
Soluble ST2 in Heart Failure: A Clinical Role beyond B-Type Natriuretic Peptide
 , ,
, ,
Abstract
:1. Introduction
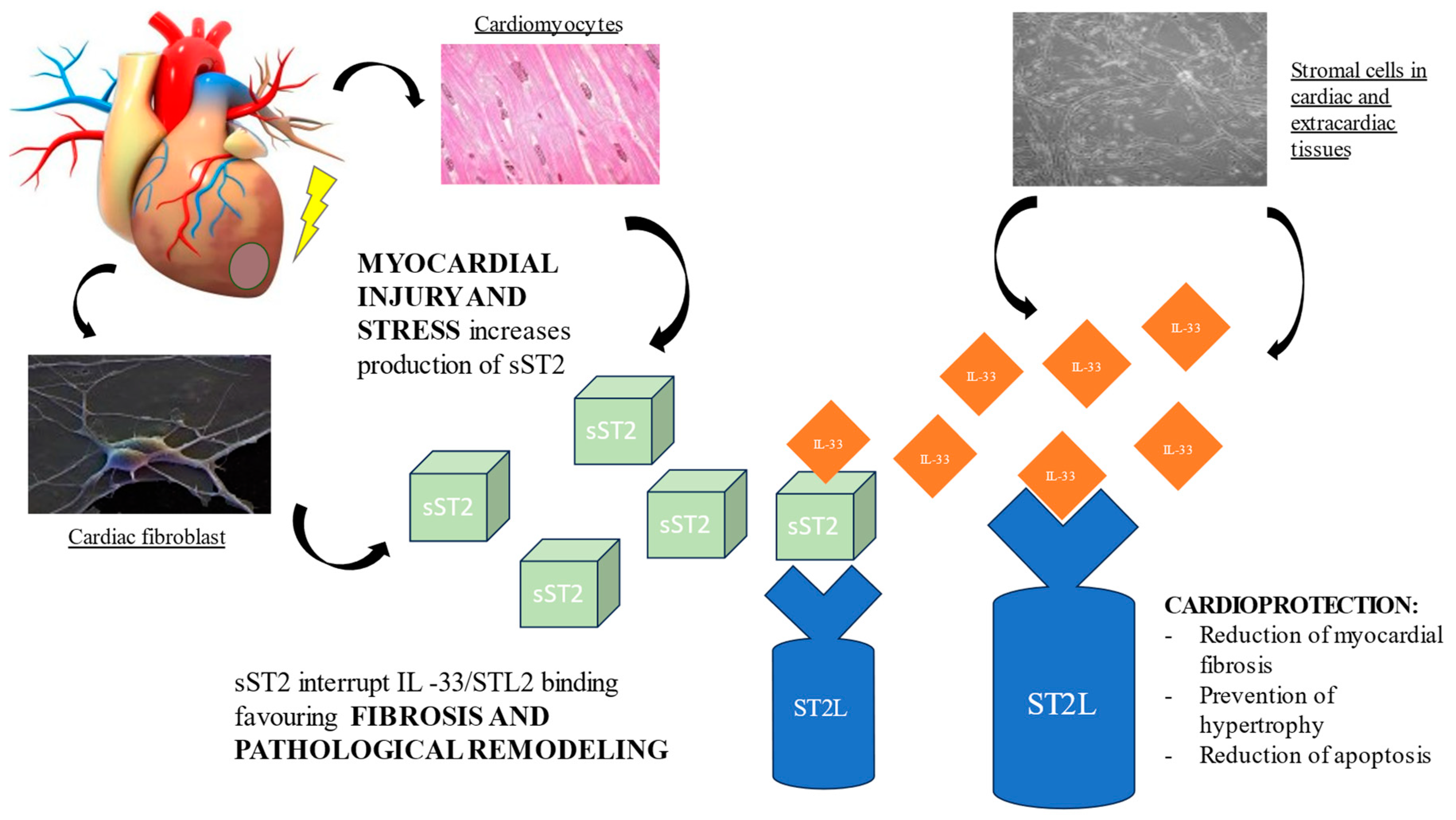
2. sST2 Biology
3. sST2 Prognostic Role
3.1. Incident HF
3.2. Acute HF
3.3. Chronic HF
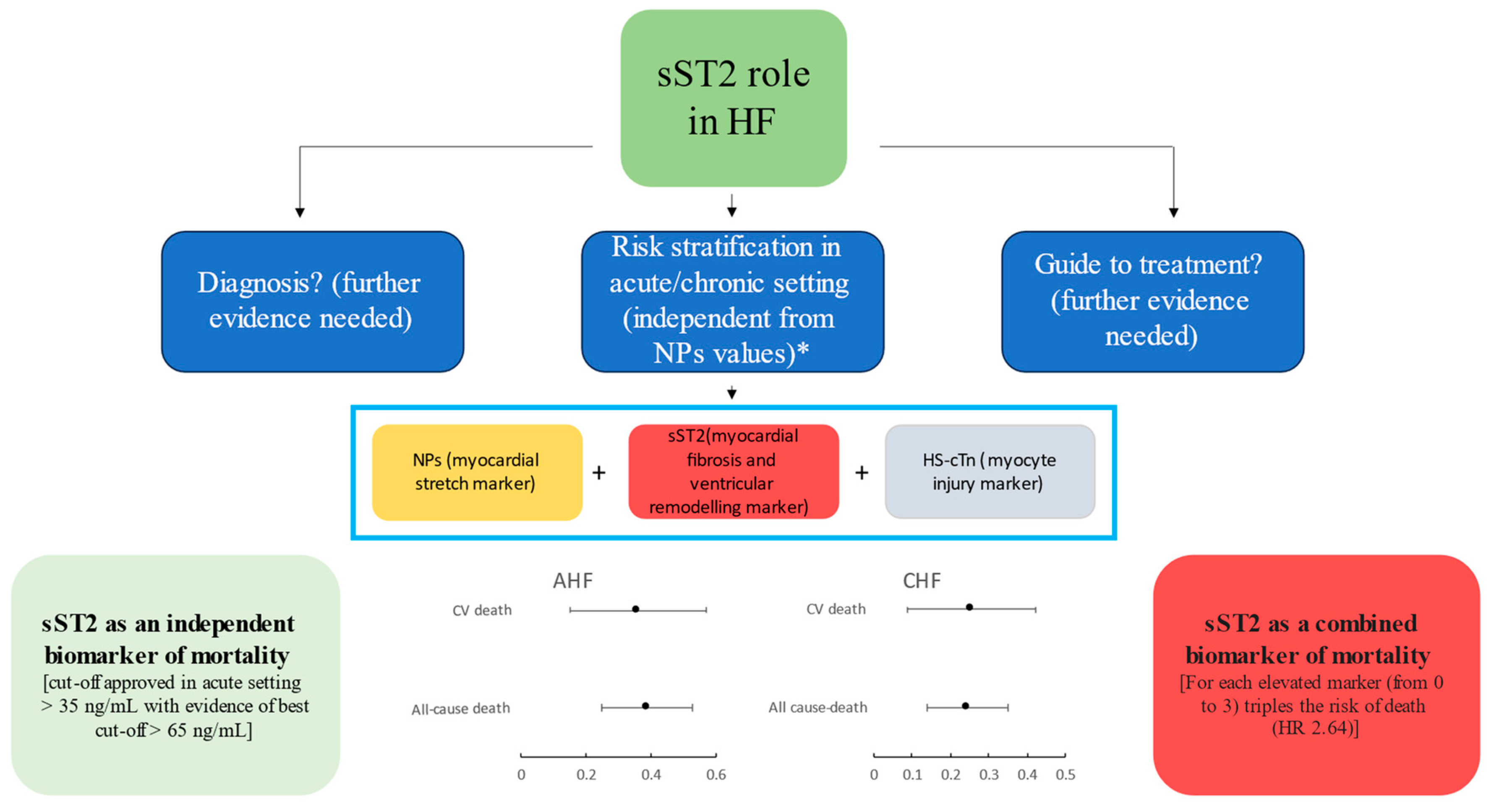
4. sST2 Assessment in Addition to NPs: Is There a Role?
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Riccardi, M.; Sammartino, A.M.; Piepoli, M.; Adamo, M.; Pagnesi, M.; Rosano, G.; Metra, M.; von Haehling, S.; Tomasoni, D. Heart failure: An update from the last years and a look at the near future. ESC Heart Fail. 2022, 9, 3667–3693. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; de la Espriella, R.; Rossignol, P.; Voors, A.A.; Mullens, W.; Metra, M.; Chioncel, O.; Januzzi, J.L.; Mueller, C.; Richards, A.M.; et al. Congestion in heart failure: A circulating biomarker-based perspective. A review from the Biomarkers Working Group of the Heart Failure Association, European Society of Cardiology. Eur. J. Heart Fail. 2022, 24, 1751–1766. [Google Scholar] [CrossRef] [PubMed]
- Authors/Task Force Members; McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [PubMed]
- Tsutsui, H.; Albert, N.M.; Coats, A.J.S.; Anker, S.D.; Bayes-Genis, A.; Butler, J.; Chioncel, O.; Defilippi, C.R.; Drazner, M.H.; Felker, G.M.; et al. Natriuretic Peptides: Role in the Diagnosis and Management of Heart Failure: A Scientific Statement From the Heart Failure Association of the European Society of Cardiology, Heart Failure Society of America and Japanese Heart Failure Society. J. Card Fail. 2023, 29, 787–804. [Google Scholar] [CrossRef]
- Braunwald, E. Biomarkers in heart failure. N. Engl. J. Med. 2008, 358, 2148–2159. [Google Scholar] [CrossRef]
- Pascual-Figal, D.A.; Pérez-Martínez, M.T.; Asensio-Lopez, M.C.; Sanchez-Más, J.; García-García, M.E.; Martinez, C.M.; Lencina, M.; Jara, R.; Januzzi, J.L.; Lax, A. Pulmonary Production of Soluble ST2 in Heart Failure. Circ. Heart Fail. 2018, 11, e005488. [Google Scholar] [CrossRef]
- Aimo, A.; Januzzi, J.L.; Bayes-Genis, A.; Vergaro, G.; Sciarrone, P.; Passino, C.; Emdin, M. Clinical and Prognostic Significance of sST2 in Heart Failure: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 2193–2203. [Google Scholar] [CrossRef]
- Sciatti, E.; Merlo, A.; Scangiuzzi, C.; Limonta, R.; Gori, M.; D’elia, E.; Aimo, A.; Vergaro, G.; Emdin, M.; Senni, M. Prognostic Value of sST2 in Heart Failure. J. Clin. Med. 2023, 12, 3970. [Google Scholar] [CrossRef]
- Dudek, M.; Kałużna-Oleksy, M.; Migaj, J.; Sawczak, F.; Krysztofiak, H.; Lesiak, M.; Straburzyńska-Migaj, E. sST2 and Heart Failure—Clinical Utility and Prognosis. J. Clin. Med. 2023, 12, 3136. [Google Scholar] [CrossRef]
- Aleksova, A.; Paldino, A.; Beltrami, A.P.; Padoan, L.; Iacoviello, M.; Sinagra, G.; Emdin, M.; Maisel, A.S. Cardiac Biomarkers in the Emergency Department: The Role of Soluble ST2 (sST2) in Acute Heart Failure and Acute Coronary Syndrome—There is Meat on the Bone. J. Clin. Med. 2019, 8, 270. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Figal, D.A.; Januzzi, J.L. The Biology of ST2: The International ST2 Consensus Panel. Am. J. Cardiol. 2015, 115, 3B–7B. [Google Scholar] [CrossRef]
- Bergers, G.; Reikerstorfer, A.; Braselmann, S.; Graninger, P.; Busslinger, M. Alternative promoter usage of the Fos-responsive gene Fit-1 generates mRNA isoforms coding for either secreted or membrane-bound proteins related to the IL-1 receptor. EMBO J. 1994, 13, 1176–1188. [Google Scholar] [CrossRef] [PubMed]
- Werenskiold, A.K.; Hoffmann, S.; Klemenz, R. Induction of a mitogen-responsive gene after expression of the Ha-ras oncogene in NIH 3T3 fibroblasts. Mol. Cell Biol. 1989, 9, 5207–5214. [Google Scholar] [CrossRef]
- Tominaga, S.-I. A putative protein of a growth specific cDNA from BALB/C-3T3 cells is highly similar to the extracellular portion of mouse interleukin 1 receptor. FEBS Lett. 1989, 258, 301–304. [Google Scholar] [CrossRef]
