
Disruption of Circadian Sleep/Wake Rhythms in Infants May Herald Future Development of Autism Spectrum Disorder
 , and
, and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Questionnaire Items
4.3. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASD | autism spectrum disorder |
| K-ASD | Kagoshima-Development Support Center for Children-ASD |
| H-ASD | Hyougo-Children’s Sleep and Development Medical Research Center-ASD |
| NBSD | nighttime basic sleep duration |
References
- Maenner, M.J.; Shaw, K.A.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Esler, A.; Furnier, S.M.; Hallas, L.; Hall-Lande, J.; Hudson, A.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2018. MMWR Surveill. Summ. 2021, 70, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Estes, A.; Zwaigenbaum, L.; Gu, H.; St John, T.; Paterson, S.; Elison, J.T.; Hazlett, H.; Botteron, K.; Dager, S.R.; Schultz, R.T.; et al. Behavioral, cognitive, and adaptive development in infants with autism spectrum disorder in the first 2 years of life. J. Neurodev. Disord. 2015, 7, 24. [Google Scholar] [CrossRef] [PubMed]
- Iverson, J.M.; Shic, F.; Wall, C.A.; Chawarska, K.; Curtin, S.; Estes, A.; Gardner, J.M.; Hutman, T.; Landa, R.J.; Levin, A.R.; et al. Early motor abilities in infants at heightened versus low risk for ASD: A Baby Siblings Research Consortium (BSRC) study. J. Abnorm. Psychol. 2019, 128, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Ornitz, E.M.; Yanagisita, M.; Koshino, Y. Infantile Autism. Shonika 1983, 24, 1581–1591. (In Japanese) [Google Scholar]
- Richdale, A.L.; Schreck, K.A. Sleep problems in autism spectrum disorders: Prevalence, nature, & possible biopsychosocial aetiologies. Sleep Med. Rev. 2009, 13, 403–411. [Google Scholar]
- Yavuz-Kodat, E.; Reynaud, E.; Geoffray, M.M.; Limousin, N.; Patricia Franco, P.; Bonnet-Brilhault, F.; Bourgin, P.; Schroder, C.M. Disturbances of Continuous Sleep and Circadian Rhythms Account for Behavioral Difficulties in Children with Autism Spectrum Disorder. J. Clin. Med. 2020, 9, 1978. [Google Scholar] [CrossRef] [PubMed]
- Cortesi, F.; Giannotti, F.; Ivanenko, A.; Johnson, K. Sleep in children with autistic spectrum disorder. Sleep Med. 2010, 11, 659–664. [Google Scholar] [CrossRef]
