
Diagnostic Accuracy of a Portable Electromyography and Electrocardiography Device to Measure Sleep Bruxism in a Sleep Apnea Population: A Comparative Study
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
Limitations
4. Materials and Methods
4.1. Sample Selection
4.2. PSG Recordings
PSG Sleep Bruxism Analysis
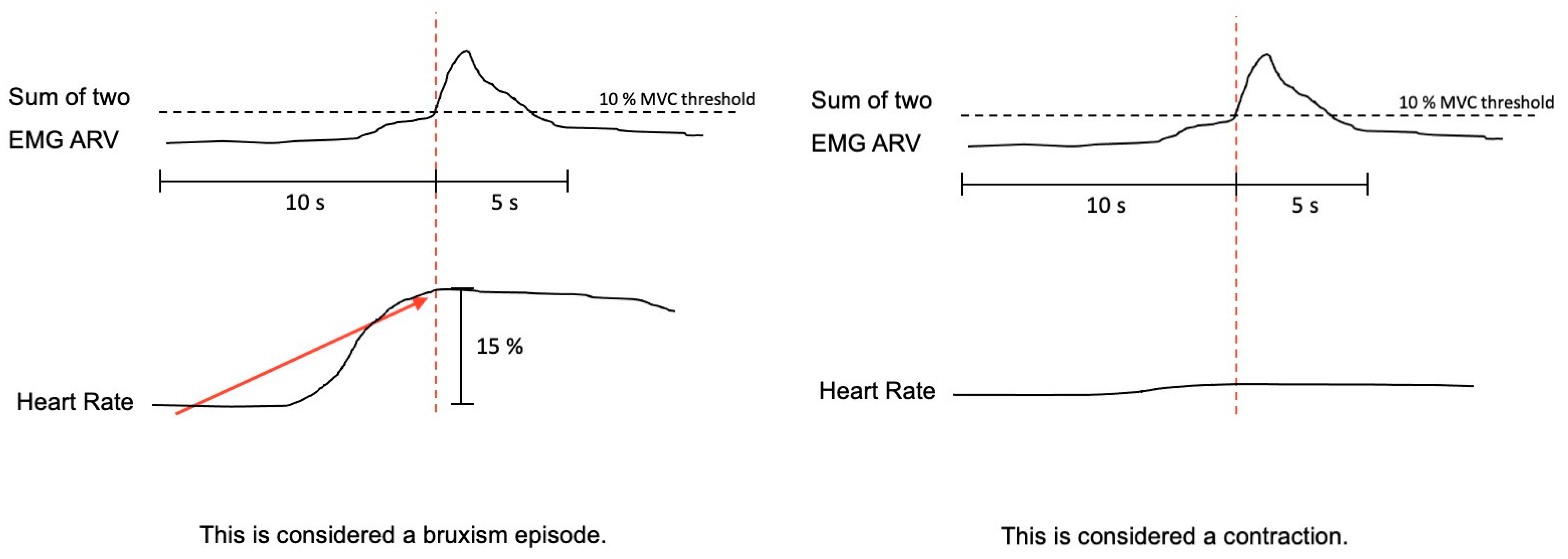
4.3. Bruxoff Sleep Bruxism Analysis
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AASM: | American Academy of Sleep Medicine |
| AH: | Apnea-Hypopnea episode |
| AHI: | Apnea-Hypopnea Index |
| BMI: | Body Mass Index |
| CT90: | total time lower 90% O2Sat. |
| DC/TMD: | Diagnostic criteria for the Temporomandibular Disorders |
| EEG: | Electroencephalogram |
| EKG: | Electrocardiogram |
| EMG: | Electromyography |
| EOG: | Electrooculogram |
| HR: | Heart Rate |
| ICC: | Intraclass Correlation Coefficient |
| MMA: | Masticatory Muscle Activity |
| MVC: | Maximum Voluntary Contraction |
| OMA: | Sleep-related Oromotor Activity |
| OSA: | Obstructive Sleep Apnea |
| PSG: | Polysomnography |
| RMMA: | Rhythmic Masticatory Muscle Activity |
| SB: | Sleep Bruxism |
| SD: | Standar Desviation |
| SEMG: | Surface electromyography |
| SLT: | Sleep Time Latency |
| SPT: | Sleep Period Time |
| TST: | Total Sleep Time |
| WASO: | Wake time After Sleep Onset |
References
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International consensus on the assessment of bruxism: Report of a work in progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, G.J.; Khoury, S.; Abe, S.; Yamaguchi, T.; Raphael, K. Bruxism physiology and pathology: An overview for clinicians. J. Oral Rehabil. 2008, 35, 476–494. [Google Scholar] [CrossRef] [PubMed]
- Castroflorio, T.; Deregibus, A.; Bargellini, A.; Debernardi, C.; Manfredini, D. Detection of sleep bruxism: Comparison between an electromyographic and electrocardiographic portable holter and polysomnography. J. Oral Rehabil. 2014, 41, 163–169. [Google Scholar] [CrossRef]
- Osses-Anguita, Á.E.; Sánchez-Sánchez, T.; Soto-Goñi, X.A.; García-González, M.; Fariñas, F.A.; Cid-Verdejo, R.; Romero, E.A.S.; Jiménez-Ortega, L. Awake and Sleep Bruxism Prevalence and Their Associated Psychological Factors in First-Year University Students: A Pre-Mid-Post COVID-19 Pandemic Comparison. Int. J. Environ. Res. Public Health 2023, 20, 2452. [Google Scholar] [CrossRef] [PubMed]
- Serra-Negra, J.M.; Lobbezoo, F.; Martins, C.C.; Stellini, E.; Manfredini, D. Prevalence of sleep bruxism and awake bruxism in different chronotype profiles: Hypothesis of an association. Med. Hypotheses 2017, 101, 55–58. [Google Scholar] [CrossRef]
- Alona, E.P.; Ilana, E. One year into the COVID-19 pandemic—Temporomandibular disorders and bruxism: What we have learned and what we can do to improve our manner of treatment. Dent. Med. Probl. 2021, 58, 215–218. [Google Scholar] [CrossRef]
- Cruz-Fierro, N.; Martínez-Fierro, M.; Cerda-Flores, R.; Gómez-Govea, M.; Delgado-Enciso, I.; Martínez-De-Villarreal, L.; González-Ramírez, M.; Rodríguez-Sánchez, I. The phenotype, psychotype and genotype of bruxism. Biomed. Rep. 2018, 8, 264–268. [Google Scholar] [CrossRef]
