Oronasal Fistula and Complete Edentulism: What to Do?

1
Dental Officer, Guru Nanak Dev Dental Hospital, Sultanpur Lodhi, Kapurthala 144626, Punjab, India
2
Medical Officer, ECHS Polyclinic, Kapurthala 144601, Punjab, India
*
Author to whom correspondence should be addressed.
Dent. J. 2014, 2(4), 142-154; https://doi.org/10.3390/dj2040142
Submission received: 19 August 2014
/
Revised: 26 October 2014
/
Accepted: 13 November 2014
/
Published: 5 December 2014
Abstract
:Oronasal fistula is an internal fistula which represents an abnormal epitheliazed tract between oral and nasal cavity, thus impairing associated functions of deglutition and speech by nasal regurgitation of fluid and nasal speech respectively, besides risk of nasal infection resulting from food lodgement. This paper provides a brief yet definitive insight on the etiology, diagnosis and surgical closure of oronasal fistula along with a case report and discussion on prosthodontic rehabilitation of a 65 year old female with an iatrogenic oronasal fistula developed as a result of maxillary molar extraction using a complete metal based denture.
1. Introduction
Fistula refers to a communicating track between two epithelial surfaces, commonly between a hollow viscus and the skin (external fistula) or between two hollow viscera (internal fistula), lined with granulation tissue which is subsequently epitheliazed [1]. By definition, Oronasal fistula (ONF) is an internal fistula and represents an abnormal epitheliazed track communicating between nasal cavity and mouth.
1.1. Etiology
ONF has multifactorial etiology; however, few possible causes are listed below:
1.1.1. Infectious
Various fungi like Rhizopus, Mucormycosis and Aspergillus spp. are found associated with ethmoidal and maxillary sinusitis, nasal and palatal ulceration which might develop into ONF sometimes. Additionally, Phycomycetes, Candida spp and Rhinosporidium spp have been known to cause mycotic infections of nasal cavity and paranasal sinuses with Aspergillus believed to be most commonly involved [2]. They can affect healthy individuals, however patients with immunity lowered by local factors (prosthesis irritation, xerostomia), medications (antibiotics use and/or abuse, immunosuppressants), treatment regimens (chemotherapy, radiotherapy) and systemic disorders (physical debilitation, malnutrition, endocrine and immune disorders) are particularly at predisposition [3]. Allergic, non-invasive, invasive or fulminant are various clinical forms of nasal mycosis which usually present clinically with nasal obstruction, rhinorrhoea, epitasis, proptosis and facial swelling [4], and are possibly sourced from insects, vegetations and patient fingernails by modes of implantation, contamination and inoculation respectively [5]. Other infections which might cause ONF are spirocheatal (syphilitic gumma), bacterial (leprosy) or parasitic (leishmaniasis) and polymicrobial (noma) [6].
1.1.2. Iatrogenic
ONF might be iatrogenic occurring as a possible postoperative complication in minor or major surgical procedures like surgical repair of cleft lip and palate, osteotomies, orthognathic surgeries and dental extractions. Further, maxillary counterparts of complete dentures incorporated with suction discs to improvise retention may also cause palatal necrosis and lead to ONF [6]. However, fistulas forming following failure of cleft palate repair have a high reported incidence ranging from 0% to 68% [7], and may occur anywhere along the original cleft(s) with hard palate and the junction of hard and soft palate showing greater predilection [8]. Multiple etiologies have been proposed regarding its formation: (1) Tissue breakdown due to tension at the site of wound closure [9]; (2) Tension after maxillary orthodontics; (3) Infection [10]; (4) Hypoxemia [8]; and rarely (5) hematoma formation, but mucoperiosteal flap necrosis is considered the most common cause, especially in the event of greater palatine artery injury [9]. Certain factors influencing ONF following cleft palate repair are severity and type of cleft, timing and technique of repair and experience level of the operating surgeon [7].
1.1.3. Traumatic
Saggital palatal fracture occurring with a palate alveolar fracture or with a comminuted Le Fort fracture may sequentiate to ONF in late post traumatic period, presenting clinically as a step deformity with or without palatal mucosal laceration and non-centralized fracture line due to vomer reinforcement in the middle. To avoid missing this diagnosis in cases with intact mucosa, palatal palpation is very important [11]. Secondly, palatal perforation caused by forceful slipping of extraction instruments (straight elevator and chisel) during upper posterior teeth removal and process of retrieving dental implant pushed into the nasal cavity also might create an oronasal communication (ONC), which if not treated timely and adequately, leads to ONF.
1.1.4. Patient Compliance
Poor patient compliance in form of careless postoperative behavior regarding oral hygiene, following prescribed drug regime and attending follow up visits might serve as a contributory factor in ONF development. It can be improved by encouragement and motivation of patient by attending surgeon and family members and if required, counseling sessions should also be arranged.
