
The Impact of Cardiac Devices on Patients’ Quality of Life—A Systematic Review and Meta-Analysis

 , , , , and
, , , , and 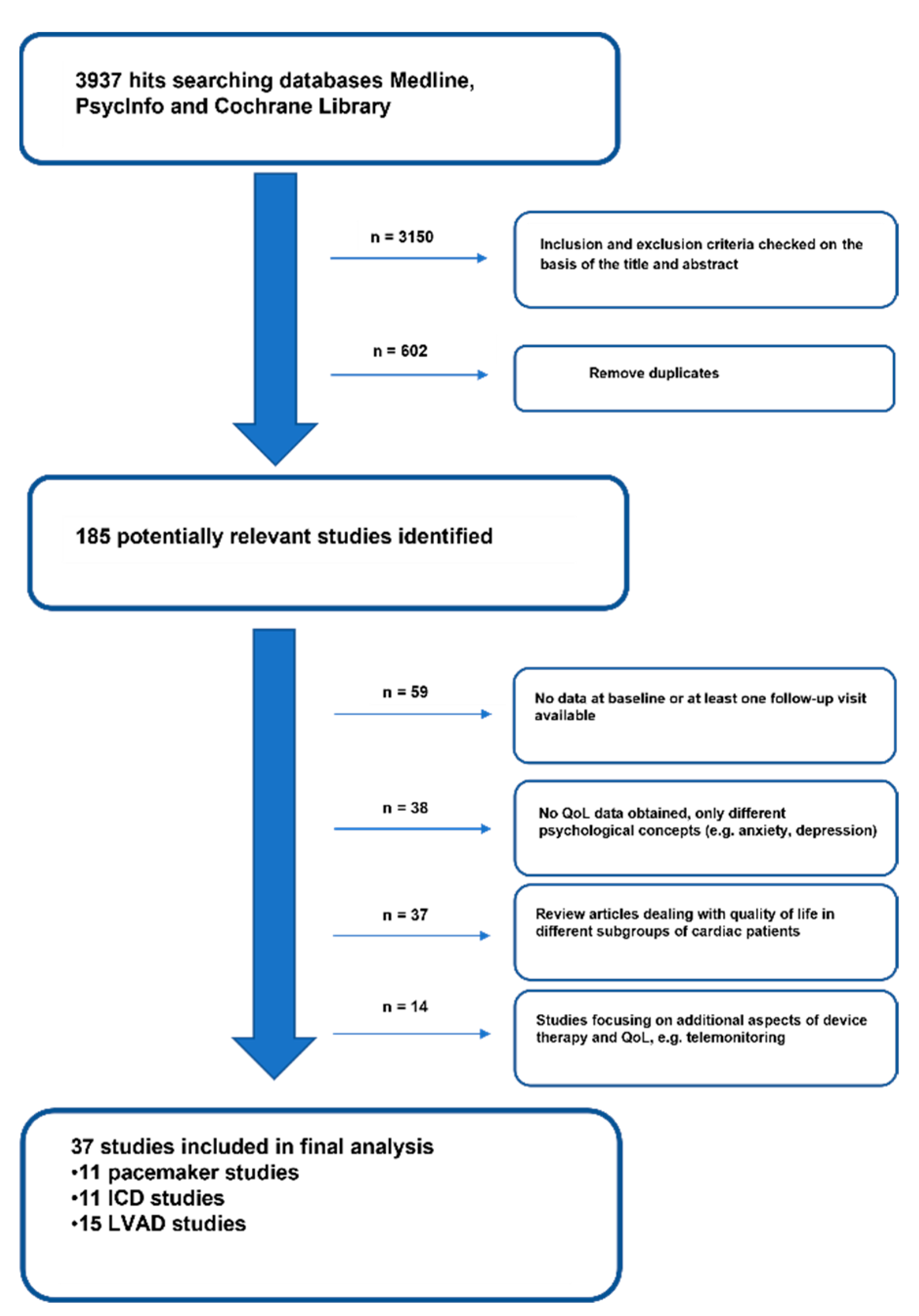{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Selection of Studies
2.2. Quality Assessment
2.3. Coding of Treatment Characteristics
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Breitenstein, A.; Steffel, J. Devices in Heart Failure Patients-Who Benefits from ICD and CRT? Front. Cardiovasc. Med. 2019, 6, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussein, A.A.; Wilkoff, B.L. Cardiac Implantable Electronic Device Therapy in Heart Failure. Circ. Res. 2019, 124, 1584–1597. [Google Scholar] [CrossRef]
- Moss, A.J.; Zareba, W.; Hall, W.J.; Klein, H.; Wilber, D.J.; Cannom, D.S.; Daubert, J.P.; Higgins, S.L.; Brown, M.W.; Andrews, M.L. Multicenter Automatic Defibrillator Implantation Trial III. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N. Engl. J. Med. 2002, 346, 877–883. [Google Scholar] [CrossRef] [Green Version]
- Ranasinghe, I.; Parzynski, C.S.; Freeman, J.V.; Dreyer, R.P.; Ross, J.S.; Akar, J.G.; Krumholz, H.M.; Curtis, J.P. Long-Term Risk for Device-Related Complications and Reoperations After Implantable Cardioverter-Defibrillator Implantation: An Observational Cohort Study. Ann. Intern. Med. 2016, 165, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, N.M.; Grubisic, M.; Andrade, J.G.; Huang, F.; Ding, L.; Gao, M.; Bashir, J. Long-term complications, reoperations and survival following cardioverter-defibrillator implant. Heart 2018, 104, 237–243. [Google Scholar] [CrossRef]
- Magyar-Russell, G.; Thombs, B.D.; Cai, J.X.; Baveja, T.; Kuhl, E.A.; Singh, P.P.; Barroso, M.M.B.; Arthurs, E.; Roseman, M.; Amin, N.; et al. The prevalence of anxiety and depression in adults with implantable cardioverter defibrillators: A systematic review. J. Psychosom. Res. 2011, 71, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Tosto, C.; Adamo, L.; Craddock, H.; Di Blasi, M.; Girgenti, R.; Clemenza, F.; Carney, R.M.; Ewald, G. Relationship between device acceptance and patient-reported outcomes in Left Ventricular Assist Device (LVAD) recipients. Sci. Rep. 2019, 9, 10778. [Google Scholar] [CrossRef] [Green Version]
- Weiss, M.; Michels, G.; Eberhardt, F.; Fehske, W.; Winter, S.; Baer, F.; Choi, Y.H.; Albus, C.; Steven, D.; Baldus, S.; et al. Anxiety, depression and quality of life in acute high risk cardiac disease patients eligible for wearable cardioverter defibrillator: Results from the prospective multicenter CRED-registry. PLoS ONE 2019, 14, e0213261. [Google Scholar] [CrossRef]
- Pyngottu, A.; Werner, H.; Lehmann, P.; Balmer, C. Health-Related Quality of Life and Psychological Adjustment of Children and Adolescents with Pacemakers and Implantable Cardioverter Defibrillators: A Systematic Review. Pediatr. Cardiol. 2019, 40, 1–16. [Google Scholar] [CrossRef]
