
Light–Dark and Activity Rhythm Therapy (L-DART) to Improve Sleep in People with Schizophrenia Spectrum Disorders: A Single-Group Mixed Methods Study of Feasibility, Acceptability and Adherence


Abstract
:1. Introduction
2. Results
2.1. Recruitment and Demographics
2.1.1. Recruitment
2.1.2. Demographics
2.1.3. Sleep Problem Phenotypes and Participant Goals
2.2. Study Attrition and Data Completeness
2.3. Attendance, Delivery, and Adherence Summary
2.3.1. Therapy Session Delivery and Attendance
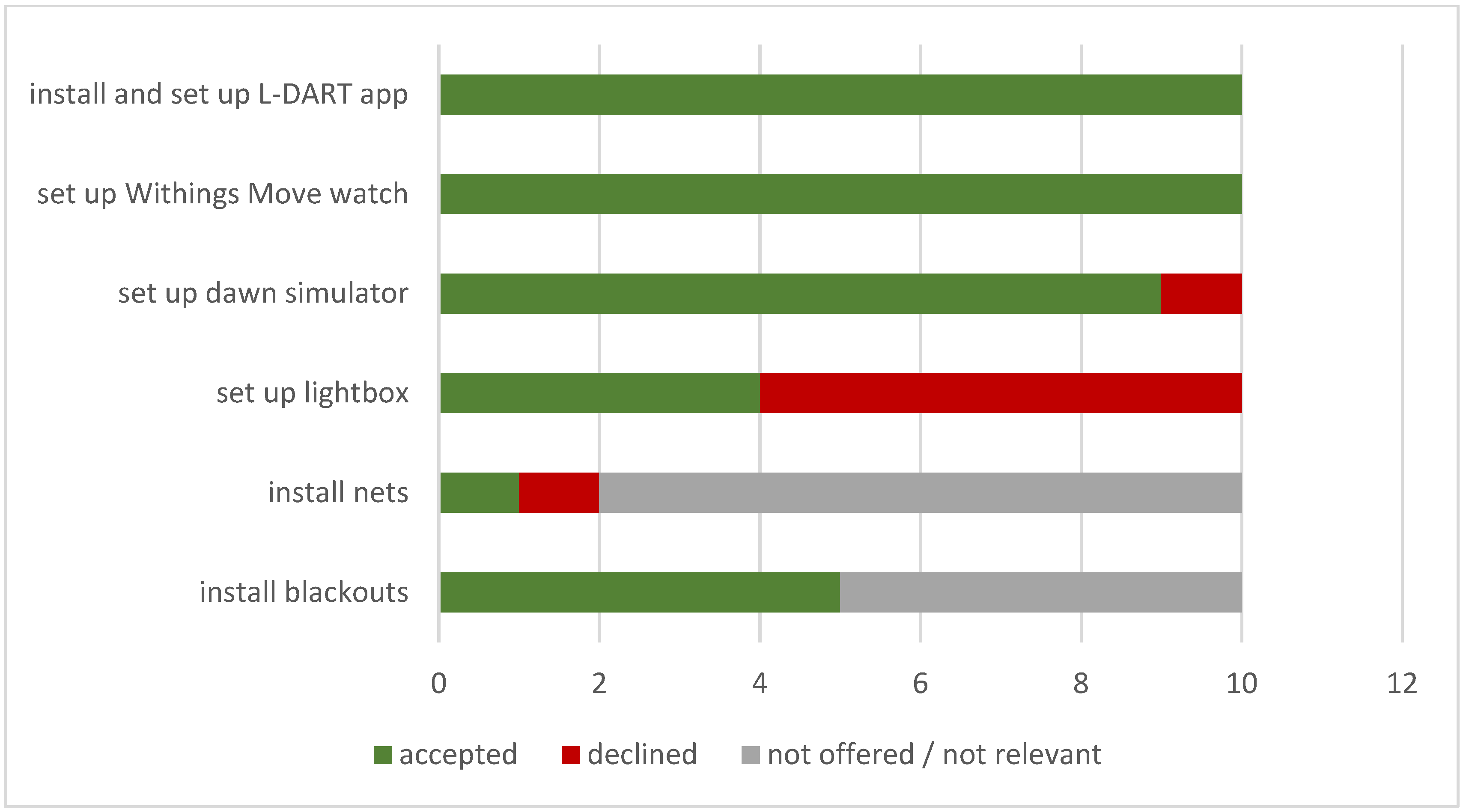
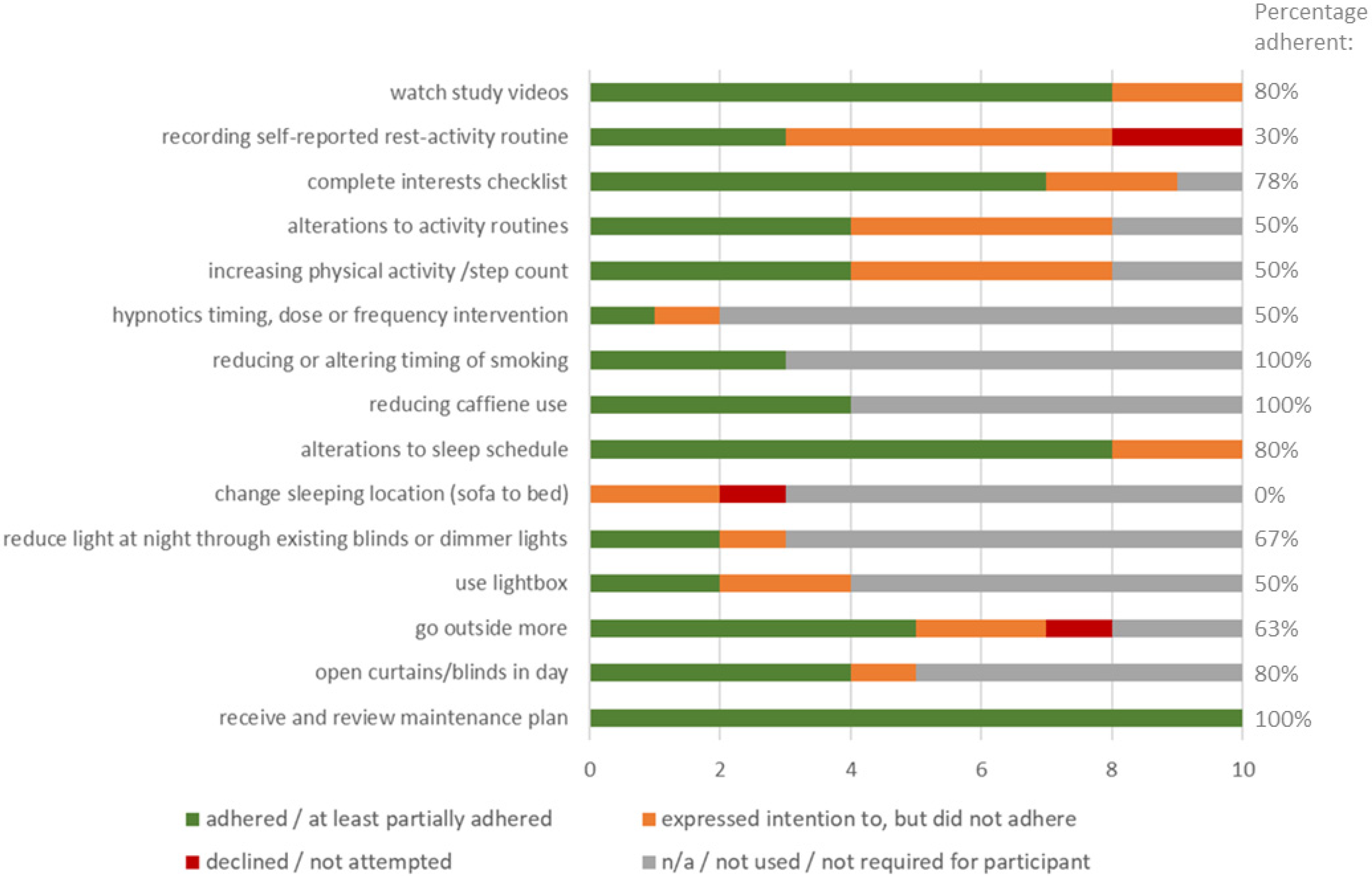
2.3.2. Intervention Component Delivery and Adherence Summary
2.4. Intervention Component Delivery, Adherence, Barriers and Facilitators, and Perceived Impact, from Qualitative Accounts, Therapy Notes, and Passive Data
2.4.1. Explaining the Intervention Rationale to Participants, Educational Content
2.4.2. Recording Self-Reported Rest Activity Routine
