1. Introduction
It is admissible that the aesthetic value of a fixed restoration may be compromised by many parameters including altered gingival architecture, dental morphology, texture and clinical crown dimensions. Therefore, both dental and gingival aesthetics have gained equal attention when restoring anterior teeth [
1]. When it comes to fixed prosthesis in the anterior region, clinicians are in general agreement that gingival levels affect normal teeth proportion and as a consequence it has a direct impact on aesthetics [
2]. An unattractive soft tissue surrounding beautiful restoration has a negative impact on the aesthetic result [
3,
4]. Periodontal therapy plays a great role in correcting gingival defects and increases the prepared tooth surface which is beneficial for retention. It provides the opportunity to recreate a harmonious gingival architecture and correct Zenith location with reference to normal anatomy [
5].
However, identifying each gingival biotype, using reliable methods, is important because they present different healing tendencies. Olsson and Lindhe examined the width thickness of the keratinized gingiva and incisor teeth shape to determine the periodontal biotype which can affect the results of periodontal therapy. They defined the thin scalloped biotype representing high scalloped gingiva and osseous contour, narrow keratinzed gingiva and a triangular tooth form whereas thick flat biotype shows flat gingiva and osseous contour, wide keratinized gingiva and a square tooth form. Other authors determined a periodontal biotype on the basis of gingival thickness. The gingiva with thickness of less than 1.5 mm was classified as a thin biotype whereas the gingiva with thickness ≥1.5 mm was classified as a thick biotype. In patients with thick flat biotype, a greater regaining of soft tissue occurs after crown lengthening procedures than in patients with thin biotype that shows higher prevalence of gingival recession [
6,
7]. In addition, post-surgery clinical results were strongly associated with the gingival and crest form. In cases with a crest bone level that is ≥3 mm apical to CEJ, an increased susceptibility for gingival recession which may expose restorative margins when finish lines are subgingivally placed. This is particularly significant for full coverage crowns as thin gingival margins allows visibility of metal substructure for porcelain fused to a metal crown [
3,
8].
To optimize soft tissues position, there are universal guidelines for clinicians to outline gingival contours and as a consequence to achieve a predictable aesthetic result. A knife edged gingival margins, a cone shaped inter dental papilla with a well-shaped dental Zenith are considered as the ideal gingival contours. They constitute important features affecting esthetic perception [
9].
Gingival Zenith is located distal to the long axis of the tooth on the labial surface of the maxillary central incisors and canines. In contrast, the maxillary lateral incisors have a symmetrical gingival height of contours with the gingival Zenith at the midline of the labial tooth surface [
10]. However, some studies have shown that lateral incisors can show a deviation of the gingival Zenith by a mean of 0.4 mm [
9].In addition, it is found that the lateral incisor is approximately, in a vertical dimension, 1 mm coronal to adjacent central incisor [
2,
9]. In addition, when restoring anterior teeth the gingival contours should not be altered by grayish shadow of metal based restorations. This compromises aesthetics and leads to a discrepancy on pink and white score which constitutes an index to evaluate esthetics in terms of harmony between the crown (white aesthetic) and surrounding soft tissues (pink aesthetics) as the gingiva presents the frame for the teeth. Besides, pink tissues firmly surrounding the neck of the teeth are key to aesthetic appearance in terms of healthy periodontiuim [
11,
12]. These parameters, already cited, must be taken into consideration when designing fixed prosthesis in the anterior region [
13]. Recently, patients’ awareness and aesthetic demands have significantly increased to the point that less than optimal aesthetics are no longer acceptable. Consequently, it exerts pressure on dental professionals who are invited to provide restorations in harmony with a healthy periodontium. This leads to the development of surgical procedures and prosthetic techniques for improving these characteristics. For that, they need to have essential tools and knowledge concerning dentogingival interface to create an optimal soft tissues profile around restorations [
2,
14]. A successful aesthetic and functional treatment is based on the evaluation of endodontic and periodontal health of the abutment. In fact, the aspect of the remaining tooth structure is important because it has a direct impact on retention requirements. Reinforcement of devitalized teeth is essential because the prepared tooth should present a retentive core. It includes aesthetic post and core systems where fiber posts are used, and classic metal post and core systems [
4]. Aesthetic crown lengthening which is defined as a procedure used to expose sound tooth structure with or without removal of alveolar bone for restorative purposes. It provides the opportunity to recreate a harmonious gingival architecture and correct Zenith location with reference to normal anatomy [
5,
15]. In the aesthetic zone, gingivectomy and apically repositioned flap seem to be the mainly used techniques. In general, the selection of a surgical procedure depends on two important components which are the apico-coronal width of keratinized gingiva and the biological width. The latter must be respected because its invasion conducts to inflammation and bone loss [
10,
16]. When a multidisciplinary approach including surgical techniques is necessary, an ultimate communication between the periodontist, prosthodontist and the laboratory technician is essential. A predictable successful aesthetic rehabilitation seems to be interplaying between the role of a skilled prosthodontist in the achievement of a natural looking morphology and surface texture and the talent of the periodontist in selecting and performing the appropriate technique to get harmonious gingival margins [
1].
