
Challenges of Health Data Use in Multidisciplinary Chronic Disease Care: Perspective from Heart Failure Care



{kind=link}
Abstract
:1. Introduction
2. Traditional and Modern Data Sources, Processing, and Implications
2.1. Traditional Heart Failure Data
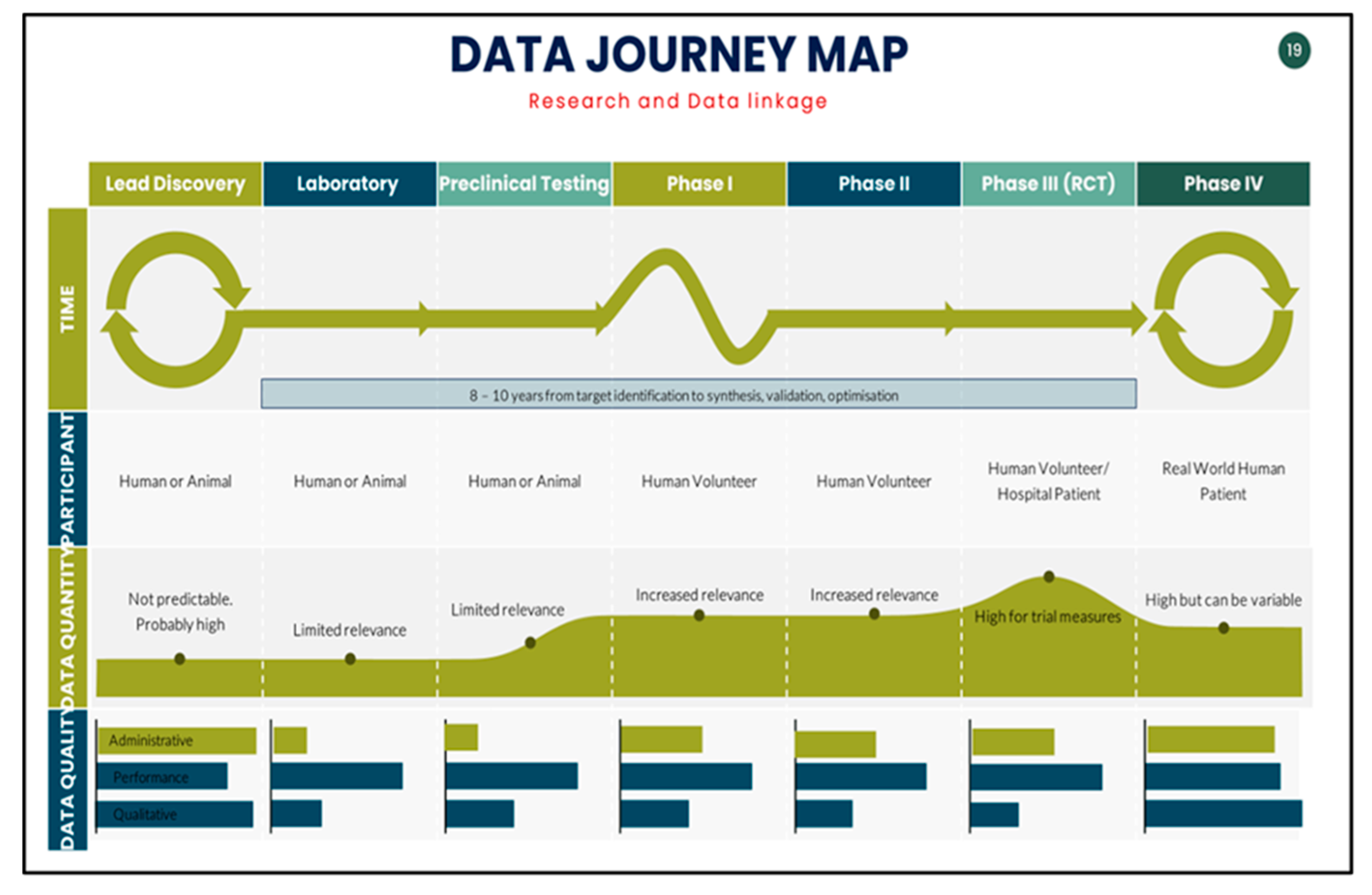
2.2. Data Journey during the Research Phase and Post-Trial Phase
2.3. The Wide Array of Data in Clinical Heart Failure Management
2.4. Dimensions of Chronic Disease Care: Implications for Heart Failure Health Data
- Chronicity: Chronic cardiovascular diseases, including CHF, make up 85% of presentations to primary care. The strength of guidelines and gaps in community outcomes confirms translational issues between evidence and community uptake;
- Complexity: CHF has a trajectory of decompensation, stability, and eventual palliation, and requires multidisciplinary care throughout the course of the illness. CHF programs are required to navigate the complexity of the disease, high resource use, and additional burdens caused by comorbid conditions. All these influence CHF outcomes. Therefore, screening, prevention, monitoring, and treatment are essential;
- Divergence: Although there have been significant advancements in therapy, chronic heart failure (CHF) remains widespread, particularly with the rise in heart failure with preserved ejection fraction (HFpEF) syndrome in the aging population. HFpEF currently constitutes over 50% of all CHF cases, especially among elderly individuals;
- Burden: It is increasingly clear that this syndrome places a significant strain on both patients and healthcare systems, even before considering the underlying causes or additional coexisting conditions. These factors are present in at least 50% of cases and include conditions such as ischemic heart disease, as well as comorbidities like diabetes, renal failure, sleep apnoea, and hypertension. This burden translates into the complexity of the disease, increased utilisation of healthcare resources, a high rate of readmissions, the need for long-term and often lifelong treatments, and regular support from multidisciplinary healthcare services;
- Heterogeneity: Risk factors including race, smoking, drug and alcohol use, and socioeconomic and other demographic factors contribute to healthcare gaps or differential distribution of health resources, e.g., geography or social isolation add sociodemographic variables to disease phenotype;