- Pinato, L.; Galina Spilla, C.S.; Markus, R.P.; da Silveira Cruz-Machado, S. Dysregulationof Circadian Rhythms in Autism Spectrum Disorders. Curr. Pharm. Des. 2019, 25, 4379–4393. [Google Scholar] [CrossRef]
- Wu, Z.Y.; Huang, S.D.; Zou, J.J.; Wang, Q.-X.; Naveed, M.; Bao, H.-N.; Wei Wang, W.; Fukunaga, K.; Han, F. Autism spectrum disorder (ASD): Disturbance of the melatonin system and its implications. Biomed. Pharmacother. 2020, 130, 110496. [Google Scholar] [CrossRef]
- Wimpory, D.; Nicholas, B.; Nash, J. Social timing, clock genes and autism: A new hypothesis. Intellect. Disabil. Res. 2002, 46, 352–358. [Google Scholar] [CrossRef]
- Horiuchi, F.; Kawabe, K.; Oka, Y.; Nakachi, K.; Hosokawa, R.; Ueno, S. The Association between Autistic Traits and Sleep Habits/Problems in Toddlers. Dev. Neuropsychol. 2020, 45, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Massoni, L.; Battaglini, S.; Cremone, I.M.; Carmassi, C.; Carpita, B. Biological correlates of altered circadian rhythms, autonomic functions and sleep problems in autism spectrum disorder. Ann. Gen. Psychiatry 2022, 21, 13. [Google Scholar] [CrossRef] [PubMed]
- Quian, J.; Scheer, F.A.J.L. Circadian System and Glucose Metabolism: Implications for Physiology and Disease. Trends. Endocrinol. Metab. 2016, 27, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Tarokh, L.; Saletin, J.M.; Carskadon, M.A. Sleep in adolescence: Physiology, cognition and mental health. Neurosci. Biobehav. Rev. 2016, 7, 182–188. [Google Scholar] [CrossRef]
- Tordjman, S.; Davlantis, K.S.; Georgieff, N.; Geoffray, M.M.; Speranza, M.; Anderson, G.M.; Xavier, J.; Botbol, M.; Oriol, C.; Bellissant, E.; et al. Autism as a disorder of biological and behavioral rhythms: Toward new therapeutic perspectives. Front. Pediatr. 2015, 3, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Geoffray, M.M.; Nicolas, A.; Speranza, M.; Georgieff, N. Are circadian rhythms new. pathways to understand Autism Spectrum Disorder? Physiol. Parisb. 2016, 110 Pt B, 434–438. [Google Scholar] [CrossRef]