- Fumagalli, S.; Pieragnoli, P.; Haugaa, K.H.; Potpara, T.S.; Rasero, L.; Ramacciati, N.; Ricciardi, G.; Solimene, F.; Mascia, G.; Mascioli, G.; et al. The influence of age on the psychological profile of patients with cardiac implantable electronic devices: Results from the Italian population in a multicenter study conducted by the European Heart Rhythm Association. Aging Clin. Exp. Res. 2019, 31, 1219–1226. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Olivo, S.A.; Macedo, L.G.; Gadotti, I.C.; Fuentes, J.; Stanton, T.; Magee, D.J. Scales to assess the quality of randomized controlled trials: A systematic review. Phys. Ther. 2008, 88, 156–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morina, N.; Hoppen, T.H.; Kip, A. Study quality and efficacy of psychological interventions for posttraumatic stress disorder: A meta-analysis of randomized controlled trials. Psychol. Med. 2021, 51, 1260–1270. [Google Scholar] [CrossRef]
- Lipsey, M.W.; Wilson, D.B. Practical Meta-Analysis; Sage: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons, Ltd.: Chichester, UK, 2009. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum: New Jersey, NJ, USA, 1988. [Google Scholar]
- Hunter, J.E.; Schmidt, F.L. Methods of Meta-Analysis: Correcting Error and Bias in Research Findings; Sage: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Pearson: Boston, MA, USA, 2013. [Google Scholar]
- Baron-Esquivias, G.; Moya-Mitjans, A.; Martinez-Alday, J.; Ruiz-Granell, R.; Lacunza-Ruiz, J.; Garcia-Civera, R.; Gutierrez-Carretero, E.; Romero-Garrido, R.; Morillo, C.A. Impact of dual-chamber pacing with closed loop stimulation on quality of life in patients with recurrent reflex vasovagal syncope: Results of the SPAIN study. Europace 2020, 22, 314–319. [Google Scholar] [CrossRef]
- Cabanas-Grandio, P.; Garcia Campo, E.; Bisbal, F.; Garcia-Seara, J.; Pachon, M.; Juan-Salvadores, P.; Paredes, E.; Molinero, A.; Martinez-Sande, J.L.; Arias, M.A.; et al. Quality of life of patients undergoing conventional vs leadless pacemaker implantation: A multicenter observational study. J. Cardiovasc. Electrophysiol. 2020, 31, 330–336. [Google Scholar] [CrossRef]
- Fleischmann, K.E.; Orav, E.J.; Lamas, G.A.; Mangione, C.M.; Schron, E.; Lee, K.L.; Goldman, L. Pacemaker implantation and quality of life in the Mode Selection Trial (MOST). Heart Rhythm. 2006, 3, 653–659. [Google Scholar] [CrossRef] [Green Version]
- Gadler, F.; Linde, C.; Daubert, C.; McKenna, W.; Meisel, E.; Aliot, E.; Chojnowska, L.; Guize, L.; Gras, D.; Jeanrenaud, X.; et al. Significant improvement of quality of life following atrioventricular synchronous pacing in patients with hypertrophic obstructive cardiomyopathy. Data from 1 year of follow-up. PIC study group. Pacing in Cardiomyopathy. Eur. Heart J. 1999, 20, 1044–1050. [Google Scholar] [CrossRef]
- Hofer, S.; Anelli-Monti, M.; Berger, T.; Hintringer, F.; Oldridge, N.; Benzer, W. Psychometric properties of an established heart disease specific health-related quality of life questionnaire for pacemaker patients. Qual. Life Res. 2005, 14, 1937–1942. [Google Scholar] [CrossRef] [PubMed]