- Griesenauer, B.; Paczesny, S. The ST2/IL-33 Axis in Immune Cells during Inflammatory Diseases. Front. Immunol. 2017, 8, 475. [Google Scholar] [CrossRef]
- Weinberg, E.O.; Shimpo, M.; De Keulenaer, G.W.; MacGillivray, C.; Tominaga, S.; Solomon, S.D.; Rouleau, J.-L.; Lee, R.T. Expression and regulation of ST2, an interleukin-1 receptor family member, in cardiomyocytes and myocardial infarction. Circulation 2002, 106, 2961–2966. [Google Scholar] [CrossRef] [PubMed]
- Bajwa, E.K.; Volk, J.A.; Christiani, D.C.; Harris, R.S.; Matthay, M.A.; Thompson, B.T.; Januzzi, J.L. Prognostic and Diagnostic Value of Plasma Soluble Suppression of Tumorigenicity-2 Concentrations in Acute Respiratory Distress Syndrome. Crit. Care Med. 2013, 41, 2521–2531. [Google Scholar] [CrossRef] [PubMed]
- Meijers, W.C.; Bayes-Genis, A.; Mebazaa, A.; Bauersachs, J.; Cleland, J.G.; Coats, A.J.; Januzzi, J.L.; Maisel, A.S.; McDonald, K.; Mueller, T.; et al. Circulating heart failure biomarkers beyond natriuretic peptides: Review from the Biomarker Study Group of the Heart Failure Association (HFA), European Society of Cardiology (ESC). Eur. J. Heart Fail. 2021, 23, 1610–1632. [Google Scholar] [CrossRef]
- Sanada, S.; Hakuno, D.; Higgins, L.J.; Schreiter, E.R.; McKenzie, A.N.; Lee, R.T. IL-33 and ST2 comprise a critical biomechanically induced and cardioprotective signaling system. J. Clin. Investig. 2007, 117, 1538–1549. [Google Scholar] [CrossRef]
- Zhang, J.; Chen, Z.; Ma, M.; He, Y. Soluble ST2 in coronary artery disease: Clinical biomarkers and treatment guidance. Front. Cardiovasc. Med. 2022, 9, 924461. [Google Scholar] [CrossRef] [PubMed]
- Scicchitano, P.; Marzullo, A.; Santoro, A.; Zito, A.; Cortese, F.; Galeandro, C.; Ciccone, A.S.; Angiletta, D.; Manca, F.; Pulli, R.; et al. The Prognostic Role of ST2L and sST2 in Patients Who Underwent Carotid Plaque Endarterectomy: A Five-Year Follow-Up Study. J. Clin. Med. 2022, 11, 3142. [Google Scholar] [CrossRef] [PubMed]
- Luo, G.; Qian, Y.; Sheng, X.; Sun, J.; Wu, Z.; Liao, F.; Feng, Q.; Yin, Y.; Ding, S.; Pu, J. Elevated Serum Levels of Soluble ST2 Are Associated With Plaque Vulnerability in Patients With Non-ST-Elevation Acute Coronary Syndrome. Front. Cardiovasc. Med. 2021, 8, 688522. [Google Scholar] [CrossRef] [PubMed]
- Fu, A.K.Y.; Hung, K.-W.; Yuen, M.Y.F.; Zhou, X.; Mak, D.S.Y.; Chan, I.C.W.; Cheung, T.H.; Zhang, B.; Fu, W.-Y.; Liew, F.Y.; et al. IL-33 ameliorates Alzheimer’s disease-like pathology and cognitive decline. Proc. Natl. Acad. Sci. USA 2016, 113, E2705–E2713. [Google Scholar] [CrossRef] [PubMed]
- Homsak, E.; Gruson, D. Soluble ST2: A complex and diverse role in several diseases. Clin. Chim. Acta 2020, 507, 75–87. [Google Scholar] [CrossRef]
- Bergis, D.; Kassis, V.; Radeke, H.H. High plasma sST2 levels in gastric cancer and their association with metastatic disease. Cancer Biomarkers 2016, 16, 117–125. [Google Scholar] [CrossRef]
- Yang, Z.-P.; Ling, D.-Y.; Xie, Y.-H.; Wu, W.-X.; Li, J.-R.; Jiang, J.; Zheng, J.-L.; Fan, Y.-H.; Zhang, Y. The Association of Serum IL-33 and sST2 with Breast Cancer. Dis. Markers 2015, 2015, 516895. [Google Scholar] [CrossRef]
- Oztas, E.; Kuzu, U.B.; Zengin, N.I.; Kalkan, I.H.; Saygili, F.; Yildiz, H.; Celik, H.T.; Akdogan, M.; Kilic, M.Y.; Koksal, A.S.; et al. Can Serum ST2 Levels Be Used as a Marker of Fibrosis in Chronic Hepatitis B Infection? Medicine 2015, 94, e1889. [Google Scholar] [CrossRef]
- Bergis, D.; Kassis, V.; Ranglack, A.; Koeberle, V.; Piiper, A.; Kronenberger, B.; Zeuzem, S.; Waidmann, O.; Radeke, H.H. High Serum Levels of the Interleukin-33 Receptor Soluble ST2 as a Negative Prognostic Factor in Hepatocellular Carcinoma. Transl. Oncol. 2013, 6, 311–318. [Google Scholar] [CrossRef]