- Melo, G.; Dutra, K.L.; Filho, R.R.; Ortega, A.d.O.L.; Porporatti, A.L.; Dick, B.; Flores-Mir, C.; Canto, G.D.L. Association between psychotropic medications and presence of sleep bruxism: A systematic review. J. Oral Rehabil. 2018, 45, 545–554. [Google Scholar] [CrossRef]
- Rintakoski, K.; Ahlberg, J.; Hublin, C.; Broms, U.; Madden, P.A.F.; Kononen, M.; Koskenvuo, M.; Lobbezoo, F.; Kaprio, J. Bruxism Is Associated with Nicotine Dependence: A Nationwide Finnish Twin Cohort Study. Nicotine Tob. Res. 2010, 12, 1254–1260. [Google Scholar] [CrossRef]
- Lavigne, G.; Kato, T.; Babiloni, A.H.; Huynh, N.; Fabbro, C.D.; Svensson, P.; Aarab, G.; Ahlberg, J.; Baba, K.; Carra, M.C.; et al. Research routes on improved sleep bruxism metrics: Toward a standardised approach. J. Sleep Res. 2021, 30, e13320. [Google Scholar] [CrossRef]
- Carra, M.C.; Bruni, O.; Huynh, N. Topical review: Sleep bruxism, headaches, and sleep-disordered breathing in children and adolescents. J. Orofac. Pain 2021, 26, 267–276. [Google Scholar]
- Lavigne, G.; Manzini, C.; Huynh, N. Sleep bruxism. In Principles and Practice of Sleep Medicine, 5th ed.; Elsevier Saunders: St. Louis, MI, USA, 2011; pp. 1129–1139. [Google Scholar]
- Glaros, A.G. Incidence of diurnal and nocturnal bruxism. J. Prosthet. Dent. 1981, 45, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Reding, G.R.; Rubright, W.C.; Zimmerman, S.O. Incidence of bruxism. J. Dent. Rest. 1966, 45, 1198–1204. [Google Scholar] [CrossRef]
- Laberge, L.; Tremblay, R.E.; Vitaro, F.; Montplaisir, J. Development of Parasomnias from Childhood to Early Adolescence. Pediatrics 2000, 106, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Winocur, E.; Guarda-Nardini, L.; Paesani, D.; Lobbezoo, F. Epidemiology of Bruxism in Adults: A Systematic Review of the Literature. J. Orofac. Pain 2013, 27, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Mikami, A.; Sugita, H.; Muraki, H.; Okura, M.; Ohi, M.; Taniguchi, M. Negative association between self-reported jaw symptoms and apnea–hypopnea index in patients with symptoms of obstructive sleep apnea syndrome: A pilot study. Sleep Breath. 2013, 17, 373–379. [Google Scholar] [CrossRef]
- Roehrs, T.; Carskadon, M.A.; Dement, W.C.; Roth, T. Day- time sleepiness and alertness. In Principles and Practice of Sleep Medicine; Saunders: Philadelphia, PA, USA, 2000; pp. 43–52. [Google Scholar]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Bassiri, A.G.; Guilleminault, C. Clinical features and evaluation of obstructive sleep apnea–hypopnea syndrome. In Principles and Practices of Sleep Medicine; Saunders WB: Philadelphia, PA, USA, 2000; pp. 869–878. [Google Scholar]
- Young, T.; Peppard, P.E.; Gottlieb, D.J. Epidemiology of Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2002, 165, 1217–1239. [Google Scholar] [CrossRef]
