnosis, timing of dialysis commencement, dialysis regimen, pregnancy term, and macronutrient, vitamin, mineral, supplement, dietary pattern, breastfeeding, and weight recommendations as well as any other relevant commentary.
2.5. Stage Five: Collating, Summarising, and Reporting the Results
Using guidance from Levac and colleagues [28], the extracted data were synthesised in several ways. First, a descriptive summary of the main findings was constructed. Then, recommendations from the included sources of evidence were reported as relevant to the overall purpose of the research question, i.e., findings were arranged into five main categories: (1) main features of selected studies, (2) recommendations regarding macronutrients, (3) recommendations regarding vitamins, (4) recommendations regarding minerals, (5) recommendations regarding other commentary. Finally, recommendations were synthesised, and the meaning of the findings was discussed as they relate to the overall study purpose, with the implications for clinical practice and future research explored.
It is important to note that in this scoping review the term ‘pregnant woman’ refers to any person with the potential to be pregnant, including transgender, non-binary, and gender-diverse people who do not have a gender identity and gender modality that aligns with their assigned sex at birth [29].
3. Results
Altogether, 3990 records were identified from the systematic search strategy (Supplementary Materials Figure S1). Of these, 3463 papers were identified from database searches, 523 papers were identified from the grey literature, and 4 papers were identified from citation searches. Following the automatic removal of 738 duplicate records, 3252 articles were screened by title and abstract. A total of 292 records were then reviewed by full text; 136 of these met the inclusion criteria [2,5,9,14,19,20,26,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221,222,223,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254,255,256,257,258,259,260,261,262,263,264,265].
3.1. Features of Selected Studies
Of the 136 articles included in this scoping review, 29 (21.3%) were published from 1970 to 1999, and 107 (78.7%) were published from 2000 to 2023. This illustrates a large increase in research around pregnancy and dialysis since the new millennium, when the first global guidelines for nutrition in chronic kidney disease (CKD) were published [50]. A total of 66 papers included in this review were case reports/case series (48.5%), followed by 46 reviews (33.8%), 15 book chapters (11%), 5 editorials (3.7%), and 4 consensus guidelines/position papers (2.9%). The vast majority of included records originated from the United States (51; 37.5%). The remaining studies were from Europe (36; 26.5%), Asia (14; 10.3%), North America (11; 8.1%), South America (3; 2.2%), Africa (3; 2.2%), Australia (3; 2.2%), Russia (2; 1.5%), Turkey (1; 0.7%), and Cuba (1; 0.7%). Eleven papers (8.1%) were multinational.
There were 118 pregnancies on dialysis reported across all case reports/case series (Supplementary Table S7). Of these pregnancies, 102 (86.4%) occurred on haemodialysis (HD) and 15 (12.7%) occurred on peritoneal dialysis (PD). One study (0.8%) did not specify the mode of dialysis used during pregnancy [123]. Additionally, a total of 90 pregnancies (76.3%) occurred after the commencement of dialysis, whilst in 27 cases (22.9%) dialysis was started during the pregnancy. One case report (0.8%) did not specify the timing of dialysis commencement [162].
3.2. Recommendations Regarding Macronutrients
Macronutrient recommendations included energy, carbohydrate, protein, fat, fibre, and fluid (see Supplementary Table S3 for a detailed summary of these recommendations). The ‘Australia and New Zealand Nutrient Reference Values (NRVs)’ for pregnancy in women aged 14–50 years [30], and the ‘Kidney Disease Outcomes Quality Initiative (KDOQI) Clinical Practice Guideline for Nutrition in CKD: 2020 Update’ [31] were used as comparators (where available) for all nutrient recommendations summarised in this scoping review. Heat maps have also been used to illustrate whether the recommendations charted in this paper are consistent with the NRV and/or KDOQI guidelines, and where any gaps in the literature may exist (see Table 1, Table 2 and Table 3).
The overall number of macronutrient recommendations collated in this review was 213, see Supplementary Table S3. There were 107 recommendations made for protein (50.2%), followed by 59 (27.7%) for energy, 14 (6.6%) for fluid [4,46,48,67,90,112,124,126,128,146,153,161,162,169], 5 (2.3%) for fat [48,106,112,124,169], 4 (1.9%) for carbohydrate [48,106,112,169], and 1 (0.5%) for fibre [112]. These figures highlight the scarcity of literature regarding carbohydrate, fat, fibre, and fluid recommendations for pregnant women receiving dialysis. A total of 23 (10.8%) additional macronutrient recommendations were also charted [1,5,41,48,56,68,86,94,101,104,105,106,112,121,124,128,133,139,141,169,177,182,183], which included general commentary as well as recommendations from studies other than the ones made or prescribed by those charted in this review. Of the 136 included papers, 29 did not make any macronutrient recommendations [3,9,14,45,66,70,78,83,88,91,92,93,95,96,97,98,111,118,119,123,130,148,152,154,155,156,159,163,165].
Approximately three-quarters (72.9%) of energy recommendations were consistent with the NRV for energy in pregnancy (an additional 1.4 MJ/day in the second trimester and 1.9 MJ/day in the third trimester) or the KDOQI guideline for dialysis (25–35 kcal/kg/day). The remaining energy recommendations varied and suggested values differed to the comparative standards. In contrast, 92.5% of protein recommendations exceeded the corresponding NRV for pregnancy (58–60 g/day or 1.00–1.02 g/kg/day in the second and third trimesters) or KDOQI guidelines (1.0–1.2 g/kg/day). Approximately 6.5% of protein recommendations were consistent with these ranges, whilst only one (0.9%) was below [120]. There are no NRV or KDOQI recommendations for carbohydrate intake in pregnant women or people undertaking dialysis. Notably, the recommendations for dietary fat intake were inconsistent with the types of fat recommended by the NRV guidelines.
There was only one recommendation for fibre made (28 g/day) [112] which was consistent with the respective NRV for pregnancy of 25–28 g/day. Most (85.7%) fluid recommendations were lower than the NRV for fluid intake during pregnancy (1.8–2.3 L/day).
Recommendations for macronutrients were specific to HD in 88 publications, and PD in 19 publications. Altogether, 43 publications made macronutrient recommendations for both HD and PD, whilst 62 made recommendations that were not specific to a mode of dialysis.
3.3. Recommendations Regarding Vitamins
A total of 42 recommendations regarding vitamin intake were made across 17 studies (see Supplementary Table S4). The majority of these were for folate (40.5%), with recommendations ranging from 0.8 to 5.0 mg/day. One publication suggested 800 µg/day of vitamin A [112], whilst another advised 600 µg/day of Biotin during HD [46]. The recommendation for Vitamin a was consistent with the corresponding pregnancy NRV.
Recommended or prescribed levels of intake for vitamin C were described in five publications [37,46,89,112,149], each of which suggested a minimum intake of 170 mg/day (one of these being specific to HD). Two studies suggested 1000–2000 IU/day of 25 OH vitamin D for those undertaking HD [33,35]. Recommendations for B vitamins were described in 16 separate publications. Four studies each suggested 3 mg/day of vitamin B1, 3.4 mg/day of vitamin B2, and a minimum intake of 20 mg/day for vitamin B3 [37,46,89,149]. One recommendation for each of these B vitamins were specific to HD [46]. Suggested intakes for vitamin B6 included greater than 5 mg/day in one publication [37], and equal to or greater than 5 mg/day in three publications [46,89,149] (one of these being specific to HD) [46]. No additional vitamin recommendations were made in any of the 136 publications.
3.4. Recommendations Regarding Minerals
A total of 83 mineral recommendations for pregnant women receiving dialysis were identified in 38 papers; however there were no suggested levels of intake for Iodine, Copper, Selenium, Manganese, or Molybdenum (see Supplementary Table S5 for a detailed summary of mineral recommendations).
There were 13 recommendations regarding sodium intake. Of these, 10 exceeded the corresponding NRV and KDOQI guidelines [35,46,48,73,87,112,124,149,169,176], whilst 3 were consistent with the KDOQI guideline only [4,82,150]. Six recommendations for potassium were lower than the respective NRV [4,82,112,124,162,169], whilst six were higher [33,35,46,48,149,176].
Twenty-one studies made recommendations for calcium ranging from 800 to 2000 mg/day. Fifteen of these were above [4,33,35,37,55,67,71,72,79,82,90,121,128,129,179], five were consistent with [32,46,73,112,169], and one was below the corresponding NRV for calcium in pregnancy (1000–1300 mg/day) [68]. All five recommendations for magnesium were 200–300 mg/day [37,46,89,112,149], each less than the NRV of 350–400 mg/day. Nine studies made recommendations for iron. Of these, seven were greater than the NRV for pregnancy [2,66,112,143,149,165,174], whilst two provided a range (20–30 mg/day) that sat both above and below the NRV recommendation (27 mg/day) [33,35]. In all, 11 zinc recommendations were charted, with 8 suggesting 15 mg/day [33,35,37,46,73,89,149,182] and 3 recommending equal to or above 15 mg/day [175,177,179], all of which were greater than the NRV for pregnancy. The NRV for phosphorous during pregnancy is 1000–1250 mg/day.
Eight publications were consistent with this [35,37,46,89,112,149,162,169]; however, three made recommendations of 800 mg/day [79,124,126] and one suggested 800–1600 mg/day [129]. A total of 14 mineral recommendations charted in this review were specific to HD [33,35,46,48], whilst 11 were specific to PD [124,126,149,150,162,176], and 4 recommendations suggested intakes for both HD and PD [169]. The remaining recommendations did not explicitly state what mode of dialysis they were specific to.
3.5. Recommendations Regarding Other Commentary
Supplementary Table S6 summarises 318 recommendations regarding additional nutritionally related commentary (112; 35.2%), weight (95; 29.9%), dietary patterns (88; 27.7%), and breastfeeding (23; 7.2%). The additional commentary included, but was not limited to, supplementation, physical activity, and diabetes management.
Diet liberalisation (including calories, protein, sodium, potassium, phosphorous and/or fluid) was suggested or prescribed in 70 studies. Seven publications specifically recommended high biological value protein to ensure adequate and optimal nutrition [48,87,107,144,161,167,176]. One study stressed that culturally appropriate diets should be prescribed, with the main objective of preventing malnutrition [98]. The authors of another publication prescribed their patient a plant-based diet at the commencement of HD as per the treating nephrologist’s advice [148]. This diet made the patient’s request to cease HD at 31 weeks gestation possible due to stability of renal function.
Additionally, 14 publications recommended breastfeeding in dialysing patients or described cases where women on dialysis decided to breastfeed their infants [34,43,45,46,52,60,70,96,98,100,125,132,164,169]. Four studies emphasized that a review of all medications is necessary to determine their compatibility with breastfeeding [45,52,70,164]. Seven articles warned that the urea content of breastmilk may be higher in renal patients which can cause diuresis in infants [46,93,143,174,177,179,182]. Of these publications, four suggested giving water with breastmilk feedings to mitigate this issue [46,177,179,182], whilst one also recommended supplementing breastmilk feedings with formula so that the nutrient needs of infants can be met. One publication advised against breastfeeding in dialysing patients due to the low concentration of nutrients and high levels of toxic substances such as pro-inflammatory cytokines and urea in breastmilk samples [93].
Another study described significant variations in breastmilk composition between pre and post HD samples, suggesting that breastfeeding after a dialysis session is preferable to breastfeeding prior to a dialysis session [60]. The same study stressed that there is no available data on breastfeeding in PD. Three publications stated that there is a lack of literature regarding the safety or efficacy of breastfeeding in infants born to mothers with CKD [177,179,182]. Breastmilk is the best source of nutrition for an infant and also exerts health benefits for the mother. Should a woman choose to breastfeed their infant while dialysing, an extra 330 kcal/day than the weight-maintenance needs of her non-pregnant counterpart during the first 6 months postpartum, and an additional 400 kcal/day during the second 6 months postpartum has been recommended [169]. Another study suggested increasing caloric intake by 500 kcal/day in dialysing women who wish to breastfeed [179].
According to four publications [47,66,106,165], the recommended total weight gain per singleton pregnancy in a dialysing woman with a healthy pre-pregnancy body mass index (BMI) is 11.5–16 kg. Thirteen publications advised a total weight gain of 1.0–1.5 kg in the first trimester [35,48,67,71,79,102,143,146,166,173,174,181,185]. Moreover, 19 studies suggested weight gain of 0.5 kg/week from the second trimester [1,2,3,35,48,52,59,60,75,77,92,118,125,146,173,175,177,179,185], whilst 12 recommended weight gain of 0.3–0.5 kg/week during the second and third trimesters of pregnancy [5,47,58,61,66,70,79,80,84,137,165,182].
Finally, 101 studies charted in this scoping review provided additional commentary regarding nutrient supplementation. Prescriptions of 1.5–2 mg/day of calcium, 0.8–5 mg/day of folate, 15 mg/day of zinc, and up to 30 mg/day of iron (preferably intravenous) were common. It was suggested that 25 OH vitamin D should be measured every trimester and supplemented if low; however, vitamins A and E should not be routinely supplemented due to risk of toxicity. Instead, doubling the dose of a water-soluble or renal-formulated vitamin was suggested, especially for intensive dialysis schedules. Other recommendations included the use of parenteral nutrition for severely decreased oral intake [37,46,78,82], lower calorie diets for patients on PD (due to calories provided by dialysate glucose absorption) [35], and regular meals and dialysis times so that daily meal, blood sugar, and insulin timing can remain constant for patients with diabetes [46]. Moderate physical activity was encouraged [110,112], and weekly follow-ups using dietary recalls and/or food intake records to evaluate nutritional adequacy in these patients was specifically suggested in two publications [175,177]. The importance of providing referral assistance to patients with low socioeconomic status to ensure access to foods and supplements that meet the increased protein and calorie needs during pregnancy was also emphasised by one publication [167].
3.6. Synthesis of Recommendations from Scoping Review Findings
A synthesis of recommendations charted in this scoping review is provided in Table 4. It is intended for clinicians requiring guidance around the nutritional management of pregnant women receiving dialysis. This synthesis is constructed using a consensus of nutritional recommendations from the current literature, clinical judgement, recently published guidance regarding vitamin requirements in CKD patients [267], and the NRVs for pregnancy or KDOQI guidelines for dialysis.
4. Discussion
Nutrition plays a pivotal role in optimising the health outcomes of people with kidney disease. This scoping review intended to collate and synthesise nutritional recommendations for pregnant women undertaking dialysis, identify where gaps in the current literature exist, and propose recommendations that will inform clinical practice.
From the 136 publications charted in this review, it is clear that recommendations regarding vitamin and mineral intake are scarce and/or vary widely. The number of recommendations concerning energy, protein, dietary patterns, weight, and nutrient supplementation is considerable; however, specific suggestions for carbohydrate, fat, fibre, and fluid intake as well as breastfeeding are lacking. The recently published literature regarding the haemodialysis prescription for pregnant women also failed to provide in depth guidance [26,193,266,268]. Evidently, nutritional recommendations in this field are still lacking, forcing healthcare providers to rely heavily on clinical judgement in an area of significant uncertainty.
This scoping review also highlighted significant heterogeneity between recommendations, particularly those regarding energy, protein, dietary patterns, weight, breastfeeding, and supplementation. Inconsistencies between the published guidance may be attributed to the sizeable time span over which the included sources of evidence were published, along with the anecdotal nature of recommendations provided by position papers, case reports/case series, and editorials.
Additionally, where recommendations were made to a specific mode of dialysis, HD dominated the majority of these recommendations. This is likely because the incidence of pregnancy in women on PD is lower than for HD due to challenges posed by high dialysate osmolality, fallopian tube injury secondary to peritoneal infection, risk of small-for-gestational-age infants, and technical difficulties with the volume and frequency of exchanges that can be provided as pregnancy progresses [5,26]. The discrepancies between recommendations and a paucity of data regarding the nutritional management of pregnant dialysing patients, especially for those on PD, presents a significant challenge for healthcare professionals when providing specific medical nutrition therapy or nutritionally related advice for this patient population.