- MacDuffie, K.E.; Shen, M.D.; Dager, S.R.; Styner, M.A.; Kim, S.H.; Paterson, S.; Pandey, J.; St John, T.; Elison, J.T.; Wolff, J.J.; et al. Sleep Onset Problems and Subcortical Development in Infants Later Diagnosed with Autism Spectrum Disorder. Am. J. Psychiatry 2020, 177, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Miike, T.; Toyoura, M.; Tonooka, S.; Konishi, Y.; Oniki, K.; Saruwatari, J.; Tajima, S.; Kinoshita, J.; Nakai, A.; Kikuchi, K. Neonatal Irritable Sleep-Wake Rhythm as a Predictor of Autism Spectrum Disorders. Neurobiol. Sleep. Circ. Rhythm. 2020, 9, 100053. [Google Scholar] [CrossRef]
- Lorsung, E.; Karthikeyan, R.; Cao, R. Biological Timing and Neurodevelopmental Disorders: A Role for Circadian Dysfunction in Autism Spectrum Disorders. Front. Neurosci. 2021, 15, 642745. [Google Scholar] [CrossRef]
- Verhoeff, M.E.; Blanken, M.L.E.; Kocevska, D.; Mileva-Seitz, V.R.; Jaddoe, V.W.V.; White, T.; Verhulst, F.; Luijk, M.P.C.M.; Tiemeier, H. The bidirectional association. between sleep problems and autism spectrum disorder: A population-based cohort study. Mol. Autism. 2018, 9, 8. [Google Scholar] [CrossRef]
- Jan, J.E.; Reiter, R.J.; Bax, M.C.; Ribary, U.; Freeman, R.D.; Wasdell, M.B. Long-term sleep. disturbances in children: A cause of neuronal loss. Eur. J. Paediatr. Neurol. 2010, 14, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Licis, A. Sleep-Wake Disorders in Childhood. Continuum 2020, 26, 1034–1069. [Google Scholar] [CrossRef] [PubMed]
- Ophoff, D.; Slaats, M.A.; Boudewyns, A.; Glazemakers, I.; Van Hoorenbeeck, K.; Verhulst, S.L. Sleep disorders during childhood: A practical review. Eur. J. Pediatr. 2018, 177, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Erren, T.C.; Reiter, R.J. Defining Chronodisruption. J. Pineal. Res. 2009, 46, 245–247. [Google Scholar] [CrossRef]
- Touitou, Y.; Reinberg, A.; Touitou, D. Association between light at night, melatonin secretion, sleep deprivation, and the internal clock: Health impacts and mechanisms of circadian disruption. Life Sci. 2017, 173, 94–106. [Google Scholar] [CrossRef] [PubMed]
- Pinilla, T.; Birch, L.L. Help me make it through the night: Behavioral entrainment of breast-fed infants’ sleep patterns. Pediatrics 1993, 91, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Henderson, J.M.T.; France, K.G.; Blampied, N.M. The consolidation of infants’ nocturnal sleep across the first year of life. Sleep Med. Rev. 2011, 15, 211–220. [Google Scholar] [CrossRef]