- Unmet needs: Future projections point at a significant increase in incidence, burden, and cost annually to >51,000 individuals and prevalence of >1.5 million cases by 2030 and an estimated annual cost of $3.8 billion in Australia. Specific considerations have to be given to priority and vulnerable populations, including elderly and Indigenous populations. These groups suffer disproportionately from disease burden, hospitalisations, non-traditional risk factors, and delays in uptake of Guideline-Based Medical Therapies (GBMTs).
3. Barriers in Interpreting/Accessing Clinical Evidence
4. Challenges to Data Collection and Processing
4.1. The Limitations of Translating Clinical Trials into HF Practice
4.2. Incidental Post-Trial Population-Level Patient Factors in Congestive Heart Failure
- Initial studies on the use of vasodilators in heart failure provided evidence to support the prognostic benefit of nitrate in combination with hydralazine for heart failure with reduced ejection fraction in the 1980s. They are still the recommended therapy in some circumstances. Accumulating evidence from the V-HEFT and V-HEFT1 studies showed a greater benefit of this combination in the African American cohort. This was then confirmed in the A-HEFT study [9]. Additional studies with ethnographic differences were noted, including a blood pressure trial using diuretics and several renin aldosterone-modulating agents such as lisinopril and losartan [10];
- Population-based genome-sequencing studies identified racial differences in allele frequency and incidence of HF [13,14]. Insofar as this extends to Black women, this population exhibits a higher incidence of peripartum cardiomyopathy, which is also less responsive to angiotensin-converting enzyme inhibitors (ACEi) and β-blockers [15]. A relative deficiency of natriuretic factors, a higher prevalence of salt sensitivity and sodium retention, as well as low physiological renin and aldosterone levels have treatment implications [16,17,18];
- Based on the evidence outlined above, a combination of modifiable and non-modifiable factors must consider acquired and modifiable socioeconomic barriers to health equity [18]. It is at this juncture that we can start to appreciate the complexity of CHF and achieving equitable outcomes at the population level.
