
Medical and Para-Medical Personnel’ Perspectives on Home Health Care Technology


Abstract
:1. Introduction
2. Materials and Methods
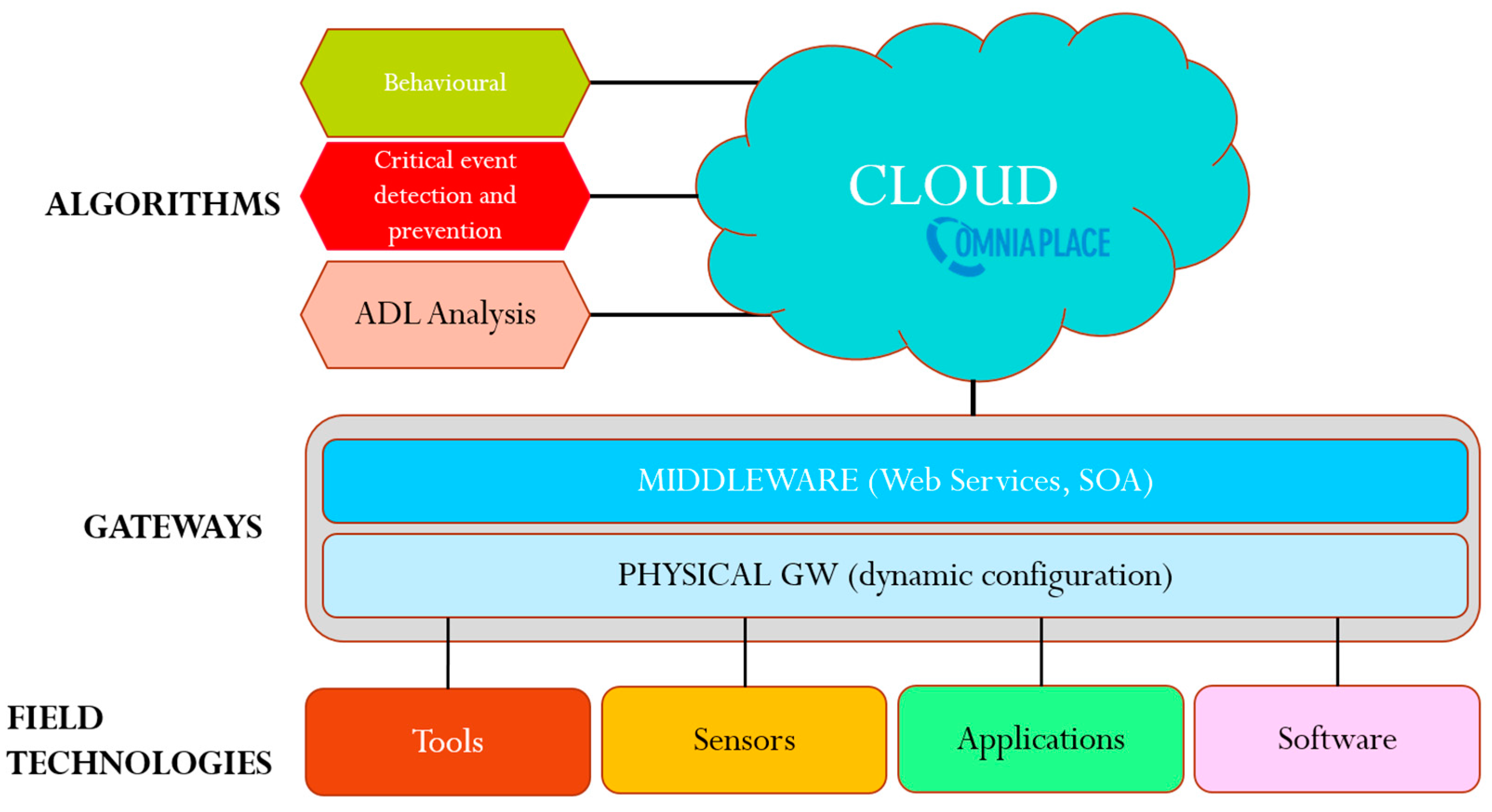
2.1. The AA@H Project
- monitor indicators for health status, physical and intellectual well-being of the individual;
- act as personal guidance, evaluate the individual’s evolution in time and promote correct life styles and behaviors;
- prevent and detect critical situations or risk (e.g., smoke in the room or fall), avoiding false alarms but promptly intervening in case of need;
- promote adequate physical activity;
- epromote active socialization and participation in community life.