1.1.5. Tumor and Cystic Resection
Tumors involving maxilla and other anatomically related structures may require surgical management and resection of involved area, resulting in ONF. Besides, developmental cysts like nasopalatine duct cyst, median palatal cyst, globulomaxillary cyst, nasoalveolar cyst and odontogenic cyst like periapical cysts also when treated by enucleation and curettage may destroy bony floor of nasal cavity and lead to ONF. Malignant tumors of upper gum and hard palate account for 1%–5% of malignant neoplasms of the oral cavity and two thirds of the lesions involving these areas are squamous cell carcinomas [12]. Table 1 proposes a list of common and uncommon tumors involving palate.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumors Involving Palate | |
|---|---|
| Common | Uncommon |
| Basal cell carcinoma | Squamous papilloma |
| Squamous cell carcinoma | Verrucous carcinoma |
| Pleomorphic adenoma | Verruciformxanthoma |
| Mucoepidermoid carcinoma | Nasopharyngeal angiofibroma |
| Adenoid cystic carcinoma | Chondroma |
| Polymorphous low grade adenocarcinoma | Liposarcoma |
| Carcinoma ex pleomorphic adenoma | Myoepithelioma |
| Oral hemangioma | Basal cell adenocarcinoma |
| Oral fibroma | Intraductal papilloma |
| Giant cell fibroma | Extramedullary plasmacytoma |
| Torus palatines | Adenomatoid odontogenic tumor |
Maxillary tumors are usually handled surgically, either by conservative approach in localised lesions or by wide or radical approach in more aggressive lesions which includes maxillectomy, a process of partial or total removal of maxilla in a patient suffering from benign or malignant neoplasm [13].The resultant surgical defect often includes part of hard and soft palate, which results in an oroantral and/or oronasal communication [14]. Rehabilitation can be accomplished either surgically or prosthetically [15].
1.1.6. Rhinolithiasis
Exogenous (such as grains, small stone fragments, plastic parts, seeds, insects, glass, wood and others) or endogenous (dry secretion, clots, cell lysis products, mucosa necrosis and tooth fragments) products may act as foreign bodies [16], and lodge into nasal cavity resulting in an uncommon disease which may present asymptomatically showing characteristic presence of mineralized tumor [17], large enough to cause nasal septum perforation or deviation, oroantral and oronasal fistula, chronic sinusitis and destruction of lateral nasal wall [18]. Usual symptoms are progressive unilateral nasal obstruction, rhinorrhea (usually purulent and fetid), cacosmia and epistaxis with headache, facial pain and epiphora seen less commonly [19].
1.1.7. Congenital
Nasal cavity is separated from oral cavity, anteriorly by premaxilla and maxilla and posteriorly by the horizontal plate of palatine bone [20]. Factors resulting in incomplete interfusion of these bones create a possibility of cleft palate development or less commonly, ONC which if not treated, may develop into ONF. These factors might include an alteration in the normal fusion process, defect in regional vascular supply, a mechanical alteration in tongue size, intoxication with substances such as alcohol, drugs or toxins, infections, lack of development and a serious defect produced by a mutant gene, or a small defect caused by several genes [21]. Few developmental disorders like fibrous dysplasia and midfacial hypoplasia might be associated with such defects.
1.2. Causes of Persistence of Fistula
The presence of maxillary sinusitis, epithelialization of the fistula tract, osteitis or osteomyelitis on fistula margins, a foreign body, dental cysts, a dental apical abscess, or tumors prevent spontaneous healing and result in chronic fistulas [1].
1.3. Diagnosis
1.3.1. Diagnostic Criterias
Few criterias which might serve in diagnosis of ONF are [22]:
- Air escape from the opening when patient blows his/her nose;
- An obvious communication between the opening and floor of the nasal cavity;
- Unobstructed penetration of Gutta percha through the opening into the nasal cavity;
- Occlusal radiographs;
- Apart from these, symptoms associated with ONF also help in its diagnosis.
1.3.2. Signs and Symptoms
Depend on the size and location of the fistula and include [23]:
- Hypernasality of voice due to audible nasal air escape during speech;
- Nasal regurgitation of fluids;
- Food lodgement into nasal cavity with risk of rhinitis and tonsillitis.
ONF is most commonly observed on the junction between soft and hard palate. However, based on size, it can be categorized into 3 types: small (<2 mm), medium (3–5 mm) and large (>5 mm) [24]. Many support that an area exceeding 4.5 mm2 to 5 mm2 (i.e., medium and large) could interfere with speech causing hypernasality, audible nasal escape and weakness of pressure consonants compared to some, which suggest that fistulas of only few millimeters square can affect speech and resonance [25]. Possible influence on speech can be examined by a simple method which includes temporarily covering the fistula with dental wax or a palatal plate [26], and observing speech quality before and after coverage. Diminished nasalization following temporary coverage suggests that fistula is the cause of nasality. Further, small fistulas cause nasal regurgitation of fluid, and nasal secretions enter the mouth several times, thus, building unpleasant taste and halitosis. Depending on the extent of functional impairment, ONF may have psychological, social, and developmental consequences and should be repaired [23].