Several limitations exist within this scoping review. For instance, the grey literature was limited to those written in English only. Therefore, despite an extensive search strategy, relevant publications may have been missed. Additionally, many included sources of evidence were more than two decades old and may not reflect current dialysis practices utilised for pregnant women.
Variance in the details of nutritional recommendations reported across the literature contributed to the heterogeneity of data extracted, and thus posed challenges with synthesising and interpreting the results. Heterogeneity in the reporting of other information was also apparent. For example, we were unable to report comprehensive information on the demographics, baseline biochemistry or anthropometry. Pre-existing supplement use and adherence was also variable and may have influenced nutrient needs. Although not mandatory in the scoping review process, an appraisal of methodological quality was not completed. Hence, the quality of evidence and risk of bias of studies within this review was not assessed but is likely to be very low. A strength of this review was the broad systematic search strategy used across five bibliographic databases as well as the grey literature. As a result, a wide range of relevant evidence in the field was explored. The use of scoping review methodology enabled the available literature to be exhaustively mapped to identify knowledge gaps and discrepancies.
As a result of this scoping review, we have constructed several recommendations for the nutritional management of pregnant women receiving dialysis. Firstly, pregnancy planning should be undertaken so that patients and the multidisciplinary team can prepare for this high-risk situation. Mothers must be counselled on the risks that these pregnancies carry, and information provided where possible in advance about the significant changes that will occur to dialysis regimens, medications, nutrition, and dry weight. These changes are critical to ensure that foetal growth and the demands of pregnancy can be accommodated [25,26,70]. Comorbid conditions, such as diabetes and hypertension, should also be well managed prior to pregnancy to optimise health outcomes for mothers and their infants [26,70].
Secondly, pre-conception dietetic counselling should be provided to patients so that plans for medical nutrition therapy can be devised and their nutritional status optimised in advance. Pregnancy itself results in increased nutritional requirements so that maternal metabolism can be maintained, and foetal development supported [269]. It has been shown that standard dialysis sessions (i.e., 4 h three times weekly) [270] can result in the removal of up to 12 g of amino acids, 600–1200 mg of phosphate, and 60–150 mmol of potassium [270,271,272,273]. Depletion of folic acid, vitamin B6, vitamin C, iron, and zinc has also been demonstrated [274,275]. Dialysis regimens during pregnancy are commonly intensified to 36 h/week over 5–7 sessions [268], leading to an even greater loss of these nutrients from the blood. Therefore, patients planning to conceive must be counselled about the necessary changes to their dietary prescription, including the need for diet liberalisation and supplementation. Individualised strategies to optimise nutrition should also be provided pre-conception, with consideration of the socioeconomic status and cultural background of each patient.
Thirdly, we suggest that clinicians use the summary of evidence provided in Table 4 as a starting point to inform their decisions regarding medical nutrition therapy for pregnant dialysing patients. Additional adjustments may also be required in those undertaking intensive daily dialysis regimens due to significantly greater nutrient losses from the blood. In these circumstances, vitamin and mineral supplementation will be required.
Lastly, interdisciplinary collaboration is critical in the management of the pregnant dialysing woman. Regular case conferencing between members of the dietetics, social work, nephrology, obstetrics and gynaecology, midwifery and critical care teams is necessary. While the safe arrival of the infant is paramount, there are ongoing challenges to mothers managing babies and children when maintaining regular dialysis for the longer term, and discussion about how these challenges will be managed by the kidney care team are also important.
Areas for future work in this field include qualitative research exploring the experiences and perspectives of pregnant women receiving dialysis and empirical studies exploring losses of protein, water-soluble vitamins, and minerals during intensive dialysis (i.e., 36 h/week over 5–7 sessions). This would assist clinicians to develop more accurate insights into the nutrient prescription and patient-centred approaches to care required by these patients. Furthermore, although there has been a 90% increase in the pregnancy success rate of this population since the year 1980 [75], the health outcomes of these women and guidelines for dietetic follow up after these pregnancies remain unclear. Therefore, we also recommend that women who have had pregnancies on dialysis should receive ongoing dietetic input and be monitored regularly postpartum to ensure optimal nutritional status in the long term. Future research examining foetal outcomes would also be useful.
5. Conclusions
This scoping review provides an exhaustive overview of nutritional recommendations for pregnant women receiving dialysis. While significant knowledge gaps and inconsistencies remain, several recommendations to inform the nutritional management of this population have been constructed. These recommendations are critical to the provision of proactive, effective, and collaborative nutritional care in this patient population, so that maternal and foetal health outcomes may be optimised.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/kidneydial4010005/s1, Figure S1: PRISMA flow diagram of study selection; Table S1: Grey literature search strategy; Table S2. Scoping review eligibility criteria; Table S3. Macronutrient recommendations from the literature for pregnant women receiving dialysis; Table S4. Vitamin recommendations from the literature for pregnant women receiving dialysis; Table S5. Mineral recommendations from the literature for pregnant women receiving dialysis; Table S6. Other relevant commentary from the literature regarding pregnant women receiving dialysis; Table S7. Summary of included case reports/case series.
Author Contributions
Conceptualization, E.C. and K.L.; methodology, E.C. and K.L.; formal analysis, E.C. and K.L.; data curation, E.C.; writing—original draft preparation, E.C.; writing—review and editing, E.C. and K.L.; supervision, K.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created as part of this research.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Nadeau-Fredette, A.-C.; Hladunewich, M.; Hui, D.; Keunen, J.; Chan, C.T. End-Stage Renal Disease and Pregnancy. Adv. Chronic Kidney Dis. 2013, 20, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Hladunewich, M.; Hercz, A.E.; Keunen, J.; Chan, C.; Pierratos, A. Pregnancy in End Stage Renal Disease. Semin. Dial. 2011, 24, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Shemin, D. Dialysis in pregnant women with chronic kidney disease. Semin. Dial. 2003, 16, 379–383. [Google Scholar] [CrossRef]
- Reddy, S.S.; Holley, J.L. Management of the Pregnant Chronic Dialysis Patient. Adv. Chronic Kidney Dis. 2007, 14, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Fisher, E.I.; Deering, S.H.; Oliver, J.D., III. Dialysis in Pregnancy. In Critical Care Obstetrics; John Wiley & Sons: Hoboken, NJ, USA, 2018; pp. 273–283. [Google Scholar]
- Ghazizadeh, S.; Lessan-Pezeshki, M. Reproduction in women with end-stage renal disease and effect of kidney transplantation. Iran. J. Kidney Dis. 2007, 1, 12–15. [Google Scholar]
- Ahmed, S.B.; Ramesh, S. Sex hormones in women with kidney disease. Nephrol. Dial. Transplant. 2016, 31, 1787–1795. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Cabiddu, G.; Daidone, G.; Guzzo, G.; Maxia, S.; Ciniglio, I.; Postorino, V.; Loi, V.; Ghiotto, S.; Nichelatti, M.; et al. The children of dialysis: Live-born babies from on-dialysis mothers in Italy—An epidemiological perspective comparing dialysis, kidney transplantation and the overall population. Nephrol. Dial. Transplant. 2014, 29, 1578–1586. [Google Scholar] [CrossRef] [PubMed]
- Cabiddu, G.; Castellino, S.; Gernone, G.; Santoro, D.; Giacchino, F.; Credendino, O.; Daidone, G.; Gregorini, G.; Moroni, G.; Attini, R.; et al. Best practices on pregnancy on dialysis: The Italian Study Group on Kidney and Pregnancy. J. Nephrol. 2015, 28, 279–288. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Minelli, F.; Versino, E.; Cabiddu, G.; Attini, R.; Vigotti, F.N.; Rolfo, A.; Giuffrida, D.; Colombi, N.; Pani, A.; et al. Pregnancy in dialysis patients in the new millennium: A systematic review and meta-regression analysis correlating dialysis schedules and pregnancy outcomes. Nephrol. Dial. Transplant. 2016, 31, 1915–1934. [Google Scholar] [CrossRef]
- Harris, M.L.; Egan, N.; Forder, P.M.; Loxton, D. Increased chronic disease prevalence among the younger generation: Findings from a population-based data linkage study to inform chronic disease ascertainment among reproductive-aged Australian women. PLoS ONE 2021, 16, e0254668. [Google Scholar] [CrossRef]
- Jesudason, S. Pregnancy and kidney disease: It is time for the birth of prospective registries. Nephrology 2021, 26, 849–850. [Google Scholar] [CrossRef] [PubMed]
- Jesudason, S.; Grace, B.S.; McDonald, S.P. Pregnancy outcomes according to dialysis commencing before or after conception in women with ESRD. Clin. J. Am. Soc. Nephrol. CJASN 2014, 9, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.; Firanek, C. Management of the pregnant dialysis patient. Adv. Ren. Replace Ther. 1998, 5, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Ladipo, O.A. Nutrition in pregnancy: Mineral and vitamin supplements. Am. J. Clin. Nutr. 2000, 72, 280S–290S. [Google Scholar] [CrossRef]
- Burrowes, J.D.; Kovesdy, C.P.; Byham-Gray, L.D. Nutrition in Kidney Disease; Springer Nature: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Laville, M.; Fouque, D. Nutritional aspects in hemodialysis. Kidney Int. Suppl. 2000, 76, S133–S139. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Broman, M.; Forni, L.; Ostermann, M.; De Waele, E.; Wischmeyer, P.E. Nutrients and micronutrients at risk during renal replacement therapy: A scoping review. Curr. Opin. Crit. Care 2021, 27, 367–377. [Google Scholar] [CrossRef]
- Holley, J.L.; Reddy, S.S. Pregnancy in Dialysis Patients: A Review of Outcomes, Complications, and Management. Semin. Dial. 2003, 16, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, C.I.; Silva, N. Pregnancy and dialysis. J. Bras. Nefrol. 2020, 42, 349–356. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Eckardt, K.U.; Dorman, N.M.; Christiansen, S.L.; Hoorn, E.J.; Ingelfinger, J.R.; Inker, L.A.; Levin, A.; Mehrotra, R.; Palevsky, P.M.; et al. Nomenclature for kidney function and disease: Report of a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney Int. 2020, 97, 1117–1129. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Conijn, A.; Consiglio, V.; Vasario, E.; Attini, R.; Deagostini, M.C.; Bontempo, S.; Todros, T. Pregnancy in dialysis patients: Is the evidence strong enough to lead us to change our counseling policy? Clin. J. Am. Soc. Nephrol. CJASN 2010, 5, 62–71. [Google Scholar] [CrossRef]
- Wiles, K.; Chappell, L.; Clark, K.; Elman, L.; Hall, M.; Lightstone, L.; Mohamed, G.; Mukherjee, D.; Nelson-Piercy, C.; Webster, P.; et al. Clinical practice guideline on pregnancy and renal disease. BMC Nephrol. 2019, 20, 401. [Google Scholar] [CrossRef]
- Haddaway, N.R.; Collins, A.M.; Coughlin, D.; Kirk, S. The Role of Google Scholar in Evidence Reviews and Its Applicability to Grey Literature Searching. PLoS ONE 2015, 10, e0138237. [Google Scholar] [CrossRef] [PubMed]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Rioux, C.; Weedon, S.; London-Nadeau, K.; Paré, A.; Juster, R.P.; Roos, L.E.; Freeman, M.; Tomfohr-Madsen, L.M. Gender-inclusive writing for epidemiological research on pregnancy. J. Epidemiol. Community Health 2022, 76, 823–827. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand; Australian Government National Health and Medical Research Council: Canberra, Australia, 2013.
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.-J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- De Jong, M.F.C.; van Hamersvelt, H.W.; van Empel, I.W.H.; Nijkamp, E.J.W.; Lely, A.T. Summary of the Dutch Practice Guideline on Pregnancy Wish and Pregnancy in CKD. Kidney Int. Rep. 2022, 7, 2575–2588. [Google Scholar] [CrossRef]
- Schmidt, M.; Stracke, S.; Schneider, U.; Kuschel, B.; Feldkamp, T.; Habbig, S.; Mayer-Pickel, K.; Hartung, A.; Bader, B.; Weinmann-Menke, J.; et al. Chronic Kidney Disease and PregnancyGuideline of the DGGG, OEGGG, DGfN (S2k Level, AWMF Registry No. 015-090). Geburtshilfe Und Frauenheilkd. 2022, 82, 795–830. [Google Scholar] [CrossRef]
- Hladunewich, M.; Schatell, D. Intensive dialysis and pregnancy. Hemodial. Int. 2016, 20, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Esposito, P.; Garibotto, G.; Picciotto, D.; Costigliolo, F.; Viazzi, F.; Conti, N.E. Nutritional Challenges in Pregnant Women with Renal Diseases: Relevance to Fetal Outcomes. Nutrients 2020, 12, 873. [Google Scholar] [CrossRef] [PubMed]
- Drugs.com. Available online: https://www.drugs.com/ (accessed on 9 February 2024).
- Hou, S. Pregnancy in chronic renal insufficiency and end-stage renal disease. Am. J. Kidney Dis. 1999, 33, 235–252. [Google Scholar] [CrossRef]
- Wiggins, K.L. Nutrition care of adult pregnant ESRD patients. In Nutrition Care of Renal Patients, 3rd ed.; Burrowes, J., Ed.; Academy of Nutrition and Dietetics: Chicago, IL, USA, 2002. [Google Scholar]
- Jungers, P.; Chauveau, D. Pregnancy in renal disease. Kidney Int. 1997, 52, 871–885. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.H. 14 Pregnancy in women on haemodialysis and peritoneal dialysis. Baillière’s Clin. Obstet. Gynaecol. 1994, 8, 481–500. [Google Scholar] [CrossRef] [PubMed]
- Giatras, I.; Levy, D.P.; Malone, F.D.; Carlson, J.A.; Jungers, P. Pregnancy during dialysis: Case report and management guidelines. Nephrol. Dial. Transplant. 1998, 13, 3266–3272. [Google Scholar] [CrossRef] [PubMed]
- Díaz, J.P.O.; Hernández, R.C.; Mayo, J.D.; Rodríguez, R.A.O.; Pérez, R.T. Diagnosis, evaluation, and management of renal diseases during Pregnancy. Rev. Habanera Cienc. Med. 2016, 15, 834–858. [Google Scholar]
- Alkhunaizi, A.; Melamed, N.; Hladunewich, M.A. Pregnancy in advanced chronic kidney disease and end-stage renal disease. Curr. Opin. Nephrol. Hypertens. 2015, 24, 252–259. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Reynolds, M.L.; Herrera, C.A. Chronic Kidney Disease and Pregnancy. Adv. Chronic Kidney Dis. 2020, 27, 461–468. [Google Scholar] [CrossRef]
- Brookhyser, J.; Wiggins, K. Medical nutrition therapy in pregnancy and kidney disease. Adv. Ren. Replace Ther. 1998, 5, 53–63. [Google Scholar] [CrossRef]
- Oliverio, A.L.; Hladunewich, M.A. End-Stage Kidney Disease and Dialysis in Pregnancy. Adv. Chronic Kidney Dis. 2020, 27, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Reyes-López, M.A.; Piccoli, G.B.; Leone, F.; Orozco-Guillén, A.; Perichart-Perera, O. Nutrition care for chronic kidney disease during pregnancy: An updated review. Eur. J. Clin. Nutr. 2020, 74, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients). J. Am. Diet. Assoc. 2005, 102, 1621–1631. [Google Scholar]
- National Kidney Foundation. Kidney Disease Outcomes Quality Initiative (KDOQI) clinical practice guidelines for nutrition in chronic renal failure. Am. J. Kidney Dis. 2000, 35, S1–S140. [Google Scholar]
- Fouque, D.; Vennegoor, M.; Pedrini, L.; Pizzarelli, F.; Tattersall, J.; Tordoir, J.; Vanholder, R.; Ter Wee, P.; Wanner, C.; Basci, A.; et al. EBPG guideline on nutrition: European best practice guidelines on haemodialysis: Endorsed by the European Renal Association-European Dialysis and Transplant Association (ERA-EDTA). Nephrol. Dial. Transplant. 2007, 22 (Suppl. S2), ii45–ii87. [Google Scholar] [CrossRef] [PubMed]
- Tangren, J.; Nadel, M.; Hladunewich, M.A. Pregnancy and End-Stage Renal Disease. Blood Purif. 2018, 45, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Alp Ikizler, T.; Flakoll, P.J.; Parker, R.A.; Hakim, R.M. Amino acid and albumin losses during hemodialysis. Kidney Int. 1994, 46, 830–837. [Google Scholar] [CrossRef]
- Vecchio, B.R.C.; Del Negro, V.; Savastano, G.; Porpora, M.G.; Piccioni, M.G. Dialysis on Pregnancy: An Overview. Women 2021, 1, 60–69. [Google Scholar] [CrossRef]
- Kapoor, N.; Makanjuola, D.; Shehata, H. Management of women with chronic renal disease in pregnancy. Obstet. Gynaecol. 2009, 11, 185–191. [Google Scholar] [CrossRef]
- Castellano, G.; Losappio, V.; Gesualdo, L. Update on pregnancy in chronic kidney disease. Kidney Blood Press. Res. 2011, 34, 253–260. [Google Scholar] [CrossRef]
- Rizzoni, G.; Ehrich, J.H.H.; Broyer, M.; Brunner, F.P.; Brynger, H.; Fassbinder, W.; Geerlings, W.; Selwood, N.H.; Tufveson, G.; Wing, A.J. Successful pregnancies in women on renal replacement therapy: Report from the EDTA Registry. Nephrol. Dial. Transplant. 1992, 7, 279–287. [Google Scholar] [CrossRef]
- Stover, J. Pregnancy and dialysis: An overview. Nephrol. Nurs. J. 2010, 37, 652–654. [Google Scholar] [PubMed]
- Hall, M.; Brunskill, N.J. Renal disease in pregnancy. Obstet. Gynaecol. Reprod. Med. 2010, 20, 131–137. [Google Scholar] [CrossRef]
- Kothari, M.; Td, H.; Singh, M. Dialysis and Pregnancy—A Review. Int. J. Nephrol. Kidney Fail. 2019, 5. [Google Scholar] [CrossRef]
- Seong Lim, C.T.; Wah, F.K. Pregnancy and Peritoneal Dialysis: An Updated Review. Eur. Med. J. Nephrol. 2018, 6, 74–84. [Google Scholar] [CrossRef]
- Hladunewich, M.; Vella, J.; August, P. Pregnancy in Patients with Nondialysis Chronic Kidney Disease; Lam, A.Q., Eckler, K., Eds. 2019. Available online: https://www.uptodate.com/contents/pregnancy-and-contraception-in-patients-with-nondialysis-chronic-kidney-disease (accessed on 9 February 2024).
