

Diagnosis and Management of Atrial Fibrillation in Acute Ischemic Stroke in the Setting of Reperfusion Therapy: Insights and Strategies for Optimized Care


Abstract
:1. Introduction
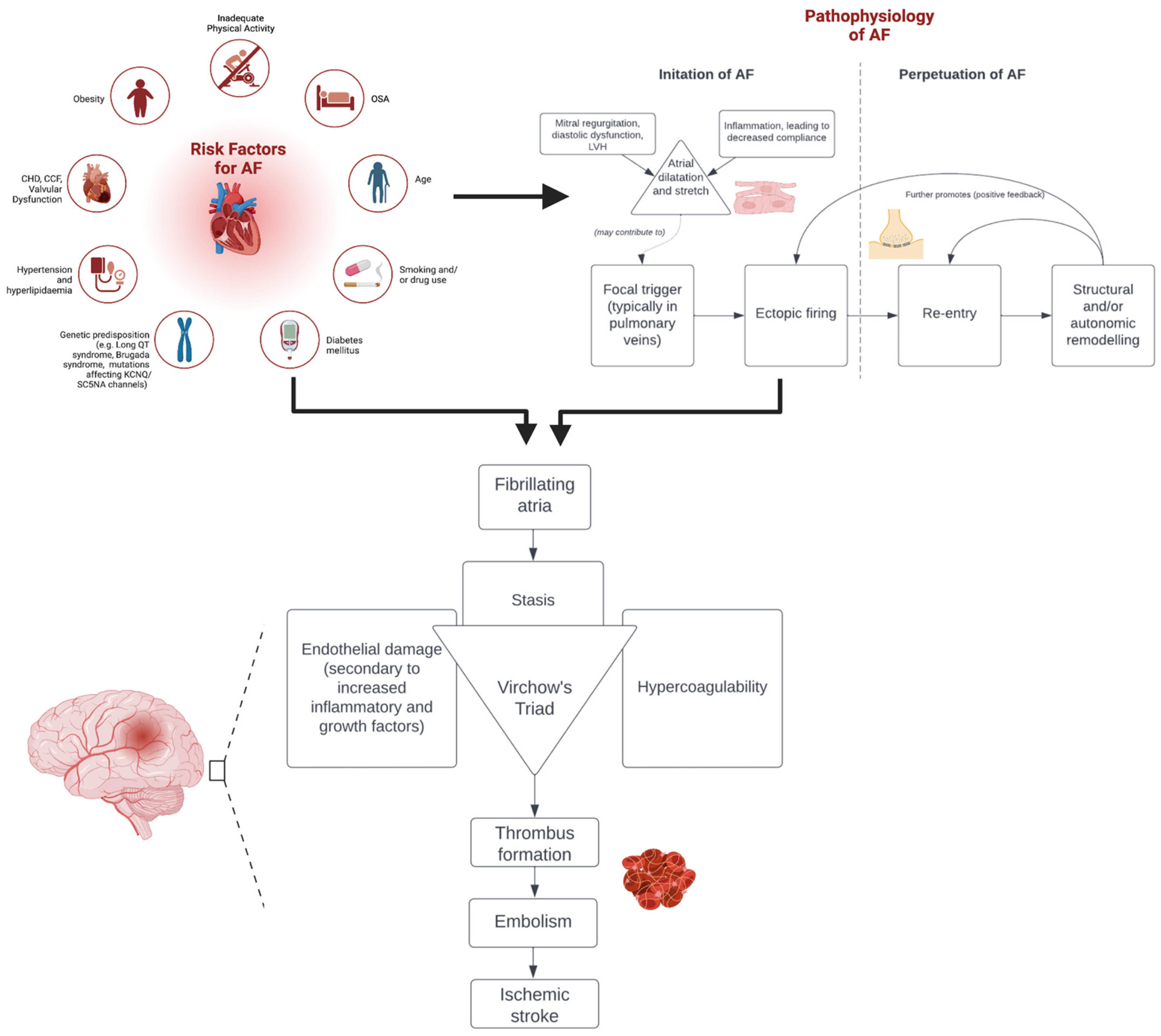
2. Link between Atrial Fibrillation and Acute Ischemic Stroke
3. Diagnostic and Therapeutic Management of Atrial Fibrillation
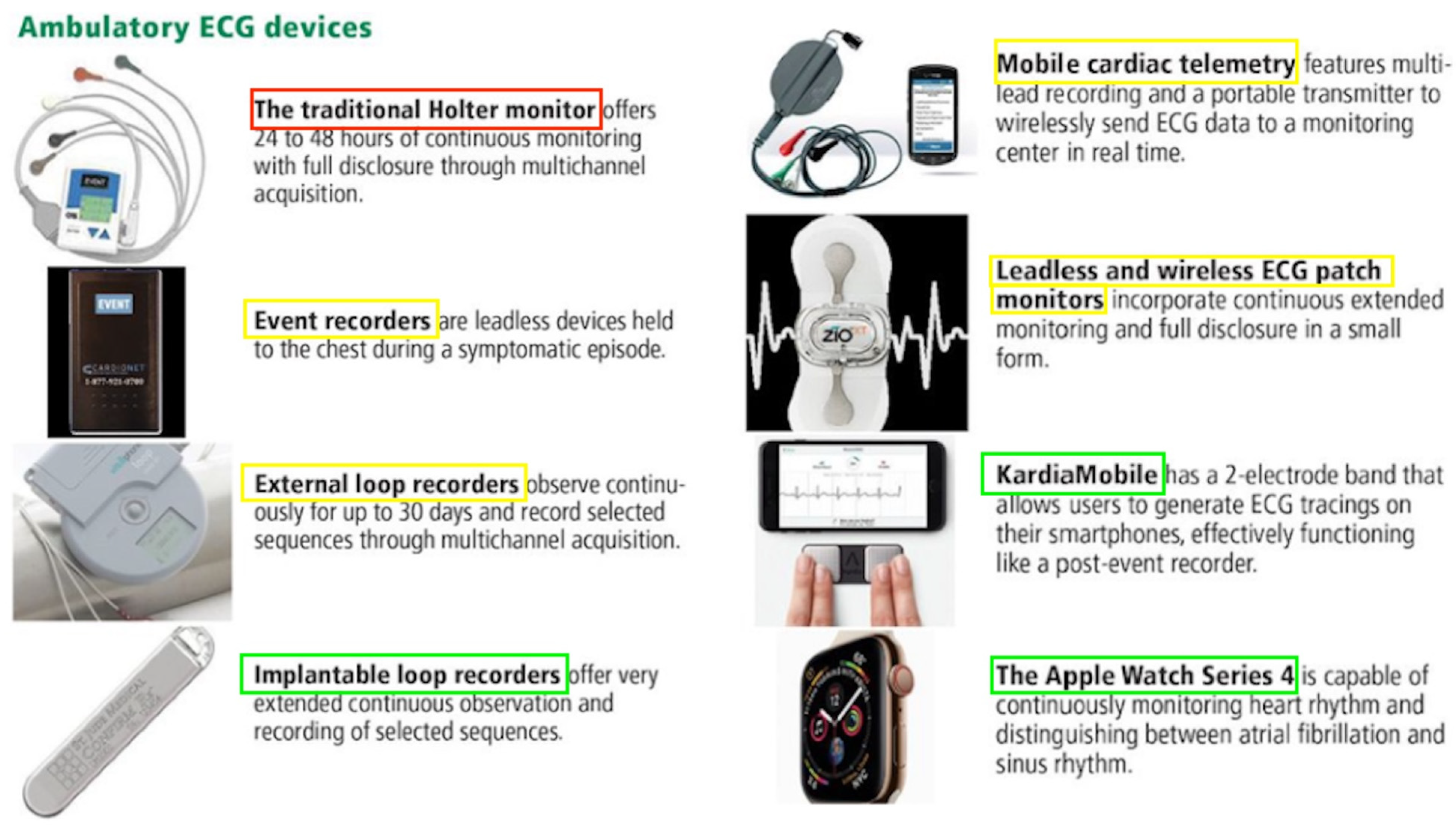
3.1. Diagnosis of Atrial Fibrillation
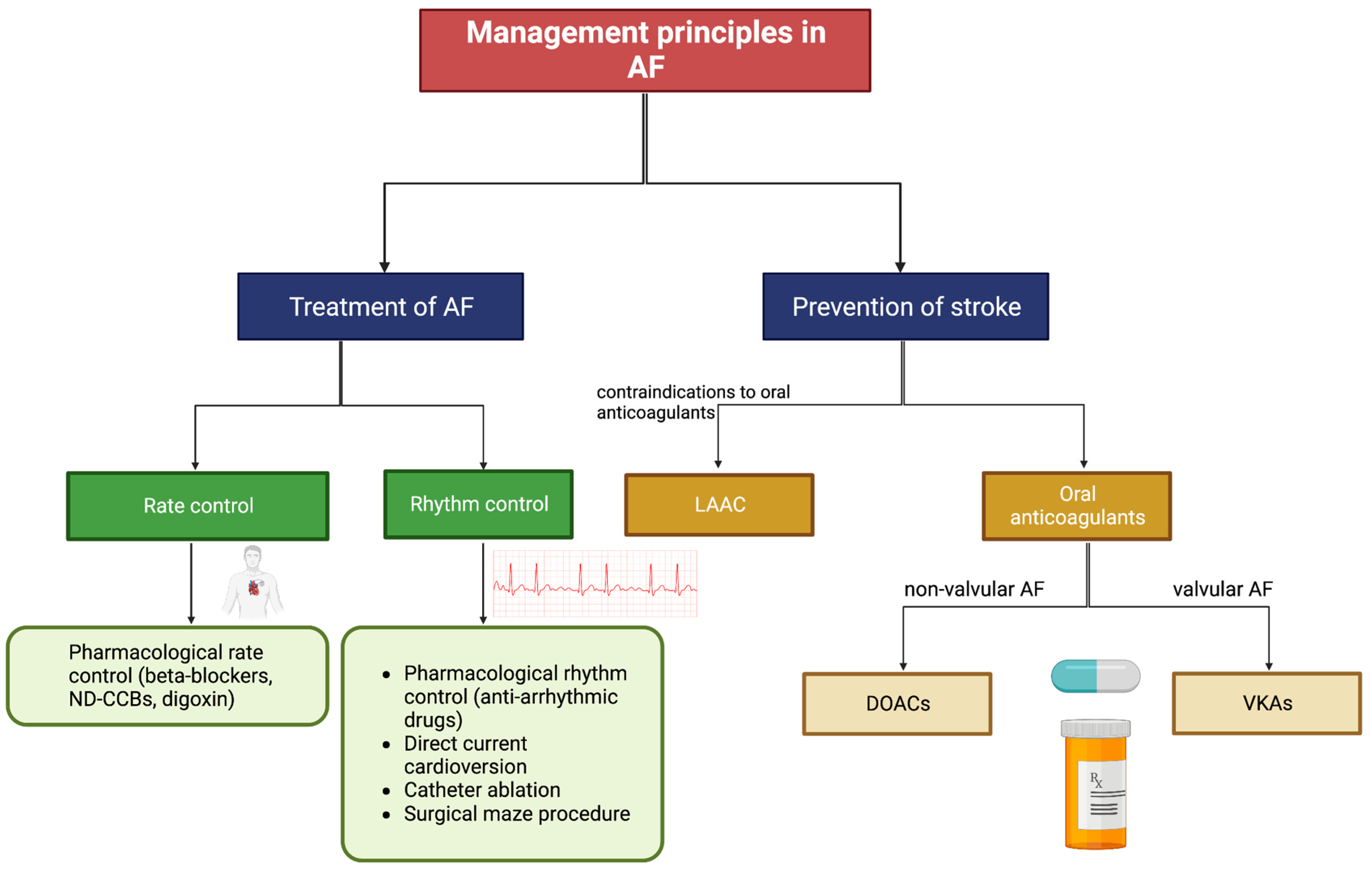
3.2. Treatment of Atrial Fibrillation
4. Impact of Atrial Fibrillation on Stroke Outcomes
5. Reperfusion Therapy in Acute Ischemic Stroke
5.1. Impact of Atrial Fibrillation on Outcomes after Intravenous Thrombolysis
5.2. Impact of Atrial Fibrillation on Outcomes after Endovascular Thrombectomy
6. Discussion
6.1. Limitations
6.2. Policy Recommendations
- Conducting an RCT that investigates how AF influences outcomes after reperfusion therapy since current data is primarily based on cohort studies. For RCTs investigating other hypotheses in AIS patients receiving reperfusion therapy, we strongly recommend that effort is made to ensure a standardised protocol for diagnosing AF and that the prevalence of different AF subtypes is reported where possible;
- Further trials that investigate how AF influences outcomes following BT. Despite being an increasingly contested field, the current lack of data prevents concrete conclusions from being drawn;
- Greater implementation of technologies for the detection of AF following AIS. Given that the prevalence of AF is highest in EVT cohorts, this may justify a greater allocation of resources toward these centres;
- Conduct cost-effectiveness analyses across a range of cardiac monitoring devices, including mobile cardiac outpatient telemetry (MCOT), implantable loop recorders, and wearable devices. Use this to guide policy on the most suitable protocol for diagnosing AF following AIS. In particular, research the efficacy of utilising MCOT for the first 30 days post-stroke followed by long-term monitoring with implantable loop recorders in patients with ischemic stroke of undetermined origin;
- Whilst long-term cardiac monitoring has been shown to be effective in AF detection, further research is required to investigate the clinical benefits of widespread AF screening;
- Further studies on the prevalence of AF in developing and under-resourced parts of the world. There is currently an alarming deficiency of AF-related research in these regions;
- Increase the awareness of AF among healthcare workers and the general population. Provide education programs among primary healthcare workers for the early detection of AF. Even interventions as simple as routine 30 s pulse checks and opportunistic ECG recordings may be highly useful without significant cost. To facilitate primary prevention of AF, provide funding for community-based activities that raise awareness about AF, and link AF with stroke awareness campaigns.
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| IVT | Intravenous thrombolysis |
| EVT | Endovascular thrombectomy |
| AIS | Acute ischemic stroke |
| AF | Atrial fibrillation |
| TIA | Transient ischemic attack |
| ECG | Electrocardiogram |
| OAC | Oral anticoagulant |
| ICM | Insertable cardiac monitor |
| ECM | External cardiac monitor |
| PPG | Photoplethysmography |
| VKA | Vitamin K antagonist |
| DOAC | Direct-acting oral anticoagulant |
| HT | Haemorrhagic transformation |
| AHA | American Heart Association |
| ASA | American Stroke Association |
| RCT | Randomised controlled trial |
| KAF | Known atrial fibrillation |
| AFDAS | Atrial fibrillation diagnosed after stroke |
| OR | Odds ratio |
| mRS | Modified Rankin Scale |
| sICH | Symptomatic intracerebral haemorrhage |
| INR | International normalised ratio |
| NIHSS | National Institutes of Health Stroke Scale |
| BT | Bridging therapy |
| CHF | Congestive heart failure |
| LAE | Left atrial enlargement |
| MCOT | Mobile cardiac outpatient telemetry |
References
- Li, H.; Song, X.; Liang, Y.; Bai, X.; Liu-Huo, W.S.; Tang, C.; Chen, W.; Zhao, L. Global, regional, and national burden of disease study of atrial fibrillation/flutter, 1990–2019: Results from a global burden of disease study, 2019. BMC Public Health 2022, 22, 2015. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Chen, Y.; Lin, R.; Huang, W.; Zhou, H.; Lin, Y.; Xu, M. Burden of atrial fibrillation and its attributable risk factors from 1990 to 2019: An analysis of the Global Burden of Disease study 2019. Front. Cardiovasc. Med. 2022, 9, 997698. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Choi, E.K.; Han, K.D.; Lee, H.; Choe, W.S.; Lee, S.R.; Cha, M.J.; Lim, W.H.; Kim, Y.J.; Oh, S. Mortality and causes of death in patients with atrial fibrillation: A nationwide population-based study. PLoS ONE 2018, 13, e0209687. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge. Int. J. Stroke 2021, 16, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Brundel, B.; Ai, X.; Hills, M.T.; Kuipers, M.F.; Lip, G.Y.H.; de Groot, N.M.S. Atrial fibrillation. Nat. Rev. Dis. Primers 2022, 8, 21. [Google Scholar] [CrossRef]
- Streur, M.; Ratcliffe, S.J.; Ball, J.; Stewart, S.; Riegel, B. Symptom Clusters in Adults With Chronic Atrial Fibrillation. J. Cardiovasc. Nurs. 2017, 32, 296–303. [Google Scholar] [CrossRef]
- Aune, D.; Mahamat-Saleh, Y.; Kobeissi, E.; Feng, T.; Heath, A.K.; Janszky, I. Blood pressure, hypertension and the risk of atrial fibrillation: A systematic review and meta-analysis of cohort studies. Eur. J. Epidemiol. 2023, 38, 145–178. [Google Scholar] [CrossRef]
- Atar, D.; Berge, E.; Le Heuzey, J.Y.; Virdone, S.; Camm, A.J.; Steffel, J.; Gibbs, H.; Goldhaber, S.Z.; Goto, S.; Kayani, G.; et al. The association between patterns of atrial fibrillation, anticoagulation, and cardiovascular events. Europace 2020, 22, 195–204. [Google Scholar] [CrossRef]
- Kamel, H.; Okin, P.M.; Elkind, M.S.; Iadecola, C. Atrial Fibrillation and Mechanisms of Stroke: Time for a New Model. Stroke 2016, 47, 895–900. [Google Scholar] [CrossRef]
- Hald, E.M.; Rinde, L.B.; Løchen, M.L.; Mathiesen, E.B.; Wilsgaard, T.; Njølstad, I.; Brækkan, S.K.; Hansen, J.B. Atrial Fibrillation and Cause-Specific Risks of Pulmonary Embolism and Ischemic Stroke. J. Am. Heart Assoc. 2018, 7, e006502. [Google Scholar] [CrossRef]
- Sposato, L.A.; Cipriano, L.E.; Saposnik, G.; Ruíz Vargas, E.; Riccio, P.M.; Hachinski, V. Diagnosis of atrial fibrillation after stroke and transient ischaemic attack: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Vinding, N.E.; Kristensen, S.L.; Rørth, R.; Butt, J.H.; Østergaard, L.; Olesen, J.B.; Torp-Pedersen, C.; Gislason, G.H.; Køber, L.; Kruuse, C.; et al. Ischemic Stroke Severity and Mortality in Patients With and Without Atrial Fibrillation. J. Am. Heart Assoc. 2022, 11, e022638. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [CrossRef] [PubMed]
- Staerk, L.; Sherer, J.A.; Ko, D.; Benjamin, E.J.; Helm, R.H. Atrial Fibrillation: Epidemiology, Pathophysiology, and Clinical Outcomes. Circ. Res. 2017, 120, 1501–1517. [Google Scholar] [CrossRef]
- Gersh, B.J.; Tsang, T.S.M.; Barnes, M.E.; Seward, J.B. The changing epidemiology of non-valvular atrial fibrillation: The role of novel risk factors. Eur. Heart J. Suppl. 2005, 7, C5–C11. [Google Scholar] [CrossRef]
- Iwasaki, Y.K.; Nishida, K.; Kato, T.; Nattel, S. Atrial fibrillation pathophysiology: Implications for management. Circulation 2011, 124, 2264–2274. [Google Scholar] [CrossRef]
- Romero, J.; Cao, J.J.; Garcia, M.J.; Taub, C.C. Cardiac imaging for assessment of left atrial appendage stasis and thrombosis. Nat. Rev. Cardiol. 2014, 11, 470–480. [Google Scholar] [CrossRef]