1.4. Surgical Closure
1.4.1. Preoperative Clinical Assessment
Osseous defects are most likely much larger than mucosal defects necessitating preoperative assessment/measurement of this size difference, which may be done radiographically as well as clinically by probing of fistula margins with a suitable instrument after local anaesthetization of the patient [22].
1.4.2. Surgical Closure Methods
They can be broadly divided in two groups: those using mucoperiosteal flaps in one form or another, e.g., hinge flaps [27], and those obtaining additional tissue usually in the form of pedicled flaps from another site in mouth, e.g., buccal mucosa [28], tongue flaps [29], mucoperiosteal alveolar ridge tissue, and mucoperiosteal elevations [30]. Although these methods may prove beneficial in certain cases, most are relatively cumbersome and are often complicated by postoperative risks and problems including tissue loss at donor site, hindered maxillary growth as a result of scar contracture, poor aesthetic result, and, most importantly, recurrence of the fistula with an incidence as high as 34% [8].
Double layered closure provides adequate coverage, added strength and vascularity of the flap and is often desirable [22]. Further, ONF cases resulting from mycotic infections should be managed with adequate antifungal treatment along with surgical or prosthodontic rehabilitation.
1.4.3. Flap Selection Factors [22,31,32]
| Patient | Defect | Surgeon |
|---|---|---|
| Age | Location | Familiarity with surgical methods surgical methods |
| General condition | Size | Experience |
| Economical status | Etiology | Dexterity |
| Willingness | Severity | |
| Associated scarring | ||
| Duration |
1.4.4. Surgical Contraindications
Surgical rehabilitation of defect is preferred in most cases; however, general medical condition and age of patient, anatomic complexity, possibility of recurrence, appearance of the area to be rehabilitated and complexity of the surgical procedure may contraindicate surgical reconstruction [31].
1.4.5. Surgical Closure in Traumatic and Iatrogenic ONF
Primary surgical closure at the time of initial injury is usually not considered, because hematoma and tissue injury compromise vascularity of donor area thus increasing the possibility of flap breakdown. Instead, delaying this closure allows surrounding tissues to regain vascularity, and often bony and soft tissue healing result in a small final defect which is easy to close and has better flap prognosis [22]. Meechan reported a case of iatrogenic ONF which presented after simple extraction of left upper central incisor and was closed by an immediate partial denture, without any surgical closure. Comparatively, in cases where the continuity of nasal lining is breached, a proper surgical closure is required [33].