- Castiglione, V.; Aimo, A.; Vergaro, G.; Saccaro, L.; Passino, C.; Emdin, M. Biomarkers for the diagnosis and management of heart failure. Heart Fail. Rev. 2022, 27, 625–643. [Google Scholar] [CrossRef]
- Andersson, C.; Enserro, D.; Sullivan, L.; Wang, T.J.; Januzzi, J.L.; Benjamin, E.J.; Vita, J.A.; Hamburg, N.M.; Larson, M.G.; Mitchell, G.F.; et al. Relations of circulating GDF-15, soluble ST2, and troponin-I concentrations with vascular function in the community: The Framingham Heart Study. Atherosclerosis 2016, 248, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.E.; Larson, M.G.; Ghorbani, A.; Cheng, S.; Vasan, R.S.; Wang, T.J.; Januzzi, J.L.J. Soluble ST2 predicts elevated SBP in the community. J. Hypertens. 2013, 31, 1431–1436. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Wollert, K.C.; Larson, M.G.; Coglianese, E.; McCabe, E.L.; Cheng, S.; Ho, J.E.; Fradley, M.G.; Ghorbani, A.; Xanthakis, V.; et al. Prognostic utility of novel biomarkers of cardiovascular stress: The Framingham Heart Study. Circulation 2012, 126, 1596–1604. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Zelnick, L.; Go, A.; Anderson, A.; Christenson, R.; Deo, R.; Defilippi, C.; Lash, J.; He, J.; Ky, B.; et al. Cardiac Biomarkers and Risk of Incident Heart Failure in Chronic Kidney Disease: The CRIC (Chronic Renal Insufficiency Cohort) Study. J. Am. Heart Assoc. 2019, 8, e012336. [Google Scholar] [CrossRef]
- Gerber, Y.; Weston, S.A.; Enriquez-Sarano, M.; Jaffe, A.S.; Manemann, S.M.; Jiang, R.; Roger, V.L. Contemporary Risk Stratification After Myocardial Infarction in the Community: Performance of Scores and Incremental Value of Soluble Suppression of Tumorigenicity-2. J. Am. Heart Assoc. 2017, 6, 5958. [Google Scholar] [CrossRef]
- Jenkins, W.S.; Roger, V.L.; Jaffe, A.S.; Weston, S.A.; AbouEzzeddine, O.F.; Jiang, R.; Manemann, S.M.; Enriquez-Sarano, M. Prognostic Value of Soluble ST2 After Myocardial Infarction: A Community Perspective. Am. J. Med. 2017, 130, 1112.e9–1112.e15. [Google Scholar] [CrossRef]
- Watson, C.J.; Tea, I.; O’Connell, E.; Glezeva, N.; Zhou, S.; James, S.; Gallagher, J.; Snider, J.; Januzzi, J.L.; Ledwidge, M.T.; et al. Comparison of longitudinal change in sST2 vs BNP to predict major adverse cardiovascular events in asymptomatic patients in the community. J. Cell. Mol. Med. 2020, 24, 6495–6499. [Google Scholar] [CrossRef]
- Hughes, M.F.; Appelbaum, S.; Havulinna, A.S.; Jagodzinski, A.; Zeller, T.; Kee, F.; Blankenberg, S.; Salomaa, V. ST2 may not be a useful predictor for incident cardiovascular events, heart failure and mortality. Heart 2014, 100, 1715–1721. [Google Scholar] [CrossRef] [PubMed]
- Suthahar, N.; Lau, E.S.; Blaha, M.J.; Paniagua, S.M.; Larson, M.G.; Psaty, B.M.; Benjamin, E.J.; Allison, M.A.; Bartz, T.M.; Januzzi, J.L.; et al. Sex-Specific Associations of Cardiovascular Risk Factors and Biomarkers With Incident Heart Failure. J. Am. Coll. Cardiol. 2020, 76, 1455–1465. [Google Scholar] [CrossRef]
- Watson, C.J.; Gallagher, J.; Wilkinson, M.; Russell-Hallinan, A.; Tea, I.; James, S.; O’reilly, J.; O’connell, E.; Zhou, S.; Ledwidge, M.; et al. Biomarker profiling for risk of future heart failure (HFpEF) development. J. Transl. Med. 2021, 19, 61. [Google Scholar] [CrossRef]
- Demyanets, S.; Kaun, C.; Pentz, R.; Krychtiuk, K.A.; Rauscher, S.; Pfaffenberger, S.; Zuckermann, A.; Aliabadi, A.; Gröger, M.; Maurer, G.; et al. Components of the interleukin-33/ST2 system are differentially expressed and regulated in human cardiac cells and in cells of the cardiac vasculature. J. Mol. Cell. Cardiol. 2013, 60, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Bartunek, J.; Delrue, L.; Van Durme, F.; Muller, O.; Casselman, F.; De Wiest, B.; Croes, R.; Verstreken, S.; Goethals, M.; de Raedt, H.; et al. Nonmyocardial Production of ST2 Protein in Human Hypertrophy and Failure Is Related to Diastolic Load. J. Am. Coll. Cardiol. 2008, 52, 2166–2174. [Google Scholar] [CrossRef] [PubMed]