- Singer, D.E.; Ziegler, P.D.; Koehler, J.L.; Sarkar, S.; Passman, R.S. Temporal Association Between Episodes of Atrial Fibrillation and Risk of Ischemic Stroke. JAMA Cardiol. 2021, 6, 1364–1369. [Google Scholar] [CrossRef]
- Lip, G.Y.; Lane, D.A. Stroke prevention in atrial fibrillation: A systematic review. JAMA 2015, 313, 1950–1962. [Google Scholar] [CrossRef]
- Chua, S.K.; Chen, L.C.; Lien, L.M.; Lo, H.M.; Liao, Z.Y.; Chao, S.P.; Chuang, C.Y.; Chiu, C.Z. Comparison of Arrhythmia Detection by 24-Hour Holter and 14-Day Continuous Electrocardiography Patch Monitoring. Acta Cardiol. Sin. 2020, 36, 251–259. [Google Scholar] [CrossRef]
- Liu, C.M.; Chang, S.L.; Yeh, Y.H.; Chung, F.P.; Hu, Y.F.; Chou, C.C.; Hung, K.C.; Chang, P.C.; Liao, J.N.; Chan, Y.H.; et al. Enhanced detection of cardiac arrhythmias utilizing 14-day continuous ECG patch monitoring. Int. J. Cardiol. 2021, 332, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Wozakowska-Kapłon, B. Changes in left atrial size in patients with persistent atrial fibrillation: A prospective echocardiographic study with a 5-year follow-up period. Int. J. Cardiol. 2005, 101, 47–52. [Google Scholar] [CrossRef]
- Force, U.P.S.T.; Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Epling, J.W., Jr.; et al. Screening for Atrial Fibrillation: US Preventive Services Task Force Recommendation Statement. JAMA 2022, 327, 360–367. [Google Scholar] [CrossRef]
- Brieger, D.; Amerena, J.; Attia, J.; Bajorek, B.; Chan, K.H.; Connell, C.; Freedman, B.; Ferguson, C.; Hall, T.; Haqqani, H.; et al. National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand: Australian Clinical Guidelines for the Diagnosis and Management of Atrial Fibrillation 2018. Heart Lung Circ. 2018, 27, 1209–1266. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Tan, S.Y.; Wang, J.K.; Li, J.; Tu, T.M.; Tan, V.H.; Yeo, C. A meta-analysis of extended ECG monitoring in detection of atrial fibrillation in patients with cryptogenic stroke. Open Heart 2022, 9, e002081. [Google Scholar] [CrossRef]
- Tsivgoulis, G.; Triantafyllou, S.; Palaiodimou, L.; Grory, B.M.; Deftereos, S.; Köhrmann, M.; Dilaveris, P.; Ricci, B.; Tsioufis, K.; Cutting, S.; et al. Prolonged Cardiac Monitoring and Stroke Recurrence: A Meta-analysis. Neurology 2022, 98, e1942–e1952. [Google Scholar] [CrossRef]
- Boriani, G.; Auricchio, A.; Botto, G.L.; Joseph, J.M.; Roberts, G.J.; Grammatico, A.; Nabutovsky, Y.; Piccini, J.P. Insertable cardiac monitoring results in higher rates of atrial fibrillation diagnosis and oral anticoagulation prescription after ischaemic stroke. Europace 2023, 25, euad212. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, P.D.; Rogers, J.D.; Ferreira, S.W.; Nichols, A.J.; Richards, M.; Koehler, J.L.; Sarkar, S. Long-term detection of atrial fibrillation with insertable cardiac monitors in a real-world cryptogenic stroke population. Int. J. Cardiol. 2017, 244, 175–179. [Google Scholar] [CrossRef]
- Ungar, A.; Pescini, F.; Rafanelli, M.; De Angelis, M.V.; Faustino, M.; Tomaselli, C.; Petrone, A.; Forleo, G.; Morani, G.; Forlivesi, S.; et al. Detection of subclinical atrial fibrillation after cryptogenic stroke using implantable cardiac monitors. Eur. J. Intern. Med. 2021, 92, 86–93. [Google Scholar] [CrossRef]
- Yaghi, S.; Ryan, M.P.; Gunnarsson, C.L.; Irish, W.; Rosemas, S.C.; Neisen, K.; Ziegler, P.D.; Reynolds, M.R. Longitudinal outcomes in cryptogenic stroke patients with and without long-term cardiac monitoring for atrial fibrillation. Heart Rhythm O2 2022, 3, 223–230. [Google Scholar] [CrossRef]
- Tsivgoulis, G.; Katsanos, A.H.; Grory, B.M.; Köhrmann, M.; Ricci, B.A.; Tsioufis, K.; Cutting, S.; Krogias, C.; Schellinger, P.D.; Campello, A.R.; et al. Prolonged Cardiac Rhythm Monitoring and Secondary Stroke Prevention in Patients With Cryptogenic Cerebral Ischemia. Stroke 2019, 50, 2175–2180. [Google Scholar] [CrossRef] [PubMed]
- Vitolo, M.; Imberti, J.F.; Maisano, A.; Albini, A.; Bonini, N.; Valenti, A.C.; Malavasi, V.L.; Proietti, M.; Healey, J.S.; Lip, G.Y.; et al. Device-detected atrial high rate episodes and the risk of stroke/thrombo-embolism and atrial fibrillation incidence: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 100–106. [Google Scholar] [CrossRef]
- Lopez Perales, C.R.; Van Spall, H.G.C.; Maeda, S.; Jimenez, A.; Laţcu, D.G.; Milman, A.; Kirakoya-Samadoulougou, F.; Mamas, M.A.; Muser, D.; Casado Arroyo, R. Mobile health applications for the detection of atrial fibrillation: A systematic review. Europace 2021, 23, 11–28. [Google Scholar] [CrossRef]
- Skrebelyte-Strøm, L.; Rønning, O.M.; Dahl, F.A.; Steine, K.; Kjekshus, H. Prediction of occult atrial fibrillation in patients after cryptogenic stroke and transient ischaemic attack: PROACTIA. Europace 2022, 24, 1881–1888. [Google Scholar] [CrossRef]
- Santana Baskar, P.; Cordato, D.; Wardman, D.; Bhaskar, S. In-hospital acute stroke workflow in acute stroke—Systems-based approaches. Acta Neurol. Scand. 2021, 143, 111–120. [Google Scholar] [CrossRef]
- Chowdhury, S.Z.; Baskar, P.S.; Bhaskar, S. Effect of prehospital workflow optimization on treatment delays and clinical outcomes in acute ischemic stroke: A systematic review and meta-analysis. Acad. Emerg. Med. 2021, 28, 781–801. [Google Scholar] [CrossRef]
- Sanders, D.; Ungar, L.; Eskander, M.A.; Seto, A.H. Ambulatory ECG monitoring in the age of smartphones. Cleve. Clin. J. Med. 2019, 86, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Lubitz, S.A.; Faranesh, A.Z.; Selvaggi, C.; Atlas, S.J.; McManus, D.D.; Singer, D.E.; Pagoto, S.; McConnell, M.V.; Pantelopoulos, A.; Foulkes, A.S. Detection of Atrial Fibrillation in a Large Population Using Wearable Devices: The Fitbit Heart Study. Circulation 2022, 146, 1415–1424. [Google Scholar] [CrossRef]
- Elbey, M.A.; Young, D.; Kanuri, S.H.; Akella, K.; Murtaza, G.; Garg, J.; Atkins, D.; Bommana, S.; Sharma, S.; Turagam, M.; et al. Diagnostic Utility of Smartwatch Technology for Atrial Fibrillation Detection—A Systematic Analysis. J. Atr. Fibrillation 2021, 13, 20200446. [Google Scholar] [CrossRef] [PubMed]
- Couderc, J.P.; Page, A.; Lutz, M.; Tsouri, G.R.; Hall, B. Assessment of facial video-based detection of atrial fibrillation across human complexion. Cardiovasc. Digit. Health J. 2022, 3, 305–312. [Google Scholar] [CrossRef]
- Buck, B.H.; Hill, M.D.; Quinn, F.R.; Butcher, K.S.; Menon, B.K.; Gulamhusein, S.; Siddiqui, M.; Coutts, S.B.; Jeerakathil, T.; Smith, E.E.; et al. Effect of Implantable vs Prolonged External Electrocardiographic Monitoring on Atrial Fibrillation Detection in Patients With Ischemic Stroke: The PER DIEM Randomized Clinical Trial. JAMA 2021, 325, 2160–2168. [Google Scholar] [CrossRef]
- Koh, K.T.; Law, W.C.; Zaw, W.M.; Foo, D.H.P.; Tan, C.T.; Steven, A.; Samuel, D.; Fam, T.L.; Chai, C.H.; Wong, Z.S.; et al. Smartphone electrocardiogram for detecting atrial fibrillation after a cerebral ischaemic event: A multicentre randomized controlled trial. Europace 2021, 23, 1016–1023. [Google Scholar] [CrossRef] [PubMed]
- Medic, G.; Kotsopoulos, N.; Connolly, M.P.; Lavelle, J.; Norlock, V.; Wadhwa, M.; Mohr, B.A.; Derkac, W.M. Mobile Cardiac Outpatient Telemetry Patch vs Implantable Loop Recorder in Cryptogenic Stroke Patients in the US—Cost-Minimization Model. Med. Devices Evid. Res. 2021, 14, 445–458. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.V.; Mahaffey, K.W.; Hedlin, H.; Rumsfeld, J.S.; Garcia, A.; Ferris, T.; Balasubramanian, V.; Russo, A.M.; Rajmane, A.; Cheung, L.; et al. Large-Scale Assessment of a Smartwatch to Identify Atrial Fibrillation. N. Engl. J. Med. 2019, 381, 1909–1917. [Google Scholar] [CrossRef] [PubMed]