- Lamas, G.A.; Orav, E.J.; Stambler, B.S.; Ellenbogen, K.A.; Sgarbossa, E.B.; Huang, S.K.; Marinchak, R.A.; Estes, N.A., 3rd; Mitchell, G.F.; Lieberman, E.H.; et al. Quality of life and clinical outcomes in elderly patients treated with ventricular pacing as compared with dual-chamber pacing. N. Engl. J. Med. 1998, 338, 1097–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mlynarska, A.; Mlynarski, R.; Golba, K.S. Influence of frailty on the quality of life patients qualified for pacemaker implantation. J. Clin. Nurs. 2018, 27, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Newman, D.; Lau, C.; Tang, A.S.; Irvine, J.; Paquette, M.; Woodend, K.; Dorian, P.; Gent, M.; Kerr, C.; Connolly, S.J. Effect of pacing mode on health-related quality of life in the Canadian Trial of Physiologic Pacing. Am. Heart J. 2003, 145, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Su, S.F.; Wu, M.S. Arrhythmia Perception and Quality of Life in Bradyarrhythmia Patients Following Permanent Pacemaker Implantation. Clin. Nurs. Res. 2021, 30, 183–192. [Google Scholar] [CrossRef]
- Udo, E.O.; van Hemel, N.M.; Zuithoff, N.P.; Nijboer, H.; Taks, W.; Doevendans, P.A.; Moons, K.G. Long term quality-of-life in patients with bradycardia pacemaker implantation. Int. J. Cardiol. 2013, 168, 2159–2163. [Google Scholar] [CrossRef] [Green Version]
- van Hemel, N.M.; Holwerda, K.J.; Slegers, P.C.; Spierenburg, H.A.; Timmermans, A.A.; Meeder, J.G.; van der Kemp, P.; Kelder, J.C.; Stofmeel, M.A. Sensor and Quality of Life I. The contribution of rate adaptive pacing with single or dual sensors to health-related quality of life. Europace 2007, 9, 233–238. [Google Scholar] [CrossRef]
- Bundgaard, J.S.; Thune, J.J.; Nielsen, J.C.; Videbaek, R.; Haarbo, J.; Bruun, N.E.; Videbaek, L.; Aagaard, D.; Korup, E.; Jensen, G.; et al. The impact of implantable cardioverter-defibrillator implantation on health-related quality of life in the DANISH trial. Europace 2019, 21, 900–908. [Google Scholar] [CrossRef]
- Carroll, D.L.; Hamilton, G.A. Long-term effects of implanted cardioverter-defibrillators on health status, quality of life, and psychological state. Am. J. Crit. Care 2008, 17, 222–230. [Google Scholar] [CrossRef]
- Gopinathannair, R.; Lerew, D.R.; Cross, N.J.; Sears, S.F.; Brown, S.; Olshansky, B. Longitudinal changes in quality of life following ICD implant and the impact of age, gender, and ICD shocks: Observations from the INTRINSIC RV trial. J. Interv. Card Electrophysiol. 2017, 48, 291–298. [Google Scholar] [CrossRef]
- Lauck, S.B.; Sawatzky, R.; Johnson, J.L.; Humphries, K.; Bennett, M.T.; Chakrabarti, S.; Kerr, C.R.; Tung, S.; Yeung-Lai-Wah, J.A.; Ratner, P.A. Sex is associated with differences in individual trajectories of change in social health after implantable cardioverter-defibrillator. Circ. Cardiovasc. Qual. Outcomes 2015, 8, S21–S30. [Google Scholar] [CrossRef] [Green Version]