4.3. Patient-Reported Outcomes in Heart Failure
- (i)
- Assisting patients in discussing concerns with their clinicians, such as changes in mental health during the course of treatment;
- (ii)
- Sensitising patients to health issues, including symptoms related to their underlying health conditions and treatments that they may not have initially considered discussing with their clinicians;
- (iii)
- Aiding in the identification of health issues that may require further investigation and management;
- (iv)
- Facilitating the tracking of health outcomes over time;
- (v)
- Allowing for comparisons between an individual patient’s outcomes and those of other patients with similar health conditions;
- (vi)
- Supporting shared decision-making by providing information on the effects of different treatments on patient-reported outcomes.
4.4. Utilising Data
5. Building Models of Care for Community Hubs with System-Wide Performance Measures
6. Framework for Facing These Challenges
6.1. Adopting the Chronic Care Model (CCM)
6.2. Improving Outcome Measures
6.3. Funding Community-Based Health Hubs
- (i)
- New data—generate usable data where previous data were of poor quality;
- (ii)
- Scarce data—bring patient data together to create a larger volume of more sociodemographically diverse data with access to regional areas;
- (iii)
- Traditional data—utilise existing data for retrospective, real-time, and prospective studies.
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- RBC Capital Markets|Navigating the Changing Face of Healthcare Episode. Available online: https://www.rbccm.com/en/gib/changing-face-of-healthcare.page (accessed on 20 June 2023).
- van Roessel, I.; Reumann, M.; Brand, A. Potentials and Challenges of the Health Data Cooperative Model. Public Health Genom. 2018, 20, 321–331. [Google Scholar] [CrossRef]
- Iyngkaran, P.; Liew, D.; McDonald, P.; Thomas, M.C.; Reid, C.; Chew, D.; Hare, D.L. Phase 4 Studies in Heart Failure—What is Done and What is Needed? Curr. Cardiol. Rev. 2016, 12, 216–230. [Google Scholar] [CrossRef]
- Taylor, J.K.; Ahmed, F.Z. Clinical Pathways Guided by Remotely Monitoring Cardiac Device Data: The Future of Device Heart Failure Management? Arrhythmia Electrophysiol. Rev. 2023, 12, e15. [Google Scholar] [CrossRef] [PubMed]
- Heneghan, C.; Goldacre, B.; Mahtani, K.R. Why clinical trial outcomes fail to translate into benefits for patients. Trials 2017, 18, 122. [Google Scholar] [CrossRef] [PubMed]
- Department of Health, The Victorian Government. Rights and Privacy; Department of Health, The Victorian Government: Melbourne, Australia, 2022.
- Yuan, B.; Li, J. The Policy Effect of the General Data Protection Regulation (GDPR) on the Digital Public Health Sector in the European Union: An Empirical Investigation. Int. J. Environ. Res. Public Health 2019, 16, 1070. [Google Scholar] [CrossRef] [PubMed]
- Wierda, E.; Eindhoven, D.C.; Schalij, M.J.; Borleffs, C.J.W.; Amoroso, G.; van Veghel, D.; Mitchell, C.R.; Mol, B.A.J.M.d.; Hirsch, A.; Ploem, M.C. Privacy of patient data in quality-of-care registries in cardiology and cardiothoracic surgery: The impact of the new general data protection regulation EU-law. Eur. Heart J. Qual. Care Clin. Outcomes 2018, 4, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Emmons-Bell, S.; Johnson, C.; Roth, G. Prevalence, incidence and survival of heart failure: A systematic review. Heart 2022, 108, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Iyngkaran, P.; Wilson, A.; Wong, J.; Prior, D.; Kaye, D.; Hare, D.L.; Bergin, P.; Jelinem, M. Part 1: The Wider Considerations in Translating Heart Failure Guidelines. Curr. Cardiol. Rev. 2021, 17, e160721190003. [Google Scholar] [CrossRef]