- Paul, I.M.; Savage, J.S.; Anzman-Frasca, S.; Marini, M.E.; Mindell, J.A.; Birch, L.L. INSIGHT Responsive Parenting Intervention and Infant Sleep. Pediatrics 2016, 138, e20160762. [Google Scholar] [CrossRef]
- Mohr, C.; Gross-Hemmi, M.H.; Meyer, A.H. Temporal Patterns of Infant Regulatory Behaviors in Relation to Maternal Mood and Soothing Strategies. Child Psychiatry Hum. Dev. 2019, 50, 566–579. [Google Scholar] [CrossRef]
- Sadeh, A.; Juda-Hanael, M.; Livne-Karp, E.; Kahn, M.; Tikotzky, L.; Anders, T.F.; Calkins, S.; Sivan, Y. Low parental tolerance for infant crying: An underlying factor in infant sleep problems? J. Sleep Res. 2016, 25, 501–507. [Google Scholar] [CrossRef]
- Touchette, E.; Dionne, G.; Forget-Dubois, N.; Petit, D.; Pérusse, D.; Falissard, B.; Tremblay, R.E.; Boivin, M.; Montplaisir, J.Y. Genetic and environmental influences on daytime and nighttime sleep duration in early childhood. Pediatrics 2013, 131, e1874–e1880. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, J.S.; Gringras, P.; Blair, P.S.; Scott, N.; Henderson, J.; Fleming, P.J.; Emond, A.M. Sleep patterns in children with autistic spectrum disorders: A prospective cohort study. Arch. Dis. Child. 2014, 99, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Halal, C.S.; Bassani, D.G.; Santos, I.S.; Tovo-Rodrigues, L.; Del-Ponte, B.; Silveira, M.F.; Bertoldi, A.D.; Barros, F.C.; Nunes, M.L. Maternal perinatal depression and infant sleep problems at 1 year of age: Subjective and actigraphy data from a population-based birth cohort study. J. Sleep Res. 2021, 30, e13047. [Google Scholar] [CrossRef]
- Satterstrom, F.K.; Kosmicki, J.A.; Wang, J.; Breen, M.S.; De Rubeis, S.; An, J.-Y.; Peng, M.; Collins, R.; Grove, J.; Klei, L.; et al. Large-Scale Exome Sequencing Study Implicates Both Developmental and Functional Changes in the Neurobiology of Autism. Cell 2020, 180, 568–584.e23. [Google Scholar] [CrossRef] [PubMed]
- Hoang, N.; Yuen, R.K.C.; Howe, J.; Drmic, I.; Ambrozewicz, P.; Russell, C.; Vorstman, J.; Weiss, S.K.; Anagnostou, E.; Malow, B.A.; et al. Sleep phenotype of individuals with autism spectrum disorder bearing mutations in the PER2 circadian rhythm gene. Am. J. Med. Genet. 2021, 185, 1120–1130. [Google Scholar] [CrossRef] [PubMed]