- Mark, D.B.; Anstrom, K.J.; Sun, J.L.; Clapp-Channing, N.E.; Tsiatis, A.A.; Davidson-Ray, L.; Lee, K.L.; Bardy, G.H. Sudden Cardiac Death in Heart Failure Trial I. Quality of life with defibrillator therapy or amiodarone in heart failure. N. Engl. J. Med. 2008, 359, 999–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passman, R.; Subacius, H.; Ruo, B.; Schaechter, A.; Howard, A.; Sears, S.F.; Kadish, A. Implantable cardioverter defibrillators and quality of life: Results from the defibrillators in nonischemic cardiomyopathy treatment evaluation study. Arch. Intern. Med. 2007, 167, 2226–2232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, S.S.; Theuns, D.A.; Muskens-Heemskerk, A.; Erdman, R.A.; Jordaens, L. Type-D personality but not implantable cardioverter-defibrillator indication is associated with impaired health-related quality of life 3 months post-implantation. Europace 2007, 9, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, D.; Gallagher, R.; Mitten-Lewis, S.; McKinley, S.; Squire, J. Australian implantable cardiac defibrillator recipients: Quality-of-life issues. Int. J. Nurs. Pract. 2002, 8, 68–74. [Google Scholar]
- Sears, S.F.; Lewis, T.S.; Kuhl, E.A.; Conti, J.B. Predictors of quality of life in patients with implantable cardioverter defibrillators. Psychosomatics 2005, 46, 451–457. [Google Scholar] [CrossRef]
- Starrenburg, A.; Pedersen, S.; van den Broek, K.; Kraaier, K.; Scholten, M.; Van der Palen, J. Gender differences in psychological distress and quality of life in patients with an ICD 1-year postimplant. Pacing Clin. Electrophysiol. 2014, 37, 843–852. [Google Scholar] [CrossRef]
- Timal, R.J.; de Gucht, V.; Rotmans, J.I.; Hensen, L.C.R.; Buiten, M.S.; de Bie, M.K.; Putter, H.; Schalij, M.J.; Rabelink, T.J.; Jukema, J.W. The impact of transvenous cardioverter-defibrillator implantation on quality of life, depression and optimism in dialysis patients: Report on the secondary outcome of QOL in the randomized controlled ICD2 trial. Qual. Life Res. 2021, 30, 1605–1617. [Google Scholar] [CrossRef]
- Alonso, W.W.; Faulkner, K.M.; Pozehl, B.J.; Hupcey, J.E.; Kitko, L.A.; Lee, C.S. A longitudinal comparison of health-related quality of life in rural and urban recipients of left ventricular assist devices. Res. Nurs. Health 2020, 43, 396–406. [Google Scholar] [CrossRef]
- Arnold, S.V.; Jones, P.G.; Allen, L.A.; Cohen, D.J.; Fendler, T.J.; Holtz, J.E.; Aggarwal, S.; Spertus, J.A. Frequency of Poor Outcome (Death or Poor Quality of Life) After Left Ventricular Assist Device for Destination Therapy: Results from the INTERMACS Registry. Circ. Heart Fail. 2016, 9, e002800. [Google Scholar] [CrossRef] [Green Version]
- Bidwell, J.T.; Lyons, K.S.; Mudd, J.O.; Grady, K.L.; Gelow, J.M.; Hiatt, S.O.; Chien, C.V.; Lee, C.S. Patient and Caregiver Determinants of Patient Quality of Life and Caregiver Strain in Left Ventricular Assist Device Therapy. J. Am. Heart Assoc. 2018, 7, e008080. [Google Scholar] [CrossRef] [PubMed]