- Inoko, Y.; Shimizu, K.; Morita, O.; Kohno, M. Relationship between masseter muscle activity and sleep-disordered breathing. Sleep Biol. Rhythm. 2004, 2, 67–68. [Google Scholar] [CrossRef]
- Saito, M.; Yamaguchi, T.; Mikami, S.; Watanabe, K.; Gotouda, A.; Okada, K.; Hishikawa, R.; Shibuya, E.; Lavigne, G. Temporal association between sleep apnea-hypopnea and sleep bruxism events. J. Sleep Res. 2014, 23, 196–203. [Google Scholar] [CrossRef]
- Saito, M.; Yamaguchi, T.; Mikami, S.; Watanabe, K.; Gotouda, A.; Okada, K.; Hishikawa, R.; Shibuya, E.; Shibuya, Y.; Lavigne, G. Weak association between sleep bruxism and obstructive sleep apnea. A sleep laboratory study. Sleep Breath. 2016, 20, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Hosoya, H.; Kitaura, H.; Hashimoto, T.; Ito, M.; Kinbara, M.; Deguchi, T.; Irokawa, T.; Ohisa, N.; Ogawa, H.; Takano-Yamamoto, T. Relationship between sleep bruxism and sleep respiratory events in patients with obstructive sleep apnea syndrome. Sleep Breath. 2014, 18, 837–844. [Google Scholar] [CrossRef] [PubMed]
- da Costa Lopes, A.J.; Cunha, T.C.A.; Monteiro, M.C.M.; Serra-Negra, J.M.; Cabral, L.C.; Júnior, P.C.S. Is there an association between sleep bruxism and obstructive sleep apnea syndrome? A systematic review. Sleep Breath. 2020, 24, 913–921. [Google Scholar] [CrossRef]
- Manfredini, D.; Guarda-Nardini, L.; Marchese-Ragona, R.; Lobbezoo, F. Theories on possible temporal relationships between sleep bruxism and obstructive sleep apnea events. An expert opinion. Sleep Breath. 2015, 19, 1459–1465. [Google Scholar] [CrossRef]
- Tan, M.; Yap, A.; Chua, A.; Wong, J.; Parot, M.; Tan, K. Prevalence of Sleep Bruxism and Its Association with Obstructive Sleep Apnea in Adult Patients: A Retrospective Polysomnographic Investigation. J. Oral Facial Pain Headache 2019, 33, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Phillips, B.A.; Okeson, J.; Paesani, D.; Gilmore, R. Effect of Sleep Position on Sleep Apnea and Parafunctional Activity. Chest 1986, 90, 424–429. [Google Scholar] [CrossRef]
- Okeson, J.P.; Phillips, B.A.; Berry, D.T.; Cook, Y.R.; Cabelka, J.F. Nocturnal bruxing events in subjects with sleep-disordered breathing and control subjects. J. Craniomandib. Disord. 1991, 5, 258–264. [Google Scholar]
- Sjöholm, T.T.; Lowe, A.A.; Miyamoto, K.; Fleetham, J.A.; Ryan, C.F. Sleep bruxism in patients with sleep-disordered breathing. Arch. Oral Biol. 2000, 45, 889–896. [Google Scholar] [CrossRef]
- Manfredini, D.; Ahlberg, J.; Castroflorio, T.; Poggio, C.E.; Guarda-Nardini, L.; Lobbezoo, F. Diagnostic accuracy of portable instrumental devices to measure sleep bruxism: A systematic literature review of polysomnographic studies. J. Oral Rehabil. 2014, 41, 836–842. [Google Scholar] [CrossRef]
- Winck, M.; Drummond, M.; Viana, P.; Pinho, J.C.; Winck, J.C. Sleep bruxism associated with obstructive sleep apnoea síndrome—A pilot study using a new portable device. Rev. Port. Pneumol. 2017, 23, 22–26. [Google Scholar]
- The AASM Manual for the Scoring of Sleep and Associated Events; American Academy of Sleep Medicine: Darien, IL, USA, 2020; Volume 2.6.