- Alvestrand, A. Nutritional requirements of dialysis patients. In The Principles and Practice of Nephrology; Manning, S., Ed.; Mosby: St Louis, MO, USA, 1995; pp. 761–766. [Google Scholar]
- Bergström, J.; Fürst, P.; Alvestrand, A.; Lindholm, B. Protein and energy intake, nitrogen balance and nitrogen losses in patients treated with continuous ambulatory peritoneal dialysis. Kidney Int. 1993, 44, 1048–1057. [Google Scholar] [CrossRef] [PubMed]
- Vázquez Rodríguez, J.G. Peritoneal dialysis and pregnancy. Cir. Cir 2010, 78, 177. [Google Scholar] [PubMed]
- Hou, S. Daily dialysis in pregnancy. Hemodial. Int. 2004, 8, 167–171. [Google Scholar] [CrossRef]
- Onder, S.; Akbar, S.; Schmidt, R.J. Reproductive endocrinology in chronic kidney disease patients: New approaches to old challenges. Semin. Dial. 2016, 9, 447–457. [Google Scholar] [CrossRef]
- Manisco, G.; Potì’, M.; Maggiulli, G.; Di Tullio, M.; Losappio, V.; Vernaglione, L. Pregnancy in end-stage renal disease patients on dialysis: How to achieve a successful delivery. Clin. Kidney J. 2015, 8, 293–299. [Google Scholar] [CrossRef]
- Reddy, S.S.; Holley, J.L. The importance of increased dialysis and anemia management for infant survival in pregnant women on hemodialysis. Kidney Int. 2009, 75, 1133–1134. [Google Scholar] [CrossRef] [PubMed]
- Wiles, K.; de Oliveira, L. Dialysis in pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2019, 57, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Furaz-Czerpak, K.R.; Fernández-Juárez, G.; Moreno-de la Higuera, M.Á.; Corchete-Prats, E.; Puente-García, A.; Martín-Hernández, R. Pregnancy in women on chronic dialysis: A review. Nefrol. Publ. Of. Soc. Esp. Nefrol. 2012, 32, 287–294. [Google Scholar] [CrossRef]
- Singh, R.; Pradeep, Y. Pregnancy in women with chronic kidney disease. Clin. Queries Nephrol. 2012, 1, 205–214. [Google Scholar] [CrossRef]
- Stover, J. Nutritional Management of Pregnancy in Chronic Kidney Disease. Adv. Chronic Kidney Dis. 2007, 14, 212–214. [Google Scholar] [CrossRef] [PubMed]
- National Research Council (US) Subcommittee on the Tenth Edition of the Recommended Dietary Allowances. The National Academies Collection: Reports funded by National Institutes of Health. In Recommended Dietary Allowances, 10th ed.; National Research Council-National Academy Press: Washington, DC, USA, 1989. [Google Scholar]
- Shehaj, L.; Kazancıoğlu, R. Pregnancy in Chronic Kidney Disease. Kidney Dial. 2023, 3, 152–162. [Google Scholar] [CrossRef]
- Vázquez-Rodríguez, J.G. Hemodialysis and pregnancy: Technical aspects. Cir. Y Cir. 2010, 78, 99. [Google Scholar]
- Porter, A. A Review of the Pregnant ESRD Patient. Kidney 2009, 18, 238. [Google Scholar] [CrossRef]
- Hou, S. Pregnancy in Peritoneal Dialysis Patients. Indian J. Perit. Dial. 2005, 8, 14–16. [Google Scholar]
- Nikolskaya, I.G.; Prokopenko, E.I. Pregnancy in end-stage chronic renal failure and hemodialysis treatment. Russ. Bull. Obstet.-Gynecol. 2014, 14, 29–36. [Google Scholar]
- Bahadi, A.; El Kabbaj, D.; Guelzim, K.; Kouach, J.; Hassani, M.; Maoujoud, O.; Aattif, M.; Kadiri, M.; Montassir, D.; Zajjari, Y.; et al. Pregnancy during hemodialysis: A single center experience. Saudi J. Kidney Dis. Transplant. 2010, 21, 646–651. [Google Scholar]
- Hui, D.; Hladunewich, M.A. Chronic Kidney Disease and Pregnancy. Obstet. Gynecol. 2019, 133, 1182–1194. [Google Scholar] [CrossRef]
- Davison, J.M. Dialysis, Transplantation, and Pregnancy. Am. J. Kidney Dis. 1991, 17, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Hou, S. Pregnancy in Women Requiring Dialysis for Renal Failure. Am. J. Kidney Dis. 1987, 9, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Oliverio, A.L.; Bramham, K.; Hladunewich, M.A. Pregnancy and CKD: Advances in Care and the Legacy of Dr Susan Hou. Am. J. Kidney Dis. 2021, 78, 865–875. [Google Scholar] [CrossRef]
- Ramin, S.M.; Vidaeff, A.C.; Yeomans, E.R.; Gilstrap, L.C. Chronic Renal Disease in Pregnancy. Obstet. Gynecol. 2006, 108, 1531–1539. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.S.; Okun, N.; Kjellstrand, C.M. Pregnancy in chronic dialysis: A review and analysis of the literature. Int. J. Artifical Organs 1998, 21, 259–268. [Google Scholar] [CrossRef]
- Giannattasio, M.; Giannattasio, F.; Gernone, G. Pharmacological and nutritional problems in pregnant patient on chronic dialysis. G. Ital. Di Nefrol. Organo Uff. Della Soc. Ital. Di Nefrol. 2017, 34, gin-34. [Google Scholar]
- Hou, S.H.; Grossman, S.D. Pregnancy in Chronic Dialysis Patients. Semin. Dial. 1990, 3, 224–229. [Google Scholar] [CrossRef]
- Grossman, S.D.; Hou, S.; Moretti, M.; Saran, M. Nutrition in the Pregnant Dialysis Patient. J. Ren. Nutr. 1993, 3, 56–66. [Google Scholar] [CrossRef]
- Bili, E.; Tsolakidis, D.; Stangou, S.; Tarlatzis, B. Pregnancy management and outcome in women with chronic kidney disease. Hippokratia 2013, 17, 163–168. [Google Scholar] [PubMed]
- Lim, T.S.C.; Shanmuganathan, M.; Wong, I.; Goh, B.L. Successful multigravid pregnancy in a 42-year-old patient on continuous ambulatory peritoneal dialysis and a review of the literature. BMC Nephrol. 2017, 18, 108. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, K.; Vuppali, M.; Abreo, K. Patient outcome in pregnancy requiring dialysis: A case series. Open Urol. Nephrol. J. 2014, 7, 52–55. [Google Scholar] [CrossRef]
- Kondakova, E.V.; Filat’eva, A.E.; Lobanova, N.A.; Nagaev, E.I.; Sarimov, R.M.; Gudkov, S.V.; Vedunova, M.V. Case report: Applicability of breastfeeding the child of a patient with kidney failure with replacement therapy. Front. Med. 2023, 10, 1098324. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Zhang, Y.; Wang, X.; Zhang, Y.; Fan, Y.; Shi, H.; Dai, H. Successful pregnancy and delivery in uremic patients with maintenance hemodialysis: A case report. Medicine 2018, 97, e13614. [Google Scholar] [CrossRef] [PubMed]
- Arai, H.; Mori, K.P.; Yokoi, H.; Mizuta, K.; Ogura, J.; Suginami, K.; Endo, T.; Ikeda, Y.; Matsubara, T.; Tsukamoto, T.; et al. Intensified hemodialysis for complicated pregnancy in a primigravida with advanced maternal age: A case report with literature review focusing on appropriate hemodialysis management during pregnancy. Ren. Replace Ther. 2020, 6, 47. [Google Scholar] [CrossRef]
- Sprenger-Mähr, H.; Zitt, E.; Kronbichler, A.; Cejna, M.; Lhotta, K. A hemodialysis patient with bone disease after pregnancy: A case report. BMC Nephrol. 2019, 20, 425. [Google Scholar] [CrossRef] [PubMed]
- Mambap, A.T.; Bechem, E.; Kan, K.M.; Laah, S.N.; Sunjoh, F.; Ashuntantang, G.E. Case report: 11 years on hemodialysis with a 4-year-old baby girl: A success story. Front. Med. 2023, 9, 1091568. [Google Scholar] [CrossRef]
- Buil, B.A.; González, C.L.; Zamora, L.M.; Lamarca, M.S.; Villagrasa, E.V.; Gil, P.I. Successful pregnancy in patients on hemodialysis. Review and Recommendations. Enferm. Nefrol. 2015, 18, 309–314. [Google Scholar]
- Seker, A. Two successive pregnancies in a patient during 14 years of hemodialysis: A case report. J. Med. Case Rep. 2016, 10, 50. [Google Scholar] [CrossRef]
- Shanmugalingam, R.; Cole-Clark, A.; Lowrie, E.; Hennessy, A.; Makris, A. Clinical Use of Angiogenic Factors in Managing a Pregnant Woman on Hemodialysis to Term. Kidney Int. Rep. 2021, 6, 1449–1453. [Google Scholar] [CrossRef] [PubMed]
- Haase, M.; Morgera, S.; Bamberg, C.; Halle, H.; Martini, S.; Hocher, B.; Diekmann, F.; Dragun, D.; Peters, H.; Neumayer, H.-H.; et al. A systematic approach to managing pregnant dialysis patients—The importance of an intensified haemodiafiltration protocol. Nephrol. Dial. Transplant. 2005, 20, 2537–2542. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Diao, W.; Tang, Q.; Jiang, X. A successful pregnancy and parturition in a patient with anuria undergoing maintenance hemodialysis for 6 years: A case report of a 3-year-follow-up. BMC Pregnancy Childbirth 2015, 15, 218. [Google Scholar] [CrossRef] [PubMed]
- Hull, A.R. More dialysis appears beneficial for pregnant ESRD patients (at least in Belgium). Am. J. Kidney Dis. 1998, 31, 863–864. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, F.; Romeo, R.; Ursu, M.; Tapia, A.; Vukusich, A. Pregnancy during dialysis. Experience in six patients. Rev. Med. Chile 2013, 141, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Choi, C.Y.; Cho, N.J.; Park, S.; Gil, H.W.; Kim, Y.S.; Lee, E.Y. A case report of successful pregnancy and delivery after peritoneal dialysis in a patient misdiagnosed with primary infertility. Medicine 2018, 97, e11148. [Google Scholar] [CrossRef] [PubMed]
- Tuot, D.; Gibson, S.; Caughey, A.B.; Frassetto, L.A. Intradialytic hyperalimentation as adjuvant support in pregnant hemodialysis patients: Case report and review of the literature. Int. Urol. Nephrol. 2010, 42, 233–237. [Google Scholar] [CrossRef]
- Molaison, E.F.; Baker, K.; Bordelon, M.A.; Brodie, P.; Powell, K. Successful management of pregnancy in a patient receiving hemodialysis. J. Ren. Nutr. 2003, 13, 229–232. [Google Scholar] [CrossRef]
- Nakabayashi, M.; Adachi, T.; Itoh, S.; Kobayashi, M.; Mishina, J.; Nishida, H. Perinatal and infant outcome of pregnant patients undergoing chronic hemodialysis. Nephron 1999, 82, 27–31. [Google Scholar] [CrossRef]
- Pires, A.; Branco, P.; Adragão, A.; Borges, A. Gravidez e Diálise. 2000. Available online: https://www.semanticscholar.org/paper/Gravidez-e-Di%C3%A1lise-Pires-Branco/247b7cda38b3f48db509588db961b4d4e57b6e17#citing-papers (accessed on 9 February 2024).