- Cowger, J.A.; Naka, Y.; Aaronson, K.D.; Horstmanshof, D.; Gulati, S.; Rinde-Hoffman, D.; Pinney, S.; Adatya, S.; Farrar, D.J.; Jorde, U.P. Quality of life and functional capacity outcomes in the MOMENTUM 3 trial at 6 months: A call for new metrics for left ventricular assist device patients. J. Heart Lung Transpl. 2018, 37, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grady, K.L.; Sherri, W.; Naftel, D.C.; Myers, S.; Gelijins, A.; Moskowitz, A.; Pagani, F.D.; Young, J.B.; Spertus, J.A.; Kirklin, J.K. Age and gender differences and factors related to change in health-related quality of life from before to 6 months after left ventricular assist device implantation: Findings from Interagency Registry for Mechanically Assisted Circulatory Support. J. Heart Lung Transpl. 2016, 35, 777–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakovljevic, D.G.; McDiarmid, A.; Hallsworth, K.; Seferovic, P.M.; Ninkovic, V.M.; Parry, G.; Schueler, S.; Trenell, M.I.; MacGowan, G.A. Effect of left ventricular assist device implantation and heart transplantation on habitual physical activity and quality of life. Am. J. Cardiol. 2014, 114, 88–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kato, N.P.; Okada, I.; Imamura, T.; Kagami, Y.; Endo, M.; Nitta, D.; Fujino, T.; Muraoka, H.; Minatsuki, S.; Maki, H.; et al. Quality of Life and Influential Factors in Patients Implanted with a Left Ventricular Assist Device. Circ. J. 2015, 79, 2186–2192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiernan, M.S.; Najjar, S.S.; Vest, A.R.; Birks, E.J.; Uriel, N.; Ewald, G.A.; Leadley, K.; Patel, C.B. Outcomes of Severely Obese Patients Supported by a Centrifugal-Flow Left Ventricular Assist Device. J. Card Fail. 2020, 26, 120–127. [Google Scholar] [CrossRef]
- Lee, C.S.; Gelow, J.M.; Chien, C.V.; Hiatt, S.O.; Bidwell, J.T.; Denfeld, Q.E.; Grady, K.L.; Mudd, J.O. Implant Strategy-Specific Changes in Symptoms in Response to Left Ventricular Assist Devices. J. Cardiovasc. Nurs. 2018, 33, 144–151. [Google Scholar] [CrossRef]
- Mehra, M.R.; Uriel, N.; Naka, Y.; Cleveland, J.C.; Yuzefpolskaya, M., Jr.; Salerno, C.T.; Walsh, M.N.; Milano, C.A.; Patel, C.B.; Hutchins, S.W.; et al. A Fully Magnetically Levitated Left Ventricular Assist Device—Final Report. N. Engl. J. Med. 2019, 380, 1618–1627. [Google Scholar] [CrossRef]
- Nassif, M.E.; Spertus, J.A.; Jones, P.G.; Fendler, T.J.; Allen, L.A.; Grady, K.L.; Arnold, S.V. Changes in disease-specific versus generic health status measures after left ventricular assist device implantation: Insights from INTERMACS. J. Heart Lung Transpl. 2017, 36, 1243–1249. [Google Scholar] [CrossRef]