- Kato, T.; Blanchet, P.J.; Montplaisir, J.Y.; Lavigne, G.J. Sleep bruxism and other disorders with orofacial activity during sleep. In Sleep and Movement Disorders; Butter-Worth Heinemann: Philadelphia, PA, USA, 2003; pp. 273–285. [Google Scholar]
- Lavigne, G.J.; Manzini, C.; Kato, T. Sleep bruxism. In Principles and Practice of Sleep Medicine, 4th ed.; Elsevier Saunder: Philadelphia, PA, USA, 2005; pp. 946–959. [Google Scholar]
- Miyawaki, S.; Lavigne, G.J.; Pierre, M.; Guitard, F.; Montplaisir, J.Y.; Kato, T. Association between sleep bruxism, swallowing-related laryngeal movement, and sleep positions. Sleep 2003, 26, 461–465. [Google Scholar] [PubMed]
- Macaluso, G.M.; Guerra, P.; Di Giovanni, G.; Boselli, M.; Parrino, L.; Terzano, M.G. Sleep Bruxism is a Disorder Related to Periodic Arousals during Sleep. J. Dent. Res. 1998, 77, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Rundo, J.V.; Downey, R. Polysomnography. Handb. Clin. Neurol. 2019, 160, 381–392. [Google Scholar] [PubMed]
- Lavigne, G.J.; Rompre, P.H.; Montplaisir, J.Y. Sleep Bruxism: Validity of Clinical Research Diagnostic Criteria in a Controlled Polysomnographic Study. J. Dent. Res. 1996, 75, 546–552. [Google Scholar] [CrossRef]
- Gamaldo, C.; Buenaver, L.; Chernyshev, O.; Derose, S.; Mehra, R.; Vana, K.; Walia, H.K.; Gonzalez, V.; Gurubhagavatula, I. OSA Assessment Tools Task Force of the American Academy of Sleep Medicine. Evaluation of Clinical Tools to Screen and Assess for Obstructive Sleep Apnea. J. Clin. Sleep Med. 2018, 14, 1239–1244. [Google Scholar] [CrossRef]
- Manfredini, D.; Ahlberg, J.; Wetselaar, P.; Svensson, P.; Lobbezoo, F. The bruxism construct: From cut-off points to a continuum spectrum. J. Oral Rehabil. 2019, 46, 991–997. [Google Scholar] [CrossRef]
- Deregibus, A.; Castroflorio, T.; Bargellini, A.; Debernardi, C. Reliability of a portable device for the detection of sleep bruxism. Clin. Oral Investig. 2014, 18, 2037–2043. [Google Scholar] [CrossRef]
- Smardz, J.; Martynowicz, H.; Wojakowska, A.; Michalek-Zrabkowska, M.; Mazur, G.; Wieczorek, T.; Wieckiewicz, M. The meaning of the masticatory muscle tonic-type electromyographic pathway correlated with sleep bruxism and sleep-related breathing disorders—A polysomnographic study. Sleep Med. 2020, 68, 131–137. [Google Scholar] [CrossRef]
- Martynowicz, H.; Gac, P.; Brzecka, A.; Poreba, R.; Wojakowska, A.; Mazur, G.; Smardz, J.; Wieckiewicz, M. The Relationship between Sleep Bruxism and Obstructive Sleep Apnea Based on Polysomnographic Findings. J. Clin. Med. 2019, 8, 1653. [Google Scholar] [CrossRef]
- Haghayegh, S.; Kang, H.A.; Khoshnevis, S.; Smolensky, M.H.; Diller, K.R. A comprehensive guideline for Bland–Altman and intra class correlation calculations to properly compare two methods of measurement and interpret findings. Physiol. Meas. 2020, 41, 055012. [Google Scholar] [CrossRef]
- Molnár, V.; Lakner, Z.; Molnár, A.; Tárnoki, D.L.; Tárnoki, D.; Kunos, L.; Jokkel, Z.; Tamás, L. The Predictive Role of the Upper-Airway Adipose Tissue in the Pathogenesis of Obstructive Sleep Apnoea. Life 2022, 12, 1543. [Google Scholar] [CrossRef] [PubMed]