- Defilippi, C.; Daniels, L.B.; Bayes-Genis, A. Structural Heart Disease and ST2: Cross-Sectional and Longitudinal Associations With Echocardiography. Am. J. Cardiol. 2015, 115, 59B–63B. [Google Scholar] [CrossRef] [PubMed]
- De La Espriella, R.; Bayés-Genis, A.; Revuelta-López, E.; Miñana, G.; Santas, E.; Llàcer, P.; García-Blas, S.; Fernández-Cisnal, A.; Bonanad, C.; Ventura, S.; et al. Soluble ST2 and Diuretic Efficiency in Acute Heart Failure and Concomitant Renal Dysfunction. J. Card. Fail. 2021, 27, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Henry-Okafor, Q.; Collins, S.P.; Jenkins, C.A.; Miller, K.F.; Maron, D.J.; Naftilan, A.J.; Weintraub, N.; Fermann, G.J.; McPherson, J.; Menon, S.; et al. Soluble ST2 as a Diagnostic and Prognostic Marker for Acute Heart Failure Syndromes. Open Biomarkers J. 2012, 5, 1–8. [Google Scholar] [CrossRef]
- Januzzi, J.L.; Peacock, W.F.; Maisel, A.S.; Chae, C.U.; Jesse, R.L.; Baggish, A.L.; O’Donoghue, M.; Sakhuja, R.; Chen, A.A.; van Kimmenade, R.R.; et al. Measurement of the Interleukin Family Member ST2 in Patients With Acute Dyspnea: Results From the PRIDE (Pro-Brain Natriuretic Peptide Investigation of Dyspnea in the Emergency Department) Study. J. Am. Coll. Cardiol. 2007, 50, 607–613. [Google Scholar] [CrossRef]
- Zhang, R.; Zhang, Y.; Zhang, J.; An, T.; Huang, Y.; Guo, X.; Januzzi, J.L.; Cappola, T.P.; Yin, S.; Wang, Y.; et al. The Prognostic Value of Plasma Soluble ST2 in Hospitalized Chinese Patients with Heart Failure. PLoS ONE 2014, 9, e110976. [Google Scholar] [CrossRef]
- Pascual-Figal, D.A.; Manzano-Fernández, S.; Boronat, M.; Casas, T.; Garrido, I.P.; Bonaque, J.C.; Pastor-Perez, F.; Valdés, M.; Januzzi, J.L. Soluble ST2, high-sensitivity troponin T- and N-terminal pro-B-type natriuretic peptide: Complementary role for risk stratification in acutely decompensated heart failure. Eur. J. Heart Fail. 2011, 13, 718–725. [Google Scholar] [CrossRef]
- Tang, W.W.; Wu, Y.; Grodin, J.L.; Hsu, A.P.; Hernandez, A.F.; Butler, J.; Metra, M.; Voors, A.A.; Felker, G.M.; Troughton, R.W.; et al. Prognostic Value of Baseline and Changes in Circulating Soluble ST2 Levels and the Effects of Nesiritide in Acute Decompensated Heart Failure. JACC Heart Fail. 2016, 4, 68–77. [Google Scholar] [CrossRef]
- Breidthardt, T.; Balmelli, C.; Twerenbold, R.; Mosimann, T.; Espinola, J.; Haaf, P.; Thalmann, G.; Moehring, B.; Mueller, M.; Meller, B.; et al. Heart Failure Therapy–Induced Early ST2 Changes May Offer Long-Term Therapy Guidance. J. Card. Fail. 2013, 19, 821–828. [Google Scholar] [CrossRef]
- Boisot, S.; Beede, J.; Isakson, S.; Chiu, A.; Clopton, P.; Januzzi, J.; Maisel, A.S.; Fitzgerald, R.L. Serial Sampling of ST2 Predicts 90-Day Mortality Following Destabilized Heart Failure. J. Card. Fail. 2008, 14, 732–738. [Google Scholar] [CrossRef]
- Aimo, A.; Vergaro, G.; Ripoli, A.; Bayes-Genis, A.; Figal, D.A.P.; de Boer, R.A.; Lassus, J.; Mebazaa, A.; Gayat, E.; Breidthardt, T.; et al. Meta-Analysis of Soluble Suppression of Tumorigenicity-2 and Prognosis in Acute Heart Failure. JACC Heart Fail. 2017, 5, 287–296. [Google Scholar] [CrossRef]
- Manzano-Fernández, S.; Mueller, T.; Pascual-Figal, D.; Truong, Q.A.; Januzzi, J.L. Usefulness of Soluble Concentrations of Interleukin Family Member ST2 as Predictor of Mortality in Patients With Acutely Decompensated Heart Failure Relative to Left Ventricular Ejection Fraction. Am. J. Cardiol. 2011, 107, 259–267. [Google Scholar] [CrossRef]