2.4.3. Interests Checklist
2.4.4. Use of Passively Monitored Activity Pattern Plots within the Therapy
2.4.5. Altering Daytime Activity Routines
2.4.6. Increasing Physical Activity Levels or Step Count
2.4.7. Alteration of Meal Timing
2.4.8. Hypnotics
2.4.9. Smoking
2.4.10. Caffeine
2.4.11. Addressing Comorbidities
2.4.12. Alterations to Sleep Schedule
2.4.13. Sleep Compression and Time in Bed Reduction
2.4.14. Stimulus Control (‘Go to Bed Only when Sleepy’, ‘Use the Bed Only for Sleep’, and ‘the 15 Min Rule’)
2.4.15. Regular Rise Time
2.4.16. Altering Overall Sleep Timing (Bed Time and Rise Time)
2.4.17. Dawn Simulator/Wake up Light
2.4.18. Increasing Daytime Natural Light Exposure
2.4.19. Light Box
2.4.20. Reducing Light at Night
2.5. Barriers and Facilitators to Adherence (Overall)
2.5.1. Expectations and Motivation
2.5.2. Format, Scheduling and Duration
2.5.3. Interpersonal Factors
2.5.4. Impact of Social and Physical Environment, including COVID Pandemic
2.5.5. Linking with Other Care Providers and Services
2.6. Acceptability
2.6.1. Quantitative Acceptability Ratings
2.6.2. Qualitative Acceptability Data
2.7. Adverse Events and Adverse Effects
2.7.1. Unrelated Adverse Events
2.7.2. Adverse Effects
2.8. Outcomes
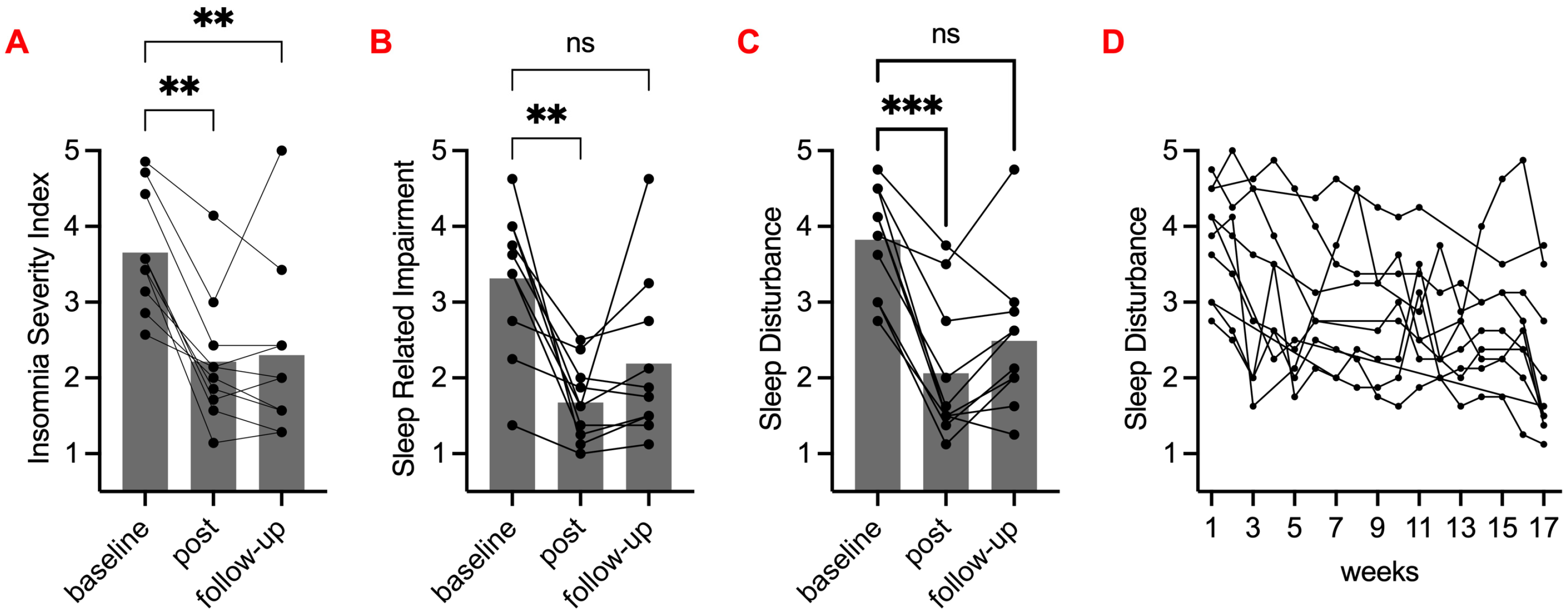
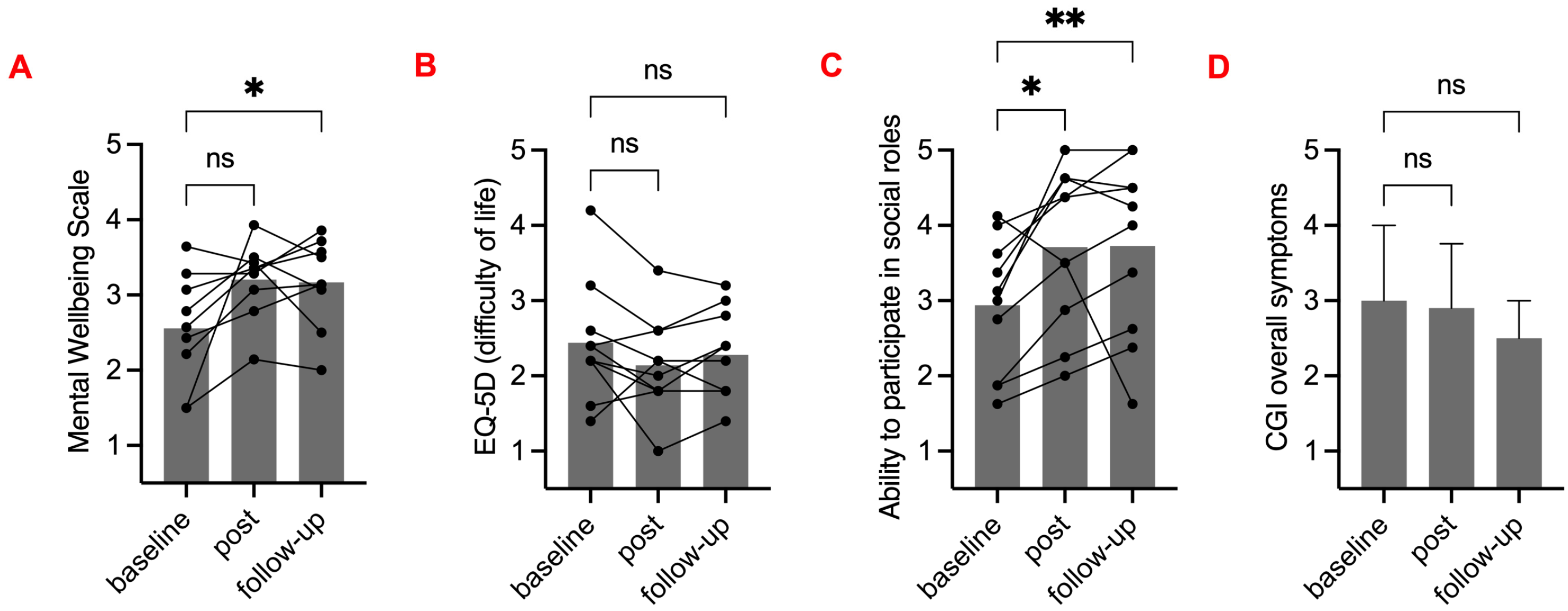
2.8.1. Self-Reported and Therapist Rated Outcomes
2.8.2. Qualitative Reports on Outcomes
“…so much more awake and alive compared to how I was.”
“…there’s more time for going out and making appointments for in the mornings, cos one time I could never make an appointment anywhere in the morning. But at this time now I can make more appointments and I can go out more. It’s changed my life, this therapy.”
3. Discussion
4. Materials and Methods
4.1. Study Population
Recruitment Method
4.2. Ethical Approval and Study Commencement
4.3. Data Collection
4.3.1. Season of Data Collection and Intervention
4.3.2. Routine Clinical Data
4.3.3. Adverse Events and Adverse Effects
4.3.4. Custom Measures
4.3.5. Qualitative Data Collection
4.3.6. Standardised Outcome Measures
4.3.7. Passive Data/Objective Data
4.4. Intervention Content and Format
4.4.1. Assessment, formulation, and goal setting
4.4.2. Intervention Components and Delivery
- Light exposure patterns across the day;
- Nature, balance, and timing of activities;
- Sleep schedule modifications;
- Optional components (when relevant) include:
- Reducing or changing the timing of the use of caffeine, alcohol, illicit drugs, and over-the-counter medications;
- Altering or regulating the timing of sleep-inducing prescribed medications;
- Addressing meal timing;
- Addressing nightmares;
- Methods to reduce or avoid daytime naps.