2. Case Presentation
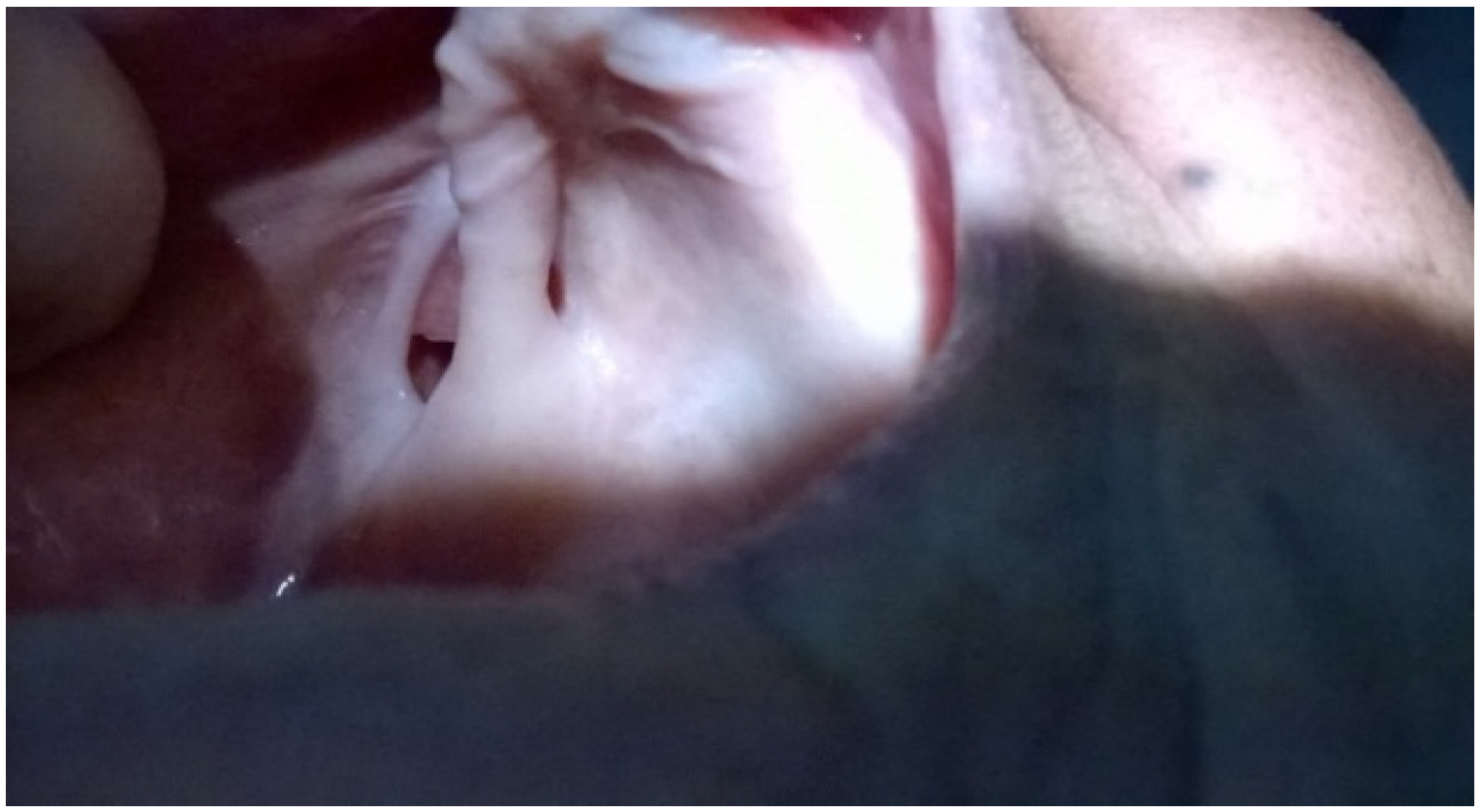
A 65 year old female patient presented at Guru Nanak Dev Dental Hospital, SultanpurLodhi, Kapurthala with a chief complaint of complete edentulousness and wished for full mouth rehabilitation. Intraoral examination showed an oronasal fistula (ONF) with oral side of the defect extending into buccal vestibule and lateral hard palate on right side (Figure 1), with a reasonable amount of residual alveolar ridge still overlying which helped in achieving necessary retention of denture(Figure 2). She further gave a history of nasal regurgitation of fluid, food lodgement in the defect and hypernasality of voice.
Figure 1.
Right lateral view.

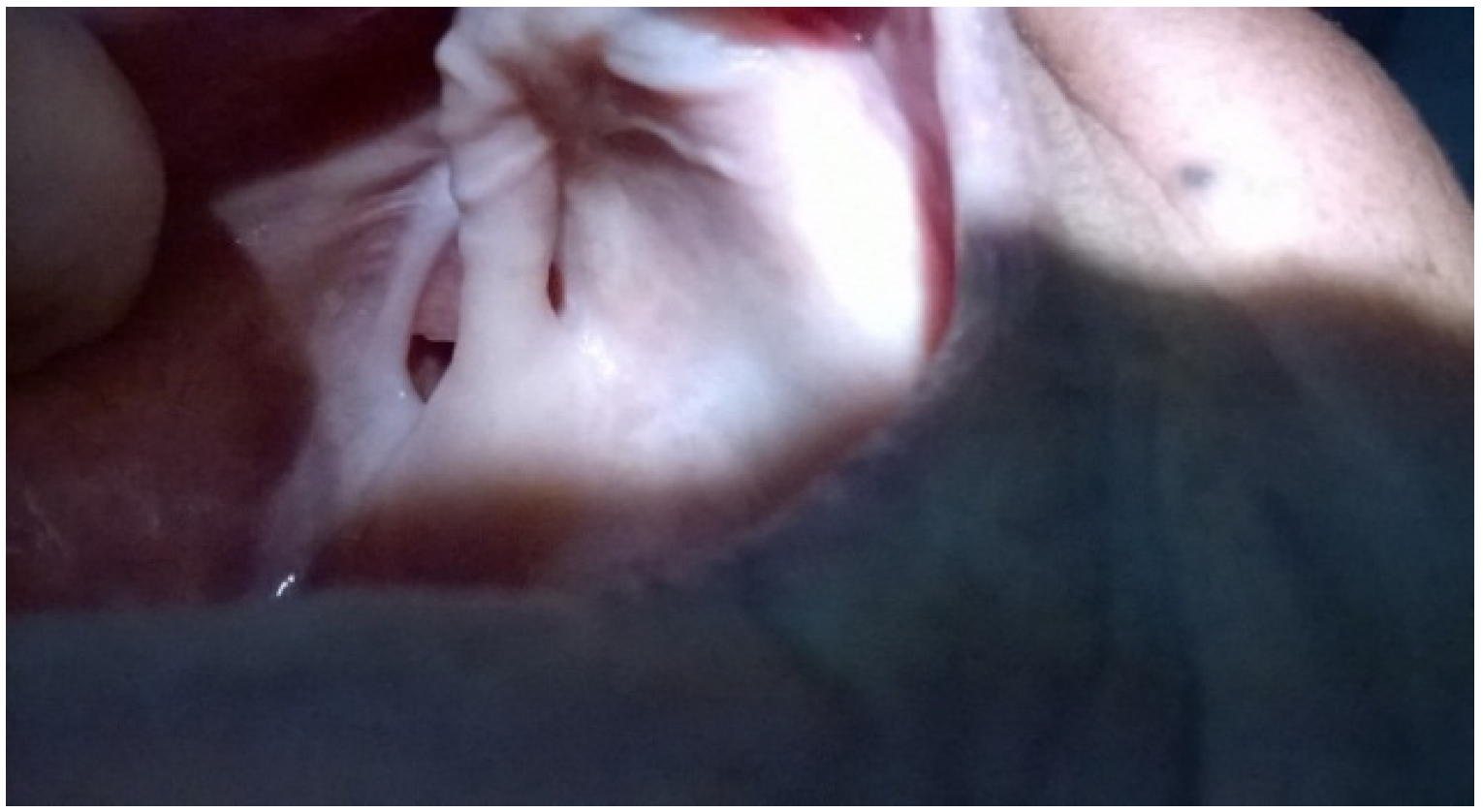
Figure 2.
Left lateral view of oronasal fistula (ONF). Fistula can be seen extending from right buccal vestibule to right lateral part of hard palate with a reasonable amount of alveolar ridge overlying the defect.
Figure 2.
Left lateral view of oronasal fistula (ONF). Fistula can be seen extending from right buccal vestibule to right lateral part of hard palate with a reasonable amount of alveolar ridge overlying the defect.
Dental history revealed an eventful extraction in this particular area during full mouth extraction course, which involved uncontrolled bleeding and was managed by a hemostatic plug and sutures but unfortunately led to infection and palatal necrosis requiring surgical removal of the necrosed area. General examination showed normal build and gait and no other abnormalities. However, the patient gave an approximately30-year long positive medical history of type 2 Diabetes Mellitus and associated diabetic neuropathy. Further, no other systemic disorders or family history of any disease was reported.
After discussing in detail possible treatment options and considering patient’s general medical condition, age, and interest, it was decided to plan a complete metal based denture which helped fulfilling two main objectives: prosthodontic restoration of complete edentulous state and obliteration of fistula to rectify associated functional, social and psychological impairments. Surgical closure was proposed but the patient immediately refused for another surgery. However, the expectations from this prosthesis were thoroughly explained to the patient.