- Mirmiran, M.; Maas, Y.G.; Ariagno, R. Development of fetal and neonatal sleep and circadian rhythms. Sleep. Med. Rev. 2003, 7, 321–334. [Google Scholar] [CrossRef] [PubMed]
- Serón-Ferré, M.; Mendez, N.; Abarzua-Catalan, L.; Vilches, N.; Valenzuela, F.J. Circadian rhythms in the fetus. Mol. Cell. Endocrinol. 2012, 349, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, K.; Michikawa, T.; Morokuma, S.; Hamada, N.; Ogawa, M.; Kato, K.; Sanefuji, M.; Shibata, E.; Tsuji, M.; Shimono, M.; et al. Association of physical activity and sleep habits during pregnancy with autistic spectrum disorder in 3-year-old infants. Commun. Med. 2022, 5, 35. [Google Scholar] [CrossRef]
- Meier-Koll, A.; Hall, U.; Hellwig, U.; Kott, G.; Meier-Koll, V. A biological oscillator system and the development of sleep-waking behavior during early infancy. Chronobiologia 1978, 5, 425–440. [Google Scholar]
- Bruni, O.; Baumgartner, E.; Sette, S.; Ancona, M.; Caso, G.; Di Cosimo, M.E.; Mannini, A.; Ometto, M.; Pasquini, A.; Ulliana, A.; et al. Longitudinal study of sleep behavior in. normal infants during the first year of life. J. Clin. Sleep. Med. 2014, 10, 1119–1127. [Google Scholar] [CrossRef]
- Benhamou, I. Sleep disorders of early childhood: A review. Isr. J. Psychiatry Relat. Sci. 2000, 37, 190–196. [Google Scholar]
- Sadeh, A.; Tikotzky, L.; Scher, A. Parenting and infant sleep. Sleep. Med. Rev. 2010, 14, 89–96. [Google Scholar] [CrossRef]
- Hiscock, H.; Cook, F.; Bayer, J.; Le, H.N.D.; Mensah, F.; Cann, W.; Symon, B.; St James-Roberts, I. Preventing early infant sleep and crying problems and postnatal depression: A randomized trial. Pediatrics 2014, 133, e346–e354. [Google Scholar] [CrossRef]
- Dönmez, R.Ö.; Temel, A.B. Effect of soothing techniques on infants’ self-regulation behaviors (sleeping, crying, feeding): A randomized controlled study. Jpn. J. Nurs. Sci. 2019, 50, 407–419. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 27, 2191–2194. [Google Scholar]



{kind=link}
{kind=link}
| Control | K-ASD | H-ASD | ||||
|---|---|---|---|---|---|---|
| Age (Years Old) | Male | Female | Male | Female | Male | Female |
| 2 | 20 (52.6%) | 18 (47.4%) | 3 (100.0%) | 0 (0.0%) | 3 (100%) | 0 (0.0%) |