- Morris, A.A.; Patel, R.S.; Binongo, J.N.G.; Poole, J.; Al Mheid, I.; Ahmed, Y.; Stoyanova, N.; Vaccarino, V.; Din-Dzietham, R.; Gibbons, G.H.; et al. Racial differences in arterial stiffness and microcirculatory function between Black and White Americans. J. Am. Heart Assoc. 2013, 2, e002154. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Ii, G.W.D.; Shetty, A.; Parihar, A.; Dave, T.; Robinson, S.W.; Gottlieb, S.S.; Donahue, M.P.; Tomaselli, G.F.; Kraus, W.E.; et al. A Genome-Wide Association Study of Idiopathic Dilated Cardiomyopathy in African Americans. J. Pers. Med. 2018, 8, 11. [Google Scholar] [CrossRef]
- Myers, V.D.; Gerhard, G.S.; McNamara, D.M.; Tomar, D.; Madesh, M.; Kaniper, S.; Ramsey, F.V.; Fisher, S.G.; Ingersoll, R.G.; Kasch-Semenza, L.; et al. Association of Variants in BAG3 With Cardiomyopathy Outcomes in African American Individuals. JAMA Cardiol. 2018, 3, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Irizarry, O.C.; Levine, L.D.; Lewey, J.; Boyer, T.; Riis, V.; Elovitz, M.A.; Arany, Z. Comparison of Clinical Characteristics and Outcomes of Peripartum Cardiomyopathy Between African American and Non–African American Women. JAMA Cardiol. 2017, 2, 1256–1260. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.K.; de Lemos, J.A.; Ayers, C.R.; Berry, J.D.; Wang, T.J. Racial Differences in Natriuretic Peptide Levels. JACC: Heart Fail. 2015, 3, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Nayak, A.; Hicks, A.J.; Morris, A.A. Understanding the Complexity of Heart Failure Risk and Treatment in Black Patients. Circ. Heart Fail. 2020, 13, e007264. [Google Scholar] [CrossRef]
- Morris, A.A.; Nayak, A.; Ko, Y.-A.; D’souza, M.; Felker, G.M.; Redfield, M.M.; Tang, W.W.; Testani, J.M.; Butler, J. Racial Differences in Diuretic Efficiency, Plasma Renin, and Rehospitalization in Subjects with Acute Heart Failure. Circ. Heart Fail. 2020, 13, e006827. [Google Scholar] [CrossRef]
- Floyd, J.; Fowler, J. Questions to measure subjective states. In Improving Survey Questions: Design and Evaluation; Sage Publications: New York, NY, USA, 1995. [Google Scholar]
- Australian Commision on Safety, Quality in Healthcare. Patient Reported Outcome Measures: An Enviornmental Scan of the Australian Healthcare; Australian Commision on Safety, Quality in Healthcare: Sydney, Australia, 2016. [Google Scholar]
- Field, J.; Holmes, M.M.; Newell, D. PROMs data: Can it be used to make decisions for individual patients? A narrative review. Patient Relat. Outcome Meas. 2019, 10, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Comín-Colet, J.; Anguita, M.; Formiga, F.; Almenar, L.; Crespo-Leiro, M.G.; Manzano, L.; Muñiz, J.; Chaves, J.; de Frutos, T.; Enjuanes, C. Health-related Quality of Life of Patients with Chronic Systolic Heart Failure in Spain: Results of the VIDA-IC Study. In Revista Española de Cardiología (English Edition); Elsevier BV: Amsterdam, The Netherlands, 2016; Volume 69, pp. 256–271. [Google Scholar]
- Psotka, M.A.; von Maltzahn, R.; Anatchkova, M.; Agodoa, I.; Chau, D.; Malik, F.I.; Patrick, D.L.; Spertus, J.A.; Wiklund, I.; Teer, J.R. Patient-Reported Outcomes in Chronic Heart Failure: Applicability for Regulatory Approval. JACC Heart Fail. 2016, 4, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, F.S.; Jackson, K.L.; Yount, S.E.; Rothrock, N.E.; Kallen, M.A.; Lacson, L.; Bilimoria, K.Y.; Kho, A.N.; Mutharasan, R.K.; McCullough, P.A.; et al. The development and initial validation of the PROMIS®+HF-27 and PROMIS+HF-10 profiles. ESC Heart Fail. 2022, 9, 3380–3392. [Google Scholar] [CrossRef]