Maxillary and mandibular preliminary impressions were taken in stainless steel stock trays using irreversible hydrocolloid as the impression agent (Neocolloid, Zhermack Clinical). Prior to this, the defect was carefully packed with petrolatum gauze to restrict passage of impression material into nasal cavity yet allowing a limited amount to flow and accurately record the vestibular and palatal boundaries of defect for obtaining its positive replica. This step was quite technique sensitive in terms of loading appropriate amount of impression material, applying optimal force during placement and intactly removing the impression without straining or tearing of the alginate. These impressions were poured with type 3 dental stone to obtain anatomic models (Figure 3a,b) on which autopolymerised acrylate custom trays were made which after necessary trimming and border molding with green stick compound (DPI PINNACLE), were used for recording functional impressions using silicone impression pastes (DPI) and poured to produce working models. The defect was again obturated with petrolatum gauze before taking functional impression for similar reasons. On a maxillary working model, the vestibular defect was filled with dental stone while the palatal part was sealed with wax to facilitate processing and accurate adaptation of cast metal base (Figure 4a, b). Further, maxillary and mandibular bite templates were made and the mesh pattern present in the portion of this metal base covering alveolar crest, containing small square perforations helped increase the bonding of modeling wax and heat cure acrylic with metal base in bite templates and final prosthesis respectively (Figure 5).
Figure 3.
(a) Primary maxillary cast showing positive replica of the defect; (b) The defect is highlighted with black circles where the small circle shows the palatal part and the large circle shows vestibular part of the defect.
Figure 3.
(a) Primary maxillary cast showing positive replica of the defect; (b) The defect is highlighted with black circles where the small circle shows the palatal part and the large circle shows vestibular part of the defect.

Figure 4.
(a) Secondary maxillary cast where the defect is obliterated with wax on the palatal side and with dental stone on the vestibular side; (b) Black circle highlights the vestibular part of defect closed with dental stone.
Figure 4.