| 3 | 20 (47.6%) | 22 (52.4%) | 14 (82.4%) | 3 (17.6%) | 4 (66.7%) | 2 (33.3%) |
| 4 | 17 (50.0%) | 17 (50.0%) | 24 (75.0%) | 8 (25.0%) | 16 (84.2%) | 3 (15.8%) |
| 5 | 13 (59.1%) | 9 (40.9%) | 30 (73.2%) | 11 (26.8%) | 5 (50.0%) | 5 (50.0%) |
| 6 | 5 (55.6%) | 4 (44.4%) | 17 (85.0%) | 3 (15.0%) | 7 (77.8%) | 2 (22.2%) |
| Total | 75 (51.7) | 70 (48.3) | 88 (77.8%) | 25 (22.1%) | 35 (74.5%) | 12 (25.5%) |
| Overall total | 145 | 113 | 47 | |||
| Weekdays | Weekends | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | K-ASD | OR (95% CI) | p | Control | K-ASD | OR (95% CI) | p | ||
| Infancy | Infancy | ||||||||
| before 21:00 | 105 | 57 | 1 | before 21:00 | 94 | 56 | 1 | ||
| 21:00 to 22:00 | 39 | 35 | 1.86 (1.04–3.36) | 0.037 | 21:00 to 22:00 | 47 | 35 | 1.41 (0.79–2.49) | 0.241 |
| after 22:00 | 1 | 21 | 36.87 (4.74–286.59) | <0.001 | after 22:00 | 4 | 22 | 9.17 (2.92–28.81) | <0.001 |
| 1–3 years of age | 1–3 years of age | ||||||||
| before 21:00 | 74 | 44 | 1 | before 21:00 | 66 | 42 | 1 | ||
| 21:00 to 22:00 | 62 | 51 | 1.42 (0.82–2.45) | 0.211 | 21:00 to 22:00 | 68 | 51 | 1.17 (0.67–2.03) | 0.579 |
| after 22:00 | 6 | 18 | 5.90 (2.08–16.76) | <0.001 | after 22:00 | 9 | 19 | 3.78 (1.50–9.54) | 0.005 |
| 3–5 years of age | 3–5 years of age | ||||||||
| before 21:00 | 41 | 40 | 1 | before 21:00 | 35 | 36 | 1 | ||
| 21:00 to 22:00 | 43 | 55 | 1.31 (0.71–2.42) | 0.396 | 21:00 to 22:00 | 47 | 53 | 1.15 (0.61–2.19) | 0.658 |
| after 22:00 | 5 | 11 | 2.28 (0.69–7.52) | 0.175 | after 22:00 | 8 | 17 | 2.04 (0.75–5.54) | 0.165 |
| Weekdays | Weekends | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | H-ASD | OR (95% CI) | p | Control | H-ASD | OR (95% CI) | p | ||
| Infancy | Infancy | ||||||||
| before 21:00 | 105 | 24 | 1 | before 21:00 | 94 | 21 | 1 | ||
| 21:00 to 22:00 | 39 | 7 | 0.92 (0.36–2.37) | 0.867 | 21:00 to 22:00 | 47 | 10 | 1.13 (0.48–2.65) | 0.788 |
| after 22:00 | 1 | 16 | 86.75 (10.40–723.59) | <0.001 | after 22:00 | 4 | 16 | 22.88 (6.43–81.51) | <0.001 |
| 1–3 years of age | 1–3 years of age | ||||||||
| before 21:00 | 74 | 18 | 1 | before 21:00 | 66 | 16 | 1 | ||
| 21:00 to 22:00 | 62 | 13 | 0.84 (0.37–1.89) | 0.672 | 21:00 to 22:00 | 68 | 14 | 0.80 (0.35–1.81) | 0.589 |