- Derkac, W.M.; Finkelmeier, J.R.; Horgan, D.J.; Hutchinson, M.D. Diagnostic yield of asymptomatic arrhythmias detected by mobile cardiac outpatient telemetry and autotrigger looping event cardiac monitors. J. Cardiovasc. Electrophysiol. 2017, 28, 1475–1478. [Google Scholar] [CrossRef]
- Gladstone, D.J.; Spring, M.; Dorian, P.; Panzov, V.; Thorpe, K.E.; Hall, J.; Vaid, H.; O’Donnell, M.; Laupacis, A.; Côté, R.; et al. Atrial fibrillation in patients with cryptogenic stroke. N. Engl. J. Med. 2014, 370, 2467–2477. [Google Scholar] [CrossRef]
- Sanna, T.; Diener, H.C.; Passman, R.S.; Di Lazzaro, V.; Bernstein, R.A.; Morillo, C.A.; Rymer, M.M.; Thijs, V.; Rogers, T.; Beckers, F.; et al. Cryptogenic stroke and underlying atrial fibrillation. N. Engl. J. Med. 2014, 370, 2478–2486. [Google Scholar] [CrossRef]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [PubMed]
- Shiozawa, M.; Koga, M.; Inoue, H.; Yamashita, T.; Yasaka, M.; Suzuki, S.; Akao, M.; Atarashi, H.; Ikeda, T.; Okumura, K.; et al. Risk of both intracranial hemorrhage and ischemic stroke in elderly individuals with nonvalvular atrial fibrillation taking direct oral anticoagulants compared with warfarin: Analysis of the ANAFIE registry. Int. J. Stroke 2023, 18, 986–995. [Google Scholar] [CrossRef]
- Saxena, R.; Koudstaal, P. Anticoagulants versus antiplatelet therapy for preventing stroke in patients with nonrheumatic atrial fibrillation and a history of stroke or transient ischemic attack. Cochrane Database Syst. Rev. 2004, 4, Cd000187. [Google Scholar] [CrossRef]
- Mohr, J.P.; Thompson, J.L.; Lazar, R.M.; Levin, B.; Sacco, R.L.; Furie, K.L.; Kistler, J.P.; Albers, G.W.; Pettigrew, L.C.; Adams, H.P., Jr.; et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N. Engl. J. Med. 2001, 345, 1444–1451. [Google Scholar] [CrossRef]
- Kim, T.J.; Lee, J.S.; Yoon, J.S.; Oh, M.S.; Kim, J.W.; Park, S.H.; Jung, K.H.; Kim, H.Y.; Kwon, J.H.; Choi, H.Y.; et al. Optimal use of antithrombotic agents in ischemic stroke with atrial fibrillation and large artery atherosclerosis. Int. J. Stroke 2023, 18, 812–820. [Google Scholar] [CrossRef]
- Soo, Y.; Zietz, A.; Yiu, B.; Mok, V.C.T.; Polymeris, A.A.; Seiffge, D.; Ambler, G.; Wilson, D.; Leung, T.W.H.; Tsang, S.F.; et al. Impact of Cerebral Microbleeds in Stroke Patients with Atrial Fibrillation. Ann. Neurol. 2023, 94, 61–74. [Google Scholar] [CrossRef]
- Carnicelli, A.P.; Hong, H.; Connolly, S.J.; Eikelboom, J.; Giugliano, R.P.; Morrow, D.A.; Patel, M.R.; Wallentin, L.; Alexander, J.H.; Cecilia Bahit, M.; et al. Direct Oral Anticoagulants Versus Warfarin in Patients With Atrial Fibrillation: Patient-Level Network Meta-Analyses of Randomized Clinical Trials With Interaction Testing by Age and Sex. Circulation 2022, 145, 242–255. [Google Scholar] [CrossRef]
- Erdem, G.; Esme, M.; Doğu, B.B. Systematic review and meta-analysis of randomized controlled trials on safety and effectiveness of oral anticoagulants for atrial fibrillation in older people. Ir. J. Med. Sci. 2022, 191, 2517–2523. [Google Scholar] [CrossRef]
- Zeng, S.; Zheng, Y.; Jiang, J.; Ma, J.; Zhu, W.; Cai, X. Effectiveness and Safety of DOACs vs. Warfarin in Patients With Atrial Fibrillation and Frailty: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 907197. [Google Scholar] [CrossRef]
- Tereshchenko, L.G.; Henrikson, C.A.; Cigarroa, J.; Steinberg, J.S. Comparative Effectiveness of Interventions for Stroke Prevention in Atrial Fibrillation: A Network Meta-Analysis. J. Am. Heart Assoc. 2016, 5, e003206. [Google Scholar] [CrossRef]
- Alrohimi, A.; Rose, D.Z.; Burgin, W.S.; Renati, S.; Hilker, N.C.; Deng, W.; Oliveira, G.H.; Beckie, T.M.; Labovitz, A.J.; Fradley, M.G.; et al. Risk of hemorrhagic transformation with early use of direct oral anticoagulants after acute ischemic stroke: A pooled analysis of prospective studies and randomized trials. Int. J. Stroke 2023, 18, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Oldgren, J.; Åsberg, S.; Hijazi, Z.; Wester, P.; Bertilsson, M.; Norrving, B. Early Versus Delayed Non-Vitamin K Antagonist Oral Anticoagulant Therapy After Acute Ischemic Stroke in Atrial Fibrillation (TIMING): A Registry-Based Randomized Controlled Noninferiority Study. Circulation 2022, 146, 1056–1066. [Google Scholar] [CrossRef] [PubMed]
- Labovitz, A.J.; Rose, D.Z.; Fradley, M.G.; Meriwether, J.N.; Renati, S.; Martin, R.; Kasprowicz, T.; Murtagh, R.; Kip, K.; Beckie, T.M.; et al. Early Apixaban Use Following Stroke in Patients With Atrial Fibrillation: Results of the AREST Trial. Stroke 2021, 52, 1164–1171. [Google Scholar] [CrossRef]
- Fridman, S.; Jimenez-Ruiz, A.; Vargas-Gonzalez, J.C.; Sposato, L.A. Differences between Atrial Fibrillation Detected before and after Stroke and TIA: A Systematic Review and Meta-Analysis. Cerebrovasc. Dis. 2022, 51, 152–157. [Google Scholar] [CrossRef]
- Sposato, L.A.; Chaturvedi, S.; Hsieh, C.Y.; Morillo, C.A.; Kamel, H. Atrial Fibrillation Detected After Stroke and Transient Ischemic Attack: A Novel Clinical Concept Challenging Current Views. Stroke 2022, 53, e94–e103. [Google Scholar] [CrossRef]
- Sposato, L.A.; Hilz, M.J.; Aspberg, S.; Murthy, S.B.; Bahit, M.C.; Hsieh, C.Y.; Sheppard, M.N.; Scheitz, J.F. Post-Stroke Cardiovascular Complications and Neurogenic Cardiac Injury: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 2768–2785. [Google Scholar] [CrossRef] [PubMed]
- Scheitz, J.F.; Nolte, C.H.; Doehner, W.; Hachinski, V.; Endres, M. Stroke-heart syndrome: Clinical presentation and underlying mechanisms. Lancet Neurol. 2018, 17, 1109–1120. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.Y.; Lee, C.H.; Wu, D.P.; Sung, S.F. Characteristics and outcomes of ischemic stroke in patients with known atrial fibrillation or atrial fibrillation diagnosed after stroke. Int. J. Cardiol. 2018, 261, 68–72. [Google Scholar] [CrossRef]
- Cerasuolo, J.O.; Cipriano, L.E.; Sposato, L.A. The complexity of atrial fibrillation newly diagnosed after ischemic stroke and transient ischemic attack: Advances and uncertainties. Curr. Opin. Neurol. 2017, 30, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Seiffge, D.J.; De Marchis, G.M.; Koga, M.; Paciaroni, M.; Wilson, D.; Cappellari, M.; Macha Md, K.; Tsivgoulis, G.; Ambler, G.; Arihiro, S.; et al. Ischemic Stroke despite Oral Anticoagulant Therapy in Patients with Atrial Fibrillation. Ann. Neurol. 2020, 87, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Lyrer, F.; Zietz, A.; Seiffge, D.J.; Koga, M.; Volbers, B.; Wilson, D.; Bonetti, B.; Schaedelin, S.; Gensicke, H.; Yoshimura, S.; et al. Atrial Fibrillation Detected before or after Stroke: Role of Anticoagulation. Ann. Neurol. 2023, 94, 43–54. [Google Scholar] [CrossRef]
- Li, J.; Gao, M.; Zhang, M.; Liu, D.; Li, Z.; Du, J.; Hou, Y. Treatment of atrial fibrillation: A comprehensive review and practice guide. Cardiovasc. J. Afr. 2020, 31, 153–158. [Google Scholar] [CrossRef]
- Leker, R.R.; Farraj, A.; Sacagiu, T.; Honig, A.; ElHasan, H.A.; Gomori, J.M.; Cohen, J.E. Atrial Fibrillation Treatment Adequacy and Outcome after Endovascular Thrombectomy. J. Stroke Cerebrovasc. Dis. 2020, 29, 104948. [Google Scholar] [CrossRef]
- Al-Shamkhani, W.; Ayetey, H.; Lip, G.Y.H. Atrial fibrillation in the Middle East: Unmapped, underdiagnosed, undertreated. Expert Rev. Cardiovasc. Ther. 2018, 16, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Friberg, L.; Rosenqvist, M. Less dementia with oral anticoagulation in atrial fibrillation. Eur. Heart J. 2018, 39, 453–460. [Google Scholar] [CrossRef]