- Giofrè, F.; Pugliese, C.; Alati, G.; Messina, A.; Tramontana, D. Three successive pregnancies in a patient with chronic renal disease progressing from chronic renal dysfunction through to institution of dialysis during pregnancy and then on to maintenance dialysis. Nephrol. Dial. Transplant. 2007, 22, 1236–1240. [Google Scholar] [CrossRef]
- Malik, G.H.; al-Wakeel, J.S.; Shaikh, J.F.; al-Mohaya, S.; Dohami, H.; Kechrid, M.; el Gamal, H. Three successive pregnancies in a patient on haemodialysis. Nephrol. Dial. Transplant. 1997, 12, 1991–1993. [Google Scholar] [CrossRef] [PubMed]
- Campos-Collado, A.X.; Reyes-López, M.A.; Orozco-Guillén, A.; Muñoz-Manrique, C.; Perichart-Perera, O. Medical nutrition therapy for chronic kidney disease in pregnancy: A case report. J. Acad. Nutr. Diet. 2016, 116, 213–218. [Google Scholar] [CrossRef]
- Wiggins, K.L. Guidelines for Nutrition Care of Renal Patients, 3rd ed.; American Dietetic Association: Chicago, IL, USA, 2001. [Google Scholar]
- Stover, J. Pregnancy and chronic kidney disease. In A Clinical Guide to Nutrition Care in Kidney Disease, 2nd ed.; Byham-Gray, L., Stover, J., Wiesen, K., Eds.; Academy of Nutrition and Dietetics: Chicago, IL, USA, 2013. [Google Scholar]
- Reister, F.; Reister, B.; Heyl, W.; Riehl, J.; Schroder, W.; Mann, H.; Rath, W. Dialysis and Pregnancy—A Case Report and Review of the Literature. Ren. Fail. 1999, 21, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Swaroop, R.; Zabaneh, R.; Parimoo, N. Pregnancy in end-stage renal disease patients on hemodialysis: Two case reports. Cases J. 2009, 2, 8139. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.; Unnikrishnan, D.; Lwin, L.N.; Villanueva, H.J.; Tannenberg, A.M. Successful triplet pregnancy in a patient on chronic haemodialysis. Nephrol. Dial. Transplant. 2004, 19, 994–997. [Google Scholar] [CrossRef] [PubMed]
- Luciani, G.; Bossola, M.; Tazza, L.; Panocchia, N.; Liberatori, M.; De Carolis, S.; Piccioni, E.; De Carolis, M.P.; Caruso, A.; Castagneto, M. Pregnancy during chronic hemodialysis: A single dialysis-unit experience with five cases. Ren. Fail. 2002, 24, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Hadj Sadek, B.; Kejji, S.; Rhou, H.; Ezzaitouni, F.; Ouzeddoun, N.; Bayahia, R.; Benamar, L. Pregnancy in chronic hemodialysis patients. J. Gynecol. Obstet. Biol. Reprod. 2011, 40, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Pepperell, R.J.; Adam, R.; Dawborn, J.K. Haemodialysis in the Management of Chronic Renal Failure during Pregnancy. Aust. N. Z. J. Obstet. Gynaecol. 1970, 10, 180–186. [Google Scholar] [CrossRef]
- Abu-Zaid, A.; Nazer, A.; AlOmar, O.; Al-Badawi, I.A. Successful pregnancy in a 31-year-old peritoneal dialysis patient with bilateral nephrectomy. Case Rep. Obstet. Gynecol. 2013, 2013, 173405. [Google Scholar] [CrossRef]
- Al-Saran, K.A.; Sabry, A.A. Pregnancy in dialysis patients: A case series. J. Med. Case Rep. 2008, 2, 10. [Google Scholar] [CrossRef]
- Ackrill, P.; Goodwin, F.; Marsh, F.; Stratton, D.; Wagman, H. Successful pregnancy in patient on regular dialysis. Br. Med. J. 1975, 2, 172–174. [Google Scholar] [CrossRef] [PubMed]
- Gómez Vázquez, J.A.; Martínez Calva, I.E.; Fernández, R.M.; León, V.E.; Cardona, M.; Noyola, H. Pregnancy in end-stage renal disease patients and treament with peritoneal dialysis: Report of two cases. Perit. Dial. Int. 2007, 27, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, E.; Ramrattan, A.; Sahadeo, A.; Brathwaite, E.; Soobrattie, S. A successful pregnancy of a dialysis patient in the Eastern Caribbean. Nephrol. Ren. Dis. 2021, 6. [Google Scholar] [CrossRef]
- Alhwiesh, A. Pregnancy in peritoneal dialysis and an infant with a ventricular septal defect. Saudi J. Kidney Dis. Transplant. 2015, 26, 111–114. [Google Scholar] [CrossRef]
- Pipili, C.; Grapsa, E.; Koutsobasili, A.; Sorvinou, P.; Poirazlar, E.; Kiosses, D.; Xatzigeorgiou, G. Pregnancy in dialysis-dependent women-the importance of frequent dialysis and collaborative care: A case report. Hemodial. Int. 2011, 15, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Ramadani, S.; Nasution, A.; Nasution, S.; Lubis, H. Pregnancy in chronic dialysis, late diagnosis, and other problems. In Proceedings of the IOP Conference Series: Earth and Environmental Science; IOP Publishing: Bristol, UK, 2018; p. 012113. [Google Scholar]
- Hussain, S.A.; Savin, V.; Piering, W.; Tomasi, J.; Blumenthal, S. Phosphorus-enriched hemodialysis during pregnancy: Two case reports. Hemodial. Int. 2005, 9, 147–152. [Google Scholar] [CrossRef]
- Kedzierska, K.; Kwiatkowski, S.; Torbé, A.; Marchelek-Myśliwiec, M.; Marcinkiewicz, O.; Bobrek-Lesiakowska, K.; Gołembiewska, E.; Kwiatkowska, E.; Rzepka, R.; Ciechanowski, K.; et al. Successful pregnancy in the patient with Fanconi-Bickel syndrome undergoing daily hemodialysis. Am. J. Med. Genet. Part A 2011, 155, 2028–2030. [Google Scholar] [CrossRef] [PubMed]
- Avram, M.M.; Bonomini, L.V.; Sreedhara, R.; Mittman, N. Predictive value of nutritional markers (albumin, creatinine, cholesterol, and hematocrit) for patients on dialysis for up to 30 years. Am. J. Kidney Dis. 1996, 28, 910–917. [Google Scholar] [CrossRef]
- López-Menchero, R.; Albero, M.D.; Cabeza, B.; Álvarez, L.; Del Pozo, C.; Sánchez, L. Successful pregnancy in a patient with systemic lupus erythematosus on hemodialysis. Nefrologia 2004, 24, 70–74. [Google Scholar]
- Coyle, M.; Sulger, E.; Fletcher, C.; Rouse, D. A successful 39-week pregnancy on hemodialysis: A case report. Nephrol. Nurs. J. J. Am. Nephrol. Nurses’ Assoc. 2008, 35, 348. [Google Scholar]
- Sheriff, M.H.R.; Hardman, M.; Lamont, C.A.R.; Shepherd, R.; Warren, D.J. Successful Pregnancy in a 44-Year-Old Haemodialysis Patient. BJOG Int. J. Obstet. Gynaecol. 1978, 85, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Walsh, A.-M. Management of a pregnant woman dependent on haemodialysis. EDTNA/ERCA J. (Engl. Ed.) 2002, 28, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.P.; Giatras, I.; Jungers, P. Pregnancy and end-stage renal disease—Past experience and new insights. Nephrol. Dial. Transplant. 1998, 13, 3005–3007. [Google Scholar] [CrossRef] [PubMed]
- Cocîrţă, E.; Peltecu, G.; Panaitescu, A.M. Pregnancy in pacients on hemodialysis for end stage renal disease. Review of the literature and case report. Obstet. Si Ginecol. 2016, 64, 177–181. [Google Scholar]
- Levy, A.; Fraser, D.; Katz, M.; Mazor, M.; Sheiner, E. Maternal anemia during pregnancy is an independent risk factor for low birthweight and preterm delivery. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 122, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Guida, B.; Pollio, F.; Nastasi, A.; Trio, R.; Laccetti, R.; Di Lieto, A.; Citarella, F.; Memoli, B. Nutritional intervention in a hemodialysis pregnant woman: A case report. Clin. Nutr. 2003, 22, 205–207. [Google Scholar] [CrossRef]
- Bagon, J.A.; Vernaeve, H.; De Muylder, X.; Lafontaine, J.J.; Martens, J.; Van Roost, G. Pregnancy and dialysis. Am. J. Kidney Dis. 1998, 31, 756–765. [Google Scholar] [CrossRef]
- McPhatter, L.L.; Drumheller, J.C. Nutritional implications of pregnancy in dialysis: A case study. Nephrol. Nurs. J. 2008, 35, 207–209. [Google Scholar]
- Stover, J. Pregnancy and dialysis. In A Clinical Guide to Nutrition Care in Kidney Disease; American Dietetic Association: Chicago, IL, USA, 2004; pp. 121–126. [Google Scholar]
- Sandhu, A.; Regmi, A.; Buchwald, D.; Tzamaloukas, A.H. Pregnancy or Uremia?—Case Report and Review of Conception, Pregnancy, and Complications in Peritoneal Dialysis Patients. Curēus 2014, 6, e206. [Google Scholar] [CrossRef]
- Brookhyser, J. The use of parenteral nutrition supplementation in pregnancy complicated by end-stage renal disease. J. Am. Diet. Assoc. 1989, 89, 93–94. [Google Scholar] [CrossRef]
- Park, J.-C.; Rhee, J.-H.; Kim, J.-I. Two cases of pregnancy in women requiring dialysis (CAPD/HD) for renal failure. Korean J. Obstet. Gynecol. 2006, 49, 1764–1770. [Google Scholar]
- Yattara, H.; Samaké, M.; Sy, S.; Diallo, D.; Coulibaly, N.; Djiguiba, K.; Fofana, A.S.; Coulibaly, S.; Toure, A.; Coulibaly, M.; et al. Pregnancy in Chronic Hemodialysis, Case Study. Le Mali Med. 2019, 34, 53–58. [Google Scholar]
- Abbassi, H.; Salah-Eddine, A.; Jersifi, H.; Samouh, N.; Moutabarrik, A.; Niang, A. Insuffisance rénale chronique et grossesse. Gynécologie Obs. Fertil. 2001, 29, 106–115. [Google Scholar] [CrossRef]
- Seed, E.; Gilbertson, E. Dialysis and a plant-based diet to achieve physiologic urea levels for fetal benefit: Normal pregnancy outcome despite chronic kidney disease and hypertension. Obstet. Med. 2022, 16, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Henderson, N. Nutritional management of pregnancy in a chronic hemodialysis patient with insulin-dependent diabetes mellitus. J. Ren. Nutr. 1996, 6, 222–228. [Google Scholar] [CrossRef]
- Melendez, R.; Franquero, C.; Gill, P.; Bakke, T. Successful pregnancy with CAPD. ANNA J. 1988, 15, 280–312. [Google Scholar] [PubMed]
- Gillit, D.; Stover, J.; Spinozzi, N.S. A Clinical Guide to Nutrition Care in End Stage Renal Disease; American Dietetic Association: Chicago, IL, USA, 1987. [Google Scholar]
- Hou, S.; Orlowski, J.; Pahl, M.; Ambrose, S.; Hussey, M.; Wong, D. Pregnancy in Women with End-Stage Renal Disease: Treatment of Anemia and Premature Labor. Am. J. Kidney Dis. 1993, 21, 16–22. [Google Scholar] [CrossRef]
- Brookhyser, J.; Kinzner, C.; Pahre, S. A case study of two successful pregnancies in a patient with end-stage renal disease. J. Ren. Nutr. 1996, 6, 26–33. [Google Scholar] [CrossRef]
- Amoah, E.; Arab, H. Pregnancy in a Hemodialysis Patient with No Residual Renal Function. Am. J. Kidney Dis. 1991, 17, 585–587. [Google Scholar] [CrossRef]
- Shah, A.; Bailey, E.; Hughes, S. Goodpasture’s syndrome, haemodialysis and pregnancy. Br. J. Hosp. Med. 2007, 68, 48–49. [Google Scholar] [CrossRef]
- Dunbeck, D.; Klopstein, K.; Heroux, J.; Brencick, K. Peritoneal dialysis patient completes successful pregnancy. ANNA J. 1992, 19, 269–272. [Google Scholar] [PubMed]
- Cattran, D.C.; Benzie, R.J. Pregnancy in a Continuous Ambulatory Peritoneal Dialysis Patient. Perit. Dial. Int. 1983, 3, 13–14. [Google Scholar] [CrossRef]
- Villa, G.; Montagna, G.; Segagni, S. Pregnancy in chronic dialysis. A case report and a review of the literature. G. Ital. Nefrol. 2007, 24, 132–140. [Google Scholar] [PubMed]
- Racette, N. Chronic Ambulatory Peritoneal Dialysis (CAPD) in Pregnancy: A Case Report and Review. J. SOGC 1997, 19, 1373–1380. [Google Scholar] [CrossRef]
- Rolfes, S.R.; DeBruyne, L.K.; Whitney, E.N. Life Span Nutrition: Conception through Life; Wadsworth Publishing Company, Inc.: Belmont, CA, USA, 1998. [Google Scholar]
- Unzelman, R.F.; Alderfer, G.R.; Chojnacki, R.E. Pregnancy and chronic hemodialysis. Trans.—Am. Soc. Artif. Intern. Organs 1973, 19, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Perry, L.A. A multidisciplinary approach to the management of pregnant patients with end-stage renal disease. J. Perinat. Neonatal Nurs. 1994, 8, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Sivasuthan, G.; Dahwa, R.; John, G.T.; Ranganathan, D. Dialysis and Pregnancy in End Stage Kidney Disease Associated with Lupus Nephritis. Case Rep. Med. 2013, 2013, 923581–923587. [Google Scholar] [CrossRef]
- Mercadal, L.; Nizard, J. Prepregnancy counselling and management of pregnancy in haemodialysis patients. Nephrol. Dial. Transplant. 2020, 35, 219–221. [Google Scholar] [CrossRef]
- Hou, S. Modification of dialysis regimens for pregnancy. Int. J. Artif. Organs 2002, 25, 823–826. [Google Scholar] [CrossRef]
- Ellis, P. Back to basics: Pregnancy and dialysis. J. Ren. Nurs. 2012, 4, 202–203. [Google Scholar] [CrossRef]
- Jagielski, J.B. Optimizing nutritional care for pregnant patients on hemodialysis. J. Ren. Nutr. 2015, 25, e19–e21. [Google Scholar] [CrossRef] [PubMed]
- McCann, L. Practical Resource for Comprehensive Nutrition Care in CKD. Pocket Guide to Nutrition Assessment of the Patient with Chronic Kidney Disease: Improving Global Outcomes Diabetes Work Group; National Kidney Foundation: New York, NY, USA, 2009. [Google Scholar]
- Lawrence, J. Pregnancy and Kidney Disease. 2012, pp. 163–170. Available online: https://www.semanticscholar.org/paper/Pregnancy-and-Kidney-Disease-Lawrence/23cf804216cf8394a10a8a0e2582f37a8815f7e4 (accessed on 9 February 2024).
- Wiggins, K.L.; Harvey, K.S. A review of guidelines for nutrition care of renal patients. J. Ren. Nutr. 2002, 12, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [CrossRef]
- Flecha, A. Pharmacologic, Breastfeeding, and Nutritional Considerations during Pregnancy and Postpartum. In Obstetric and Gynecologic Nephrology: Women’s Health Issues Patient Kidney Disease; Springer: Cham, Switzerland, 2020; pp. 245–266. [Google Scholar] [CrossRef]
- Pahl, M.V. Pregnancy in Kidney Disease. In Endocrine Disorders in Kidney Disease: Diagnosis and Treatment; Springer: Cham, Switzerland, 2019; pp. 139–150. [Google Scholar] [CrossRef]
- Sandhu, A.S. Peritoneal Dialysis and Pregnancy. In Some Special Problems in Peritoneal Dialysis; IntechOpen: London, UK, 2016. [Google Scholar] [CrossRef]
- Stover, J. Pregnancy. In Nutrition in Kidney Disease; Humana: Totowa, NJ, USA, 2008; pp. 419–428. [Google Scholar]
- Vidal, M.L.; Ursu, M.; Martinez, A.; Roland, S.S.; Wibmer, E.; Pereira, D.; Subiza, K.; Alonso, W.; Seijas, L.; Piazze, S.; et al. Nutritional control of pregnant women on chronic hemodialysis. J. Ren. Nutr. Off. J. Counc. Ren. Nutr. Natl. Kidney Found. 1998, 8, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Stover, J. Pregnancy. In Nutrition in Kidney Disease; Byham-Gray, L.D., Burrowes, J.D., Chertow, G.M., Eds.; Humana Press: Totowa, NJ, USA, 2014; pp. 291–298. [Google Scholar]
- Hou, S. Pregnancy in women treated with dialysis: Lessons from a large series over 20 years. Am. J. Kidney Dis. 2010, 56, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Stover, J.; Trolinger, M. Pregnancy. In Nutrition in Kidney Disease; Humana: Louisville, KY, USA, 2020; pp. 347–355. [Google Scholar]
- Kominiarek, M.A.; Rajan, P. Nutrition Recommendations in Pregnancy and Lactation. Med. Clin. N. Am. 2016, 100, 1199–1215. [Google Scholar] [CrossRef]
- Plant, L. Pregnancy and dialysis. In Renal Disease in Pregnancy; RCOG Press: London, UK, 2008; pp. 61–68. [Google Scholar]
- Stover, J. Pregnancy and Chronic Kidney Disease; Humana Press: Totowa, NJ, USA, 2022. [Google Scholar]
- Goody, A.J.; Umans, J.G. Pregnancy and dialysis. In Replacement of Renal Function by Dialysis; Springer: Berlin/Heidelberg, Germany, 2004; pp. 1249–1257. [Google Scholar]
- Vellanki, K.; Hou, S. Chronic Kidney Disease in Pregnancy. In Obstetric and Gynecologic Nephrology: Women’s Health Issues in the Patient with Kidney Disease; Springer: Cham, Switzerland, 2019; pp. 165–181. [Google Scholar] [CrossRef]
- Shahid, K.; Plant, L.; Hladunewich, M. Pregnancy and Dialysis. In Renal Disease in Pregnancy; Cambridge University Press: Cambridge, UK, 2018; p. 107. [Google Scholar]
- Piccoli, G.B.; Attini, R.; Torreggiani, M.; Orozco-Guillén, A. Pregnancy in Dialysis Patients. In Handbook of Dialysis Therapy; Elsevier: Amsterdam, The Netherlands, 2023; pp. 513–529. [Google Scholar]
- Hou, S. Pregnancy in Women on Dialysis: Is Success a Matter of Time? Clin. J. Am. Soc. Nephrol. 2008, 3, 312–313. [Google Scholar] [CrossRef]
- McKay, D.B.; Josephson, M.A. Pregnancy after Kidney Transplantation. Clin. J. Am. Soc. Nephrol. 2008, 3, S117–S125. [Google Scholar] [CrossRef]
- ACOG Committee Opinion No. 495: Vitamin D: Screening and supplementation during pregnancy. Obs. Gynecol. 2011, 118, 197–198. [CrossRef]
- Barua, M.; Hladunewich, M.; Keunen, J.; Pierratos, A.; McFarlane, P.; Sood, M.; Chan, C.T. Successful Pregnancies on Nocturnal Home Hemodialysis. Clin. J. Am. Soc. Nephrol. 2008, 3, 392–396. [Google Scholar] [CrossRef]
- Dietary Reference Intakes (DRI’s): Recommended Intakes for Individuals, Vitamins and Dietary Reference Intakes (DRI’s): Recommended Intakes for Individuals, Elements; Institute of Medicine, US National Academies: Washington, DC, USA, 2004.