- Molnár, V.; Molnár, A.; Lakner, Z.; Tárnoki, D.L.; Tárnoki, D.; Jokkel, Z.; Kunos, L.; Tamás, L. The prognostic role of ultrasound and magnetic resonance imaging in obstructive sleep apnoea based on lateral oropharyngeal wall obstruction. Sleep Breath. 2023, 27, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Thie, N.M.; Huynh, N.; Miyawaki, S.; Lavigne, G.J. Topical review: Sleep bruxism and the role of peripheral sensory influences. J. Orofac. Pain 2003, 17, 191–213. [Google Scholar]
- Gallo, L.M.; Lavigne, G.; Rompre, P.; Palla, S. Reliability of scoring EMG orofacial events: Polysomnography compared with ambulatory recordings. J. Sleep Res. 1997, 6, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Shochat, T.; Gavish, A.; Arons, E.; Hadas, N.; Molotsky, A.; Lavie, P.; Oksenberg, A. Validation of the BiteStrip screener for sleep bruxism. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2007, 104, e32–e39. [Google Scholar] [CrossRef] [PubMed]
- Mainieri, V.C.; Saueressig, A.C.; Pattussi, M.P.; Fagondes, S.C.; Grossi, M.L. Validation of the Bitestrip versus polysomnography in the diagnosis of patients with a clinical history of sleep bruxism. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2012, 113, 612–617. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Abe, S.; Rompré, P.H.; Manzini, C.; Lavigne, G.J. Comparison of ambulatory and polysomnographic recording of jaw muscle activity during sleep in normal subjects. J. Oral Rehabil. 2012, 39, 2–10. [Google Scholar] [CrossRef]
- Stuginski-Barbosa, J.; Porporatti, A.L.; Costa, Y.M.; Svensson, P.; Conti, P.C.R. Diagnostic validity of the use of a portable single-channel electromyography device for sleep bruxism. Sleep Breath. 2016, 20, 695–702. [Google Scholar] [CrossRef]
- Miettinen, T.; Myllymaa, K.; Muraja-Murro, A.; Westeren-Punnonen, S.; Hukkanen, T.; Töyräs, J.; Lappalainen, R.; Mervaala, E.; Sipilä, K.; Myllymaa, S. Screen-printed ambulatory electrode set enables accurate diagnostics of sleep bruxism. J. Sleep Res. 2018, 27, 103–112. [Google Scholar] [CrossRef]
- Maeda, M.; Yamaguchi, T.; Mikami, S.; Yachida, W.; Saito, T.; Sakuma, T.; Nakamura, H.; Saito, M.; Mizuno, M.; Yamada, K.; et al. Validity of single-channel masseteric electromyography by using an ultraminiature wearable electromyographic device for diagnosis of sleep bruxism. J. Prosthodont. Res. 2020, 64, 90–97. [Google Scholar] [CrossRef]
- Sakuma, T.; Yamaguchi, T.; Maeda, M.; Saito, T.; Nakamura, H.; Mikami, S.; Saito, M.; Nakajima, T.; Mizuno, M.; Yamada, K.; et al. Comparison of the occurrence of sleep bruxism under accustomed conditions at home and under polysomnography conditions in a sleep laboratory. J. Prosthodont. Res. 2022, 66, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Yanez-Regonesi, F.; Eisa, E.; Judge, S.; Carlson, C.; Okeson, J.; Moreno-Hay, I. Diagnostic accuracy of a portable device (Bruxoff®) to measure sleep bruxism. J. Oral Rehabil. 2023, 50, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Maluly, M.; Andersen, M.; Dal-Fabbro, C.; Garbuio, S.; Bittencourt, L.; de Siqueira, J.; Tufik, S. Polysomnographic Study of the Prevalence of Sleep Bruxism in a Population Sample. J. Dent. Res. 2013, 92 (Suppl. S7), S97–S103. [Google Scholar] [CrossRef] [PubMed]