4.5. Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meyer, N.; Faulkner, S.M.; McCutcheon, R.A.; Pillinger, T.; Dijk, D.-J.; MacCabe, J.H. Sleep and Circadian Rhythm Disturbance in Remitted Schizophrenia and Bipolar Disorder: A Systematic Review and Meta-analysis. Schizophr. Bull. 2020, 46, 1126–1143. [Google Scholar] [CrossRef] [PubMed]
- Barrett, E.A.; Aminoff, S.R.; Simonsen, C.; Romm, K.L. Opening the curtains for better sleep in psychotic disorders-considerations for improving sleep treatment. Compr. Psychiatry 2020, 103, 152207. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, M.; Rahim, M.; Hall, C. The prevalence and management of poor sleep quality in a secondary care mental health population. J. Clin. Sleep Med. 2015, 11, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, K.; Knutson, K.; Leproult, R.; Tasali, E.; Van Cauter, E. Sleep loss: A novel risk factor for insulin resistance and Type 2 diabetes. J. Appl. Physiol. 2005, 99, 2008–2019. [Google Scholar] [CrossRef] [PubMed]
- Krystal, A.D.; Thakur, M.; Roth, T. Sleep Disturbance in Psychiatric Disoders: Effects on Function and Quality of Life in Mood Disorders, Alcoholism, and Schizophrenia. Ann. Clin. Psychiatry 2008, 20, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Meerlo, P.; Sgoifo, A.; Suchecki, D. Restricted and disrupted sleep: Effects on autonomic function, neuroendocrine stress systems and stress responsivity. Sleep Med. Rev. 2008, 12, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Haus, E.L.; Smolensky, M.H. Shift work and cancer risk: Potential mechanistic roles of circadian disruption, light at night, and sleep deprivation. Sleep Med. Rev. 2013, 17, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Afonso, P.; Brissos, S.; Cañas, F.; Bobes, J.; Bernardo-Fernandez, I. Treatment adherence and quality of sleep in schizophrenia outpatients. Int. J. Psychiatry Clin. Pract. 2014, 18, 70–76. [Google Scholar] [CrossRef]
- Wulff, K.; Joyce, E. Circadian rhythms and cognition in schizophrenia. Br. J. Psychiatry 2011, 198, 250–252. [Google Scholar] [CrossRef]
- Faulkner, S.; Bee, P. Experiences, perspectives and priorities of people with schizophrenia spectrum disorders regarding sleep disturbance and its treatment: A qualitative study. BMC Psychiatry 2017, 17, 158. [Google Scholar] [CrossRef]
- Jagannath, A.; Peirson, S.N.; Foster, R.G. Sleep and circadian rhythm disruption in neuropsychiatric illness. Curr. Opin. Neurobiol. 2013, 23, 888–894. [Google Scholar] [CrossRef] [PubMed]
- Waite, F.; Sheaves, B.; Isham, L.; Reeve, S.; Freeman, D. Sleep and schizophrenia: From epiphenomenon to treatable causal target. Schizophr. Res. 2020, 221, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Auslander, L.A.; Jeste, D.V. Perceptions of problems and needs for service among middle-aged and elderly outpatients with schizophrenia and related psychotic disorders. Community Ment. Health J. 2002, 38, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Waite, F.; Evans, N.; Myers, E.; Startup, H.; Lister, R.; Harvey, A.G.; Freeman, D. The patient experience of sleep problems and their treatment in the context of current delusions and hallucinations. Psychol. Psychother. Theory Res. Pract. 2015, 89, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, S.; Bee, P. Perspectives on Sleep, Sleep Problems, and Their Treatment, in People with Serious Mental Illnesses: A Systematic Review. PLoS ONE 2016, 11, e0163486. [Google Scholar] [CrossRef] [PubMed]
- Bersani, F.S.; Iannitelli, A.; Pacitti, F.; Bersani, G. Sleep and biorythm disturbances in schizophrenia, mood and anxiety disorders: A review. Riv. Psichiatr. 2012, 47, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Eklund, M.; Erlandsson, L.; Leufstadius, C. Time use in relation to valued and satisfying occupations among people with persistent mental illness: Exploring occupational balance. J. Occup. Sci. 2010, 17, 231–238. [Google Scholar] [CrossRef]
- Wulff, K.; Dijk, D.-J.; Middleton, B.; Foster, R.G.; Joyce, E.M. Sleep and circadian rhythm disruption in schizophrenia. Br. J. Psychiatry 2012, 200, 308–316. [Google Scholar] [CrossRef]
- Skeldon, A.C.; Dijk, D.-J.; Meyer, N.; Wulff, K. Extracting Circadian and Sleep Parameters from Longitudinal Data in Schizophrenia for the Design of Pragmatic Light Interventions. Schizophr. Bull. 2022, 48, 447–456. [Google Scholar] [CrossRef]