(a) Secondary maxillary cast where the defect is obliterated with wax on the palatal side and with dental stone on the vestibular side; (b) Black circle highlights the vestibular part of defect closed with dental stone.

Figure 5.
Cast metal base adapted on secondary cast. The part of metal base overlying alveolar crest region contains mesh pattern with small square perforations to improve the bonding of wax and heat cure acrylic with metal plate in bite templates and final prosthesis respectively.
Figure 5.
Cast metal base adapted on secondary cast. The part of metal base overlying alveolar crest region contains mesh pattern with small square perforations to improve the bonding of wax and heat cure acrylic with metal plate in bite templates and final prosthesis respectively.

These bite templates were then used for recording maxillo-mandibular jaw relations (Figure 6) and transferred on to a mean value articulator for diagnostic wax up. Artificial acrylic teeth were selected, arranged, and after patient’s approval (Figure 7), this waxed prosthesis was processed and a heat cured acrylic complete denture with metal base was obtained which was delivered to the patient along with necessary instructions regarding its adequate use, care, and maintenance. The patient attended only one weekly follow up visit and seemed quite satisfied with the prosthesis.
Figure 6.
Maxillo-mandibular relations.

Figure 7.
Try-in.

3. Discussion
In this case, ONF developed following eventful extraction of maxillary molar with uncontrolled postoperative socket infection causing necrosis of adjoining tissues which were surgically removed. Long term diabetes and age factor might have fuelled the postoperative infection by slowing the healing process, lowering immunity through reduced chemotaxis of neutrophils, and enhancing bacterial growth via high blood sugar level. The treatments which could have been proposed in this case are listed as below:
3.1. Surgical Closure of the Defect
Following failure of spontaneous healing post initial surgery, we could have tried different mucoperiosteal flaps and bone grafts, although the success rate was very difficult to establish considering the long diabetic history and mature age of the patient in addition to anatomic complexity of defect. Nevertheless, it was clearly refused by the patient due to reasons best known to her which possibly might be: ignorance, financial inadequacy, lack of awareness and will.
3.2. Prosthodontic Rehabilitation
Since this patient was completely edentulous, a complete denture was necessary with or without surgical closure of fistula. Also, maxillary obturator prosthesis is more frequent treatment modality than surgical reconstruction due to ease of fabrication and maintenance [34].
3.2.1. Implant Supported Denture
This method required placement of dental implants in both maxilla and mandible in order to support the overdenture. However, it was not preferred in this case due to different reasons which included mediocre socio-economic status of patient, long term diabetic history, old age, and poor bone support in the involved area. The palatal and vestibular portions of the defect communicated with each other beneath the residual alveolar ridge thus compromising local bony structure and making implant placement quite challenging.
3.2.2. Prosthesis Incorporating Magnets
In this method, maxillary prosthesis consisted of two separate components, a bulb obturator to seal off the defect and maxillary denture for dental rehabilitation. Both these components were incorporated with magnets to increase retention of maxillary denture. However, the usefulness of this method in this case was doubtful possibly because it is used in:
- Cases with large sized defects where the weight of single piece prosthesis is over the limit and counteracts retentive force of denture thus compromising its success.
- When volume of prosthesis is large enough to interfere with its removal from mouth.
- When the defect is in or near center compared to off center position as seen in this case making it difficult to manage.
3.2.3. Conventional Denture
After discussing available options with the patient and satisfying her will, it was decided to manage the defect prosthodontically with conventional complete denture. The complete process of its fabrication has been explained in detail above under Section 2. After delivering the final prosthesis, the patient was scheduled for follow up visits, of which she attended just one. However, she seemed quite satisfied with the prosthesis and did not experience any impairment.
3.3. Prosthetic Rehabilitation
In case an ONF progresses further to form an oronasal defect involving nasal structures along with palate, treatment plan should also include rehabilitation of facial structure with the help of bio materials. Methyl methacrylate resin has been used as a maxillofacial material because it is easy to work with, hygienic, durable, and economical. Also, it can be satisfactorily colored to match individual skin tone. However, its use is limited by its rigidity. Although attempts have been made to greatly improve the properties of various maxillofacial materials, there is still no ideal material that resembles or duplicates human skin. Approaches and techniques that attempt to achieve an accurate skin color match include trial-and-error mixing, shade guides, pigment dispersion systems and color measurements using a colorimeter or spectrophotometre [35].
4. Conclusion
Oronasal fistulas are abnormal epitheliazed tracts communicating between nasal and oral cavity which have multiple etiologic factors and result in speech and deglutition related functional impairments. In this case, an eventful maxillary molar extraction during full mouth extraction course caused uncontrollable postoperative infection and resultant palatal necrosis thus adding an Iatrogenic ONF to completely edentulous state. Accordingly, case management was done with two main objectives of sealing the debilitating defect and rehabilitation of complete edentulism. After detailed discussion regarding available treatment options, a metal based complete denture was planned, which successfully solved both objectives. This case was handled prosthodontically, mainly because a denture was essential for rehabilitation of complete edentulism even if the defect was closed successfully. Secondly, the patient directly refused another surgery. However, the patient was well satisfied with the final prosthesis and its outcomes.