- Tsujisaka, A.; Haraki, S.; Nonoue, S.; Mikami, A.; Adachi, H.; Mizumori, T.; Yatani, H.; Yoshida, A.; Kato, T. The occurrence of respiratory events in young subjects with a frequent rhythmic masticatory muscle activity: A pilot study. J. Prosthodont. Res. 2018, 62, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.U.; Tan, M.W.Y.; Tan, S.H.X.; Chua, A.P. Sleep bruxism events: An epiphenomenon of severe obstructive sleep apnea? Clin. Oral Investig. 2023, 27, 4633–4642. [Google Scholar] [CrossRef] [PubMed]
- Okura, M.; Kato, T.; Mashita, M.; Muraki, H.; Sugita, H.; Ohi, M.; Taniguchi, M. Relationships between respiratory and oromotor events differ between motor phenotypes in patients with obstructive sleep apnea. Front. Neurol. 2023, 21, 14. [Google Scholar] [CrossRef]
- Kato, T.; Montplaisir, J.Y.; Blanchet, P.J.; Lund, J.P.; Lavigne, G.J. Idiopathic myoclonus in the oromandibular region during sleep: A possible source of confusion in sleep bruxism diagnosis. Mov. Disord. 1999, 14, 865–871. [Google Scholar] [CrossRef]
- Carra, M.C.; Huynh, N.; Lavigne, G.J. Diagnostic accuracy of sleep bruxism scoring in absence of audio-video recording: A pilot study. Sleep Breath. 2015, 19, 183–190. [Google Scholar] [CrossRef]
- Raphael, K.G.; Santiago, V.; Lobbezoo, F. Is bruxism a disorder or a behaviour? Rethinking the international consensus on defining and grading of bruxism. J. Oral Rehabil. 2016, 43, 791–798. [Google Scholar] [CrossRef]
- Merletti, R.; Hermens, H. Introduction to the special issue on the SENIAM European Concerted Action. J. Electromyogr. Kinesiol. 2000, 10, 283–286. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. European recommendations for surface electromyography: Results of the SENIAM Project. Roessingh Res. Dev. 1999, 8, 13–54. [Google Scholar]
- De Luca, C.J. The Use of Surface Electromyography in Biomechanics. J. Appl. Biomech. 1997, 13, 135–163. [Google Scholar] [CrossRef]
- Martinot, J.-B.; Le-Dong, N.-N.; Cuthbert, V.; Denison, S.; Gozal, D.; Lavigne, G.; Pépin, J.-L. Artificial Intelligence Analysis of Mandibular Movements Enables Accurate Detection of Phasic Sleep Bruxism in OSA Patients: A Pilot Study. Nat. Sci. Sleep 2021, 13, 1449–1459. [Google Scholar] [CrossRef]
- Vicente-Samper, J.M.; Tamantini, C.; Ávila-Navarro, E.; De La Casa-Lillo, M.; Zollo, L.; Sabater-Navarro, J.M.; Cordella, F. An ML-Based Approach to Reconstruct Heart Rate from PPG in Presence of Motion Artifacts. Biosensors 2023, 13, 718. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef]
- Almarshad, M.A.; Al-Ahmadi, S.; Islam, M.S.; BaHammam, A.S.; Soudani, A. Adoption of Transformer Neural Network to Improve the Diagnostic Performance of Oximetry for Obstructive Sleep Apnea. Sensors 2023, 23, 7924. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Lavigne, G.; Rompré, P.; Kato, T.; Urade, M.; Huynh, N. Is there a First Night Effect on Sleep Bruxism? A Sleep Laboratory Study. J. Clin. Sleep Med. 2013, 9, 1139–1145. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Paesani, D.A. Bruxismo: Teoría y Práctica; Quintessence: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- De Leeuw, R.; Klasser, G.D. Orofacial Pain, Guidelines for Assessment, Diagnosis, and Management, 5th ed.; The American Academy of Orofacial Pain: Oceanville, NJ, USA, 2008. [Google Scholar]