- Spertus, J.A.; Jones, P.G. Development and Validation of a Short Version of the Kansas City Cardiomyopathy Questionnaire. Circ. Cardiovasc. Qual. Outcomes 2015, 8, 469–476. [Google Scholar] [CrossRef]
- Chew, D.S.; Whitelaw, S.; Vaduganathan, M.; Mark, D.B.; Van Spall, H.G.C. Patient-Reported Outcome Measures in Cardiovascular Disease: An Evidence Map of the Psychometric Properties of Health Status Instruments. Ann. Intern. Med. 2022, 175, 1431–1439. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Fonarow, G.C.; Breathett, K.; Jurgens, C.Y.; Pisani, B.A.; Pozehl, B.J.; Spertus, J.A.; Taylor, K.G.; Thibodeau, J.T.; Yancy, C.W.; et al. 2020 ACC/AHA Clinical Performance and Quality Measures for Adults with Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e000099. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, A.R. Performance Improvement in Healthcare: Is Personalized Site Feedback Enough? Circ. Cardiovasc. Qual. Outcomes 2015, 8, 335–337. [Google Scholar] [CrossRef]
- MacInnes, J.; Williams, L. A review of integrated heart failure care. Prim. Health Care Res. Dev. 2019, 20, e57. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.H.; Austin, B.T.; Von Korff, M. Organizing Care for Patients with Chronic Illness. Milbank Q. 1996, 74, 511–544. [Google Scholar] [CrossRef]
- Grover, A.; Joshi, A. An Overview of Chronic Disease Models: A Systematic Literature Review. Glob. J. Health Sci. 2015, 7, 210–227. [Google Scholar] [CrossRef]
- Asch, S.M.; Baker, D.W.; Keesey, J.W.B.; Broder, M.M.; Schonlau, M.; Rosen, M.B.; Wallace, P.L.R.; Keeler, E.B. Does the Collaborative Model Improve Care for Chronic Heart Failure? Med. Care 2005, 43, 667–675. [Google Scholar] [CrossRef]
- Australian Research Alliance for Children and Youth (ARACY). The Regulation of Health Information Privacy in Australia. (n.d). Available online: https://www.aracy.org.au/publications-resources/area?command=record&id=115&cid=6 (accessed on 20 June 2023).
- McDonagh, T.A.; Metra, M.; Adamo, M.; Baumbach, A.; Böhm, M.; Burri, H.; Čelutkiene, J.; Chioncel, O.; Cleland, J.G.F.; Coats, A.J.S.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Victorian Auditor’s General Office (VAGO). Security of Patient’s Hospital Data; Victorian Auditor’s General Office: Melbourne, Australia, 2019. [Google Scholar]
- Iyngkaran, P.; Liew, D.; Neil, C.; Driscoll, A.; Marwick, T.H.; Hare, D.L. Moving from Heart Failure Guidelines to Clinical Practice: Gaps Contributing to Readmissions in Patients with Multiple Comorbidities and Older Age. Clin. Med. Insights Cardiol. 2018, 12, 1179546818809358. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iyngkaran, P.; Usmani, W.; Hanna, F.; de Courten, M. Challenges of Health Data Use in Multidisciplinary Chronic Disease Care: Perspective from Heart Failure Care. J. Cardiovasc. Dev. Dis. 2023, 10, 486. https://doi.org/10.3390/jcdd10120486
Iyngkaran P, Usmani W, Hanna F, de Courten M. Challenges of Health Data Use in Multidisciplinary Chronic Disease Care: Perspective from Heart Failure Care. Journal of Cardiovascular Development and Disease. 2023; 10(12):486. https://doi.org/10.3390/jcdd10120486
Chicago/Turabian StyleIyngkaran, Pupalan, Wania Usmani, Fahad Hanna, and Maximilian de Courten. 2023. "Challenges of Health Data Use in Multidisciplinary Chronic Disease Care: Perspective from Heart Failure Care" Journal of Cardiovascular Development and Disease 10, no. 12: 486. https://doi.org/10.3390/jcdd10120486
APA StyleIyngkaran, P., Usmani, W., Hanna, F., & de Courten, M. (2023). Challenges of Health Data Use in Multidisciplinary Chronic Disease Care: Perspective from Heart Failure Care. Journal of Cardiovascular Development and Disease, 10(12), 486. https://doi.org/10.3390/jcdd10120486