- Giannone, M.E.; Filippini, T.; Whelton, P.K.; Chiari, A.; Vitolo, M.; Boriani, G.; Vinceti, M. Atrial Fibrillation and the Risk of Early-Onset Dementia: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2022, 11, e025653. [Google Scholar] [CrossRef]
- Jacobs, V.; Woller, S.C.; Stevens, S.; May, H.T.; Bair, T.L.; Anderson, J.L.; Crandall, B.G.; Day, J.D.; Johanning, K.; Long, Y.; et al. Time outside of therapeutic range in atrial fibrillation patients is associated with long-term risk of dementia. Heart Rhythm. 2014, 11, 2206–2213. [Google Scholar] [CrossRef]
- Caramelli, B.; Yu, P.C.; Cardozo, F.A.M.; Magalhães, I.R.; Spera, R.R.; Amado, D.K.; Escalante-Rojas, M.C.; Gualandro, D.M.; Calderaro, D.; Tavares, C.A.M.; et al. Effects of dabigatran versus warfarin on 2-year cognitive outcomes in old patients with atrial fibrillation: Results from the GIRAF randomized clinical trial. BMC Med. 2022, 20, 374. [Google Scholar] [CrossRef]
- Bunch, T.J.; May, H.; Cutler, M.; Woller, S.C.; Jacobs, V.; Stevens, S.M.; Carlquist, J.; Knowlton, K.U.; Muhlestein, J.B.; Steinberg, B.A.; et al. Impact of anticoagulation therapy on the cognitive decline and dementia in patients with non-valvular atrial fibrillation (cognitive decline and dementia in patients with non-valvular atrial fibrillation [CAF] trial). J. Arrhythm. 2022, 38, 997–1008. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.A.; Michaud, J.; Dell’Aniello, S.; Moodie, E.E.M.; Brophy, J.M.; Durand, M.; Guertin, J.R.; Boivin, J.F.; Renoux, C. Oral Anticoagulants and the Risk of Dementia in Patients With Nonvalvular Atrial Fibrillation: A Population-Based Cohort Study. Neurology 2023, 100, e1309–e1320. [Google Scholar] [CrossRef]
- Maan, A.; Mansour, M.; Ruskin, J.N.; Heist, E.K. Current Evidence and Recommendations for Rate Control in Atrial Fibrillation. Arrhythm. Electrophysiol. Rev. 2013, 2, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, R.; Justino, G.B.; Graffunder, F.P.; Benevides, L.; Knijnik, L.; Sanchez, L.M.F.; d’Avila, A. Catheter Ablation is Superior to Antiarrhythmic Drugs as First-Line Treatment for Atrial Fibrillation: A Systematic Review and Meta-Analysis. Arq. Bras. Cardiol. 2022, 119, 87–94. [Google Scholar] [CrossRef]
- Razzack, A.A.; Lak, H.M.; Pothuru, S.; Rahman, S.; Hassan, S.A.; Hussain, N.; Najeeb, H.; Reddy, K.T.; Syeda, H.; Yasmin, F.; et al. Efficacy and Safety of Catheter Ablation vs. Antiarrhythmic Drugs as Initial Therapy for Management of Symptomatic Paroxysmal Atrial Fibrillation: A Meta-Analysis. Rev. Cardiovasc. Med. 2022, 23, 112. [Google Scholar] [CrossRef]
- Chen, S.; Pürerfellner, H.; Ouyang, F.; Kiuchi, M.G.; Meyer, C.; Martinek, M.; Futyma, P.; Zhu, L.; Schratter, A.; Wang, J.; et al. Catheter ablation vs. antiarrhythmic drugs as ‘first-line’ initial therapy for atrial fibrillation: A pooled analysis of randomized data. Europace 2021, 23, 1950–1960. [Google Scholar] [CrossRef]
- Saglietto, A.; De Ponti, R.; Di Biase, L.; Matta, M.; Gaita, F.; Romero, J.; De Ferrari, G.M.; Anselmino, M. Impact of atrial fibrillation catheter ablation on mortality, stroke, and heart failure hospitalizations: A meta-analysis. J. Cardiovasc. Electrophysiol. 2020, 31, 1040–1047. [Google Scholar] [CrossRef]
- Labori, F.; Bonander, C.; Persson, J.; Svensson, M. Clinical follow-up of left atrial appendage occlusion in patients with atrial fibrillation ineligible of oral anticoagulation treatment-a systematic review and meta-analysis. J. Interv. Card. Electrophysiol. 2021, 61, 215–225. [Google Scholar] [CrossRef]
- Uchino, K. Anticoagulation Conundrum in Acute Ischemic Stroke with Atrial Fibrillation. N. Engl. J. Med. 2023, 388, 2479–2480. [Google Scholar] [CrossRef]
- Kimura, S.; Toyoda, K.; Yoshimura, S.; Minematsu, K.; Yasaka, M.; Paciaroni, M.; Werring, D.J.; Yamagami, H.; Nagao, T.; Yoshimura, S.; et al. Practical “1-2-3-4-Day” Rule for Starting Direct Oral Anticoagulants After Ischemic Stroke With Atrial Fibrillation: Combined Hospital-Based Cohort Study. Stroke 2022, 53, 1540–1549. [Google Scholar] [CrossRef] [PubMed]
- Fischer, U.; Koga, M.; Strbian, D.; Branca, M.; Abend, S.; Trelle, S.; Paciaroni, M.; Thomalla, G.; Michel, P.; Nedeltchev, K.; et al. Early versus Later Anticoagulation for Stroke with Atrial Fibrillation. N. Engl. J. Med. 2023, 388, 2411–2421. [Google Scholar] [CrossRef]
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Wu, Z.; Dong, Y.; Lip, G.Y.H.; Liu, C. Effectiveness of early rhythm control in improving clinical outcomes in patients with atrial fibrillation: A systematic review and meta-analysis. BMC Med. 2022, 20, 340. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.; Suling, A.; Metzner, A.; Schnabel, R.; Borof, K.; Goette, A.; Haeusler, K.; Zapf, A.; Wegscheider, K.; Fabritz, L.; et al. Early rhythm-control therapy for atrial fibrillation in patients with a history of stroke: A subgroup analysis of the EAST-AFNET 4 trial. Lancet Neurol. 2023, 22, 45–54. [Google Scholar] [CrossRef]
- Park, J.; Shim, J.; Lee, J.M.; Park, J.K.; Heo, J.; Chang, Y.; Song, T.J.; Kim, D.H.; Lee, H.A.; Yu, H.T.; et al. Risks and Benefits of Early Rhythm Control in Patients With Acute Strokes and Atrial Fibrillation: A Multicenter, Prospective, Randomized Study (the RAFAS Trial). J. Am. Heart Assoc. 2022, 11, e023391. [Google Scholar] [CrossRef]
- Alobaida, M.; Alrumayh, A. Rate control strategies for atrial fibrillation. Ann. Med. 2021, 53, 682–692. [Google Scholar] [CrossRef]
- Al-Khatib, S.M.; Allen LaPointe, N.M.; Chatterjee, R.; Crowley, M.J.; Dupre, M.E.; Kong, D.F.; Lopes, R.D.; Povsic, T.J.; Raju, S.S.; Shah, B.; et al. Rate- and rhythm-control therapies in patients with atrial fibrillation: A systematic review. Ann. Intern. Med. 2014, 160, 760–773. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.T.; Campbell, B.C.; Christensen, S.; Desmond, P.M.; De Silva, D.A.; Parsons, M.W.; Churilov, L.; Lansberg, M.G.; Mlynash, M.; Olivot, J.M.; et al. Worse stroke outcome in atrial fibrillation is explained by more severe hypoperfusion, infarct growth, and hemorrhagic transformation. Int. J. Stroke 2015, 10, 534–540. [Google Scholar] [CrossRef]
- Nunn, A.; Bath, P.M.; Gray, L.J. Analysis of the Modified Rankin Scale in Randomised Controlled Trials of Acute Ischaemic Stroke: A Systematic Review. Stroke Res. Treat. 2016, 2016, 9482876. [Google Scholar] [CrossRef]
- McGrath, E.; Kapral, M.; Fang, J.; Eikelboom, J.; O’Conghaile, A.; Canavan, M.; O’Donnell, M. Association of atrial fibrillation with mortality and disability after ischemic stroke. Neurology 2013, 81, 825–832. [Google Scholar] [CrossRef]
- Tracz, J.; Gorczyca-Głowacka, I.; Rosołowska, A.; Wożakowska-Kapłon, B. Long-Term Outcomes after Stroke in Patients with Atrial Fibrillation: A Single Center Study. Int. J. Environ. Res. Public Health 2023, 20, 3491. [Google Scholar] [CrossRef] [PubMed]
- Findler, M.; Molad, J.; Bornstein, N.M.; Auriel, E. Worse Outcome in Patients with Acute Stroke and Atrial Fibrillation Following Thrombolysis. Isr. Med. Assoc. J. 2017, 19, 293–295. [Google Scholar] [PubMed]
- Ottosen, T.P.; Svendsen, M.L.; Hansen, M.L.; Brandes, A.; Andersen, G.; Husted, S.E.; Johnsen, S.P. Preadmission oral anticoagulant therapy and clinical outcome in patients hospitalised with acute stroke and atrial fibrillation. Dan. Med. J. 2014, 61, A4904. [Google Scholar]
- Hsu, J.Y.; Liu, P.P.; Sposato, L.A.; Huang, H.K.; Liu, A.B.; Lai, E.C.; Lin, S.J.; Hsieh, C.Y.; Loh, C.H. Oral anticoagulant decreases stroke recurrence in patients with atrial fibrillation detected after stroke. Front. Cardiovasc. Med. 2022, 9, 929304. [Google Scholar] [CrossRef]