- Sugano, A.; Seo, Y.; Ishizu, T.; Sai, S.; Yamamoto, M.; Hamada-Harimura, Y.; Machino-Ohtsuka, T.; Obara, K.; Nishi, I.; Aonuma, K.; et al. Soluble ST2 and brain natriuretic peptide predict different mode of death in patients with heart failure and preserved ejection fraction. J. Cardiol. 2019, 73, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.B.; Kop, W.J.; Christenson, R.H.; Diercks, D.B.; Henderson, S.; Hanson, K.; Li, S.-Y.; Defilippi, C.R. Prognostic Utility of ST2 in Patients with Acute Dyspnea and Preserved Left Ventricular Ejection Fraction. Clin. Chem. 2011, 57, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Ky, B.; French, B.; McCloskey, K.; Rame, J.E.; McIntosh, E.; Shahi, P.; Dries, D.L.; Tang, W.W.; Wu, A.H.; Fang, J.C.; et al. High-Sensitivity ST2 for Prediction of Adverse Outcomes in Chronic Heart Failure. Circ. Heart Fail. 2011, 4, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Aimo, A.; Januzzi, J.L.; Vergaro, G.; Richards, A.M.; Lam, C.S.; Latini, R.; Anand, I.S.; Cohn, J.N.; Ueland, T.; Gullestad, L.; et al. Circulating levels and prognostic value of soluble ST2 in heart failure are less influenced by age than N-terminal pro-B-type natriuretic peptide and high-sensitivity troponin T. Eur. J. Heart Fail. 2020, 22, 2078–2088. [Google Scholar] [CrossRef] [PubMed]
- Emdin, M.; Aimo, A.; Vergaro, G.; Bayes-Genis, A.; Lupón, J.; Latini, R.; Meessen, J.; Anand, I.S.; Cohn, J.N.; Gravning, J.; et al. sST2 Predicts Outcome in Chronic Heart Failure Beyond NT−proBNP and High-Sensitivity Troponin T. J. Am. Coll. Cardiol. 2018, 72, 2309–2320. [Google Scholar] [CrossRef]
- Felker, G.M.; Fiuzat, M.; Thompson, V.; Shaw, L.K.; Neely, M.L.; Adams, K.F.; Whellan, D.J.; Donahue, M.P.; Ahmad, T.; Kitzman, D.W.; et al. Soluble ST2 in ambulatory patients with heart failure: Association with functional capacity and long-term outcomes. Circ. Heart Fail. 2013, 6, 1172–1179. [Google Scholar] [CrossRef]
- Broch, K.; Ueland, T.; Nymo, S.H.; Kjekshus, J.; Hulthe, J.; Muntendam, P.; McMurray, J.J.; Wikstrand, J.; Cleland, J.G.; Aukrust, P.; et al. Soluble ST2 is associated with adverse outcome in patients with heart failure of ischaemic aetiology. Eur. J. Heart Fail. 2012, 14, 268–277. [Google Scholar] [CrossRef]
- Najjar, E.; Faxén, U.L.; Hage, C.; Donal, E.; Daubert, J.-C.; Linde, C.; Lund, L.H. ST2 in heart failure with preserved and reduced ejection fraction. Scand. Cardiovasc. J. 2019, 53, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Fernández, S.; Januzzi, J.; Pastor-Pérez, F.; Bonaque-González, J.; Boronat-Garcia, M.; Pascual-Figal, D.; Montalban-Larrea, S.; Navarro-Peñalver, M.; Andreu-Cayuelas, J.; Valdés, M. Serial Monitoring of Soluble Interleukin Family Member ST2 in Patients with Acutely Decompensated Heart Failure. Cardiology 2012, 122, 158–166. [Google Scholar] [CrossRef]
- Huet, F.; Nicoleau, J.; Dupuy, A.; Curinier, C.; Breuker, C.; Castet-Nicolas, A.; Lotierzo, M.; Kalmanovich, E.; Zerkowski, L.; Akodad, M.; et al. STADE-HF (sST2 As a help for management of HF): A pilot study. ESC Heart Fail. 2020, 7, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Maisel, A.; Xue, Y.; van Veldhuisen, D.J.; Voors, A.A.; Jaarsma, T.; Pang, P.S.; Butler, J.; Pitt, B.; Clopton, P.; de Boer, R.A. Effect of Spironolactone on 30-Day Death and Heart Failure Rehospitalization (from the COACH Study). Am. J. Cardiol. 2014, 114, 737–742. [Google Scholar] [CrossRef] [PubMed]
- van Vark, L.C.; Lesman-Leegte, I.; Baart, S.J.; Postmus, D.; Pinto, Y.M.; Orsel, J.G.; Westenbrink, B.D.; Rocca, H.P.B.-L.; van Miltenburg, A.J.; Boersma, E.; et al. Prognostic Value of Serial ST2 Measurements in Patients With Acute Heart Failure. J. Am. Coll. Cardiol. 2017, 70, 2378–2388. [Google Scholar] [CrossRef]
- Januzzi, J.L.; Mebazaa, A.; Di Somma, S. ST2 and Prognosis in Acutely Decompensated Heart Failure: The International ST2 Consensus Panel. Am. J. Cardiol. 2015, 115, 26B–31B. [Google Scholar] [CrossRef]
- Aimo, A.; Maisel, A.S.; Castiglione, V.; Emdin, M. sST2 for Outcome Prediction in Acute Heart Failure: Which Is the Best Cutoff? J. Am. Coll. Cardiol. 2019, 74, 478–479. [Google Scholar] [CrossRef]