- Grossman, S.; Hou, S. Handbook of Dialysis, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2000; pp. 624–636. [Google Scholar]
- Hladunewich, M.A.; Hou, S.; Odutayo, A.; Cornelis, T.; Pierratos, A.; Goldstein, M.; Tennankore, K.; Keunen, J.; Dini, H.; Chan, C.T. Intensive Hemodialysis Associates with Improved Pregnancy Outcomes: A Canadian and United States Cohort Comparison. J. Am. Soc. Nephrol. 2014, 25, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Wiebe, N.; Hemmelgarn, B.; Klarenbach, S.; Field, C.; Manns, B.; Thadhani, R.; Gill, J. Trace elements in hemodialysis patients: A systematic review and meta-analysis. BMC Med. 2009, 7, 25. [Google Scholar] [CrossRef] [PubMed]
- Molloy, A.M.; Kirke, P.N.; Brody, L.C.; Scott, J.M.; Mills, J.L. Effects of folate and vitamin B12 deficiencies during pregnancy on fetal, infant, and child development. Food Nutr. Bull. 2008, 29, S101–S111, discussion S112-S105. [Google Scholar] [CrossRef] [PubMed]
- Bastos Maia, S.; Rolland Souza, A.S.; Costa Caminha, M.F.; Lins da Silva, S.; Callou Cruz, R.; Carvalho Dos Santos, C.; Batista Filho, M. Vitamin A and Pregnancy: A Narrative Review. Nutrients 2019, 11, 681. [Google Scholar] [CrossRef]
- Okundaye, I.; Abrinko, P.; Hou, S. Registry of Pregnancy in Dialysis Patients. Obstet. Gynecol. Surv. 1998, 53, 665–667. [Google Scholar] [CrossRef]
- Toma, H.; Tanabe, K.; Tokumoto, T.; Kobayashi, C.; Yagisawa, T. Pregnancy in women receiving renal dialysis or transplantation in Japan: A nationwide survey. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 1999, 14, 1511–1516. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Jang, H.; Chung, B.H.; Youn, Y.A.; Sung, I.K.; Kim, Y.S.; Yang, C.W. The successful clinical outcomes of pregnant women with advanced chronic kidney disease. Kidney Res. Clin. Pract. 2016, 35, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine; National Research Council Committee to Reexamine IOM. Pregnancy Weight Guidelines. In Weight Gain during Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Breymann, C.; Visca, E.; Huch, R.; Huch, A. Efficacy and safety of intravenously administered iron sucrose with and without adjuvant recombinant human erythropoietin for the treatment of resistant iron-deficiency anemia during pregnancy. Am. J. Obstet. Gynecol. 2001, 184, 662–667. [Google Scholar] [CrossRef]
- Khalafallah, A.A.; Dennis, A.E.; Ogden, K.; Robertson, I.; Charlton, R.H.; Bellette, J.M.; Shady, J.L.; Blesingk, N.; Ball, M. Three-year follow-up of a randomised clinical trial of intravenous versus oral iron for anaemia in pregnancy. BMJ Open 2012, 2, e000998. [Google Scholar] [CrossRef]
- Juul, S.E.; Derman, R.J.; Auerbach, M. Perinatal Iron Deficiency: Implications for Mothers and Infants. Neonatology 2019, 115, 269–274. [Google Scholar] [CrossRef]
- Muth, I.; Stover, J. Pregnancy and Dialysis: A Discussion and Case Review: A Clinical Guide to Nutrition Care in End Stage Renal Disease, 2nd ed.; American Dietetic Association: Chicago, IL, USA, 1994. [Google Scholar]
- Mahan, L.; Escott-Stump, S. Krause’s Food, Nutrition and Diet Therapy, 9th ed.; Saunders: Philadelphia, PA, USA, 1996. [Google Scholar]
- Imbasciati, E.; Ponticelli, C. Pregnancy and Renal Disease: Predictors for Fetal and Maternal Outcome. Am. J. Nephrol. 2008, 11, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Abrams, B. Weight gain and energy intake during pregnancy. Clin. Obstet. Gynecol. 1994, 37, 515–527. [Google Scholar] [CrossRef] [PubMed]
- Gottschlich, M.M.; Shronts, E.P.; Matarese, L.E. Nutrition Support Dietetics: Core Curriculum; American Society for Parenteral and Enteral Nutrition: Silver Spring, MD, USA, 1993; pp. 125–136. Available online: https://books.google.com.au/books?id=HIuFOwAACAAJ (accessed on 9 February 2024).
- Blackburn, G.L.; Bell, S.J.; Mullen, J.L. Nutritional Medicine: A Case Management Approach; Saunders Philadelphia: Philadelphia, PA, USA, 1989. [Google Scholar]
- Cotton, A. Enteral Nutrition in the Dialysis Patient. Diet. Curr. 1995, 22, 1–2. [Google Scholar]
- Maurer, G.; Abriola, D. Pregnancy following renal transplant. J. Perinat. Neonatal Nurs. 1994, 8, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, K.M.; Catalano, P.M.; Yaktine, A.L. New guidelines for weight gain during pregnancy: What obstetrician/gynecologists should know. Curr. Opin. Obstet. Gynecol. 2009, 21, 521–526. [Google Scholar] [CrossRef]
- Hod, M.; Kapur, A.; Sacks, D.A.; Hadar, E.; Agarwal, M.; Di Renzo, G.C.; Roura, L.C.; McIntyre, H.D.; Morris, J.L.; Divakar, H. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care. Int. J. Gynecol. Obstet. 2015, 131, S173–S211. [Google Scholar] [CrossRef]
- Duarte-Gardea, M.O.; Gonzales-Pacheco, D.M.; Reader, D.M.; Thomas, A.M.; Wang, S.R.; Gregory, R.P.; Piemonte, T.A.; Thompson, K.L.; Moloney, L. Academy of Nutrition and Dietetics Gestational Diabetes Evidence-Based Nutrition Practice Guideline. J. Acad. Nutr. Diet. 2018, 118, 1719–1742. [Google Scholar] [CrossRef] [PubMed]
- Chronic Kidney Disease (2010) Evidence-Based Nutrition Practice Guideline; Academy of Nutrition and Dietetics: Chicago, IL, USA, 2015.
- Hou, S. Pregnancy and renal disease. In Educational Review Manual in Nephrology; Castle Connolly Graduate Medical Publishing, Ltd.: New York, NY, USA, 2008; pp. 251–278. [Google Scholar]
- Lim, C.T.S.; Wah, F.K. Pregnancy and peritoneal dialysis: An updated review. Nephrology 2018, 6, 74–81. [Google Scholar]
- Young, B.E.; McNanley, T.J.; Cooper, E.M.; McIntyre, A.W.; Witter, F.; Harris, Z.L.; O’Brien, K.O. Vitamin D insufficiency is prevalent and vitamin D is inversely associated with parathyroid hormone and calcitriol in pregnant adolescents. J. Bone Min. Res. 2012, 27, 177–186. [Google Scholar] [CrossRef]
- Achebe, M.M.; Gafter-Gvili, A. How I treat anemia in pregnancy: Iron, cobalamin, and folate. Blood 2017, 129, 940–949. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Renvela (Sevelamer Carbonate) Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/022127s011lbl.pdf (accessed on 9 February 2024).
- Horjus, C.; Groot, I.; Telting, D.; van Setten, P.; van Sorge, A.; Kovacs, C.S.; Hermus, A.; de Boer, H. Cinacalcet for hyperparathyroidism in pregnancy and puerperium. J. Pediatr. Endocrinol. Metab. 2009, 22, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Hussar, D.A. New drugs 05, part I. Nursing 2005, 35, 54–61, quiz 61–53. [Google Scholar] [CrossRef]
- Podymow, T.; August, P.; Akbari, A. Management of renal disease in pregnancy. Obstet. Gynecol. Clin. N. Am. 2010, 37, 195–210. [Google Scholar] [CrossRef] [PubMed]
- Luders, C.; Titan, S.M.; Kahhale, S.; Francisco, R.P.; Zugaib, M. Risk Factors for Adverse Fetal Outcome in Hemodialysis Pregnant Women. Kidney Int. Rep. 2018, 3, 1077–1088. [Google Scholar] [CrossRef]
- Schoenaker, D.A.; Soedamah-Muthu, S.S.; Mishra, G.D. The association between dietary factors and gestational hypertension and pre-eclampsia: A systematic review and meta-analysis of observational studies. BMC Med. 2014, 12, 157. [Google Scholar] [CrossRef] [PubMed]
- Hussey, M.J.; Pombar, X. Obstetric care for renal allograft recipients or for women treated with hemodialysis or peritoneal dialysis during pregnancy. Adv. Ren. Replace Ther. 1998, 5, 3–13. [Google Scholar] [CrossRef]
- Chertow, G.M.; Ling, J.; Lew, N.L.; Lazarus, J.M.; Lowrie, E.G. The association of intradialytic parenteral nutrition administration with survival in hemodialysis patients. Am. J. Kidney Dis. 1994, 24, 912–920. [Google Scholar] [CrossRef]
- Smolle, K.H.; Kaufmann, P.; Holzer, H.; Druml, W. Intradialytic parenteral nutrition in malnourished patients on chronic haemodialysis therapy. Nephrol. Dial. Transpl. 1995, 10, 1411–1416. [Google Scholar]
- Ikizler, T.A.; Wingard, R.L.; Hakim, R.M. Interventions to treat malnutrition in dialysis patients: The role of the dose of dialysis, intradialytic parenteral nutrition, and growth hormone. Am. J. Kidney Dis. 1995, 26, 256–265. [Google Scholar] [CrossRef]
- Descombes, E.; Hanck, A.B.; Fellay, G. Water soluble vitamins in chronic hemodialysis patients and need for supplementation. Kidney Int. 1993, 43, 1319–1328. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Cano, N.J.; Franch, H.; Fouque, D.; Himmelfarb, J.; Kalantar-Zadeh, K.; Kuhlmann, M.K.; Stenvinkel, P.; TerWee, P.; Teta, D.; et al. Prevention and treatment of protein energy wasting in chronic kidney disease patients: A consensus statement by the International Society of Renal Nutrition and Metabolism. Kidney Int. 2013, 84, 1096–1107. [Google Scholar] [CrossRef] [PubMed]
- Regitz-Zagrosek, V.; Blomstrom Lundqvist, C.; Borghi, C.; Cifkova, R.; Ferreira, R.; Foidart, J.M.; Gibbs, J.S.; Gohlke-Baerwolf, C.; Gorenek, B.; Iung, B.; et al. ESC Guidelines on the management of cardiovascular diseases during pregnancy: The Task Force on the Management of Cardiovascular Diseases during Pregnancy of the European Society of Cardiology (ESC). Eur. Heart J. 2011, 32, 3147–3197. [Google Scholar] [CrossRef] [PubMed]
- Suitor, C.W. Perspectives on nutrition during pregnancy: Part I, Weight gain; Part II, Nutrient supplements. J. Am. Diet. Assoc. 1991, 91, 96–98. [Google Scholar] [CrossRef]
- Makoff, R. Water-Soluble Vitamin Status in Patients with Renal Disease Treated with Hemodialysis or Peritoneal Dialysis. J. Ren. Nutr. 1991, 1, 56–73. [Google Scholar] [CrossRef]
- Japanese Society of Nephrology. Clinical Practice Guidelines for the Management of Pregnancy in Kidney Disease Patients. Available online: http://cdn.jsn.or.jp/data/jsn-pregnancy.pdf (accessed on 9 February 2024).
- WHO. Guideline: Calcium Supplementation in Pregnant Women; WHO: Geneva, Switzerland, 2013; pp. 1–35. [Google Scholar]
- Giovannetti, S.; Maggiore, Q. A Low-Nitrogen Diet with Proteins of High Biological Value for Severe Chronic Uraemia. Lancet 1964, 283, 1000–1003. [Google Scholar] [CrossRef]
- Kaiser, L.; Allen, L.H. Position of the American Dietetic Association: Nutrition and Lifestyle for a Healthy Pregnancy Outcome. J. Am. Diet. Assoc. 2008, 108, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Smith, W.T.; Darbari, S.; Kwan, M.; O’Reilly-Green, C.; Devita, M.V. Pregnancy in Peritoneal Dialysis: A Case Report and Review of Adequacy and Outcomes. Int. Urol. Nephrol. 2005, 37, 145–151. [Google Scholar] [CrossRef]
- Macdougall, I.C. Optimal Iron Management in Patients Receiving Erythropoietin Therapy. Semin. Dial. 1998, 11, 10–13. [Google Scholar] [CrossRef]
- Confortini, P. Full term pregnancy and successful delivery in a patient on chronic hemodialysis. Proc. Eur. Dial. Transpl. Assoc. 1971, 8, 74–80. [Google Scholar]
- Tu, J. Nutrition and Fasting in Vietnamese Culture. Available online: http://ethnomed.org/cultures/vietnamese/viet_food.html (accessed on 9 February 2024).