Acknowledgements
We would like to thank the patient for her cooperation throughout the procedure and consent.
Author Contributions
Both authors contributed equally to this work.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Das, S. Examination of a Sinus or a Fistula. In A manual on Clinical Surgery, 5th ed.; Old Mayors Court: Calcutta, India, 2001; p. 55. [Google Scholar]
- Stammberger, H.; Jaske, R.; Beaufort, F. Aspergillosis of the paranasal sinuses, X-ray diagnosis, histopathology of clinical aspects. Ann. Otol. Rhinol. Laryngol. 1984, 93, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Nikawa, H.; Egusa, H.; Makihira, S.; Yamashiro, H.; Fukushima, H.; Jin, C.; Nishimura, M.; Pudji, R.R.; Hamada, T. Alteration of the coadherence of candida albicans with oral bacteria by dietary sugars. Oral Microbiol. Immun. 2001, 16, 279–283. [Google Scholar] [CrossRef]
- Mackay, I.S.; Bull, T.R. Rhinology. In Scott-Brown’s Otolaryngology, 6th ed.; Butterworth Heinemann: Oxford, UK, 1997; Volume 4, pp. 39–49. [Google Scholar]
- Martinson, F.D. Zygomycosis in otorhinolaryngology practice. Prog. Oto. Rhino. Laryngol. 1983, 29, 224–230. [Google Scholar]
- Eppley, B.; Sclaroff, A. Oronasal fistula secondary to maxillary augmentation. Int. J. Oral. Surg. 1984, 13, 535–538. [Google Scholar] [CrossRef] [PubMed]
- Emory, R.E.; Clay, R.P.; Bite, U.; Jackson, I.T. Fistula formation and repair after palatal closure: An institutional perspective. Plast. Reconstr. Surg. 1997, 99, 1535–1538. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.R.; Kalinowski, J.; LaRossa, D.; Randall, P. Cleft palate fistulas: A multivariate statistical analysis of prevalence, etiology and surgical management. Plast. Reconstr. Surg. 1991, 87, 1041–1047. [Google Scholar] [CrossRef] [PubMed]
- Reid, D.A.C. Fistula in the hard palate following cleft palate surgery. Br. J. Plast. Surg. 1962, 15, 377–384. [Google Scholar] [CrossRef] [PubMed]
- McClelland, R.M.A.; Patterson, T.J.S. The influence of penicillin on the complication rate after repair of clefts of the lip and palate. Br. J. Plast. Surg. 1963, 16, 144–145. [Google Scholar] [CrossRef]
- Mathog, R.H.; Arden, R.I.; Marks, S.C. Maxillary Trauma. In Trauma of the Nose and Paranasal Sinuses; Thieme: New York, NY, USA, 1995; p. 55. [Google Scholar]
- Muller, S.; Waldron, C.A. Primary intra osseous squamous carcinoma. Int. J. Oral Maxillofac. Surg. 1991, 20, 362–365. [Google Scholar] [CrossRef] [PubMed]
- Spiro, R.H.; Strong, E.W.; Shah, J.P. Maxillectomy and its classification. Head Neck. 1997, 19, 309–314. [Google Scholar] [PubMed]
- Jacobs, C. Carcinomas of the Head and Neck; Jacobs, C., Ed.; Kluwer Academic Publishers: Boston, MA, USA, 1990; pp. 83–113. [Google Scholar]
- Thawley, S.E.; Batsakis, J.G.; Lindberg, R.D.; Panje, W.R.; Donley, S. Comprehensive Management of Head and Neck Tumors, 2nd ed.; Thawley, S.E., Batsakis, J.G., Lindberg, R.D., Panje, W.R., Donley, S., Eds.; Elsevier: St. Louis, MO, USA, 1998; pp. 526–527. [Google Scholar]
- Aksungur, E.H.; Binokay, F.B.; Biçakçi, K.; Apaydin, D.; Oguz, M.; Aydogan, B. A rhinolith which is mimicking a nasal benign tumor. Eur. J. Radiol. 1999, 31, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.G.; Sahni, R.C. Unilateral rhinolithiasis. Australas. Radiol. 1981, 25, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Price, H.I.; Batnitzky, S.; Karlin, C.A.; Norris, C.W. Giant nasal rhinolith. Am. J. Neuroradiol. 1981, 2, 371–373. [Google Scholar] [PubMed]
- Celikkanat, S.; Turgut, S.; Özcan, I.; Balyan, A.R.; Ozdem, C. Rhinolithiasis. Rhinology 1997, 53, 39–40. [Google Scholar]