- Zach, V.; Bähr, F.L.; Edelmann, F. Suppression of Tumourigenicity 2 in Heart Failure With Preserved Ejection Fraction. Card. Fail. Rev. 2020, 6, 1–7. [Google Scholar] [CrossRef]
- Sanders-van Wijk, S.; van Empel, V.; Davarzani, N.; Maeder, M.T.; Handschin, R.; Pfisterer, M.E.; Brunner-La Rocca, H.-P. TIME-CHF investigators. Circulating biomarkers of distinct pathophysiological pathways in heart failure with preserved vs. reduced left ventricular ejection fraction. Eur. J. Heart Fail. 2015, 17, 1006–1014. [Google Scholar] [CrossRef]
- Cunningham, J.W.; Claggett, B.L.; O’meara, E.; Prescott, M.F.; Pfeffer, M.A.; Shah, S.J.; Redfield, M.M.; Zannad, F.; Chiang, L.-M.; Rizkala, A.R.; et al. Effect of Sacubitril/Valsartan on Biomarkers of Extracellular Matrix Regulation in Patients With HFpEF. J. Am. Coll. Cardiol. 2020, 76, 503–514. [Google Scholar] [CrossRef]
- Januzzi, J.L.; Myhre, P.L. The Challenges of NT-proBNP Testing in HFpEF: Shooting Arrows in the Wind. JACC Heart Fail. 2020, 8, 382–385. [Google Scholar] [CrossRef]
- Felker, G.M.; Anstrom, K.J.; Adams, K.F.; Ezekowitz, J.A.; Fiuzat, M.; Houston-Miller, N.; Januzzi, J.L.; Mark, D.B.; Piña, I.L.; Passmore, G.; et al. Effect of Natriuretic Peptide-Guided Therapy on Hospitalization or Cardiovascular Mortality in High-Risk Patients With Heart Failure and Reduced Ejection Fraction: A Randomized Clinical Trial. JAMA 2017, 318, 713–720. [Google Scholar] [CrossRef]
- Stienen, S.; Salah, K.; Moons, A.H.; Bakx, A.L.; van Pol, P.; Kortz, R.A.M.; Ferreira, J.P.; Marques, I.; Schroeder-Tanka, J.M.; Keijer, J.T.; et al. NT-proBNP (N-Terminal pro-B-Type Natriuretic Peptide)-Guided Therapy in Acute Decompensated Heart Failure: PRIMA II Randomized Controlled Trial (Can NT-ProBNP-Guided Therapy During Hospital Admission for Acute Decompensated Heart Failure Reduce Mortality and Readmissions?). Circulation 2018, 137, 1671–1683. [Google Scholar]
- Beetler, D.J.; Bruno, K.A.; Di Florio, D.N.; Douglass, E.J.; Shrestha, S.; Tschöpe, C.; Cunningham, M.W.; Krejčí, J.; Bienertová-Vašků, J.; Pankuweit, S.; et al. Sex and age differences in sST2 in cardiovascular disease. Front. Cardiovasc. Med. 2023, 9, 1073814. [Google Scholar] [CrossRef]
- Bayes-Genis, A.; Zamora, E.; de Antonio, M.; Galán, A.; Vila, J.; Urrutia, A.; Díez, C.; Coll, R.; Altimir, S.; Lupón, J. Soluble ST2 Serum Concentration and Renal Function in Heart Failure. J. Card. Fail. 2013, 19, 768–775. [Google Scholar] [CrossRef]
- Shi, Y.; Liu, J.; Liu, C.; Shuang, X.; Yang, C.; Qiao, W.; Dong, G. Diagnostic and prognostic value of serum soluble suppression of tumorigenicity-2 in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2022, 9, 937291. [Google Scholar] [CrossRef]
- Friões, F.; Lourenço, P.; Laszczynska, O.; Almeida, P.-B.; Guimarães, J.-T.; Januzzi, J.L.; Azevedo, A.; Bettencourt, P. Prognostic value of sST2 added to BNP in acute heart failure with preserved or reduced ejection fraction. Clin. Res. Cardiol. 2015, 104, 491–499. [Google Scholar] [CrossRef]
- Bayes-Genis, A.; de Antonio, M.; Galán, A.; Sanz, H.; Urrutia, A.; Cabanes, R.; Cano, L.; González, B.; Díez, C.; Pascual, T.; et al. Combined use of high-sensitivity ST2 and NTproBNP to improve the prediction of death in heart failure. Eur. J. Heart Fail. 2012, 14, 32–38. [Google Scholar] [CrossRef]
- Pascual-Figal, D.A.; Ordoñez-Llanos, J.; Tornel, P.L.; Vázquez, R.; Puig, T.; Valdés, M.; Cinca, J.; de Luna, A.B.; Bayes-Genis, A.; MUSIC Investigators. Soluble ST2 for Predicting Sudden Cardiac Death in Patients With Chronic Heart Failure and Left Ventricular Systolic Dysfunction. J. Am. Coll. Cardiol. 2009, 54, 2174–2179. [Google Scholar] [CrossRef]
- Lupón, J.; Simpson, J.; McMurray, J.J.; de Antonio, M.; Vila, J.; Subirana, I.; Barallat, J.; Moliner, P.; Domingo, M.; Zamora, E.; et al. Barcelona Bio-HF Calculator Version 2.0: Incorporation of angiotensin II receptor blocker neprilysin inhibitor (ARNI) and risk for heart failure hospitalization. Eur. J. Heart Fail. 2018, 20, 938–940. [Google Scholar] [CrossRef]