- Rose, E.A.; Gelijns, A.C.; Moskowitz, A.J.; Heitjan, D.F.; Stevenson, L.W.; Dembitsky, W.; Long, J.W.; Ascheim, D.D.; Tierney, A.R.; Levitan, R.G.; et al. Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure Study G. Long-term use of a left ventricular assist device for end-stage heart failure. N. Engl. J. Med. 2001, 345, 1435–1443. [Google Scholar] [CrossRef]
- Starling, R.C.; Estep, J.D.; Horstmanshof, D.A.; Milano, C.A.; Stehlik, J.; Shah, K.B.; Bruckner, B.A.; Lee, S.; Long, J.W.; Selzman, C.H.; et al. Risk Assessment and Comparative Effectiveness of Left Ventricular Assist Device and Medical Management in Ambulatory Heart Failure Patients: The ROADMAP Study 2-Year Results. JACC Heart Fail. 2017, 5, 518–527. [Google Scholar] [CrossRef] [PubMed]
- Voltolini, A.; Salvato, G.; Frigerio, M.; Cipriani, M.; Perna, E.; Pisu, M.; Mazza, U. Psychological outcomes of left ventricular assist device long-term treatment: A 2-year follow-up study. Artif. Organs 2020, 44, 67–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimpfer, D.; Gustafsson, F.; Potapov, E.; Pya, Y.; Schmitto, J.; Berchtold-Herz, M.; Morshuis, M.; Shaw, S.M.; Saeed, D.; Lavee, J.; et al. Two-year outcome after implantation of a full magnetically levitated left ventricular assist device: Results from the ELEVATE Registry. Eur. Heart J. 2020, 41, 3801–3809. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Gandek, B. Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. J. Clin. Epidemiol. 1998, 51, 903–912. [Google Scholar] [CrossRef]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Faller, H.; Steinbuchel, T.; Schowalter, M.; Spertus, J.A.; Stork, S.; Angermann, C.E. The Kansas City Cardiomyopathy Questionnaire (KCCQ)—A new disease-specific quality of life measure for patients with chronic heart failure. Psychother. Psychosom. Med. Psychol. 2005, 55, 200–208. [Google Scholar] [CrossRef]
- Buiting, H.M.; Olthuis, G. Importance of Quality-of-Life Measurement Throughout the Disease Course. JAMA Netw. Open 2020, 3, e200388. [Google Scholar] [CrossRef] [Green Version]
- Pequeno, N.P.F.; Cabral, N.L.A.; Marchioni, D.M.; Lima, S.; Lyra, C.O. Quality of life assessment instruments for adults: A systematic review of population-based studies. Health Qual. Life Outcomes 2020, 18, 208. [Google Scholar] [CrossRef]
- Chernoff, R.A.; Messineo, G.; Kim, S.; Pizano, D.; Korouri, S.; Danovitch, I.; IsHak, W.W. Psychosocial Interventions for Patients with Heart Failure and Their Impact on Depression, Anxiety, Quality of Life, Morbidity and Mortality: A Systematic Review and Meta-Analysis. Psychosom. Med. 2022, 84, 560–580. [Google Scholar] [CrossRef]
- Habibovic, M.; Denollet, J.; Cuijpers, P.; Spek, V.R.; van den Broek, K.C.; Warmerdam, L.; van der Voort, P.H.; Herrman, J.P.; Bouwels, L.; Valk, S.S.; et al. E-health to manage distress in patients with an implantable cardioverter-defibrillator: Primary results of the WEBCARE trial. Psychosom. Med. 2014, 76, 593–602. [Google Scholar] [CrossRef]