2.2. Participants
2.3. The Focus Group
2.4. Data Analysis
3. Results
3.1. Technologies for Ageing in Place
3.2. Clinical Outcomes
3.3. Enablers and Barriers
3.4. Personalized Approach
3.5. Accuracy of Measurements
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kvedar, J.; Coye, M.J.; Everett, W. Connected health: A review of technologies and strategies to improve patient care with telemedicine and telehealth. Health Aff. 2014, 33, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Pol, M.C.; van Nes, F.; van Hartingsveldt, M.; Buurman, B.M.; de Rooij, S.E.; Kröse, B.J.A. Older people’s perspectives regarding the use of sensor monitoring in their home. Gerontology 2014, 56, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Peek, S.T.; Luijkx, K.G.; Rijnaard, M.D.; Nieboer, M.E.; van der Voort, C.S.; Aarts, S.; Wouters, E.J. Older adults’ reasons for using technology while aging in place. Gerontology 2016, 62, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Stroulia, E.; Nikolaidis, I.; Miguel-Cruz, A.; Rios Rincon, A. Smart homes and home health monitoring technologies for older adults: A systematic review. Int. J. Med. Inform. 2016, 91, 44–59. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, P.; Ghapanchi, A.H. Investigating the effectiveness of technologies applied to assist seniors: A systematic literature review. Int. J. Med. Inform. 2016, 85, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Van Gemert-Pijnen, J.E.; Nijland, N.; van Limburg, M.; Ossebaard, H.C.; Kelders, S.M.; Eysenbach, G.; Seydel, E.R. A holistic framework to improve the uptake and impact of eHealth technologies. J. Med. Internet Res. 2011, 13, e111. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.M.; Freeman, M.; Kaye, J.; Vuckovic, N.; Buckley, D.I. A systematic review of clinician and staff views on the acceptability of incorporating remote monitoring technology into primary care. Telemed. E-Health 2014, 20, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- MacNeill, V.; Sanders, C.; Fitzpatrick, R.; Hendy, J.; Barlow, J.; Knapp, M.; Rogers, A.; Bardsley, M.; Newman, S.P. Experiences of front-line health professionals in the delivery of telehealth: A qualitative study. Br. J. Gen. Pract. 2014, 64, e401–e407. [Google Scholar] [CrossRef] [PubMed]
- Odeh, B.; Kayyali, R.; Nabhani-Gebara, S.; Philip, N. Implementing a telehealth service: Nurses’ perceptions and experiences. Br. J. Nurs. 2014, 23, 1133–1137. [Google Scholar] [CrossRef] [PubMed]
- Kolltveit, B.-C.H.; Gjengedal, E.; Graue, M.; Iversen, M.M.; Thorne, S.; Kirkevold, M. Telemedicine in diabetes foot care delivery: Health care professionals’ experience. BMC Health Serv. Res. 2016, 16, 134. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.I.; Gollamudi, S.S.; Steinhubl, S. Digital technology to enable aging in place. Exp. Gerontol. 2016, 88, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Fisk, D.A.; Rogers, W.A.; Charness, N.; Czaja, J.S.; Sharit, J. Designing for Older Adults: Principle and Creative Factor Approaches; CRC Press: Boca Raton, FL, USA, 2009. [Google Scholar]
- Carrettero, S.; Stewart, J.; Centeno, C.; Barbabella, F.; Schmidt, A.; Lamontagne-Godwin, F.; Lamura, G. Can Technology-based Services support Long-term Care Challenges in Home Care? Analysis of Evidence from Social Innovation Good Practices across the EU: CARICT Project Summary Report. In JRC Scientific and Policy Reports; Publications Office of the European Union: Luxembourg, 2012. [Google Scholar]