- Yang, J.; Wu, Y.; Gao, X.; Shang, Q.; Xu, Y.; Han, Q.; Li, J.; Chen, C.; Bivard, A.; Parsons, M.W.; et al. Poor collateral flow with severe hypoperfusion explains worse outcome in acute stroke patients with atrial fibrillation. Int. J. Stroke 2023, 18, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Lee, M.J.; Chung, J.W.; Bang, O.Y.; Kim, G.M.; Chung, C.S.; Lee, K.H. NIHSS sub-item scores predict collateral flow in acute middle cerebral artery infarction. Interv. Neuroradiol. 2018, 24, 678–683. [Google Scholar] [CrossRef]
- Rebello, L.C.; Bouslama, M.; Haussen, D.C.; Grossberg, J.A.; Dehkharghani, S.; Anderson, A.; Belagaje, S.R.; Bianchi, N.A.; Grigoryan, M.; Frankel, M.R.; et al. Stroke etiology and collaterals: Atheroembolic strokes have greater collateral recruitment than cardioembolic strokes. Eur. J. Neurol. 2017, 24, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Bang, O.Y.; Kim, S.J.; Kim, G.M.; Chung, C.S.; Lee, K.H.; Ovbiagele, B.; Liebeskind, D.S.; Saver, J.L. Role of statin in atrial fibrillation-related stroke: An angiographic study for collateral flow. Cerebrovasc. Dis. 2014, 37, 77–84. [Google Scholar] [CrossRef]
- Hu, Y.; Ji, C. Efficacy and safety of thrombolysis for acute ischemic stroke with atrial fibrillation: A meta-analysis. BMC Neurol. 2021, 21, 66. [Google Scholar] [CrossRef]
- Alobaida, M.; Harrison, S.L.; Lane, D.A.; Underhill, P.; Hill, A.; Lip, G.Y.H. Outcomes in patients with ischaemic stroke undergoing endovascular thrombectomy: Impact of atrial fibrillation. J. Stroke Cerebrovasc. Dis. 2023, 32, 106917. [Google Scholar] [CrossRef] [PubMed]
- Brinjikji, W.; Madalina Mereuta, O.; Dai, D.; Kallmes, D.F.; Savastano, L.; Liu, Y.; Nimjee, S.M.; Nogueira, R.G.; Abbasi, M.; Kadirvel, R. Mechanisms of fibrinolysis resistance and potential targets for thrombolysis in acute ischaemic stroke: Lessons from retrieved stroke emboli. Stroke Vasc. Neurol. 2021, 6, 658–667. [Google Scholar] [CrossRef]
- Sanák, D.; Herzig, R.; Král, M.; Bártková, A.; Zapletalová, J.; Hutyra, M.; Skoloudík, D.; Vlachová, I.; Veverka, T.; Horák, D.; et al. Is atrial fibrillation associated with poor outcome after thrombolysis? J. Neurol. 2010, 257, 999–1003. [Google Scholar] [CrossRef]
- Mehrpour, M.; Afrakhte, M.; Shojaei, S.F.; Sohrabi, A.; Ashayeri, R.; Esmaeili, S.; Bahadori, M. Factors predicting the outcome of intravenous thrombolysis in stroke patients before rt-PA administration. Caspian. J. Intern. Med. 2019, 10, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.F.; Chen, C.F.; Hu, H.H.; Ho, B.L.; Chen, C.H.; Chan, L.; Lin, H.J.; Sun, Y.; Lin, Y.Y.; Chen, P.L.; et al. Comparison of Different Dosages of Alteplase in Atrial Fibrillation-Related Acute Ischemic Stroke After Intravenous Thrombolysis: A Nationwide, Multicenter, Prospective Cohort Study in Taiwan. J. Am. Heart Assoc. 2022, 11, e023032. [Google Scholar] [CrossRef]
- Wu, H.; Liu, Y.; Miao, G.; Ge, J.; You, S.; Zhang, X.; Liu, H.; Zhou, Y.; Lu, T.; Cao, Y.; et al. Effect of the interaction between atrial fibrillation and rt-PA dose on the prognosis of acute ischaemic stroke with intravenous thrombolysis. Postgrad. Med. J. 2023, 99, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Tong, X.; George, M.G.; Yang, Q.; Gillespie, C. Predictors of in-hospital death and symptomatic intracranial hemorrhage in patients with acute ischemic stroke treated with thrombolytic therapy: Paul Coverdell Acute Stroke Registry 2008–2012. Int. J. Stroke 2014, 9, 728–734. [Google Scholar] [CrossRef]
- Yue, R.; Li, D.; Yu, J.; Li, S.; Ma, Y.; Huang, S.; Zeng, Z.; Zeng, R.; Sun, X. Atrial Fibrillation is Associated With Poor Outcomes in Thrombolyzed Patients With Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. Medicine 2016, 95, e3054. [Google Scholar] [CrossRef]
- Zhang, J.B.; Ding, Z.Y.; Yang, Y.; Sun, W.; Hai, F.; Sui, X.N.; Li, X.Y.; Wang, H.Z.; Wang, X.T.; Zheng, J.L. Thrombolysis with alteplase for acute ischemic stroke patients with atrial fibrillation. Neurol. Res. 2010, 32, 353–358. [Google Scholar] [CrossRef]
- Sung, S.F.; Chen, Y.W.; Tseng, M.C.; Ong, C.T.; Lin, H.J. Atrial fibrillation predicts good functional outcome following intravenous tissue plasminogen activator in patients with severe stroke. Clin. Neurol. Neurosurg. 2013, 115, 892–895. [Google Scholar] [CrossRef]
- Padjen, V.; Bodenant, M.; Jovanovic, D.R.; Ponchelle-Dequatre, N.; Novakovic, N.; Cordonnier, C.; Beslac-Bumbasirevic, L.; Leys, D. Outcome of patients with atrial fibrillation after intravenous thrombolysis for cerebral ischaemia. J. Neurol. 2013, 260, 3049–3054. [Google Scholar] [CrossRef]
- Patel, J.; Bhaskar, S.M.M. Atrial Fibrillation and Reperfusion Therapy in Acute Ischaemic Stroke Patients: Prevalence and Outcomes—A Comprehensive Systematic Review and Meta-Analysis. Neurol. Int. 2023, 15, 1014–1043. [Google Scholar] [CrossRef]
- Fu, J.; Cappelen-Smith, C.; Edwards, L.; Cheung, A.; Manning, N.; Wenderoth, J.; Parsons, M.; Cordato, D. Comparison of functional outcomes after endovascular thrombectomy in patients with and without atrial fibrillation. Vessel Plus 2021, 5, 33. [Google Scholar] [CrossRef]
- Lasek-Bal, A.; Żak, A.; Binek, Ł.; Student, S.; Tomalski, W.; Krzan, A.; Puz, P.; Uchwat, U. The effect of atrial fibrillation on the safety and efficacy of mechanical thrombectomy in patients with stroke. Pol. Arch. Intern. Med. 2022, 132, 16148. [Google Scholar] [CrossRef] [PubMed]
- Akbik, F.; Alawieh, A.; Cawley, C.M.; Howard, B.M.; Tong, F.C.; Nahab, F.; Saad, H.; Dimisko, L.; Mustroph, C.; Samuels, O.B.; et al. Differential effect of mechanical thrombectomy and intravenous thrombolysis in atrial fibrillation associated stroke. J. Neurointerv. Surg. 2021, 13, 883–888. [Google Scholar] [CrossRef]
- Tong, X.; Li, S.; Liu, W.; Ren, Z.; Liu, R.; Jia, B.; Zhang, X.; Huo, X.; Luo, G.; Ma, G.; et al. Endovascular treatment for acute ischemic stroke in patients with versus without atrial fibrillation: A matched-control study. BMC Neurol. 2021, 21, 377. [Google Scholar] [CrossRef]
- Smaal, J.A.; de Ridder, I.R.; Heshmatollah, A.; van Zwam, W.H.; Dippel, D.; Majoie, C.B.; Brown, S.; Goyal, M.; Campbell, B.; Muir, K.W.; et al. Effect of atrial fibrillation on endovascular thrombectomy for acute ischemic stroke. A meta-analysis of individual patient data from six randomised trials: Results from the HERMES collaboration. Eur. Stroke J. 2020, 5, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Zha, M.; Gao, J.; Du, J.; Liu, R.; Liu, X. Increased intracranial hemorrhage of mechanical thrombectomy in acute ischemic stroke patients with atrial fibrillation. J. Thromb. Thrombolysis 2021, 51, 536–544. [Google Scholar] [CrossRef]
- Ždraljević, M.; Pekmezović, T.; Stanarčević, P.; Vukašinović, I.; Berisavac, I.; Ercegovac, M.; Vitošević, F.; Nestorović, D.; Cvetić, V.; Padjen, V.; et al. Atrial fibrillation is associated with poor long-term outcome after mechanical thrombectomy for anterior large vessel occlusion stroke. J. Stroke Cerebrovasc. Dis. 2022, 31, 106755. [Google Scholar] [CrossRef]
- Kobeissi, H.; Ghozy, S.; Seymour, T.; Gupta, R.; Bilgin, C.; Kadirvel, R.; Rabinstein, A.A.; Kallmes, D.F. Outcomes of Patients With Atrial Fibrillation Following Thrombectomy for Stroke: A Systematic Review and Meta-analysis. JAMA Netw. Open 2023, 6, e2249993. [Google Scholar] [CrossRef]