- Okundaye, I.; Hou, S. Management of pregnancy in women undergoing continuous ambulatory peritoneal dialysis. Adv. Perit. Dial. 1996, 12, 151–155. [Google Scholar]
- Luders, C.; Martins Castro, M.C.; Titan, S.M.; De Castro, I.; Elias, R.M.; Abensur, H.; Romão, J.E., Jr. Obstetric Outcome in Pregnant Women on Long-term Dialysis: A Case Series. Am. J. Kidney Dis. 2010, 56, 77–85. [Google Scholar] [CrossRef]
- Hou, S. Conception and pregnancy in peritoneal dialysis patients. Perit. Dial. Int. 2001, 21 (Suppl. S3), S290–S294. [Google Scholar] [CrossRef] [PubMed]
- Keller, F.; Griesshammer, M.; Häussler, U.; Paulus, W.; Schwarz, A. Pregnancy and renal failure: The case for application of dosage guidelines. Drugs 2001, 61, 1901–1920. [Google Scholar] [CrossRef] [PubMed]
- Moranne, O.; Samouelian, V.; Lapeyre, F.; Pagniez, D.; Subtil, D.; Dequiedt, P.; Boulanger, E. Pregnancy and hemodialysis. Nephrologie 2004, 25, 287–292. [Google Scholar] [PubMed]
- Hou, S. Pregnancy in women with chronic renal disease. N. Engl. J. Med. 1985, 312, 836–839. [Google Scholar] [CrossRef] [PubMed]
- Kioko, E.M.; Shaw, K.M.; Clarke, A.D.; Warren, D.J. Successful pregnancy in a diabetic patient treated with continuous ambulatory peritoneal dialysis. Diabetes Care 1983, 6, 298–300. [Google Scholar] [CrossRef]
- Katz, M.; Quagliorello, J.; Young, B.K. Severe polycystic kidney disease in pregnancy: Report of fetal survival. Obstet. Gynecol. 1979, 53, 119–124. [Google Scholar]
- Schiro, K. Pregnancy and hemodialysis: Nutrition considerations. Am. Kidney Found. Newsl. Health Prof. 1987, 11, 3–11. [Google Scholar]
- Bakke, T. Nutrition considerations in renal disease: Pregnant patient on dialysis. Dial. Transplant. 1989, 18, 4. [Google Scholar]
- Rolfes, S.R.; DeBruyne, L.K.; Whitney, E.N. Life Span Nutrition: Conception through Life. 1990. Available online: https://www.semanticscholar.org/paper/Life-Span-Nutrition%3A-Conception-Through-Life-Rolfes-DeBruyne/1cf0d35c934138f87e122d5233d545abd6ca37ac (accessed on 9 February 2024).
- Pitkin, R. Calcium and the parathyroid gland. In Medical Complications during Pregnancy; Burrow, G., Ferris, T., Eds.; W.B. Saunders Company: Philadelphia, PA, USA, 1988; pp. 271–276. [Google Scholar]
- Allen, L.H. Anemia and iron deficiency: Effects on pregnancy outcome. Am. J. Clin. Nutr. 2000, 71, 1280s–1284s. [Google Scholar] [CrossRef]
- Williams, D.; Davison, J. Chronic kidney disease in pregnancy. BMJ 2008, 336, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Erick, M. Nutrition during pregnancy and lactation. In Krause’s Food and Nutrition Therapy; Mahan, L.K., Escott-Stump, S., Eds.; Saunders/Elsevier: St. Louis, MO, USA, 2008; p. 187. [Google Scholar]
- Korzets, A.; Azoulay, O.; Ori, Y.; Zevin, D.; Boaz, M.; Herman, M.; Chagnac, A.; Gafter, U. The use of intradialytic parenteral nutrition in acutely ill haemodialysed patients. J. Ren. Care 2008, 34, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Hou, S. Obstetrics and gynecology in dialysis patients. In Handbook of Dialysis; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2015. [Google Scholar]
- Frederiksen, M.C. Physiologic changes in pregnancy and their effect on drug disposition. Semin. Perinatol. 2001, 25, 120–123. [Google Scholar] [CrossRef] [PubMed]
- Hollis, B.W.; Wagner, C.L. Nutritional vitamin D status during pregnancy: Reasons for concern. Cmaj 2006, 174, 1287–1290. [Google Scholar] [CrossRef] [PubMed]
- Schroth, R.J.; Lavelle, C.L.; Moffatt, M.E. Review of vitamin D deficiency during pregnancy: Who is affected? Int. J. Circumpolar Health 2005, 64, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Lindheimer, M.; Katz, A. Renal physiology and disease in pregnancy. In The Kidney: Physiology and Pathophysiology, 3rd ed.; Seldin, D., Giebisch, G., Eds.; Lippincott, Williams & Wilkins: New York, NY, USA, 2000; pp. 2597–2644. [Google Scholar]
- Reddy, G.S.; Norman, A.W.; Willis, D.M.; Goltzman, D.; Guyda, H.; Solomon, S.; Philips, D.R.; Bishop, J.E.; Mayer, E. Regulation of vitamin D metabolism in normal human pregnancy. J. Clin. Endocrinol. Metab. 1983, 56, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Cole, D.E.; Hussain, S.A.; Piering, W.E.; Savin, V.J. Phosphate enriched hemodialysis during pregnancy A case report. J. Am. Soc. Nephrol. 2001, 12, 263A. [Google Scholar]
- Cabiddu, G.; Castellino, S.; Gernone, G.; Santoro, D.; Moroni, G.; Giannattasio, M.; Gregorini, G.; Giacchino, F.; Attini, R.; Loi, V.; et al. A best practice position statement on pregnancy in chronic kidney disease: The Italian Study Group on Kidney and Pregnancy. J. Nephrol. 2016, 29, 277–303. [Google Scholar] [CrossRef]
- Chazot, C.; Steiber, A.; Kopple, J.D. Vitamin Needs and Treatment for Chronic Kidney Disease Patients. J. Ren. Nutr. 2022, 33, S21–S29. [Google Scholar] [CrossRef]
- Tangirala, N.; Hladunewich, M.A. Hemodialysis Prescription in Pregnant Women. Kidney News 2023, 15, 17. [Google Scholar]
- Mousa, A.; Naqash, A.; Lim, S. Macronutrient and Micronutrient Intake during Pregnancy: An Overview of Recent Evidence. Nutrients 2019, 11, 443. [Google Scholar] [CrossRef] [PubMed]
- Waheed, A.A.; Pedraza, F.; Lenz, O.; Isakova, T. Phosphate control in end-stage renal disease: Barriers and opportunities. Nephrol. Dial. Transpl. 2013, 28, 2961–2968. [Google Scholar] [CrossRef] [PubMed]
- Uribarri, J. The Obsession with High Dietary Protein Intake in ESRD Patients on Dialysis: Is It Justified? Nephron 2000, 86, 105–108. [Google Scholar] [CrossRef]
- Raj, D.S.; Sun, Y.; Tzamaloukas, A.H. Hypercatabolism in dialysis patients. Curr. Opin. Nephrol. Hypertens. 2008, 17, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Musso, C.G. Potassium metabolism in patients with chronic kidney disease. Part II: Patients on dialysis (stage 5). Int. Urol. Nephrol. 2004, 36, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Cano, N.J.; Aparicio, M.; Brunori, G.; Carrero, J.J.; Cianciaruso, B.; Fiaccadori, E.; Lindholm, B.; Teplan, V.; Fouque, D.; Guarnieri, G. ESPEN Guidelines on Parenteral Nutrition: Adult renal failure. Clin. Nutr. 2009, 28, 401–414. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Kopple, J.D. Trace elements and vitamins in maintenance dialysis patients. Adv. Ren. Replace Ther. 2003, 10, 170–182. [Google Scholar] [CrossRef]
Figure 1.
Physiological impact of end-stage kidney disease on female fertility. Information sourced from references [1,2,3,6].

Figure 2.
Hypothalamic–pituitary–ovarian axis in end-stage kidney disease. Abbreviations: CKD, chronic kidney disease; GnRH, gonadotropin-releasing hormone; LH, luteinizing hormone; FSH, follicle-stimulating hormone. Adapted from reference [7].
Figure 2.
Hypothalamic–pituitary–ovarian axis in end-stage kidney disease. Abbreviations: CKD, chronic kidney disease; GnRH, gonadotropin-releasing hormone; LH, luteinizing hormone; FSH, follicle-stimulating hormone. Adapted from reference [7].


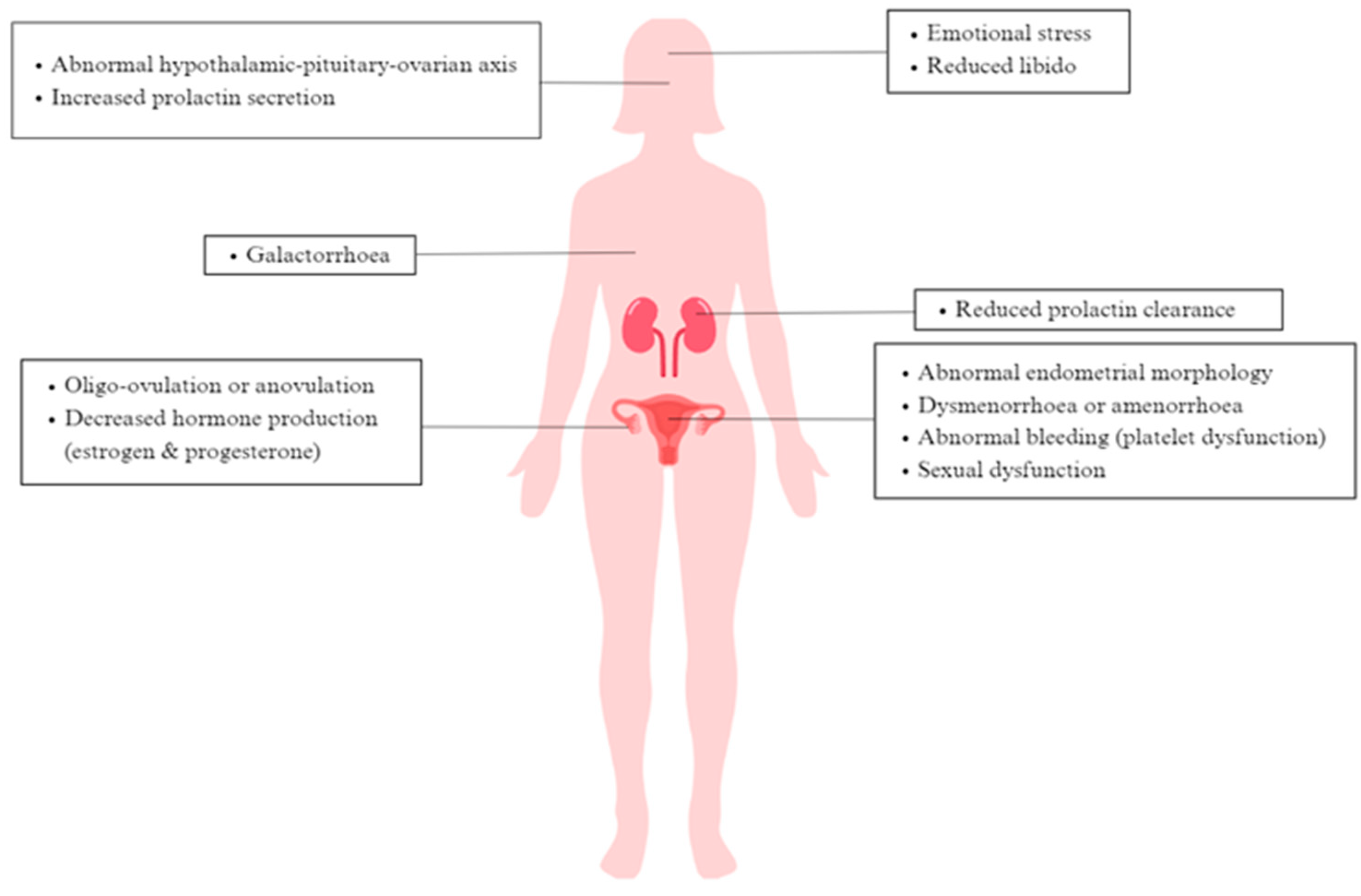{kind=link}
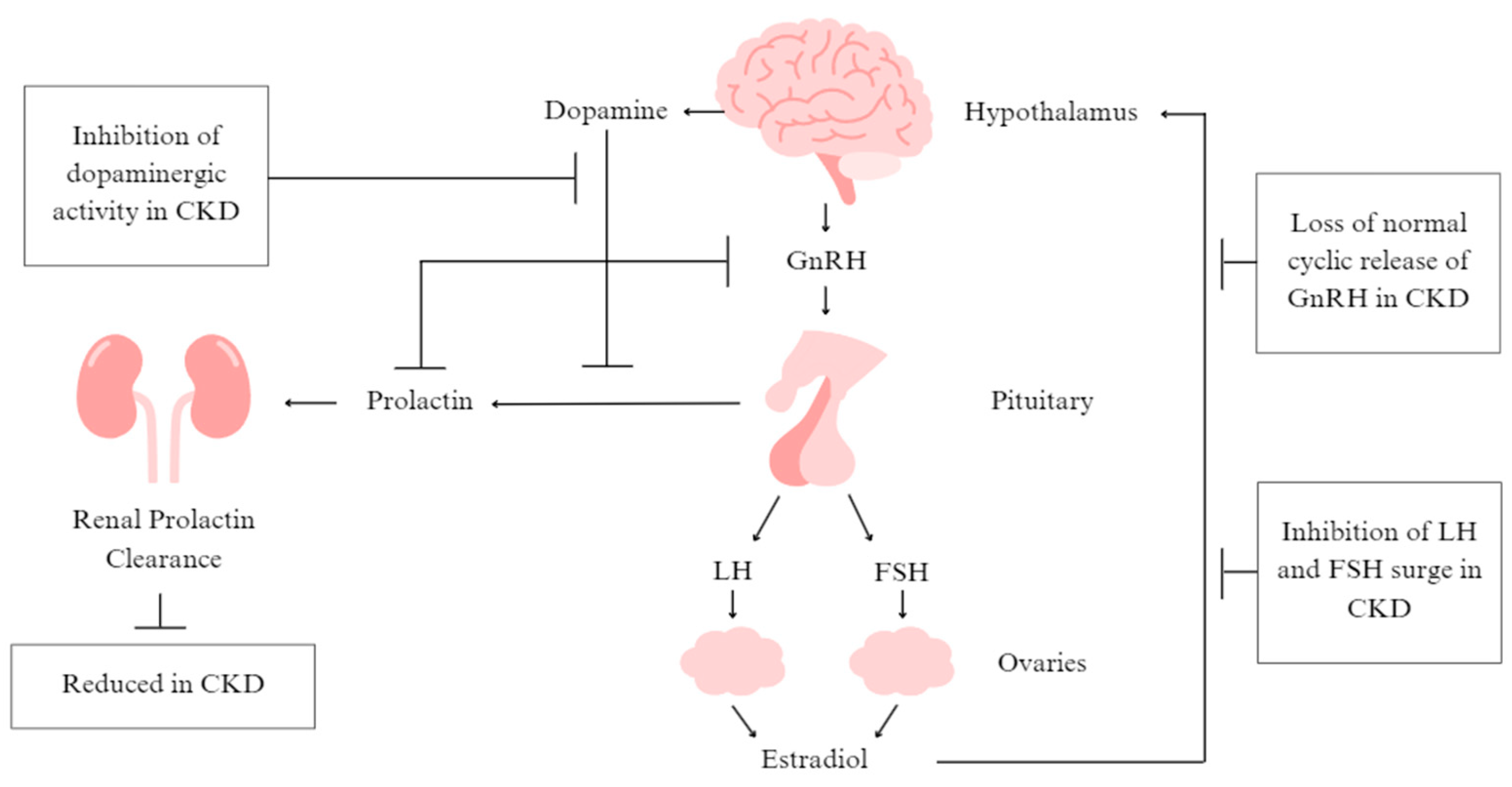{kind=link}
Table 1.
Summary and heat map of macronutrient recommendations for pregnant women receiving dialysis (data included from n = 106 papers with recommendations).
Table 1.