- Smardz, J.; Wieckiewicz, M.; Michalek-Zrabkowska, M.; Gac, P.; Poreba, R.; Wojakowska, A.; Blaszczyk, B.; Mazur, G.; Martynowicz, H. Is camera recording crucial for the correct diagnosis of sleep bruxism in polysomnography? J. Sleep Res. 2023, 13, 32. [Google Scholar] [CrossRef]
- Goyal, M.; Johnson, J. Obstructive Sleep Apnea Diagnosis and Management. Mo. Med. 2017, 114, 120–124. [Google Scholar] [PubMed]
- Lavigne, G.J.; Rompré, P.H.; Poirier, G.; Huard, H.; Kato, T.; Montplaisir, J.Y. Rhythmic Masticatory Muscle Activity during Sleep in Humans. J. Dent. Res. 2001, 80, 443–448. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 22 | |
|---|---|
| Mean ± SD | |
| Physical data | |
| Age | 46.55 ± 11.06 |
| BMI | 27.23 ± 5.38 |
| Sleep data | |
| SPT (min) | 411.55 ± 27.31 |
| TST (min) | 330.05 ± 62.42 |
| SLT (min) | 13.86 ± 26.87 |
| Sleep efficiency (%) | 81.66 ± 14.89 |
| WASO (min) | 56.30 ± 47.86 |
| Awakes (number) | 44.05 ± 25.16 |
| Sleep stage distribution | |
| N1/SPT (%) | 25.12 ± 16.60 |
| N2/SPT (%) | 43.85 ± 9.37 |
| N3/SPT (%) | 15.99 ± 10.91 |
| R/SPT (%) | 15.43 ± 5.92 |
| Pulse oximetry data | |
| Mean (%) | 93.45 ± 2.98 |
| Max (%) | 98.32 ± 1.04 |
| Min (%) | 81.09 ± 11.03 |
| CT90 (%) | 12.94 ± 23.65 |
| Sleep apnea data | |
| No. apneas | 106.18 ± 161.17 |
| No. hypopneas | 30.32 ± 31.24 |
| No. apneas + hypopneas | 136.50 ± 172.87 |
| AHI | 25.25 ± 32.83 |
| N = 22 | ||
|---|---|---|
| Mean ± SD | t | |
| Polysomnography | ||
| No. episodes/night | 8.41 ± 10.85 | 3.63 |
| No. episodes/h | 1.49 ± 2.05 | 3.39 |
| No. phasic episodes | 2.00 ± 4.48 | 2.09 |
| No. tonic episodes | 5.55 ± 7.06 | 3.68 |
| No. mixed episodes | 0.86 ± 1.67 | 2.42 |
| Automatic Bruxoff | ||
| No. episodes/night | 22.68 ± 16.02 | 6.64 |
| No. episodes/h | 3.92 ± 2.71 | 6.78 |
| No. phasic episodes | 5.82 ± 5.37 | 5.06 |
| No. tonic episodes | 5.77 ± 6.90 | 3.87 |
| No. mixed episodes | 1.23 ± 1.87 | 3.06 |
| Manual Bruxoff | ||
| No. episodes/night | 14.64 ± 10.76 | 6.37 |
| No. episodes/h | 2.54 ± 1.95 | 6.13 |
| No. phasic episodes | 5.27 ± 4.50 | 5.49 |
| No. tonic episodes | 8.05 ± 7.82 | 4.82 |
| No. mixed episodes | 1.32 ± 2.00 | 3.07 |
| N = 22 | |||
|---|---|---|---|
| Non OSA ± SD N = 6 | OSA ± SD N = 16 | F | |
| SB Polysomnography | |||
| Total episodes | 13.71 ± 13.76 * | 5.93 ± 8.64 * | 4.58 |
| Phasic episodes | 4.43 ± 7.39 * | 0.87 ± 1.52 * | 10.10 |
| Tonic episodes | 8.14 ± 8.57 | 4.33 ± 6.20 | 1.83 |
| Mixed episodes | 1.14 ± 1.86 | 0.73 ± 16.62 | 0.25 |
| Ep./h | 2.11 ± 2.07 | 1.20 ± 2.07 | 0.74 |
| SB Automatic Bruxoff | |||
| Total episodes | 23.14 ± 11.69 | 22.47 ± 18.07 | 0.95 |
| Phasic episodes | 7.14 ± 6.25 | 5.20 ± 5.04 | 0.331 |
| Tonic episodes | 5.00 ± 4.65 | 6.13 ± 7.97 | 2.76 |