- Aimo, A.; Vergaro, G.; Passino, C.; Ripoli, A.; Ky, B.; Miller, W.L.; Bayes-Genis, A.; Anand, I.; Januzzi, J.L.; Emdin, M. Prognostic Value of Soluble Suppression of Tumorigenicity-2 in Chronic Heart Failure: A Meta-Analysis. JACC Heart Fail. 2017, 5, 280–286. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author | Patients | Type of Cohort | Results |
|---|---|---|---|
| Wang et al. [33] | 3428 | Asymptomatic community-based population | sST2 was associated with the risk of developing HF (HR per 1 SD 1.45; 95% CI 1.23–1.70; p < 0.001). |
| Bansal et al. [34] | 3314 | CKD population | sST2 was associated with the risk of developing HF (HR per 1 SD 1.19; 95% CI, 1.05–1.35), in particular with preserved ejection fraction (HR = 1.27; 95% CI, 1.07–1.51). |
| Watson et al. [37] | 282 | Asymptomatic community-based population | The sST2 increase from baseline to follow up led to an increased risk of incident MACE by approximately 7.9%. |
| Hughes et al. [38] | 844 | Asymptomatic community-based population | sST2 did not improve long-term prediction of CV event, including HF (HR per 1 SD 1.06; 95% CI = 0.96–1.17). |
| Suthahar et al. [39] | 22,756 | Asymptomatic community-based population | sST2 levels were not significantly associated with incident HF in either women or men (HR per 1 SD in women 1.12; 95% CI 1.02–1.22; HR in men 1.08; 95% CI 1.02–1.22; p for interaction 0.40). |
| Authors | HF Setting | Patients | Mean/Median Age (Years) | Mean LVEF (%) | Follow-Up Duration | Results |
|---|---|---|---|---|---|---|
| Januzzi et al. [46] | AHF | 593 | NA | NA | 1 year | sST2 concentration ≥0.20 ng/mL strongly predicted death at 1 year (HR 9.3, 95% CI 1.3–17.8; p = 0.03). |
| Zhang et al. [47] | AHF | 1528 | 58 | 40 | 573 days | Concentrations of sST2 were elevated among patients with all-cause death and cardiac transplantation (33.6% vs. 55.6%, p < 0.001). |
| Pascual-Figal et al. [48] | AHF | 107 | 72 | 47 | 739 days | sST2 concentrations were higher in patients who died (HR per 10 ng/mL 1.09, 95% CI 1.03–1.15, p = 0.005 in multivariable analysis). |
| Tang et al. [49] | AHF | 858 | 66 | 26 | 180 days | Higher sST2 levels were associated with an increased mortality risk at 180 days (baseline sST2 value: HR per log increase 2.21 (95% CI 1.57–3.13); follow-up sST2 value: HR 2.64 (95% CI 1.82–3.84, both p < 0.001)). |
| Breidthardt et al. [50] | AHF | 207 | 80 | 40 | 368 days | sST2 decreased significantly during the first 48 h in survivors compared with non-survivors, and early sST2 changes independently predicted 1-year mortality (HR 1.07 for every increase of 10%; p = 0.02). |
| Boisot et al. [51] | AHF | 150 | NA | NA | 90 days | Patients whose sST2 values decreased by 15.5% or more during the study period had a 7% lower chance of death compared to those whose sST2 levels failed to decrease. |
| Aimo et al. [52] | AHF | 4835 | NA | NA | 405 days | Both admission and discharge sST2 were predictive of all-cause death and CV death, while discharge sST2 predicted rehospitalization for HF. |
| Manzano-Fernández et al. [53] | AHF | 447 | 73 | 46 | 1 year | Elevated sST2 concentrations were associated with a greater mortality risk in HFpEF (HR 1.41 per ng/mL, 95% CI 1.14–1.76, p = 0.002) and HFrEF (HR 1.20 per ng/mL, 95% CI 1.10–1.32, p < 0.001). |
| Sugano et al. [54] | AHF | 191 | 76 | 60 | 445 days | sST2 concentrations were associated with all-cause death, CV death and non-CV death. |
| Shah et al. [55] | AHF | 387 | 58 | NA | 1 year | sST2 was predictive of mortality (HR per log 2.14, 95% CI 1.37–3.38, p < 0.001). |
| Ky et al. [56] | CHF | 1141 | 56 | 32 | 2.8 years | Patients with sST2 >36.3 ng/mL had a markedly increased risk of adverse outcomes (adjusted HR 1.9; 95% CI:1.3–2.9; p = 0.002). |