| after 22:00 | 6 | 16 | 18.52 (5.43–63.20) | <0.001 | after 22:00 | 9 | 16 | 12.60 (4.00–39.70) | <0.001 |
| 3-5 years of age | 3–5 years of age | ||||||||
| before 21:00 | 41 | 21 | 1 | before 21:00 | 35 | 16 | 1 | ||
| 21:00 to 22:00 | 43 | 13 | 0.57 (0.25–1.33) | 0.193 | 21:00 to 22:00 | 47 | 18 | 0.82 (0.36–1.88) | 0.639 |
| after 22:00 | 5 | 8 | 5.53 (1.40–21.85) | 0.015 | after 22:00 | 8 | 8 | 3.55 (1.01–12.50) | 0.049 |
| Weekdays | Weekends | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | K-ASD | OR (95% CI) | p | Control | K-ASD | OR (95% CI) | p | ||
| Infancy | Infancy | ||||||||
| before 07:00 | 91 | 40 | 1 | before 07:00 | 73 | 36 | 1 | ||
| 07:00 to 08:00 | 51 | 46 | 2.16 (1.22–3.84) | 0.008 | 07:00 to 08:00 | 65 | 49 | 1.78 (1.00–3.15) | 0.049 |
| after 08:00 | 3 | 27 | 27.19 (7.37–100.35) | <0.001 | after 08:00 | 6 | 28 | 10.84 (3.95–29.75) | <0.001 |
| 1–3 years of age | 1–3 years of age | ||||||||
| before 07:00 | 114 | 52 | 1 | before 07:00 | 75 | 41 | 1 | ||
| 07:00 to 08:00 | 28 | 42 | 3.88 (2.08–7.25) | <0.001 | 07:00 to 08:00 | 63 | 45 | 1.49 (0.85–2.63) | 0.168 |
| after 08:00 | 2 | 19 | 26.62 (5.66–125.13) | <0.001 | after 08:00 | 6 | 25 | 9.67 (3.47–26.97) | <0.001 |
| 3–5 years of age | 3–5 years of age | ||||||||
| before 07:00 | 69 | 69 | 1 | before 07:00 | 43 | 48 | 1 | ||
| 07:00 to 08:00 | 20 | 30 | 1.66 (0.83–3.32) | 0.155 | 07:00 to 08:00 | 43 | 44 | 0.97 (0.53–1.80) | 0.931 |
| after 08:00 | 1 | 5 | 4.38 (0.47–40.83) | 0.195 | after 08:00 | 4 | 12 | 2.62 (0.75–9.14) | 0.132 |
| Weekdays | Weekends | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | H-ASD | OR (95% CI) | p | Control | H-ASD | OR (95% CI) | p | ||
| Infancy | Infancy | ||||||||
| before 07:00 | 91 | 20 | 1 | before 07:00 | 73 | 16 | 1 | ||
| 07:00 to 08:00 | 51 | 13 | 1.20 (0.54–2.68) | 0.649 | 07:00 to 08:00 | 65 | 16 | 1.25 (0.57–2.76) | 0.575 |
| after 08:00 | 3 | 14 | 30.80 (7.28–130.26) | <0.001 | after 08:00 | 6 | 15 | 13.27(4.24–41.61) | <0.001 |
| 1–3 years of age | 1–3 years of age | ||||||||
| before 07:00 | 114 | 21 | 1 | before 07:00 | 75 | 16 | 1 | ||
| 07:00 to 08:00 | 28 | 14 | 2.91 (1.28–6.63) | 0.011 | 07:00 to 08:00 | 63 | 16 | 1.27 (0.58–2.81) | 0.549 |