- Lang, J. Nasal cavity. In Clinical Anatomy of the Nose, Nasal Cavity and Paranasal Sinuses; Thieme: New York, NY, USA, 1989; p. 46. [Google Scholar]
- Abadi, B.; Johnson, J.D. The prosthodontic management of cleft palate patients. J. Prosthet. Dent. 1982, 48, 297–302. [Google Scholar] [PubMed]
- Ahmed, M.V.; Naz, F.; Chand, M.A.U.H.; Tambuwala, A.; Kaul, D. Repair of iatrogenic oronasal fistula after periapical surgery. Univ. Res. J. Dent. 2012, 2, 83–86. [Google Scholar]
- EL-Leathy, M.M.; Attia, M.F. Closure of palatal fistula with bucco-labial myomucosal pedicled flap. Ann. Pediatr. Surg. 2009, 5, 104–108. [Google Scholar]
- Muzzafar, A.R.; Byrd, H.S.; Rohrich, R.J.; Johns, D.F.; LeBlanc, D.; Beran, S.J.; Anderson, C.; Papaioannoua, A.A. Incidence of cleft palate fistula: An institutional experience with two stage palate repair. Plast. Reconstr. Surg. 2001, 108, 1515–1518. [Google Scholar] [CrossRef] [PubMed]
- Henningson, G.; Isberg, A. Oronasal fistulas and speech production. In Multidisciplinary Management of Cleft Lip and Palate, 1st ed.; Bardach, J., Morris, H.L., Eds.; WB Saunders: Philadelphia, PA, USA, 1990; pp. 787–791. [Google Scholar]
- Riski, J.E. Evaluation and management of speech, language, and articulation disorders. In Cleft Lip and Palate from Origin to Treatment; Wyszynski, D.F., Ed.; Oxford University Press: New York, NY, USA, 2002; pp. 354–367. [Google Scholar]
- Rintala, A.E. A double, overlapping hinge flap to close palatal fistulae. Scand. J. Plast. Reconstr. Surg. 1971, 5, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Nakakita, N.; Maeda, K.; Ando, S.; Ojimi, H.; Utsugi, R. Use of a buccal musculomucosal flap to close palatal fistulae after cleft palate repair. Br. J. Plast. Surg. 1990, 43, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Argamaso, R.V. The tongue flap: Placement and fixation for closure of post palatoplasty fistulae. Cleft Palate J. 1990, 27, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Stark, R.B. Cleft palate. In Plastic Surgery of the Head and Neck; Churchill Livingstone: New York, NY, USA, 1987; pp. 1300–1301. [Google Scholar]
- Shah, S.A.; Naqash, T.A.; Abdullah, S.; Zargar, N.M.; Jangral, S. Prosthetic rehabilitation of a patient with limited mouth opening consequent to partial maxillectomy: A clinical report. Int. J. Health Sci. Res. 2013, 3, 82–87. [Google Scholar]
- Diah, E.; Lu, L.J.; Yun, C.; Wang, R.; Wahyuni, L.K.; Chen, Y.R. Cleft oronasal fistula: A review of treatment results and surgical management algorithm proposal. Chang. Gung Med. J. 2007, 30, 529–537. [Google Scholar] [PubMed]
- Meechan, J.G. Oronasal fistula occurring after simple dental extraction. Br. J. Oral. Surg. 1983, 2, 229–232. [Google Scholar] [CrossRef]
- Mukohyama, H.; Haraguchi, M.; Sumita, Y.I.; Iida, H.; Hata, Y.; Kishimoto, S.; Taniguchi, H. Rehabilitation of a bilateral maxillectomy patient with a free fibula osteocutaneous flap. J. Oral Rehabil. 2005, 32, 541–544. [Google Scholar] [CrossRef] [PubMed]
- Anantharaju, A.; Kamath, G.; Mody, P.; Nooji, D. Prosthetic rehabilitation of oro-nasal defect. J. Indian Prosthodont. Soc. 2011, 11, 242–245. [Google Scholar] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kaur, P.; Kaur, J. Oronasal Fistula and Complete Edentulism: What to Do? Dent. J. 2014, 2, 142-154. https://doi.org/10.3390/dj2040142
AMA Style
Kaur P, Kaur J. Oronasal Fistula and Complete Edentulism: What to Do? Dentistry Journal. 2014; 2(4):142-154. https://doi.org/10.3390/dj2040142
Chicago/Turabian StyleKaur, Pushappreet, and Jaspinder Kaur. 2014. "Oronasal Fistula and Complete Edentulism: What to Do?" Dentistry Journal 2, no. 4: 142-154. https://doi.org/10.3390/dj2040142