2. Clinical Report
A 25-year-old dental student presented to the department of prosthetic dentistry with a chief complaint of poor aesthetics due to her imperfect metal ceramic single crown in the lateral incisor. She was bothered about the visible dark areas under the crown margins and requested an aesthetic rehabilitation. She also expressed her dissatisfaction with its color and shape. Intra oral examination showed dark gingival margins in the lateral incisor caused by metal frame (
Figure 1). Soft tissues were evaluated as healthy with a wide band of attached gingiva in the maxillary region and a good oral hygiene.Visual assessment and Periodontal probing revealed a thick healthy gingival biotype with gingival thickness of 2 mm. and a sulcus depth of 2 mm. Bone sounding revealed a crest position in close relationship relative to anticipated post-surgical gingival margin level (2.5 mm). As the patient presents a thick periodontal biotype, this would significantly influence the post-operative procedure in favor of the esthetically desired outcome as this type is less prone to post-surgical recession.
Aesthetic assessment showed a squared teeth form, a size discrepancy and a non-symmetrical gingival architecture between the left and right lateral incisors (
Figure 2). A slight asymmetry between the gingival margins of the right and left central incisors was noticeable. However, the patient did not express her dissatisfaction about it and refused any surgery on her sound teeth.
Gingival zenith was evaluated as non-aesthetic as it occupies a location that does not coincide with the long axis of the tooth.
Gingival display was evaluated as more than 4 mm on the side of the lateral incisor when smiling. Radiographic examination revealed an adequate root canal filing with no bone loss.
Figure 1.
Intra oral view showing the grayish shadow caused by the metal based crown.
Figure 1.
Intra oral view showing the grayish shadow caused by the metal based crown.
Figure 2.
Gingival display due to the asymmetrical ZENITH.
Figure 2.
Gingival display due to the asymmetrical ZENITH.
To meet aesthetic goals, the treatment plan included aesthetic crown lengthening followed by an all ceramic crown replacing the defective restoration in the lateral incisor.
After careful evaluation, diagnostic casts were waxed to visualize the future gingival margins and, as a consequence, the restoration features. A symmetrical gingival margin and ideal tooth length were drawn on the cast.
The margin level of the lateral incisor was planned to be 1 mm coronal to the central incisor. The waxed cast served as a guide for provisional restoration which had been optimized after the periodontal therapy until the objectives desired in the final restoration were achieved. The old crown was removed and the remaining tooth structure was evaluated as sound. Radiological reevaluation showed an adequate distance between the bone crest and the residual dental tissue (>3 mm) including biological width (
Figure 3).
Provisional restoration was placed prior to crown lengthening in order to help condition the marginal gingiva into a more favorable level and architecture, to change the existing faulty crown dimensions and morphology prior to establishing the need for crown lengthening. Aesthetic crown lengthening was performed to correct gingival asymmetries and to reposition the dentogingival complex adequately to the aesthetic restoration. However, the surgical repositioning of the gingival margin did not expose the osseous crest but, nevertheless, was in violation of the biological width. A mucoperiosteal flap was elevated to gain access to the alveolar crest. Alveolar bone recontouring of 1.5 mm was performed to recreate a distance of 3 mm, including the biological width, between the alveolar crest and the finishing line. It was located in accordance with the planned reconstruction. Interproximal bone was recontoured judiciously to minimize chances of losing the papilla. It was ramped and festooned from the labial to palatal aspect to expose adequate tooth structure.