- Loo, J.H.; Leow, A.S.; Jing, M.; Sia, C.H.; Chan, B.P.; Seet, R.C.; Teoh, H.L.; Meyer, L.; Fiehler, J.; Papanagiotou, P.; et al. Impact of atrial fibrillation on the treatment effect of bridging thrombolysis in ischemic stroke patients undergoing endovascular thrombectomy: A multicenter international cohort study. J. Neurointerv. Surg. 2023; ahead of print. [Google Scholar] [CrossRef]
- Akbik, F.; Alawieh, A.; Dimisko, L.; Howard, B.M.; Cawley, C.M.; Tong, F.C.; Nahab, F.; Samuels, O.B.; Maier, I.; Feng, W.; et al. Bridging thrombolysis in atrial fibrillation stroke is associated with increased hemorrhagic complications without improved outcomes. J. Neurointerv. Surg. 2022, 14, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Mujanovic, A.; Kurmann, C.C.; Dobrocky, T.; Olivé-Gadea, M.; Maegerlein, C.; Pierot, L.; Mendes Pereira, V.; Costalat, V.; Psychogios, M.; Michel, P.; et al. Bridging intravenous thrombolysis in patients with atrial fibrillation. Front. Neurol. 2022, 13, 945338. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.Y.; Huang, M.; Wang, A.L.; Ge, G.; Ma, M.; Zhi, H.; Wang, L.N. Atrial fibrillation burden and the risk of stroke: A systematic review and dose-response meta-analysis. World J. Clin. Cases 2022, 10, 939–953. [Google Scholar] [CrossRef]
- Chen, Y.; Huang, Q.F.; Sheng, C.S.; Zhang, W.; Shao, S.; Wang, D.; Cheng, Y.B.; Wang, Y.; Guo, Q.H.; Zhang, D.Y.; et al. Detection rate and treatment gap for atrial fibrillation identified through screening in community health centers in China (AF-CATCH): A prospective multicenter study. PLoS Med. 2020, 17, e1003146. [Google Scholar] [CrossRef]
- Santos, I.S.; Goulart, A.C.; Olmos, R.D.; Thomas, G.N.; Lip, G.Y.H.; Lotufo, P.A.; Benseñor, I.M. Atrial fibrillation in low- and middle-income countries: A narrative review. Eur. Heart J. Suppl. 2020, 22, O61–O77. [Google Scholar] [CrossRef]
- Schwamm, L.H.; Kamel, H.; Granger, C.B.; Piccini, J.P.; Katz, J.M.; Sethi, P.P.; Sidorov, E.V.; Kasner, S.E.; Silverman, S.B.; Merriam, T.T.; et al. Predictors of Atrial Fibrillation in Patients With Stroke Attributed to Large- or Small-Vessel Disease: A Prespecified Secondary Analysis of the STROKE AF Randomized Clinical Trial. JAMA Neurol. 2023, 80, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Diederichsen, S.Z.; Frederiksen, K.S.; Xing, L.Y.; Haugan, K.J.; Højberg, S.; Brandes, A.; Graff, C.; Olesen, M.S.; Krieger, D.; Køber, L.; et al. Severity and Etiology of Incident Stroke in Patients Screened for Atrial Fibrillation vs Usual Care and the Impact of Prior Stroke: A Post Hoc Analysis of the LOOP Randomized Clinical Trial. JAMA Neurol. 2022, 79, 997–1004. [Google Scholar] [CrossRef]
- Myint, P.K.; Staufenberg, E.F.; Sabanathan, K. Post-stroke seizure and post-stroke epilepsy. Postgrad. Med. J. 2006, 82, 568–572. [Google Scholar] [CrossRef]
- Fialho, G.L.; Pang, T.D.; Kong, W.Y.; Tran, A.P.; Yu, C.G.; Rodriguez, I.D.; Nearing, B.D.; Waks, J.W.; Maher, T.R.; Clarke, J.R.; et al. Individuals with chronic epilepsy have elevated P-wave heterogeneity comparable to patients with atrial fibrillation. Epilepsia 2023, 64, 2361–2372. [Google Scholar] [CrossRef]
- Mohammaden, M.H.; Stapleton, C.J.; Brunozzi, D.; Hussein, A.E.; Khedr, E.M.; Atwal, G.; Alaraj, A. Predictors of Poor Outcome Despite Successful Mechanical Thrombectomy of Anterior Circulation Large Vessel Occlusions Within 6 h of Symptom Onset. Front. Neurol. 2020, 11, 907. [Google Scholar] [CrossRef]
- Jiao, J.; Liu, S.; Cui, C.; Cao, Y.; Jia, Z.; Liu, H.; Wang, C.; Hang, Y.; Ni, H.; Chen, M.; et al. Endovascular thrombectomy for acute ischemic stroke in elderly patients with atrial fibrillation. BMC Neurol. 2022, 22, 100. [Google Scholar] [CrossRef]
- Shao, R.; Wang, Z.; Shi, H.; Li, Y.; Zhuang, Y.; Xu, J.; Xu, M. Stroke severity modified the effect of chronic atrial fibrillation on the outcome of thrombolytic therapy. Medicine 2022, 101, e29322. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Yoon, W.; Kim, T.S.; Kim, H.S.; Heo, T.W.; Park, M.S. Histologic Analysis of Retrieved Clots in Acute Ischemic Stroke: Correlation with Stroke Etiology and Gradient-Echo MRI. Am. J. Neuroradiol. 2015, 36, 1756–1762. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Killingsworth, M.C.; Bhaskar, S.M.M. Is Composition of Brain Clot Retrieved by Mechanical Thrombectomy Associated with Stroke Aetiology and Clinical Outcomes in Acute Ischemic Stroke?-A Systematic Review and Meta-Analysis. Neurol. Int. 2022, 14, 748–770. [Google Scholar] [CrossRef] [PubMed]
- Sporns, P.B.; Hanning, U.; Schwindt, W.; Velasco, A.; Minnerup, J.; Zoubi, T.; Heindel, W.; Jeibmann, A.; Niederstadt, T.U. Ischemic Stroke: What Does the Histological Composition Tell Us About the Origin of the Thrombus? Stroke 2017, 48, 2206–2210. [Google Scholar] [CrossRef]
- Baek, J.H.; Kim, B.M.; Heo, J.H.; Kim, D.J.; Nam, H.S.; Kim, Y.D. Outcomes of Endovascular Treatment for Acute Intracranial Atherosclerosis-Related Large Vessel Occlusion. Stroke 2018, 49, 2699–2705. [Google Scholar] [CrossRef]
- Guglielmi, V.; LeCouffe, N.E.; Zinkstok, S.M.; Compagne, K.C.J.; Eker, R.; Treurniet, K.M.; Tolhuisen, M.L.; van der Worp, H.B.; Jansen, I.G.H.; van Oostenbrugge, R.J.; et al. Collateral Circulation and Outcome in Atherosclerotic Versus Cardioembolic Cerebral Large Vessel Occlusion. Stroke 2019, 50, 3360–3368. [Google Scholar] [CrossRef]
- Talari, K.; Goyal, M. Retrospective studies—Utility and caveats. J. R. Coll. Physicians Edinb. 2020, 50, 398–402. [Google Scholar] [CrossRef]
- Majersik, J.J. Ethics and Bias in Clinical Trial Enrollment in Stroke. Curr. Cardiol. Rep. 2019, 21, 49. [Google Scholar] [CrossRef]
- Heshmatollah, A.; Fransen, P.S.S.; Berkhemer, O.A.; Beumer, D.; van der Lugt, A.; Majoie, C.; Oostenbrugge, R.J.; van Zwam, W.H.; Koudstaal, P.J.; Roos, Y.; et al. Endovascular thrombectomy in patients with acute ischaemic stroke and atrial fibrillation: A MR CLEAN subgroup analysis. EuroIntervention 2017, 13, 996–1002. [Google Scholar] [CrossRef]
- Padjen, V.; Jovanovic, D.; Berisavac, I.; Ercegovac, M.; Stefanovic Budimkic, M.; Stanarcevic, P.; Beslac Bumbasirevic, L. Effect of intravenous thrombolysis on stroke associated with atrial fibrillation. J. Stroke Cerebrovasc. Dis. 2014, 23, 2199–2205. [Google Scholar] [CrossRef]
- Seet, R.C.; Zhang, Y.; Wijdicks, E.F.; Rabinstein, A.A. Relationship between chronic atrial fibrillation and worse outcomes in stroke patients after intravenous thrombolysis. Arch. Neurol. 2011, 68, 1454–1458. [Google Scholar] [CrossRef] [PubMed]
- Lin, L. Bias caused by sampling error in meta-analysis with small sample sizes. PLoS ONE 2018, 13, e0204056. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Li, X.; Dong, W.; Ye, M.; Cao, Y.; Zhang, M.; Cheng, Q.; Zhou, J.; Chen, G.; Yu, M.; et al. Factors Associated with Thrombolysis Outcome in Ischemic Stroke Patients with Atrial Fibrillation. Neurosci. Bull. 2016, 32, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Vitolo, M.; Diemberger, I.; Proietti, M.; Valenti, A.C.; Malavasi, V.L.; Lip, G.Y.H. Optimizing indices of atrial fibrillation susceptibility and burden to evaluate atrial fibrillation severity, risk and outcomes. Cardiovasc. Res. 2021, 117, 1–21. [Google Scholar] [CrossRef]
- Wineinger, N.E.; Barrett, P.M.; Zhang, Y.; Irfanullah, I.; Muse, E.D.; Steinhubl, S.R.; Topol, E.J. Identification of paroxysmal atrial fibrillation subtypes in over 13,000 individuals. Heart Rhythm. 2019, 16, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Friberg, L.; Hammar, N.; Rosenqvist, M. Stroke in paroxysmal atrial fibrillation: Report from the Stockholm Cohort of Atrial Fibrillation. Eur. Heart J. 2010, 31, 967–975. [Google Scholar] [CrossRef] [PubMed]