| after 08:00 | 2 | 11 | 37.43 (7.17–195.51) | <0.001 | after 08:00 | 6 | 14 | 14.74 (4.48–48.47) | <0.001 |
| 3–5 years of age | 3–5 years of age | ||||||||
| before 07:00 | 69 | 29 | 1 | before 07:00 | 43 | 19 | 1 | ||
| 07:00 to 08:00 | 20 | 11 | 1.35 (0.56–3.28) | 0.504 | 07:00 to 08:00 | 43 | 15 | 0.79 (0.35–1.79) | 0.571 |
| after 08:00 | 1 | 2 | 10.59 (0.85–131.34) | 0.066 | after 08:00 | 4 | 5 | 3.13 (0.71–13.74) | 0.130 |
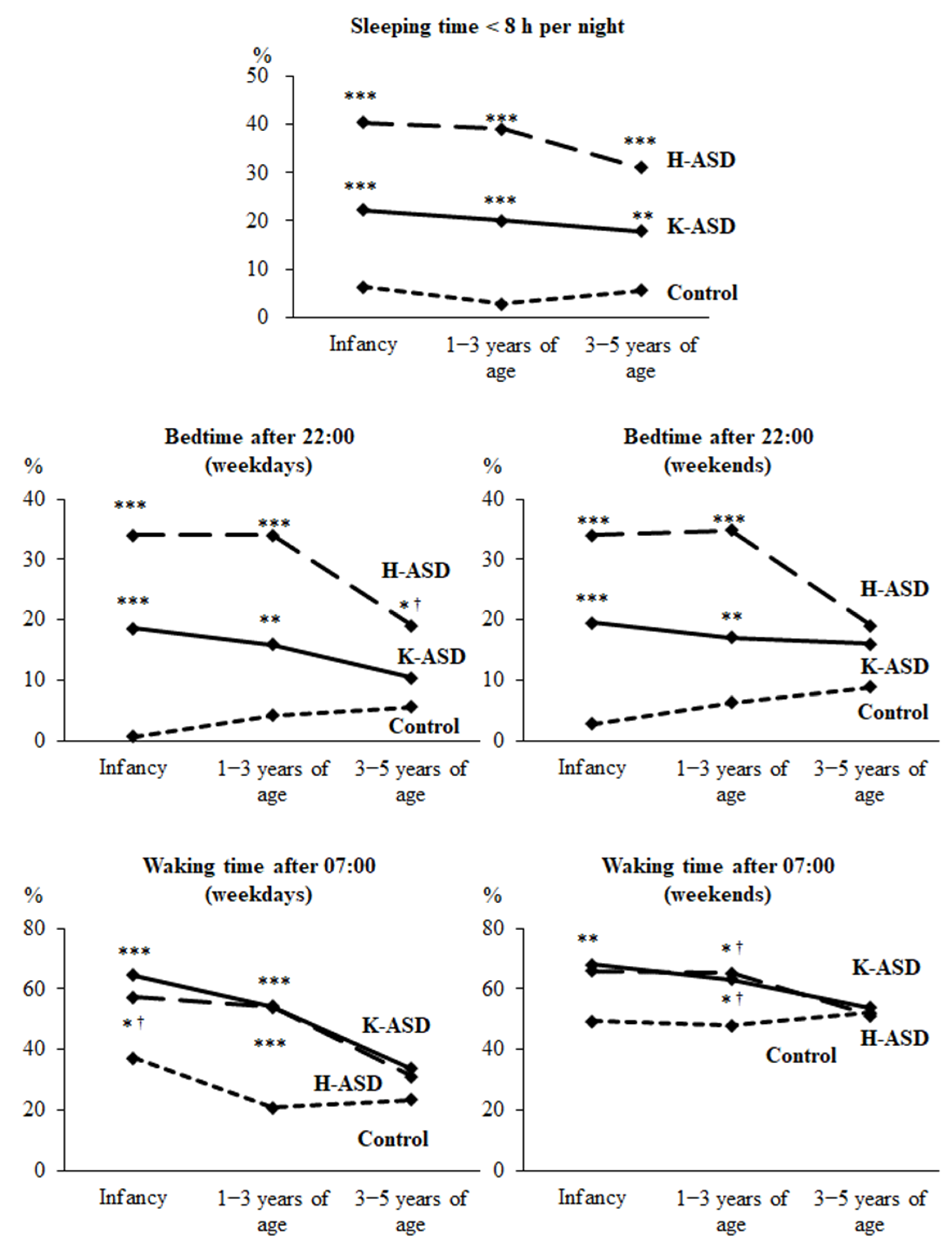
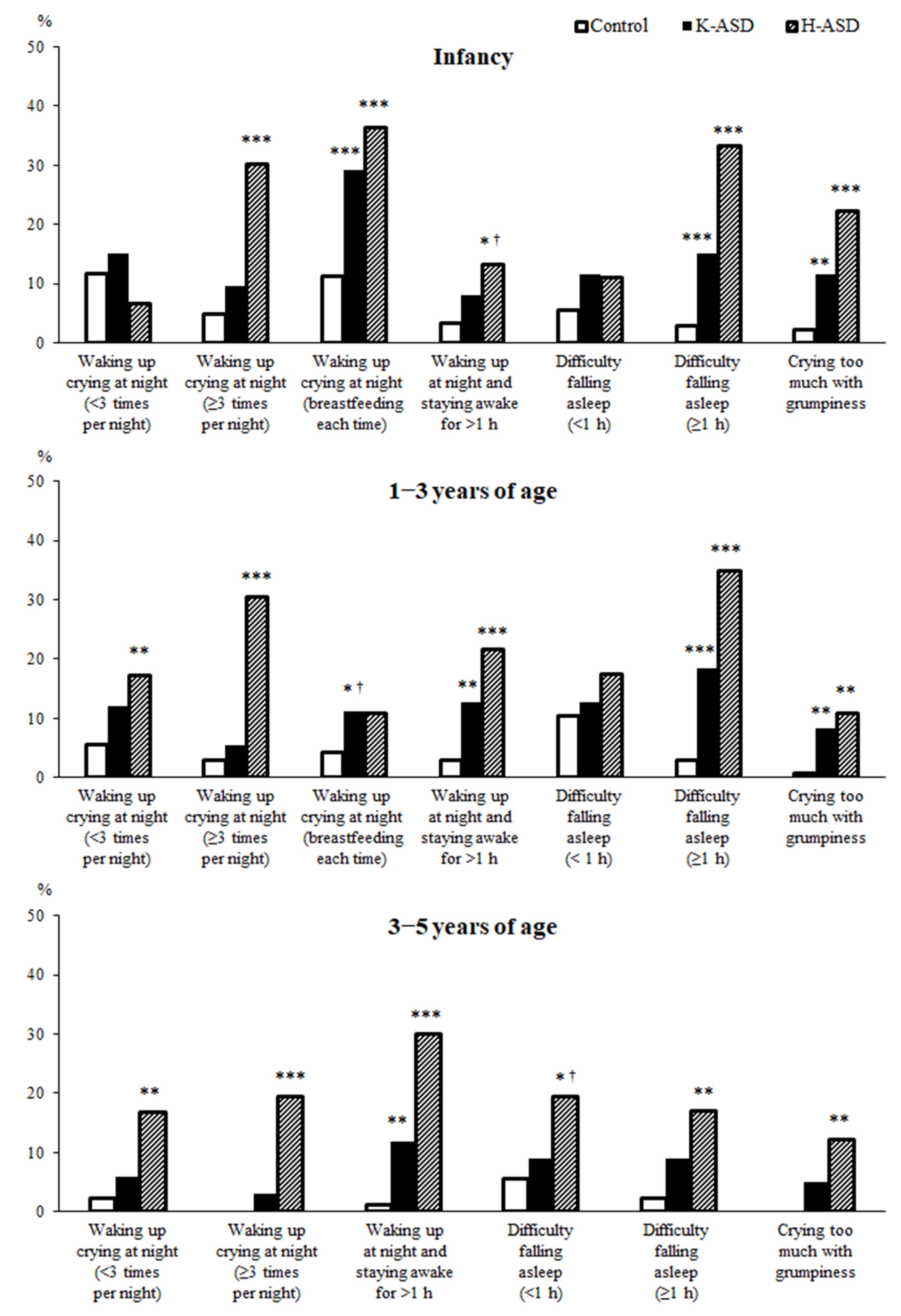
| Short Sleep (<8 h) | Sleep Onset Time after 22:00, Weekdays | Wake-up Time after 7:00, Weekdays | Waking up Crying at Night (Breast Feeding Each Time) | Waking Up Crying at Night (<3 Times per Night) | Waking up Crying at Night (≥3 Times per Night) | Waking up at Night and Staying Awake for >1 h | Difficulty Falling Asleep (>1 h) | Crying too Much with Grumpiness | |
|---|---|---|---|---|---|---|---|---|---|
| Infancy | |||||||||
| K-ASD | *** | *** | *** | *** | *** | ** | |||
| H-ASD | *** | *** | *** | *** | *** | *** | |||
| 1–3 years | |||||||||
| K-ASD | *** | ** | *** | ** | *** | ** | |||
| H-ASD | *** | *** | *** | ** | *** | *** | *** | ** | |
| 3–5 years | |||||||||
| K-ASD | ** | *** | |||||||
| H-ASD | *** | ** | *** | *** | ** | ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miike, T.; Oniki, K.; Toyoura, M.; Tonooka, S.; Tajima, S.; Kinoshita, J.; Saruwatari, J.; Konishi, Y. Disruption of Circadian Sleep/Wake Rhythms in Infants May Herald Future Development of Autism Spectrum Disorder. Clocks & Sleep 2024, 6, 170-182. https://doi.org/10.3390/clockssleep6010012
Miike T, Oniki K, Toyoura M, Tonooka S, Tajima S, Kinoshita J, Saruwatari J, Konishi Y. Disruption of Circadian Sleep/Wake Rhythms in Infants May Herald Future Development of Autism Spectrum Disorder. Clocks & Sleep. 2024; 6(1):170-182. https://doi.org/10.3390/clockssleep6010012
Chicago/Turabian StyleMiike, Teruhisa, Kentaro Oniki, Makiko Toyoura, Shiro Tonooka, Seiki Tajima, Jun Kinoshita, Junji Saruwatari, and Yukuo Konishi. 2024. "Disruption of Circadian Sleep/Wake Rhythms in Infants May Herald Future Development of Autism Spectrum Disorder" Clocks & Sleep 6, no. 1: 170-182. https://doi.org/10.3390/clockssleep6010012