Figure 3.
Radiological reevaluation showing the distance between crestal bone and inter proximal preparation level.
Figure 3.
Radiological reevaluation showing the distance between crestal bone and inter proximal preparation level.
Sutures were finally advocated after reapplication of the gingiva to provide a healing less exposing the operation site to the oral environment (
Figure 4) [
18].
Provisional restoration was relined and modified within the refined preparation according to new gingival margins. It was cemented with non Eugenol Temporary Cement (
Figure 5) which would guide the healing process.
Figure 4.
Crown lengthening.
Figure 4.
Crown lengthening.
A special care was given to the buccal morphology of the provisional through which a correct Zenith was created and post operatively maintained.
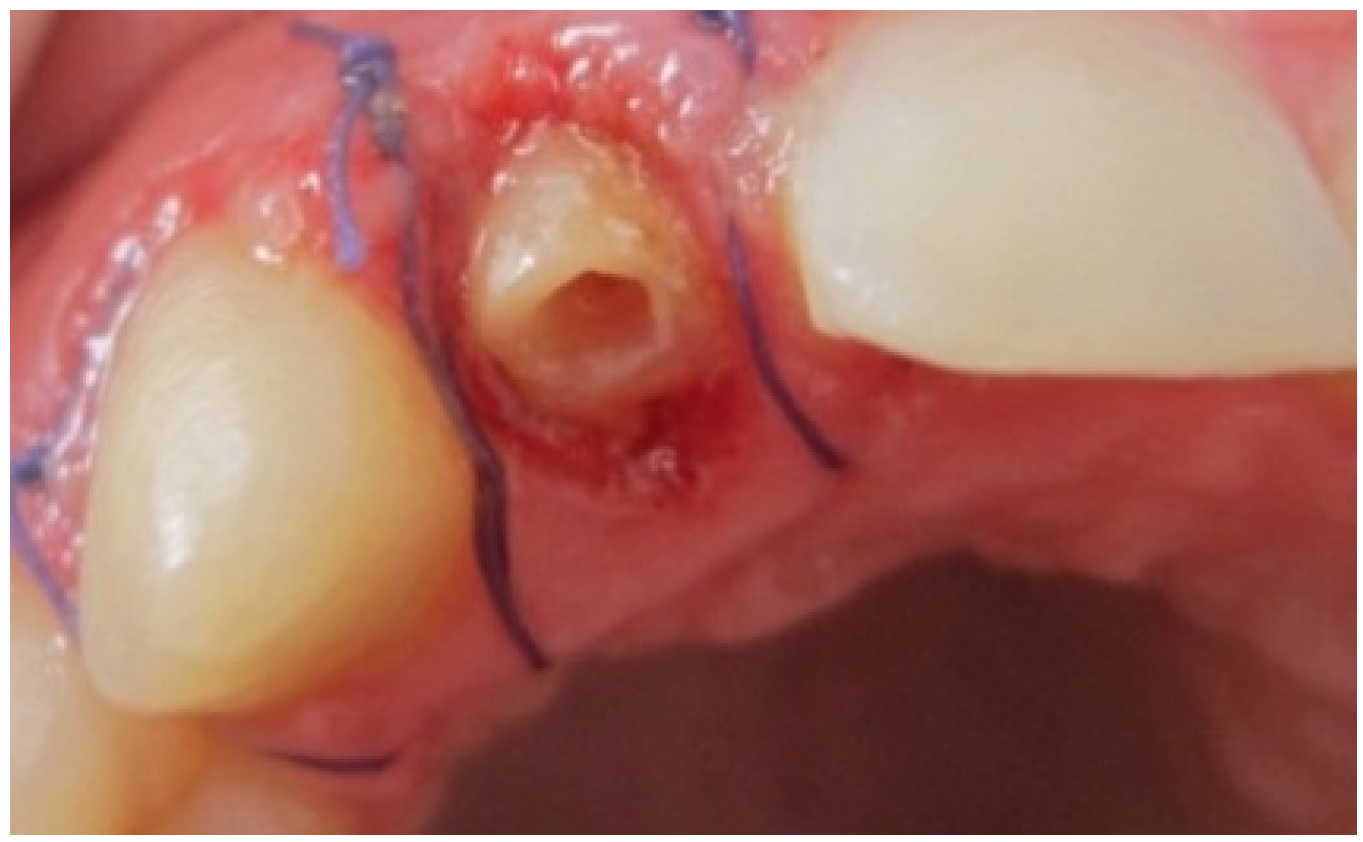
After 4 months of maturation, the abutment tooth was refined after placement and buildup of post and core materials (
Figure 6). Later, a full arch impression was taken using a silicone material. An impression of the opposing dentition was also made with irreversible hydrocolloid. The shade was determined with the shade guide (VITA). The final restoration, Zirconia based crown, showing natural appearance with a correct gingival architecture was performed using the CAD/CAM technology. All of the team, including the prosthodontist, periodontist and the ceramist, were satisfied by the result—an aesthetic and functional restoration with a good marginal adaptation and an improved pink and white score (
Figure 7). The most grateful of all was, however, our satisfied patient.