- Naser, N.; Dilic, M.; Durak, A.; Kulic, M.; Pepic, E.; Smajic, E.; Kusljugic, Z. The Impact of Risk Factors and Comorbidities on The Incidence of Atrial Fibrillation. Mater. Sociomed. 2017, 29, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Mertz, V.; Cottin, Y.; Bentounes, S.A.; Pastier-Debeaumarché, J.; Didier, R.; Herbert, J.; Zeller, M.; Lip, G.Y.H.; Fauchier, L. Prognosis of Atrial Fibrillation with or without Comorbidities: Analysis of Younger Adults from a Nationwide Database. J. Clin. Med. 2022, 11, 1981. [Google Scholar] [CrossRef]
- Huang, J.C.; Bhaskar, S.M.M. Clot Morphology in Acute Ischemic Stroke Decision Making. Int. J. Mol. Sci. 2022, 23, 12373. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Number of Patients (n) | Study Design | Technique(s) and Timescale | Outcomes (Primarily Regarding AF Detection Rate) |
|---|---|---|---|---|
| Buck et al. [42] | 300 | RCT | 12-month ILR vs. 30-day ELR | In ischemic stroke patients monitored for 12 months using an ILR, AF was detected in 15.3% of patients compared to 4.7% of patients monitored with a 30-day ELR (RR 3.29 [95% CI 1.45–7.42], p = 0.03). |
| Koh et al. [43] | 203 | RCT | 30 days of KardiaMobile ECG (used for 30 s 3 times per day) vs. one additional round of 24-h Holter monitoring | In patients with a recent cryptogenic stroke or TIA, AF of duration ≥ 30 s was detected in 9.5% of patients in the KardiaMobile group compared to 2.0% in those receiving 24 h Holter monitoring (p = 0.024). |
| Liu et al. [21] | 158 | Prospective | 14-day ECG patch vs. 24-h Holter monitoring | AF and/or atrial flutter was detected in 9.5% of patients wearing the 14-day ECG patch compared to 3.8% in patients with 24 h Holter monitoring (p = 0.042). |
| Medic et al. [44] | 1000 | Retrospective (economic model) | 30-day MCOT followed by ILR vs. ILR alone over 12 months | In patients with cryptogenic stroke, 30-day MCOT followed by an ILR had an AF detection rate of 20.9% compared to a detection rate of 4.5% when using an ILR alone. Cost-effectiveness analysis revealed 7.72 times lower costs per AF patient detected when using MCOT initially (USD 29,598 per patient with detected AF) compared to when using an ILR only (USD 228,507 per patient with detected AF). |
| Chua et al. [20] | 32 | Prospective | 14-day ECG patch vs. 24-h Holter monitoring | Paroxysmal AF and/or atrial flutter was detected in 19% of patients wearing the ECG patch compared to 3% in patients with 24 h Holter monitoring (p < 0.05). |
| Perez et al. [45] | 419,297 | Prospective | 8 months of monitoring with an Apple Watch | Of Apple Watch wearers among the general population, 0.52% received a notification regarding an irregular pulse over 8 months. Of the patients who were notified to have an irregular pulse and subsequently wore and returned an ECG patch, AF was confirmed in 34%. Comparatively, in those who did not receive a notification regarding an irregular pulse, a diagnosis of AF was established in 1.0% of patients. |
| Derkac et al. [46] | 78,490 | Retrospective | MCOT vs. ILR analysed over 8 months | AF was diagnosed in 23.5% of patients with MCOT compared to 11.3% of patients with an ILR. It should be noted that the median prescription time for the MCOT group was 20 days compared to 30 days in those with the ILR group, despite the latter device having the potential to be used for a considerably longer duration. |
| Gladstone et al. [47] | 572 | RCT | 30 days of event-triggered loop recorder vs. 24 h ECG | AF was detected in 16.1% of patients with the event-triggered loop recorder compared to 3.2% of patients with 24 h ECG monitoring (p < 0.001). Episodes of AF spanning 150 s or longer were recorded in 9.9% of patients with event-triggered recorders compared to 2.5% of those with standard 24 h ECG monitoring (p < 0.001). These differences had clinical implications as 18.6% of patients in the loop recorder group had commenced anticoagulant therapy compared to 11.1% of those in the 24 h ECG monitoring group (p = 0.01). |
| Sanna et al. [48] | 441 | RCT | 6 months of ILR vs. conventional follow-up (ECG assessment at follow-up visits, with exact protocol at the discretion of each site) | AF was detected in 8.9% of patients with an ILR by 6 months compared to 1.4% in patients receiving conventional follow-up following a cryptogenic stroke (HR 6.4 [95% CI 1.9 to 21.7], p < 0.001). By 12 months, AF was detected in 12.4% of patients with an ILR compared to 2.0% in those with conventional follow-up (HR 7.3 [95% CI 2.6 to 20.8], p < 0.001). In the patients followed up for 36 months, these rates grew to 30% and 3.0% respectively (HR 8.8 [95% CI 3.5 to 22.2], p < 0.001). |
| Study | Number of Patients (n) | Study Design | Treatment(s) | Outcomes (Primarily Regarding the Incidence of Stroke) | Haemorrhagic Adverse Events |
|---|---|---|---|---|---|
| Carnicelli et al. [59] | 71,683 | Meta-analysis | Standard-dose DOACs vs. lower-dose DOACs vs. warfarin | Relative to warfarin, standard-dose DOACs were linked to significant decreases in the risk of stroke or systemic embolism (HR 0.81 [95% CI 0.74–0.89]) and mortality (HR 0.92 [95% CI 0.87–0.97]). When compared to warfarin, lower-dose DOACs were not associated with a significant difference in the risk of stroke or systemic embolism (HR 1.06 [95% CI 0.95–1.19]). However, there was a significant decrease in mortality (HR 0.90, [95% CI 0.83–0.97]. | Relative to warfarin, standard-dose DOACs were linked to a significant decrease in the risk of intracranial bleeding (HR 0.45 [95% CI 0.37–0.56]) but not in the risk of major bleeding (HR 0.86, 95% CI [0.74–1.01]). On the other hand, when compared to warfarin, lower dose DOACs were associated with a lower risk of both intracranial bleeding (HR 0.28 [95% CI 0.21–0.37]) and major bleeding (HR 0.63 [95% CI 0.45–0.88]). |
| Erdem et al. [60] | 73,122 | Meta-analysis | DOACs vs. warfarin | Compared to warfarin, there was a decreased risk of stroke or systemic embolism when taking DOACs in patients ≥ 75 years old (RR 0.57 [95% CI 0.42–0.76]) and patients < 75 years old (RR 0.74, 95% CI [0.43, 1.27]). This was statistically significant for ages ≥75 years but not ages <75 years. | Compared to warfarin, there was a significantly lower risk of major bleeding in patients taking DOACs who were ≥75 years old (RR 0.74 [95% CI 0.63–0.87]) as well as in those <75 years old (RR 0.64 [95% CI 0.44–0.93]). |
| Zeng et al. [61] | 835,520 | Meta-analysis | DOACs vs. warfarin | Relative to warfarin, DOACs were associated with a significantly lower risk of ischemic stroke (HR 0.79 [95% CI 0.71–0.87]) and mortality (HR 0.90 [95% CI 0.84–0.96]). | Relative to warfarin, DOACs were associated with a significantly lower risk of intracranial bleeding (HR 0.58 [95% CI 0.52–0.65]) and major bleeding (HR 0.79 [95% CI 0.64–0.97]) but no significant decrease in the risk of gastrointestinal bleeding (HR 0.97 [95% CI 0.73–1.29]). |
| Tereshchenko et al. [62] | 96,017 | Meta-analysis | Aspirin vs. VKAs vs. DOACs vs. placebo | After adjusting for other variables, treatment with VKAs and DOACs led to significantly lower rates of stroke or systemic embolism compared to placebo. However, the odds were not significantly lower for patients taking aspirin compared to placebo (aOR 0.77 [95% CI 0.53–1.11]). | After adjusting for other variables, there was no significant difference in the rates of major bleeding between treatments with aspirin, VKAs, and DOACs. |
| Study | Number of Patients (n) | Number of Patients with AF and AF Prevalence (%) | Study Design | Functional Outcomes | Mortality | sICH |
|---|---|---|---|---|---|---|