- Habibovic, M.; Broers, E.; Heumen, D.; Widdershoven, J.; Pedersen, S.S.; Denollet, J. Optimism as predictor of patient-reported outcomes in patients with an implantable cardioverter defibrillator (data from the WEBCARE study). Gen. Hosp. Psychiatry 2018, 50, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Sobczak-Kaleta, M.A.; Qawoq, H.D.; Krawczyk, M.; Wierzbowska-Drabik, K.; Kasprzak, J.D. Cognitive behavioral intervention improves quality of life and perceived illness acceptance in patients after cardiac electrotherapy devices implantation. Psychiatr. Pol. 2019, 53, 1037–1051. [Google Scholar] [CrossRef]
- Rakhshan, M.; Khoshnood, Z.; Ansari, L.; Aslani, A. Body Image and Adjustment Among Patients with Heart Rhythm Management Devices Following Cardiac Rehabilitation Program: A Randomized Controlled Clinical Trial. Clin. Med. Res. 2022, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Habibovic, M.; Pedersen, S.S.; Broers, E.R.; Alings, M.; Theuns, D.; van der Voort, P.H.; Bouwels, L.; Herrman, J.P.; Denollet, J. Prevalence of anxiety and risk associated with ventricular arrhythmia in patients with an implantable cardioverter defibrillator. Int. J. Cardiol. 2020, 310, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.S.; Hoogwegt, M.T.; Jordaens, L.; Theuns, D.A. Pre-implantation psychological functioning preserved in majority of implantable cardioverter defibrillator patients 12 months post implantation. Int. J. Cardiol. 2013, 166, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.S.; Mastenbroek, M.H.; Carter, N.; Barr, C.; Neuzil, P.; Scholten, M.; Lambiase, P.D.; Boersma, L.; Johansen, J.B.; Theuns, D.A. A Comparison of the Quality of Life of Patients with an Entirely Subcutaneous Implantable Defibrillator System Versus a Transvenous System (from the EFFORTLESS S-ICD Quality of Life Substudy). Am. J. Cardiol. 2016, 118, 520–526. [Google Scholar] [CrossRef]
- Polikandrioti, M.; Tzirogiannis, K.; Zyga, S.; Gerogianni, G.; Stefanidou, S.; Tsami, A.; Panoutsopoulos, G. Assessment of fatigue in patients with a permanent cardiac pacemaker: Prevalence and associated factors. Arch. Med. Sci. Atheroscler. Dis. 2018, 3, e166–e173. [Google Scholar] [CrossRef] [Green Version]
- Polikandrioti, M.; Tzirogiannis, K.; Zyga, S.; Koutelekos, I.; Vasilopoulos, G.; Theofilou, P.; Panoutsopoulos, G. Effect of anxiety and depression on the fatigue of patients with a permanent pacemaker. Arch. Med. Sci. Atheroscler. Dis. 2018, 3, e8–e17. [Google Scholar] [CrossRef]
- Edmondson, D.; von Kanel, R. Post-traumatic stress disorder and cardiovascular disease. Lancet Psychiatry 2017, 4, 320–329. [Google Scholar] [CrossRef] [Green Version]
- Havranek, E.P.; Mujahid, M.S.; Barr, D.A.; Blair, I.V.; Cohen, M.S.; Cruz-Flores, S.; Davey-Smith, G.; Dennison-Himmelfarb, C.R.; Lauer, M.S.; Lockwood, D.W.; et al. Social Determinants of Risk and Outcomes for Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 2015, 132, 873–898. [Google Scholar] [CrossRef] [Green Version]