Figure 6.
Aesthetic post and core system build up.
Figure 6.
Aesthetic post and core system build up.
Figure 7.
Final result showing an improvement of aesthetic appearance.
Figure 7.
Final result showing an improvement of aesthetic appearance.
3. Discussion
Crown lengthening has been suggested to reduce the amount of gingival display because it is considered as unaesthetic when it is more than 3 mm in length [
17]. In addition, it raises the height of the lateral incisor and corrects the gingival architecture in order to obtain a correct gingival Zenith location. In addition to establishing gingival symmetry, it would facilitate the achievement of a proper height-to-width ratio for the lateral incisor and increase the retention of the definitive restoration. Gingivectomy is shown in cases when a large band of attached gingival is available [
15].
The time span between the surgery and the final positioning of the gingival margins has been stated by Gibson who reported that the stability is achieved after 4 months while Bragger
et al. found that changes occur for up 6 months after treatment. These changes included both increase and decrease in clinical crown length determined by the finally stabilized position of the gingival margins [
5,
15]. Whereas, other authors mentioned that osseous remodeling continues histologically for longer than 12 months [
5], soft tissues healing is mostly completed after 8 weeks and the definitive restoration can be placed successfully within 8–12 weeks [
5].
Despite the fact that general periodontal stability is reached after 3 months, other authors have recommended a period of 6 months in the aesthetic zone before dealing with any prosthetic treatment [
1].This approach arises on one hand from the studies’ results which proved that a recession of 2 mm was observed in 12% of the patients when a surgical technique is performed. On the other hand, the stability of the most critical zone which is defined as the distance between the level of the finishing line and the level of alveolar crest is reached after a period of 6 months [
18]. Moreover, impression taking can be traumatic with the use of retraction cord. When a crown lengthening was performed, special care must be given to the impression step to avoid recession. This can be achieved by the use of a minimally invasive procedure avoiding any traumatic procedure during gingival retraction by choosing one step master impression with a gingival retraction paste/gels such as Expasyl which is a universally accepted and widely used gingival paste [
19].
The use of a metal free post and core systems has facilitated the aesthetic restoration of endodontically treated teeth. The objective of a post-and-core buildup was to sufficiently replace missing coronal tooth structure to provide adequate retention and resistance for the crown. In addition to the biocompatibility of the restoration, it allows the preservation of maximum coronal and root structure. As shown, this post and cores system requires sound hard tissues supra gingivally placed which is necessary for a successful secure bonding.
The demand for aesthetics has risen dramatically and zirconia seems to be an adequate material which can respond to those aesthetic demands with a high resistance to fracture and a natural appearance. It is the most suitable material to be used when covering devitalized teeth because it does not allow light transmission through the abutment tooth and it masks its intrinsic coloration. Allying free metal post and core system with an all ceramic restoration achieves a high aesthetic level avoiding dark areas under the prosthesis which can be produced by the use of a non-aesthetic post and core system.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}