Summary and heat map of macronutrient recommendations for pregnant women receiving dialysis (data included from n = 106 papers with recommendations).
| Energy | Carbohydrate | Protein | Fat | Fibre | Fluid | |
|---|---|---|---|---|---|---|
| Nutrient Reference Value for female (Pregnancy, 14–50 years) [30] | 1st trimester: No additional requirement 2nd trimester: additional 1.4 MJ/day 3rd trimester: additional 1.9 MJ/day | No EAR, RDI or AI set | RDI: 58–60 g/day or 1.00–1.02 g/kg/day | AI: 10 g/day Linoleic acid: 1.0 g/day Alpha-Linoleic acid:110–115 mg/day | AI: 25–28 g/day | AI: 1.8–2.3 L/day |
| KDOQI Nutrition Guidelines [31] | 25–35 kcal/kg/day | Not reported | 1.0–1.2 g/kg/day (HD/PD) | Not reported | Not reported | Not reported |
| Consensus Guidelines/Position Papers | ||||||
| de Jong et al. (2022) [32] | 1.5–1.8 g/kg IBW (HD) | |||||
| Schmidt et al. (2022) [33] | 1st trimester: 30–35 kcal/kg/day 2nd/3rd trimesters: 30–35 kcal/kg/day + 300 kcal (HD) 1st trimester: 25–30 kcal/kg/day 2nd/3rd trimesters: 25–30 kcal/kg/day (+300 kcal) (CAPD) | 1.2 g/kg pre-pregnancy weight/day + 10 g/day (HD/CAPD) | ||||
| Wiles et al. (2019) [26] | 1.5–1.8 g/kg IBW/day (HD) | |||||
| Reviews | ||||||
| Esposito et al. (2020) [35] | 1st trimester: 30–35 kcal/kg/day (HD), 25–30 kcal/kg/day (PD) 2nd/3rd trimester: 30–35 kcal/kg/day (+300 kcal) (HD), 25–30 kcal/kg/day (+300 kcal) (PD) | 1.2 g/kg/day + 10 g/day (HD/PD) | ||||
| Jungers and Chauveau (1997) [39] | 1 g/kg/day + 20 g/day (HD/PD) | |||||
| Holley and Reddy (2003) [19] | 1.8 g/kg | |||||
| Díaz et al. (2016) [42] | 30–35 kcal/day (HD/PD) | 1.5–1.8 g/kg/day (HD/PD) | ||||
| Alkhunaizi et al. (2015) [43] | 1.5–1.8 g/kg (HD) | |||||
| Nadeau-Fredette et al. (2013) [1] | ≥1.1 g/kg/day | |||||
| Hladunewich and Schatell (2016) [34] | 1.5–1.8 g/kg/day | |||||
| Brookhyser and Wiggins (1998) [46] | 2nd/3rd trimesters: Basal energy expenditure × activity factor (1.2 to 1.4) +300 kcal (indivdualise) | 1.2 g/kg IBW + 10 g (HD) 1.4 g/kg IBW + 10 g (PD) | 1000–2000 mL | |||
| Reddy and Holley (2007) [4] | 30–35 kcal/kg/day | 1.5 g/kg (HD) 1.8 g/kg (PD) | 750–1500 mL/day | |||
| Oliverio and Hladunewich (2020) [47] | 1.5–1.8 g/kg/day | |||||
| Reyes-López et al. (2020) [48] | 1st trimester: 105–146 kJ/kg/day + 289 kJ 2nd trimester: 105–146 kJ/kg/day + 1100–1423 kJ 3rd trimester: 105–146 kJ/kg/day + 1891–2096 kJ | ≥175 g/day | 1st trimester: 1.1–1.5 g/kg/day + 0.7 g 2nd trimester: 1.1–1.5 g/kg/day + 9.6 g 3rd trimester: 1.1–1.5 g/kg/day + 31.2 g [50,51] | Saturated fatty acids 7% TEI Monounsaturated fatty acids 20% TEI | 3 L/day | |
| Tangren et al. (2018) [52] | 1.5–1.8 g/kg/day (HD) [53] | |||||
| Vecchio et al. (2021) [54] | 35 kcal/kg (HD) 25 kcal/kg (PD) | 1.2 g/kg pre-gestational weight/day (HD) 1.4 g/kg pre-gestational weight/day (PD) [266] | ||||
| Kapoor et al. (2009) [55] | 1.5 g/kg (HD) 1.8 g/kg (PD) | |||||
| Castellano et al. (2011) [56] | 1 g/kg + 20 g/day (HD) OR 1.8 g/kg (HD) | |||||
| Hladunewich et al. (2011) [2] | 1.5–1.8 g/kg (HD) | |||||
| Stover (2010) [58] | 1st trimester: 30–35 kcal/kg IBW/day 2nd/3rd trimesters: 30–35 kcal/kg IBW/day + 300 kcal/day | 1.2–1.8 g/kg IBW/day (HD) 1.2–1.3 g/kg IBW (PD) | ||||
| Hall and Brunskill (2010) [59] | ≥1.8 g/kg | |||||
| Kothari et al. (2019) [60] | 25–35 kcal/kg pregnant weight/day | 1.5–1.8 g/kg pre-pregnancy weight/day +20 g/day | ||||
| Lim and Wah (2018) [61] | 30–35 kcal/kg | 1.8 g/kg(HD) [63] 1.4–2.1 g/kg (PD) | ||||
| Vázquez-Rodríguez (2010) [65] | 35–40 kcal/kg (PD) | 1 g/kg + 20 g/day to 1.8 g/kg (PD) | ||||
| Onder et al. (2016) [67] | 30–35 kcal/kg | 1.5 g/kg (HD) 1.8 g/kg (PD) | 750–1500 mL/day | |||
| Furaz-Czerpak et al. (2012) [71] | 30–35 kcal/kg [4,19,68,69] | 1.5 g/kg (HD) 1.8 g/kg (PD) | ||||
| Singh and Pradeep (2012) [72] | 1 g/kg/day + 20 g/day | |||||
| Stover (2007) [73] | 1st trimester: 35 kcal/kg pre-pregnancy IBW/day 2nd/3rd trimesters: 35 kcal/kg pre-pregnancy IBW/day + 300 kcal/day | 1.2–1.3 g/kg IBW + ≥10 g/day | ||||
| Shehaj and Kazancıoglu (2023) [75] | 25–35 kcal/kg pregnant weight/day | 1.8 g/pre-pregnancy weight/day + 20 g/day | ||||
| Vázquez-Rodríguez (2010) [76] | 1 g/kg/day + 20 g/24 h OR 1.8 g/kg/day | |||||
| Porter (2009) [77] | 30–35 kcal/kg | 1.3–1.5 g/kg | ||||
| Nikolskaya and Prokopenko (2014) [79] | 30–35 kcal/kg + 300 kcal/day | 1.5–1.8 g/kg | ||||
| Hui and Hladunewich (2019) [81] | 1.5–1.8 g/kg | |||||
| Hou (1999) [37] | 35 kcal/kg + 300 kcal (HD) 25 kcal/kg + 300 kcal (PD) | 1.2 g/kg ideal pre-gravid weight + 10 g (HD) 1.4 g/kg ideal pre-gravid weight + 10 g + dialysate losses (PD) | ||||
| Davison (1991) [82] | 70 g/day | |||||
| Oliverio et al. (2021) [84] | 1.5–1.8 g/kg | |||||
| Ramin et al. (2006) [85] | 1.8 g/kg | |||||
| Chan et al. (1998) Canada [86] | >1.5 g/kg (HD) >1.8 g/kg (CAPD) | |||||
| Giannattasio et al. (2017) [87] | 1.5–1.8 g/kg | |||||
| Grossman et al. (1993) [89] | 25–45 kcal/kg + 250–300 kcal/day | 1.0–1.5 g/kg + 10–20 g/day | ||||
| Bili et al. (2013) [90] | 30–35 kcal/kg | 1.5 g/kg (HD) 1.8 g/kg (PD) | 0.75–1.5 L/day | |||
| Case Reports/Case Series | ||||||
| Cao et al. (2018) [94] | 35–40 kcal/kg | 1 g/kg + 20 g/day | ||||
| Manisco et al. (2015) [68] | 25–35 kcal/kg | 1.2–1.4 g/kg pre-pregnancy weight/day + 20 g/day | ||||
| Seker (2016) [99] | 2000 kcal/day | 1.5 g/kg | ||||
| Shanmugalingam et al. (2021) [100] | Not reported | 1.8–2 g/kg | ||||
| Haase et al. (2005) [101] | 3000 kcal/day | >100 g/day | ||||
| Yu et al. (2015) [102] | Not reported | 1 g/kg/day + 20 g/day | ||||
| Espinoza et al. (2013) [104] | 35 kcal/kg + 300 kcal | 1.8 g/kg | ||||
| Choi et al. (2018) [105] | 2000 kcal/day | 1.5 g/kg | ||||
| Tuot et al. (2009) [106] | 2100–2250 kcal/day (REE × 1.2–1.3 + 300 kcal) | 100 g dextrose (340 kcal) from IDPN | 75–85 g/day protein (metabolically active weight × 1.4–1.5) and 95 g protein (15% amino acids, 380 kcal) from IDPN | 40 g of lipid (400 kcal) from IDPN | ||
| Ribeiro and Silva (2020) [20] | 35 kcal/kg + 300 kcal/day | 1.8 g/kg of pre-pregnancy weight + 10–20 g/day [108,109] | ||||
| Giofre’ et al. (2007) [110] | 35 kcal/kg | 1.8–2 g/kg | ||||
| Campos-Collado et al. (2016) [112] | ~2000 kcal/day | 55% TEI, then 45% TEI | 1.4 g/kg pre-gestational IBW + 10 g/day | 26% TEI | 28 g/day | 1000–1100 mL/day (no fluid restriction) |
| Reister et al. (1999) [115] | 1.02 g/kg | |||||
| Swaroop et al. (2009) [116] | 1 g/kg + 20 g/day | |||||
| Yoo et al. (2004) [117] | 1.8 g/kg | |||||
| Giatras et al. (1998) [41] | 3000 kcal/day | >100 g/day | ||||
| Pepperell et al. (1970) [120] | 40 g/day protein diet | |||||
| Abu-Zaid et al. (2013) [121] | 3000 kcal/day | 100 g/day | ||||
| Al-Saran and Sabry (2008) [122] | 1 g/kg + 20 g/day | |||||
| Gómez Vázquez et al. (2007) [124] | 30–45 kcal/kg | 1.3–1.5 g/kg | <30% polyunsaturated | Variable 1.5 L to unlimited | ||
| Mohammed et al. (2021) [125] | 2500–3000 kcal/day | 1.5–1.8 g/kg | ||||
| Alhwiesh (2015) [126] | 45 kcal/kg | 1.5 g/kg | 1500 mL/day | |||
| Pipili et al. (2011) [127] | 1.8 g/kg | |||||
| Ramadani et al. (2018) [128] | 30–35 kcal/kg/day | 0.6–1.5 g/kg | 750–1500 mL/day | |||
| Hussain et al. (2005) [129] | 1.6–1.8 g/kg | |||||
| Bahadi et al. (2010) [80] | 1.8 g/kg/day | |||||
| López-Menchero et al. (2004) [132] | 35 kcal/kg gestational weight/day + 300 kcal/day | 1–1.2 g/kg pre-pregnancy weight/day + 10–20 g/day | ||||
| Coyle et al. (2008) [133] | IBW + 10 g | |||||
| Sheriff et al. (1978) [134] | 80 g/day | |||||
| Walsh (2002) [135] | 1.8 g/kg | |||||
| Cocîrţă et al. (2016) [137] | 1.8 g/kg (HD) | |||||
| Guida et al. (2003) [139] | 35 kcal/kg + 300–400 kcal/day | 1.2 g/kg + 6 g/day | ||||
| McPhatter and Drumheller (2008) [141] | 70 g/day | |||||
| Sandhu et al. (2014) [143] | 1 g/kg/day + 20 g/day | |||||
| Brookhyser (1989) [144] | 1900 kcal/day + 300 kcal/day | 1.5 g/kg/day (125 g high biological value protein) | ||||
| Park et al. (2006) [145] | 1.5–1.8 g/kg | |||||
| Yattara et al. (2019) [146] | 30–35 kcal/kg/day | 1.2 g/kg | 750–1500 mL/day [147] | |||
| Henderson (1996) [149] | 2000 kcals/day (30 kcals/kg pre-gravida weight + 250 kcals/day, then 2200 kcals/day at 28 weeks gestation | 70–80 g of protein/day (1.2 g/kg IBW + 10–20 g/day) [89] | ||||
| Melendez et al. (1988) [150] | 35–45 kcal/kg IBW + 300 kcal/day | 1.2–1.5 g/kg IBW + 30 g/day (CAPD) | ||||
| Vidal et al. (1998) [176] | 1st trimester: 35 kcal/kg IBW/day 2nd trimester: 35 kcal/kg dry weight/day + 300 kcal/day | 1st trimester: 1.1–1.2 g/kg IBW/day 2nd trimester: 1.5 g/kg dry weight/day | ||||
| Brookhyser et al. (1996) [153] | 1700–1900 kcal/day | >70 g/day | 40 oz/day (liberalised) | |||
| Cattran and Benzie (1983) [157] | 60 g/day | |||||
| Villa et al. (2007) [158] | 1.2–1.3 g/kg OR 1.8 g/kg | |||||
| Molaison et al. (2003) [107] | Increase daily intake by 300 calories [253] | Increase intake by 10 g/day [253] | ||||
| Stover (2004) [142] | 35 kcal/kg IBW or SBW/day + 300 kcal (2nd/3rd trimesters) | 1.2 g/kg IBW/day + 10 g/day (2nd/3rd trimesters) | ||||
| Unzelman et al. (1973) [161] | 2200 kcal/day | 80 g/day | Unrestricted | |||
| Perry (1994) [162] | 2000 kcal/day | 60 g/day | 800 mL/day, then 500 mL/day above urine output | |||
| Editorials | ||||||
| Levy et al. (1998) [136] | 1 g/kg + 20 g/day | |||||
| Mercadal and Nizard (2019) [164] | 1.5–2 g/kg | |||||
| Ellis (2012) [166] | 1.8 g/kg (HD) | |||||
| Jagielski (2015) [167] | 30–35 kcal/kg/day + 300 kcal/day (2nd/3rd trimesters) (HD) | 1.2 g/kg + 10 g/day (HD) | ||||
| Book Chapters | ||||||
| Lawrence (2012) [169] | 1st trimester: BEE × activity factor (1.2–1.4) or 35 kcal/kg of pre- pregnancy IBW 2nd/3rd trimesters: Add 300 kcal/dL (HD/PD) [37,73,170] | Remaining calories to be met with CHO sources (after protein and fat requirements have been met) | 1.1–1.4 g/kg of pre-pregnancy IBW + 10 g/day (HD) 1.2–1.5 g/kg of pre-pregnancy IBW + 10 g/day (PD) [37,73,170] | Saturated fat < 7% TEI, trans-fat < 1% TEI, cholesterol < 300 mg/day Hyperlipidemia: Total fat intake 25–35% TEI, saturated fat < 7% TEI, remaining fat calories (up to 20%) distributed toward monounsaturated fats and polyunsaturated fats, cholesterol < 200 mg/day | 1000–2000 mL/IDWG ≤ 2 kg (HD) No recommendation (PD) | |
| Flecha (2020) [172] | 1 g/kg/day + 20 g/day | |||||
| Pahl (2019) [173] | 3000 kcal/day | 1.8 g/kg/day [41] | ||||
| Sandhu (2016) [174] | 1 g/kg/day + 20 g/day | |||||
| Hou (1994) [40] | 1 g/kg/day + 20 g (HD) 1.5 g/kg/day + 20 g (CAPD) | |||||
| Fisher et al. (2018) [5] | 30–35 kcal/kg/day | 1.5 g/kg (HD) 1.8 g/kg/(PD) | ||||
| Stover (2008) [175] | 35 kcal per kg/day of pre-gravida IBW + 300 kcal/day (2nd/3rd trimesters) | 1.2 g/kg pre-gravida IBW + 10 g/day (HD) 1.2–1.3 g/kg pre-gravida IBW + 10 g/day (PD) | ||||
| Stover (2014) [177] | 35 kcal/kg pre-gravida SBW + 300/day (in 2nd/3rd trimesters) | 1.2 g/kg pre-gravida SBW + 10–25 g/day (HD) 1.2–1.3 g/kg pre-gravida SBW + 10–25 g/day (PD) | ||||
| Stover and Trolinger (2020) [179] | 1st trimester: 35 kcal/kg/day of pre-gravida SBW 2nd/3rd trimesters: 35 kcal/kg/day + 350–450 kcal/day | 1.2 g/kg SBW + 10–25 g/day (HD) 1.2–1.3 g/kg SBW + 10–25 g/day (PD) | ||||
| Plant (2008) [181] | Up to 3000 kcal/day | Up to 1.8 g/kg | ||||
| Stover (2022) [182] | 25–35 kcal/kg pre-pregnancy weight/day + 300 kcal/day (2nd/3rd trimesters) | 1.0–1.2 g/kg pre-pregnancy weight/day + 10–25 g/day | ||||
| Goody and Umans (2004) [183] | >35 kcal/kg/day + 300 kcal/day | 1.2 g/kg ideal pre-gravid weight + 10 g (HD) | ||||
| Vellanki and Hou (2019) [184] | 1.0–1.1 g/kg | |||||
| Shahid et al. (2018) [185] | 1.5–1.8 g/kg (HD) | |||||
| Piccoli et al. (2023) [186] | 1.2–1.5 g/kg | |||||
Legend: Red, inconsistent with NRV for pregnancy (women aged 14–50 years) and/or KDOQI guidelines for dialysis; blue, consistent with NRV for pregnancy (women aged 14–50 years) and/or KDOQI guidelines for dialysis; yellow, no relevant NRV for pregnancy (women aged 14–50 years) or KDOQI guidelines for dialysis; grey, no data. Abbreviations: NRV, nutrient reference value; KDOQI, Kidney Disease Outcomes Quality Initiative; EAR, estimated average requirement; RDI, recommended daily intake; AI, adequate intake; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; DPA, docosapentaenoic acid; HD, haemodialysis; PD, peritoneal dialysis; CAPD, continuous ambulatory peritoneal dialysis; IBW, ideal body weight; REE, resting energy expenditure; IDPN, intradialytic parenteral nutrition; TEI, total energy intake; BEE, basal energy expenditure; CHO, carbohydrate(s); SBW, standard body weight.