- Chaddha, A.; Robinson, E.A.; Kline-Rogers, E.; Alexandris-Souphis, T.; Rubenfire, M. Mental Health and Cardiovascular Disease. Am. J. Med. 2016, 129, 1145–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Copeland, L.A.; Sako, E.Y.; Zeber, J.E.; Pugh, M.J.; Wang, C.P.; MacCarthy, A.A.; Restrepo, M.I.; Mortensen, E.M.; Lawrence, V.A. Mortality after cardiac or vascular operations by preexisting serious mental illness status in the Veterans Health Administration. Gen. Hosp. Psychiatry 2014, 36, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Werner, H.; Balmer, C.; Lehmann, P. Posttraumatic stress and health-related quality of life in parents of children with cardiac rhythm devices. Qual. Life Res. 2019, 28, 2471–2480. [Google Scholar] [CrossRef] [PubMed]
- Grady, K.L.; Andrei, A.C.; Elenbaas, C.; Warzecha, A.; Baldridge, A.; Kao, A.; Spertus, J.A.; Pham, D.T.; Dew, M.A.; Hsich, E.; et al. Health-Related Quality of Life in Older Patients with Advanced Heart Failure: Findings finrom the SUSTAIN-IT Study. J. Am. Heart Assoc. 2022, 11, e024385. [Google Scholar] [CrossRef] [PubMed]
- Rubio, R.; Palacios, B.; Varela, L.; Fernandez, R.; Camargo Correa, S.; Estupinan, M.F.; Calvo, E.; Jose, N.; Ruiz Munoz, M.; Yun, S.; et al. Quality of life and disease experience in patients with heart failure with reduced ejection fraction in Spain: A mixed-methods study. BMJ Open 2021, 11, e053216. [Google Scholar] [CrossRef] [PubMed]
- Mitacchione, G.; Schiavone, M.; Gasperetti, A.; Viecca, M.; Curnis, A.; Forleo, G.B. Atrioventricular synchronous leadless pacemaker: State of art and broadened indications. Rev. Cardiovasc. Med. 2021, 22, 395–401. [Google Scholar] [CrossRef]
- Mitacchione, G.; Arabia, G.; Schiavone, M.; Cerini, M.; Gasperetti, A.; Salghetti, F.; Bontempi, L.; Viecca, M.; Curnis, A.; Forleo, G.B. Intraoperative sensing increase predicts long-term pacing threshold in leadless pacemakers. J. Interv. Card Electrophysiol. 2022, 63, 679–686. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Willy, K.; Ellermann, C.; Reinke, F.; Rath, B.; Wolfes, J.; Eckardt, L.; Doldi, F.; Wegner, F.K.; Köbe, J.; Morina, N. The Impact of Cardiac Devices on Patients’ Quality of Life—A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2022, 9, 257. https://doi.org/10.3390/jcdd9080257
Willy K, Ellermann C, Reinke F, Rath B, Wolfes J, Eckardt L, Doldi F, Wegner FK, Köbe J, Morina N. The Impact of Cardiac Devices on Patients’ Quality of Life—A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease. 2022; 9(8):257. https://doi.org/10.3390/jcdd9080257
Chicago/Turabian StyleWilly, Kevin, Christian Ellermann, Florian Reinke, Benjamin Rath, Julian Wolfes, Lars Eckardt, Florian Doldi, Felix K. Wegner, Julia Köbe, and Nexhmedin Morina. 2022. "The Impact of Cardiac Devices on Patients’ Quality of Life—A Systematic Review and Meta-Analysis" Journal of Cardiovascular Development and Disease 9, no. 8: 257. https://doi.org/10.3390/jcdd9080257