| Aimo et al. [57] | CHF | 5301 | 66 | 28 | 5 years | sST2 independently predicted 1- and 5-year all-cause and CV deaths, and 1-,3-, 6-, and 12-month HF hospitalizations. |
| Emdin et al. [58] | CHF | 4268 | 68 | NA | 2.4 years | The risk of all-cause death, CV death, and HF hospitalization increased by 26%, 25%, and 30%, respectively, per each doubling of sST2. |
| Felker et al. [59] | CHF | 910 | 59 | 24 | 1 year | sST2 was significantly associated with death or HF hospitalization, CV death or HF hospitalization, and all-cause mortality. |
| Broch et al. [60] | CHF | 1449 | 72 | 32 | 2.6 years | sST2 was significantly associated with CV death, non-fatal MI and stroke (HR per unit 1.99; 95% CI 1.68–2.36; p < 0.001). |
| Najjar et al. [61] | CHF | 86 | 73 | 70 | 522 days | Among HFpEF, sST2 was associated with death and HF hospitalization (HR per log increase 6.62, 95% CI 1.04–42.28, p = 0.046). |
| Authors | HF Setting | Patients | Biomarkers | Results |
|---|---|---|---|---|
| Januzzi et al. [46] | AHF | 593 | sST2 and NT-proBNP | Combination of sST2 and NT-proBNP more accurately predicted death (AUC 0.80) than the single biomarker assessment (AUC 0.72 and 0.74, respectively, both p < 0.001). |
| Zhang et al. [47] | AHF | 1528 | sST2 and NT-proBNP | Combination of sST2 and NT-proBNP more accurately predicted all causes of death and transplantation at 1 month (AUC 0.84) than the single biomarker assessment (AUC 0.79 for NT-proBNP and AUC 0.82 for sST2). |
| Tang et al. [49] | AHF | 858 | sST2 and NT-proBNP | Adding 48 to 72 h of follow-up sST2 to the ASCEND-HF risk model, plus follow-up NT-proBNP, correctly reclassified 15.6% of subjects for the 180-day death endpoint. |
| Friões et al. [77] | AHF | 195 | sST2 and BNP | Net reclassification index after adding BNP to sST2 concentrations was 0.70 (p < 0.001) in patients with HFrEF and 0.31 (p = 0.21) in patients with HFpEF. |
| Pascual-Figal et al. [48] | AHF | 107 | sST2, NT-proBNP and hs-TnT | For each elevated marker (from 0 to 3), an adjusted analysis suggested a tripling of the risk of death (for each elevated marker, HR 2.64, 95% CI 1.63–4.28, p < 0.001). |
| Ky et al. [56] | CHF | 1141 | sST2 and NT-proBNP | Combination of sST2 and NT-proBNP more accurately predicted death and cardiac transplantation (AUC 0.80) than the single biomarker assessment (AUC 0.75 and AUC 0.77, respectively). The addition of sST2 and NT-proBNP reclassified 14.9% of patients into more appropriate risk groups. |
| Bayes-Genis et al. [78] | CHF | 891 | sST2 and NT-proBNP | Patients with elevated concentrations of both sST2 and NT-proBNP had a markedly increased risk of all-cause death (HR 6.38, 95% CI 4.67–9.25, p < 0.001). |
| Pascual-Figal et al. [79] | CHF | 99 | sST2 and NT-proBNP | The presence of both elevated NT-proBNP and sST2 (OR 37.3, 95% CI 4.0–350; p = 0.002) was more predictive of SCD than evaluating each biomarker separately. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccardi, M.; Myhre, P.L.; Zelniker, T.A.; Metra, M.; Januzzi, J.L.; Inciardi, R.M. Soluble ST2 in Heart Failure: A Clinical Role beyond B-Type Natriuretic Peptide. J. Cardiovasc. Dev. Dis. 2023, 10, 468. https://doi.org/10.3390/jcdd10110468
Riccardi M, Myhre PL, Zelniker TA, Metra M, Januzzi JL, Inciardi RM. Soluble ST2 in Heart Failure: A Clinical Role beyond B-Type Natriuretic Peptide. Journal of Cardiovascular Development and Disease. 2023; 10(11):468. https://doi.org/10.3390/jcdd10110468
Chicago/Turabian StyleRiccardi, Mauro, Peder L. Myhre, Thomas A. Zelniker, Marco Metra, James L. Januzzi, and Riccardo M. Inciardi. 2023. "Soluble ST2 in Heart Failure: A Clinical Role beyond B-Type Natriuretic Peptide" Journal of Cardiovascular Development and Disease 10, no. 11: 468. https://doi.org/10.3390/jcdd10110468