- Hubbard, J.; Ruppert, E.; Gropp, C.-M.; Bourgin, P. Non-circadian direct effects of light on sleep and alertness: Lessons from transgenic mouse models. Sleep Med. Rev. 2013, 17, 445–452. [Google Scholar] [CrossRef]
- Tao, Q.; Mu, Y.-M.; Huang, X.-D.; Zhu, S.; Hu, Z.-F.; So, K.-F.; Ren, C.-R. Alerting effects of light in healthy individuals: A systematic review and meta-analysis. Neural Regen. Res. 2022, 17, 1929–1936. [Google Scholar] [CrossRef] [PubMed]
- Wright, K.P., Jr.; McHill, A.W.; Birks, B.R.; Griffin, B.R.; Rusterholz, T.; Chinoy, E.D. Entrainment of the human circadian clock to the natural light-dark cycle. Curr. Biol. 2013, 23, 1554–1558. [Google Scholar] [CrossRef] [PubMed]
- Ashton, A.; Foster, R.G.; Jagannath, A. Photic Entrainment of the Circadian System. Int. J. Mol. Sci. 2022, 23, 729. [Google Scholar] [CrossRef] [PubMed]
- Geoffroy, P.A.; Schroder, C.M.; Reynaud, E.; Bourgin, P. Efficacy of light therapy versus antidepressant drugs, and of the combination versus monotherapy, in major depressive episodes: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 48, 101213. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Jiang, R.; Zhang, K.; Qian, Z.; Chen, P.; Lv, Y.; Yao, Y. Light therapy in non-seasonal depression: An update meta-analysis. Psychiatry Res. 2020, 291, 113247. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, D.C.; Fogerson, P.M.; Ospri, L.L.; Thomsen, M.B.; Layne, R.M.; Severin, D.; Zhan, J.; Singer, J.H.; Kirkwood, A.; Zhao, H.; et al. Light Affects Mood and Learning through Distinct Retina-Brain Pathways. Cell 2018, 175, 71–84.e18. [Google Scholar] [CrossRef] [PubMed]
- Burns, A.C.; Windred, D.P.; Rutter, M.K.; Olivier, P.; Vetter, C.; Saxena, R.; Lane, J.M.; Phillips, A.J.; Cain, S.W. Low daytime light and bright night-time light are associated with psychiatric disorders: An objective light study in >85,000 UK Biobank participants. medRxiv 2022. medRxiv:2022:2022-10. [Google Scholar]
- Chiu, V.W.; Harvey, R.H.; Sloan, N.B.; Ree, M.; Lin, A.; Janca, A.; Waters, F. Cognitive and Behavioral Factors Associated with Insomnia in Inpatients with Schizophrenia and Related Psychoses. J. Nerv. Ment. Dis. 2015, 203, 798–803. [Google Scholar] [CrossRef]
- Gurpegui, M.; Aguilar, M.C.; Martínez-Ortega, J.M.; Diaz, F.J.; de Leon, J. Caffeine Intake in Outpatients with Schizophrenia. Schizophr. Bull. 2004, 30, 935–945. [Google Scholar] [CrossRef]
- Thompson, L.; Pennay, A.; Zimmermann, A.; Cox, M.; Lubman, D.I. “Clozapine makes me quite drowsy, so when I wake up in the morning those first cups of coffee are really handy”: An exploratory qualitative study of excessive caffeine consumption among individuals with schizophrenia. BMC Psychiatry 2014, 14, 116. [Google Scholar] [CrossRef]
- Hombali, A.; Seow, E.; Yuan, Q.; Chang, S.H.S.; Satghare, P.; Kumar, S.; Verma, S.K.; Mok, Y.M.; Chong, S.A.; Subramaniam, M. Prevalence and correlates of sleep disorder symptoms in psychiatric disorders. Psychiatry Res. 2019, 279, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Yoon, B.; Choi, H.; Park, S.; Pac, J. Prevalence of restless legs syndrome and its correlates in schizophrenic inpatients. In European Neuropsychopharmacology; Elsevier: Naju, Republic of Korea, 2011; pp. S460–S461, (24th Congress of the European College of Neuropsychopharmacology; Volume 21). [Google Scholar]
- Myles, H.; Myles, N.; Vincent, A.D.; Wittert, G.; Adams, R.; Chandratilleke, M.; Liu, D.; Mercer, J.; Vakulin, A.; Chai-Coetzer, C.L.; et al. Pilot cohort study of obstructive sleep apnoea in community-dwelling people with schizophrenia. Ir. J. Psychol. Med. 2020, 38, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Reeve, S.; Sheaves, B.; Freeman, D. Excessive sleepiness in patients with psychosis: An initial investigation. PLoS ONE 2021, 16, e0245301. [Google Scholar] [CrossRef] [PubMed]
- Chiu, V.W.; Ree, M.; Janca, A.; Iyyalol, R.; Dragovic, M.; Waters, F. Sleep profiles and CBT-I response in schizophrenia and related psychoses. Psychiatry Res. 2018, 268, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, S.M.; Drake, R.J.; Ogden, M.; Gardani, M.; Bee, P.E. A mixed methods expert opinion study on the optimal content and format for an occupational therapy intervention to improve sleep in schizophrenia spectrum disorders. PLoS ONE 2022, 17, e0269453. [Google Scholar] [CrossRef] [PubMed]