- Spinsante, S.; Stara, V.; Felici, E.; Montanini, L.; Raffaeli, L.; Rossi, L.; Gambi, E. The Human Factor in the Design of Successful Ambient Assisted Living Technologies. In Ambient Assisted Living and Enhanced Living Environments: Principles, Technologies and Control; Butterworth-Heinemann: Oxford, UK, 2016; Chapter 4; pp. 61–89. [Google Scholar]
- Bowles, K.H.; Dykes, P.; Demiris, G. The Use of Health Information Technology to Improve Care and Outcomes for Older Adults. Res. Gerontol. Nurs. 2015, 8, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Lattanzio, F.; Abbatecola, A.M.; Bevilacqua, R.; Chiatti, C.; Corsonello, A.; Rossi, L.; Bernabei, R. Advanced technology care innovation for older people in Italy: Necessity and opportunity to promote health and wellbeing. J. Am. Med. Dir. Assoc. 2014, 15, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Wahl, H.W.; Matthews, J.T.; Dabbs, A.D.V.; Beach, S.R.; Czaja, S.J. Advancing the aging and technology agenda in gerontology. Gerontologist 2014, 55, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Spanakis, E.G.; Santana, S.; Tsiknakis, M.; Marias, K.; Sakkalis, V.; Teixeira, A.; Tziraki, C. Technology-Based Innovations to Foster Personalized Healthy Lifestyles and Well-Being: A Targeted Review. J. Med. Internet Res. 2016, 18, e128. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N. Scenario | Description of Characters | Indicators of AA@H System | Outcomes of AA@H System |
|---|---|---|---|
| First Scenario | Pino is 68 and lives with his wife, Lucia. Since 5 years he suffers from diabetes and high blood pressure. The medical prescription is to follow a specific diet and make physical activity every day in order to reduce glycaemia and the onset of possible complications | nutrition, weight, mobility, cardiac and physiological parameters | Health prevention Active Ageing |
| Second Scenario | Gina is 76 and live alone since eight years ago her husband passed away. She is in good health apart from a slight overweight, hypertions and some initial cognitive decline | nutrition, weight, stress, mobility, socialization, sleep-wake cycle, cardiac and physiological parameters | Health prevention Active Ageing |
| Socio-Demographics Characteristics | |
|---|---|
| Age (mean ± SD) | 43.2 ± 9.4 |
| Range | 29–60 |
| Gender (M/F) | 4/6 |
| Profession | 3 Geriatricians, 1 Practitioners 2 Nurse |
| Job experience (years) | Mean: 10 ± 2 Range: 1–30 |
| Work setting | INRCA Hospital |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stara, V.; Rossi, L.; Borrelli, G. Medical and Para-Medical Personnel’ Perspectives on Home Health Care Technology. Informatics 2017, 4, 14. https://doi.org/10.3390/informatics4020014
Stara V, Rossi L, Borrelli G. Medical and Para-Medical Personnel’ Perspectives on Home Health Care Technology. Informatics. 2017; 4(2):14. https://doi.org/10.3390/informatics4020014
Chicago/Turabian StyleStara, Vera, Lorena Rossi, and Gianfranco Borrelli. 2017. "Medical and Para-Medical Personnel’ Perspectives on Home Health Care Technology" Informatics 4, no. 2: 14. https://doi.org/10.3390/informatics4020014
APA StyleStara, V., Rossi, L., & Borrelli, G. (2017). Medical and Para-Medical Personnel’ Perspectives on Home Health Care Technology. Informatics, 4(2), 14. https://doi.org/10.3390/informatics4020014