| Hu & Ji [110] | 8509 | 2125 (24.97%) | Meta- analysis | AF patients reported significantly lower odds of favourable functional outcomes (90-day mRS ≤ 2) following IVT compared to non-AF patients (OR 0.55 [95% CI 0.43–0.70], p < 0.001). Comparing AF patients who received IVT with AF patients who did not, there was no significant difference in the odds of favourable functional outcomes (OR 1.37 [95% CI 0.72–2.60, p = 0.331). | AF patients reported significantly higher odds of mortality following IVT compared to non-AF patients (OR 2.05 [95% CI 1.79–2.36], p < 0.001). Comparing AF patients who received IVT with AF patients who did not, there was no significant difference in mortality (OR 0.95 [95% CI 0.63–1.44], p = 0.813). | AF patients reported significantly higher odds of sICH compared to non-AF patients (OR 3.44 [95% CI 2.04–5.82], p < 0.001). The odds of sICH were significantly higher in AF patients receiving IVT compared to AF patients not receiving IVT (OR 3.44 [95% CI 2.04–5.82], p < 0.001). |
| Yue et al. [118] | 14,801 | 3432 (23.19%) | Meta- analysis | AF patients were significantly less likely to experience favourable outcomes (90-day mRS ≤ 2) following IVT (OR 1.95 [95% CI 1.33–2.85], p = 0.001). | AF patients had significantly higher odds of mortality 90 days following IVT (OR 2.13 [95% CI 1.68–2.70], p < 0.001). | The odds of sICH were significantly higher amongst AF patients (OR 1.28 [95% CI 1.08–1.52], p = 0.006). |
| Patel & Bhaskar [122] | 39,650 | 11,163 (28.15%) a | Meta-analysis | AF patients had significantly lowers odds of favourable functional outcomes (90-day mRS ≤ 2) at 90 days following IVT (OR 0.512 [95% CI 0.376–0.696], p < 0.001) | AF was associated with significantly higher odds of sICH following IVT (OR 1.690 [95% CI 1.400–2.039], p = 0.851). | AF was associated with significantly higher odds of 90-day mortality following IVT (OR 1.799 [95% CI 1.218–2.657], p = 0.003) |
| Study | Number of Patients (n) | Number of Patients with AF and AF Prevalence (%) | Study Design | Functional Outcomes | Mortality | sICH |
|---|---|---|---|---|---|---|
| Kobeissi et al. [107] | 6131 | 2305 (37.60%) | Meta-analysis | No significant difference in the odds of functional independence (90-day mRS ≤ 2) between patients with AF and those without AF (OR 0.72 [95% CI 0.47–1.10], p = 0.13). Confounders were not adjusted for. However, following sensitivity analysis, the rate of functional independence was significantly lower for AF patients (OR 0.65 [95% CI 0.52–0.81], p < 0.001). | Mortality was significantly higher in patients with AF (OR 1.47 [95% CI 1.12–1.92], p = 0.005). | No significant difference in the odds of sICH between AF patients compared to non-AF patients (OR 1.05 [95% CI 0.84–1.31], p = 0.68). |
| Patel & Bhaskar [122] | 21,148 | 8857 (41.88%) a | Meta-analysis | There was no significant association between AF and favourable functional outcomes (90-day mRS ≤ 2) following EVT (OR 0.826 [95% CI 0.651–1.049], p = 0.117). | There was no significant association between AF and sICH following EVT (OR 0.982 [95% CI 0.815–1.184], p = 0.851). | There was no significant association between AF and 90-day mortality at post-EVT (OR 1.236 [95% CI 0.969–1.578], p = 0.088). |
| Smaal et al. [104] | 1351 | 447 (33.09%) | Meta-analysis | After adjusting for other factors, there was no significant association between favourable functional outcomes (90-day mRS ≤ 2) and AF status (aOR 1.14 [95% CI 0.87–1.51], p = 0.337). | There was no significant association between AF and 90-day mortality (aOR 1.14 [95% CI 0.83–1.57], p = 0.410). | There was no significant association between AF and sICH (aOR 0.57 [95% CI 0.3–1.07], p = 0.082). |
| Study | Number of Patients (n) | Number of Patients with AF and AF Prevalence (%) | Study Design | Functional Outcomes | Mortality | sICH |
|---|---|---|---|---|---|---|
| Loo et al. [131] | 705 | 314 (44.54%) | Retrospective | For patients with AF, there was no significant difference in the likelihood of favourable functional outcomes (90-day mRS ≤ 2) between those receiving bridging therapy compared to those treated with EVT alone (35.0% vs. 33.3%, p = 0.761). However, for patients without AF, the rate of favourable functional outcomes was significantly higher in those receiving bridging therapy compared to those treated with EVT alone (45.2% vs. 23.7%, p < 0.001). | For patients with AF, there was no significant difference in the likelihood of mortality between those receiving bridging therapy compared to those treated with EVT alone (11.9% vs. 14.5%, p = 0.631). For patients without AF, there was no significant difference in the likelihood of mortality between those receiving bridging therapy compared to those treated with EVT alone (11.7% vs. 14.5, p = 0.559). | For patients with AF, there was no significant difference in the likelihood of sICH between those receiving bridging therapy compared to those treated with EVT alone (11.0% vs. 7.7%, p = 0.323). For patients without AF, there was no significant difference in the likelihood of sICH between those receiving bridging therapy compared to those treated with EVT alone (12.8% vs. 13.9%, p = 0.765). |
| Akbik et al. [132] | 6461 | 2311 (35.77%) | Retrospective | In non-AF patients, treatment with bridging therapy was associated with a significantly increased likelihood of favourable functional outcomes (90-day mRS ≤ 2) compared to receiving EVT alone (aOR 1.29 [95% CI 1.03–1.60], p = 0.025). However, in AF patients, there was no significant association between bridging therapy and favourable functional outcomes (aOR 1.28 [95% CI 0.94–1.74], p = 0.11). | Comparing AF patients treated with bridging therapy to AF patients treated with EVT alone, there was no significant difference in mortality (27.3% vs. 25.7%, p = 0.593). | There were significantly elevated odds of sICH or parenchymal haematoma type 2 in AF patients who were treated with bridging therapy compared to those treated with EVT alone (aOR 1.66 [95% CI 1.07–2.57], p = 0.024). |
| Mujanovic et al. [133] | 2941 | 1347 (45.80%) | Retrospective | Treatment with bridging therapy was associated with a significantly higher likelihood of favourable functional outcomes (90-day mRS ≤ 2) compared to EVT alone (aOR 1.61 [95% CI 1.24–2.11], p < 0.001). There was no significant association between AF and favourable functional outcomes following bridging therapy (aOR 0.98 [95% CI 0.66–1.46], p = 0.924). | There was no significant difference in the likelihood of mortality between AF patients treated with bridging therapy compared to EVT alone (21.6% vs. 28.1%, p = 0.038). | There was no significant association between AF and sICH following bridging therapy (aOR 1.37 [95% CI 0.67–2.83], p = 0.390). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, J.; Bhaskar, S.M.M. Diagnosis and Management of Atrial Fibrillation in Acute Ischemic Stroke in the Setting of Reperfusion Therapy: Insights and Strategies for Optimized Care. J. Cardiovasc. Dev. Dis. 2023, 10, 458. https://doi.org/10.3390/jcdd10110458
Patel J, Bhaskar SMM. Diagnosis and Management of Atrial Fibrillation in Acute Ischemic Stroke in the Setting of Reperfusion Therapy: Insights and Strategies for Optimized Care. Journal of Cardiovascular Development and Disease. 2023; 10(11):458. https://doi.org/10.3390/jcdd10110458
Chicago/Turabian StylePatel, Jay, and Sonu M. M. Bhaskar. 2023. "Diagnosis and Management of Atrial Fibrillation in Acute Ischemic Stroke in the Setting of Reperfusion Therapy: Insights and Strategies for Optimized Care" Journal of Cardiovascular Development and Disease 10, no. 11: 458. https://doi.org/10.3390/jcdd10110458