- Matthews, E.E.; Arnedt, J.T.; McCarthy, M.S.; Cuddihy, L.J.; Aloia, M.S. Adherence to cognitive behavioral therapy for insomnia: A systematic review. Sleep Med. Rev. 2013, 17, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.B.; Espie, C.A.; Epstein, D.R.; Friedman, L.; Morin, C.M.; Pigeon, W.R.; Spielman, A.J.; Kyle, S.D. The evidence base of sleep restriction therapy for treating insomnia disorder. Sleep Med. Rev. 2014, 18, 415–424. [Google Scholar] [CrossRef]
- Solet, J.M. Sleep and rest. In Willard and Spackman’s Occupational Therapy, 12th ed.; Schell, B.A., Gillen, G., Scaffa, M., Cohn, E.S., Eds.; Wolters Kluwer-Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2014; pp. 714–730. [Google Scholar]
- Green, A.; Brown, C. An Occupational Therapist’s Guide to Sleep and Sleep Problems; Jessica Kingsley Publishers: London, UK, 2015. [Google Scholar]
- Faulkner, S.M.; Drake, R.J.; Eisner, E.; Bee, P.E. Sleep problems and referral intentions in mental health services: Service user self-report and staff proxy report surveys. BMC Psychiatry 2023, 23, 583. [Google Scholar] [CrossRef]
- Kallestad, H.; Hansen, B.; Langsrud, K.; Ruud, T.; Morken, G.; Stiles, T.C.; Gråwe, R.W. Differences between patients’ and clinicians’ report of sleep disturbance: A field study in mental health care in Norway. BMC Psychiatry 2011, 11, 186. [Google Scholar] [CrossRef]
- Rehman, A.; Waite, F.; Sheaves, B.; Biello, S.; Freeman, D.; Gumley, A. Clinician perceptions of sleep problems, and their treatment, in patients with non-affective psychosis. Psychosis 2017, 9, 129–139. [Google Scholar] [CrossRef]
- Maurer, L.F.; Espie, C.A.; Kyle, S.D. How does sleep restriction therapy for insomnia work? A systematic review of mechanistic evidence and the introduction of the Triple-R model. Sleep Med. Rev. 2018, 42, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Ryu, S.-H.; Lee, B.R.; Kim, K.H.; Lee, E.; Choi, J. Effects of artificial light at night on human health: A literature review of observational and experimental studies applied to exposure assessment. Chronobiol. Int. 2015, 32, 1294–1310. [Google Scholar] [CrossRef] [PubMed]
- van Maanen, A.; Meijer, A.M.; van der Heijden, K.B.; Oort, F.J. The effects of light therapy on sleep problems: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 29, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Burns, A.C.; Saxena, R.; Vetter, C.; Phillips, A.J.; Lane, J.M.; Cain, S.W. Time spent in outdoor light is associated with mood, sleep, and circadian rhythm-related outcomes: A cross-sectional and longitudinal study in over 400,000 UK Biobank participants. J. Affect. Disord. 2021, 295, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Böhmer, M.N.; Oppewal, A.; Valstar, M.J.; Bindels, P.J.E.; van Someren, E.J.W.; Maes-Festen, D.A.M. Light up: An intervention study of the effect of environmental dynamic lighting on sleep–wake rhythm, mood and behaviour in older adults with intellectual disabilities. J. Intellect. Disabil. Res. 2022, 66, 756–781. [Google Scholar] [CrossRef] [PubMed]
- Sheaves, B.; Isham, L.; Bradley, J.; Espie, C.; Barrera, A.; Waite, F.; Harvey, A.G.; Attard, C.; Freeman, D. Adapted CBT to Stabilize Sleep on Psychiatric Wards: A Transdiagnostic Treatment Approach. Behav. Cogn. Psychother. 2018, 46, 661–675. [Google Scholar] [CrossRef] [PubMed]
- Harvey, A.G.; Dong, L.; Hein, K.; Yu, S.H.; Martinez, A.J.; Gumport, N.B.; Smith, F.L.; Chapman, A.; Lisman, M.; Mirzadegan, I.A.; et al. A randomized controlled trial of the Transdiagnostic Intervention for Sleep and Circadian Dysfunction (TranS-C) to improve serious mental illness outcomes in a community setting. J. Consult. Clin. Psychol. 2021, 89, 537–550. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Waite, F.; Startup, H.; Myers, E.; Lister, R.; McInerney, J.; Harvey, A.G.; Geddes, J.; Zaiwalla, Z.; Luengo-Fernandez, R.; et al. Efficacy of cognitive behavioural therapy for sleep improvement in patients with persistent delusions and hallucinations (BEST): A prospective, assessor-blind, randomised controlled pilot trial. Lancet Psychiatry 2015, 2, 975–983. [Google Scholar] [CrossRef]
- Bradley, J.; Freeman, D.; Chadwick, E.; Harvey, A.G.; Mullins, B.; Johns, L.; Sheaves, B.; Lennox, B.; Broome, M.; Waite, F. Treating Sleep Problems in Young People at Ultra-High Risk of Psychosis: A Feasibility Case Series. Behav. Cogn. Psychother. 2018, 46, 276–291. [Google Scholar] [CrossRef]
- Gonçalves, B.; Adamowicz, T.; Louzada, F.M.; Moreno, C.R.; Araujo, J.F. A fresh look at the use of nonparametric analysis in actimetry. Sleep Med. Rev. 2015, 20, 84–91. [Google Scholar] [CrossRef]