Table 2.
Summary and heat map of vitamin recommendations for pregnant women receiving dialysis (data included from n= 17 papers with recommendations).
Table 2.
Summary and heat map of vitamin recommendations for pregnant women receiving dialysis (data included from n= 17 papers with recommendations).
| Daily Amounts | Vitamin A (RE) | Vitamin C | Vitamin D | Vitamin E | Vitamin K | Vitamin B1 | Vitamin B2 | Vitamin B3 | Vitamin B5 | Vitamin B6 | Vitamin B12 | Folate | Biotin |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NRV Female (Pregnancy, 14–50 years) [30] | RDI: 700–800 µg/day | RDI: 55–60 mg/day | AI: 5 µg/day | AI: 7–8 mg/day | AI: 60 µg/day | RDI: 1.4 mg/day | RDI: 1.4 mg/day | RDI: 18 mg/day | AI: 5 mg/day | RDI: 1.9 mg/day | RDI: 2.6 µg/day | RDI: 600 µg/day | AI: 30 µg/day |
| KDOQI Dialysis Guidelines [31] | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported |
| Consensus Guidelines/Position Papers | |||||||||||||
| Schmidt et al. (2022) [33] | 25–50 μg | 2–5 mg | |||||||||||
| Reviews | |||||||||||||
| Esposito et al. (2020) [35] | 25–50 μg | 2–5 mg | |||||||||||
| Brookhyser and Wiggins (1998) [46] | ≥170 mg | 3 mg (HD) | 3.4 mg (HD) | ≥20 mg (HD) | ≥5 mg (HD) | 1.8 mg (HD) | 600 µg (HD) | ||||||
| Reddy and Holley (2007) [4] | 1 mg | ||||||||||||
| Hou (1999) [37] | ≥170 mg | 3 mg | 3.4 mg | ≥20 mg | >5 mg | 1.8 mg | |||||||
| Grossman et al. (1993) [89] | ≥170 mg | 3 mg | 3.4 mg | ≥20 mg | ≥5 mg | 1.8 mg | |||||||
| Case Reports/Case Studies | |||||||||||||
| Campos-Collado et al. (2016) [112] | 800 μg | ≥170 mg | 1.8 mg | ||||||||||
| Yoo et al. (2004) [117] | 800 μg | ||||||||||||
| Yattara et al. (2019) [146] | 1.8 mg | ||||||||||||
| Henderson (1996) [149] | ≥170 mg | 3 mg | 3.4 mg | ≥20 mg | ≥5 mg | 1.8 mg | |||||||
| Shah et al. (2007) [155] | 800 μg | ||||||||||||
| Racette (1997) [159] | 1.8 mg | ||||||||||||
| Book Chapters | |||||||||||||
| Lawrence (2012) [169] | ≥1.8 mg | ||||||||||||
| Stover (2008) [175] | ≥2 mg | ||||||||||||
| Stover (2014) [177] | 2–4 mg | ||||||||||||
| Stover and Trolinger (2020) [179] | 2–4 mg | ||||||||||||
| Stover (2022) [182] | 2–4 mg | ||||||||||||
Legend: Red, inconsistent with NRV for pregnancy (women aged 14–50 years) and/or KDOQI guidelines for dialysis; blue, consistent with NRV for pregnancy (women aged 14–50 years) and/or KDOQI guidelines for dialysis; grey, no data. Abbreviations: NRV, nutrient reference value; KDOQI, Kidney Disease Outcomes Quality Initiative; RDI, recommended daily intake; AI, adequate intake.
Table 3.
Summary and heat map of mineral recommendations for pregnant women receiving dialysis (data included from n = 38 papers with recommendations).
Table 3.
Summary and heat map of mineral recommendations for pregnant women receiving dialysis (data included from n = 38 papers with recommendations).
| Daily Amount | Na | K | Ca | Mg | Fe | Zn | P | I | Cu | Se | Mn | Mo |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NRV Female (Pregnancy, 14–50 years) [30] | AI: 460–920 mg/day (20–40 mmol/day) | AI: 2800 mg/day (72 mmol/day) | RDI: 1000–1300 mg/day | RDI: 350–400 mg/day | RDI: 27 mg/day | RDI: 10–11 mg/day | RDI: 1000–1250 mg/day | RDI: 220 µg/day | AI: 1.2–1.3 mg/day | RDI: 65 µg/day | AI: 5 mg/day | RDI: 50 µg/day |
| KDOQI Nutrition Guidelines [31] | <100 mmol/day (<2.3 g/day salt) | Adjust intake to maintain serum potassium within normal range. | Adjust intake considering use of vitamin D analogs and calcimimetics to avoid hypercalcemia or calcium overload. | Not reported | Not reported | Not reported | Adjust intake to maintain normal serum phosphate levels. Consider the bio- availability of phosphorus sources. | Not reported | Not reported | Not reported | Not reported | Not reported |
| Consensus Guidelines/Position Papers | ||||||||||||
| de Jong et al. (2022) [32] | ≥1000 mg/day | |||||||||||
| Schmidt et al. (2022) [33] | 3 g/day (<75 mmol/day) (HD) | 1500–2000 mg (HD) | 20–30 mg (HD) | 15 mg (HD) | ||||||||
| Reviews | ||||||||||||
| Esposito et al. (2020) [35] | 80 mmol or 4 g/day (salt) | 3 g/day (<75 mmol/day) or 50 mmol (HD) | 1500–2000 mg (HD) | 20–30 mg (HD) | 15 mg (HD) | 1000–1250 mg | ||||||
| Brookhyser and Wiggins (1998) [46] | ~2–3 g(salt) | ~2–3 g | ~1200 mg | 200–300 mg (HD) | 15 mg (HD) | 1200 mg (HD) | ||||||
| Reddy and Holley (2007) [4] | 80 mmol | 50 mmol | 1500–2000 mg | |||||||||
| Reyes-López et al. (2020) [48] | 3–4 g (salt) (HD) | 3 g (HD) | ||||||||||
| Kapoor et al. (2009) [55] | 1500 mg | |||||||||||
| Hladunewich et al. (2011) [2] | >30 mg | |||||||||||
| Hou (2004) [66] | >1 g over usual requirement | |||||||||||
| Onder et al. (2016) [67] | 1500–2000 mg | |||||||||||
| Furaz-Czerpak et al. (2012) [71] | 1500 mg | |||||||||||
| Singh and Pradeep (2012) [72] | 1500 mg | |||||||||||
| Stover (2007) [73] | 2–4 g | ≥1000 mg | 15 mg | |||||||||
| Nikolskaya and Prokopenko (2014) [79] | 1500 mg | 800 mg for high serum phosphate | ||||||||||
| Hou (1999) [37] | 2000 mg/day | 200–300 mg | 15 mg | 1200 mg | ||||||||
| Davison (1991) [82] | 80 mmol | 50 mmol | 1500 mg | |||||||||
| Giannattasio et al. (2017) [87] | 100 mmol | |||||||||||
| Grossman et al. (1993) [89] | 200–300 mg | 15 mg | 1200 mg | |||||||||
| Bili et al. (2013) [90] | 1500 mg | |||||||||||
| Case Reports/Case Series | ||||||||||||
| Manisco et al. (2015) [68] | 800 mg | |||||||||||
| Campos- Collado et al. (2016) [112] | 2–3 g salt | 2512 mg/day (40 mg/kg IBW/day, restriction of foods > 250 mg/serve) | 1000–1200 mg | 200–300 mg | 200 mg | 1200 mg | ||||||
| Abu-Zaid et al. (2013) [121] | 1500 mg | |||||||||||
| Gómez Vázquez et al. (2007) [124] | 3 g (salt) | 2 g | 800 mg | |||||||||
| Alhwiesh (2015) [126] | 800 mg | |||||||||||
| Ramadani et al. (2018) [128] | 1500 mg | |||||||||||
| Hussain et al. (2005) [129] | 1500 mg | 800–1600 mg | ||||||||||
| Sandhu et al. (2014) [143] | 30 mg | |||||||||||
| Henderson (1996) [149] | 4 g (salt) | 3 g | 200–300 mg | 200 mg | 15 mg | 1200 mg | ||||||
| Melendez et al. (1988) [150] | 2 g salt | |||||||||||
| Vidal et al. (1998)[176] | 1st trimester: 3–4 g/day (salt) 2nd/3rd trimesters: flexible | 1st trimester: 3 g/day 2nd/3rd trimesters: flexible | ||||||||||
| Perry (1994) [162] | 60 mmol | 1200 mg | ||||||||||
| Editorials | ||||||||||||
| Hou (2002) [165] | >1 g above usual requirement | |||||||||||
| Book Chapters | ||||||||||||
| Lawrence (2012) [169] | ~2–3 g/day (salt) (HD) ~2–4 g/day (salt) (PD) [37,73,170] | HD: ~40 mg/kg pre-pregnancy IBW (individualise per serum values) | ~1000–1200 mg | ~1200 mg | ||||||||
| Sandhu (2016) [174] | 30 mg | |||||||||||
| Stover (2008) [175] | ≥15 mg | |||||||||||
| Stover (2014) [177] | ≥15 mg | |||||||||||
| Stover and Trolinger (2020) [179] | 1500 mg | ≥15 mg | ||||||||||
| Stover (2022) [182] | 5 mg | |||||||||||
Legend: Red, inconsistent with NRV for pregnancy (women aged 14–50 years) and/or KDOQI guidelines for dialysis; blue, consistent with NRV for pregnancy (women aged 14–50 years) and/or KDOQI guidelines for dialysis; grey, no data. Abbreviations: NRV, nutrient reference value; KDOQI, Kidney Disease Outcomes Quality Initiative; Na, sodium; K, potassium; Ca, calcium; Mg, magnesium; Fe, iron; Zn, zinc; P, phosphorous; I, iodine; Cu, copper; Se, selenium; Mn, manganese; Mb, molybdenum; AI, adequate intake; RDI, recommended daily intake; HD, haemodialysis; IBW, ideal body weight; NaCl, sodium chloride; PD, peritoneal dialysis.
Table 4.
Synthesis of nutrition recommendations for pregnant women undertaking dialysis from scoping review findings.
Table 4.
Synthesis of nutrition recommendations for pregnant women undertaking dialysis from scoping review findings.
| Macronutrients | |
| Energy # † | 1st trimester: 25–35 kcal/kg/day 2nd/3rd trimesters: 25–35 kcal/kg/day + 300 kcal/day |
| Carbohydrate | After protein and fat requirements have been satisfied, meet remaining calorie requirements with carbohydrate sources Factor in calories received from glucose in PD dialysate |
| Protein | 1.5–1.8 g/kg/day (HD/PD) |
| Fat * | Linoleic acid: 10 g/day (AI) a-Linoleic acid: 1.0 g/day (AI) Total LC n-3, DHA+EPA+DPA: 110–115 mg/day (AI) Absence of hyperlipidemia: Hyperlipidemia: Saturated fat <7% TEI Saturated fat <7% TEI Trans fat <1% TEI Total fat 25–35% TEI Cholesterol <300 mg/day Cholesterol of <200 mg/day Remaining fat calories (up to 20%) distributed primarily toward monounsaturated fats and secondarily toward polyunsaturated fats |
| Fibre * | 25–28 g/day (AI) |
| Fluid † | Liberalise if undertaking daily or longer hours dialysis |
| Vitamins ╪ | |
| Vitamin A | 800 µg/day; do not supplement |
| Vitamin C | Minimum 170 mg/day |
| Vitamin D | 1000–2000 IU/day (25 OH vitamin D/D3) (HD) |
| Vitamin E * | 7–8 mg/day (AI); do not supplement |
| Vitamin K * | 60 µg/day (AI); supplementation usually not necessary |
| Vitamin B1 | 3 mg/day |
| Vitamin B2 | 3.4 mg/day |
| Vitamin B3 | Minimum 20 mg/day |
| Vitamin B5 * | 5 mg/day (AI) |
| Vitamin B6 | Minimum 5 mg/day |
| Vitamin B12 * | 2.4 µg/day |
| Folate | Minimum 1.8 mg/day |
| Biotin | 600 µg/day (HD) |
| Minerals ╪ | |
| Sodium | Individualise but maintain reduced salt diet |
| Potassium | Individualise and liberalise if undertaking daily or longer hours dialysis |
| Calcium | 1500–2000 mg/day |
| Magnesium | 200–300 mg/day |
| Iron | Minimum 30 mg/day |
| Zinc | Minimum 15 mg/day |
| Phosphorous | Approximately 1200 mg/day (RDI) |
| Iodine * | 220 µg/day (RDI) |
| Copper * | 1.2–1.3 mg/day (AI) |
| Selenium * | 65 µg/day (RDI) |
| Manganese * | 5 mg/day (AI) |
| Molybdenum * | 50 µg/day (RDI) |
| Nutrient Supplementation ╪ | |
Vitamins
Minerals
| |
| Dietary Patterns | |
| |
| Weight | |
| |
| Breastfeeding ‡ | |
| |
# Take into account energy expenditure, body mass index, pregnancy weight gain, and mode of renal replacement therapy (with the higher end of these ranges generally for HD). * Evidence unclear, recommendations developed with clinical judgement and adapted from references [30]. † Take into account urine output and mode of renal replacement therapy. ╪ Individualise according to serum concentrations, blood pressure, medications, hydration status, and mode of renal replacement therapy (with the higher end of these ranges generally for HD). ‡ Assess on an individual basis. Legend: PD, peritoneal dialysis; HD, haemodialysis; AI, adequate intake; TEI, total energy intake; RDI, recommended daily intake; PTH, parathyroid hormone; BMI, body mass index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Cutajar, E.; Lambert, K. Nutritional Recommendations for Pregnant Women Receiving Dialysis: A Scoping Review. Kidney Dial. 2024, 4, 46-77. https://doi.org/10.3390/kidneydial4010005
AMA Style
Cutajar E, Lambert K. Nutritional Recommendations for Pregnant Women Receiving Dialysis: A Scoping Review. Kidney and Dialysis. 2024; 4(1):46-77. https://doi.org/10.3390/kidneydial4010005
Chicago/Turabian StyleCutajar, Elyce, and Kelly Lambert. 2024. "Nutritional Recommendations for Pregnant Women Receiving Dialysis: A Scoping Review" Kidney and Dialysis 4, no. 1: 46-77. https://doi.org/10.3390/kidneydial4010005