| Mixed episodes | 1.43 ± 1.81 | 1.13 ± 1.95 | 0.00 |
| Ep./h | 4.38 ± 2.38 | 3.70 ± 2.90 | 0.80 |
| SB Manual Bruxoff | |||
| Total episodes | 16.14 ± 10.73 | 13.93 ± 11.08 | 0.20 |
| Phasic episodes | 6.43 ± 6.47 * | 4.73 ± 3.39 * | 5.07 |
| Tonic episodes | 8.57 ± 8.26 | 7 80 ± 7.89 | 0.03 |
| Mixed episodes | 1.14 ± 1.86 | 1.40 ± 2.13 | 0.18 |
| Ep./h | 3.15 ± 2.35 | 2.26 ± 1.74 | 1.19 |
| N = 22 | |||||
|---|---|---|---|---|---|
| Non OSA ± SD N = 6 | Mild OSA ± SD N = 7 | Moderate OSA ± SD N = 3 | Severe OSA ± SD N = 6 | F | |
| SB Polysomnography | |||||
| Total episodes | 16 ± 13.55 | 5.57 ± 6.13 | 10.33 ± 17.89 | 3.17 ± 4.66 | 1.83 |
| Tonic episodes | 9.50 ± 8.52 | 5.85 ± 2.21 | 6.67 ± 11.54 | 2.17 ± 2.86 | 1.18 |
| Phasic episodes | 5.17 ± 7.80 | 0.57 ± 1.13 | 1.67 ± 2.88 | 0.67 ± 1.21 | 1.52 |
| Mixed episodes | 1.33 ± 1.97 | 0.43 ± 0.78 | 2.00 ± 3.46 | 0,33 ± 0.82 | 0.97 |
| Episodes/h | 2.46 ± 2.03 | 0.93 ± 1.01 | 2.67 ± 4.61 | 0.80 ± 0.70 | 1.40 |
| SB Automatic Bruxoff | |||||
| Total episodes | 24.50 ± 12.19 | 26 ± 20.44 | 18 ± 24.26 | 19.33 ± 12.13 | 0.26 |
| Tonic episodes | 4.83 ± 5.07 | 6.71 ± 5.67 | 8 ± 13 | 4.50 ± 8.12 | 0.21 |
| Phasic episodes | 7.67 ± 6.68 | 7.29 ± 5.31 | 2.33 ± 3.21 | 4.00 ± 4.56 | 1.06 |
| Mixed episodes | 1.67 ± 1.86 | 0.86 ± 1.21 | 1.33 ± 1.52 | 1.27 ± 2.86 | 0.72 |
| Episodes/h | 4.68 ± 2.45 | 4.34 ± 3.24 | 2.6 ± 3.55 | 3.33 ± 2.19 | 0.50 |
| SB Manual Bruxoff | |||||
| Total episodes | 16.83 ± 11.58 | 16.14 ± 10.30 | 14 ± 18.19 | 11.00 ± 8.22 | 0.32 |
| Tonic episodes | 9 ± 8.96 | 8.29 ± 6.39 | 7.67 ± 11.59 | 7.00 ± 8.44 | 0.61 |
| Phasic episodes | 6.5 ± 7.09 | 6.71 ± 3.86 | 4 ± 2.64 | 3.00 ± 1.55 | 0.92 |
| Mixed episodes | 1.33 ± 1.96 | 1.14 ± 1.86 | 2.33 ± 4.04 | 1.00 ± 1.26 | 0.29 |
| Episodes/h | 3.33 ± 2.52 | 2.6 ± 1.41 | 2.03 ± 2.65 | 1.95 ± 1.71 | 0.55 |
| SB Episodes (N = 22) | |||
|---|---|---|---|
| Non OSA N = 6 | Mild OSA N = 7 | Moderate OSA N = 3 | Severe OSA N = 6 |
| 0.61 | 0.53 * | 0.24 | 0.23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cid-Verdejo, R.; Domínguez Gordillo, A.A.; Sánchez-Romero, E.A.; Ardizone García, I.; Martínez Orozco, F.J. Diagnostic Accuracy of a Portable Electromyography and Electrocardiography Device to Measure Sleep Bruxism in a Sleep Apnea Population: A Comparative Study. Clocks & Sleep 2023, 5, 717-733. https://doi.org/10.3390/clockssleep5040047
Cid-Verdejo R, Domínguez Gordillo AA, Sánchez-Romero EA, Ardizone García I, Martínez Orozco FJ. Diagnostic Accuracy of a Portable Electromyography and Electrocardiography Device to Measure Sleep Bruxism in a Sleep Apnea Population: A Comparative Study. Clocks & Sleep. 2023; 5(4):717-733. https://doi.org/10.3390/clockssleep5040047
Chicago/Turabian StyleCid-Verdejo, Rosana, Adelaida A. Domínguez Gordillo, Eleuterio A. Sánchez-Romero, Ignacio Ardizone García, and Francisco J. Martínez Orozco. 2023. "Diagnostic Accuracy of a Portable Electromyography and Electrocardiography Device to Measure Sleep Bruxism in a Sleep Apnea Population: A Comparative Study" Clocks & Sleep 5, no. 4: 717-733. https://doi.org/10.3390/clockssleep5040047