- Bastien, C.; Valliers, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric Indicators to Detect Insomnia Cases and Evaluate Treatment Response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Yu, L.; Moul, D.E.; Germain, A.; Stover, A.; Dodds, N.E.; Johnston, K.L.; Shablesky-Cade, M.A.; Pilkonis, P.A. Development and Validation of Patient-Reported Outcome Measures for Sleep Disturbance and Sleep-Related Impairments. Sleep 2010, 33, 781–792. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Buysse, D.J.; Germain, A.; Moul, D.E.; Stover, A.; Dodds, N.E.; Johnston, K.L.; Pilkonis, P.A. Development of Short Forms from the PROMISTM Sleep Disturbance and Sleep-Related Impairment Item Banks. Behav. Sleep Med. 2011, 10, 6–24. [Google Scholar] [CrossRef] [PubMed]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [PubMed]
- Janssen, M.F.; Pickard, A.S.; Golicki, D.; Gudex, C.; Niewada, M.; Scalone, L.; Swinburn, P.; Busschbach, J. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Qual. Life Res. 2013, 22, 1717–1727. [Google Scholar] [CrossRef] [PubMed]
- Hahn, E.A.; on behalf of the PROMIS Cooperative Group; DeVellis, R.F.; Bode, R.K.; Garcia, S.F.; Castel, L.D.; Eisen, S.V.; Bosworth, H.B.; Heinemann, A.W.; Rothrock, N.; et al. Measuring social health in the patient-reported outcomes measurement information system (PROMIS): Item bank development and testing. Qual. Life Res. 2010, 19, 1035–1044. [Google Scholar] [CrossRef] [PubMed]
- Haro, J.M.; Kamath, S.A.; Ochoa, S.; Novick, D.; Rele, K.; Fargas, A.; Rodríguez, M.J.; Rele, R.; Orta, J.; Kharbeng, A.; et al. The Clinical Global Impression–Schizophrenia scale: A simple instrument to measure the diversity of symptoms present in schizophrenia. Acta Psychiatr. Scand. Suppl. 2003, 107, 16–23. [Google Scholar] [CrossRef]
- Szaulińska, K.; Wichniak, A. BMI-NECK: A simple assessment of risk of obstructive sleep apnea in schizophrenia. J. Psychiatr. Res. 2020, 125, 33–37. [Google Scholar] [CrossRef]
- Harwood, A.R.G. L-DART App [Internet]. Research IT, University of Manchester. 2021. Available online: https://play.google.com/store/apps/details?id=uk.ac.manchester.ldart&pli=1 (accessed on 11 November 2023).
- www.RE-AIM.org. 2023. Available online: www.re-aim.org (accessed on 1 December 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant number | Sleep Problem Phenotype | Complaints/Treatment Goals to Change | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sol | Agitation and Psychological Distress in the Night | Sleep Maintenance | Sleep Quality/Refreshingness | Nightmares or Bad Dreams | Physical Sensations or Pain Around Sleep | Short Sleep Duration | Excessive Sleep Duration | Inappropriate Sleep Timing | Daytime Alertness | ||
| 1 | Insomnia | x | x | x | |||||||
| 2 | Poor sleep hygiene/pain | x | x | x | x | ||||||
| 3 | Insomnia/poor sleep hygiene/poor sleep environment | x | x | x | |||||||
| 4 | Excessive caffeine/OSA (on CPAP) | x | x | x | |||||||
| 5 | Non-24 h sleep phase disorder | x | x | x | x | ||||||
| 6 | Irregular/reversed sleep timing | x | x | x | x | ||||||
| 7 | Hypersomnia | x | x | x | |||||||
| 8 | Insomnia | x | x | x | |||||||
| 9 | Paradoxical insomnia/daytime inactivity | x | x | x | |||||||
| 10 | Poor sleep hygiene/poor sleep environment/pain | x | x | x | x | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faulkner, S.; Didikoglu, A.; Byrne, R.; Drake, R.; Bee, P. Light–Dark and Activity Rhythm Therapy (L-DART) to Improve Sleep in People with Schizophrenia Spectrum Disorders: A Single-Group Mixed Methods Study of Feasibility, Acceptability and Adherence. Clocks & Sleep 2023, 5, 734-754. https://doi.org/10.3390/clockssleep5040048
Faulkner S, Didikoglu A, Byrne R, Drake R, Bee P. Light–Dark and Activity Rhythm Therapy (L-DART) to Improve Sleep in People with Schizophrenia Spectrum Disorders: A Single-Group Mixed Methods Study of Feasibility, Acceptability and Adherence. Clocks & Sleep. 2023; 5(4):734-754. https://doi.org/10.3390/clockssleep5040048
Chicago/Turabian StyleFaulkner, Sophie, Altug Didikoglu, Rory Byrne, Richard Drake, and Penny Bee. 2023. "Light–Dark and Activity Rhythm Therapy (L-DART) to Improve Sleep in People with Schizophrenia Spectrum Disorders: A Single-Group Mixed Methods Study of Feasibility, Acceptability and Adherence" Clocks & Sleep 5, no. 4: 734-754. https://doi.org/10.3390/clockssleep5040048