Atrial Fibrillation Predicts Long-Term Outcome after Transcatheter Edge-to-Edge Mitral Valve Repair by MitraClip Implantation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Baseline and Procedural and Post-Procedural Characteristics
2.3. Clinical Follow-Up/Outcome
2.4. Statistical Analysis
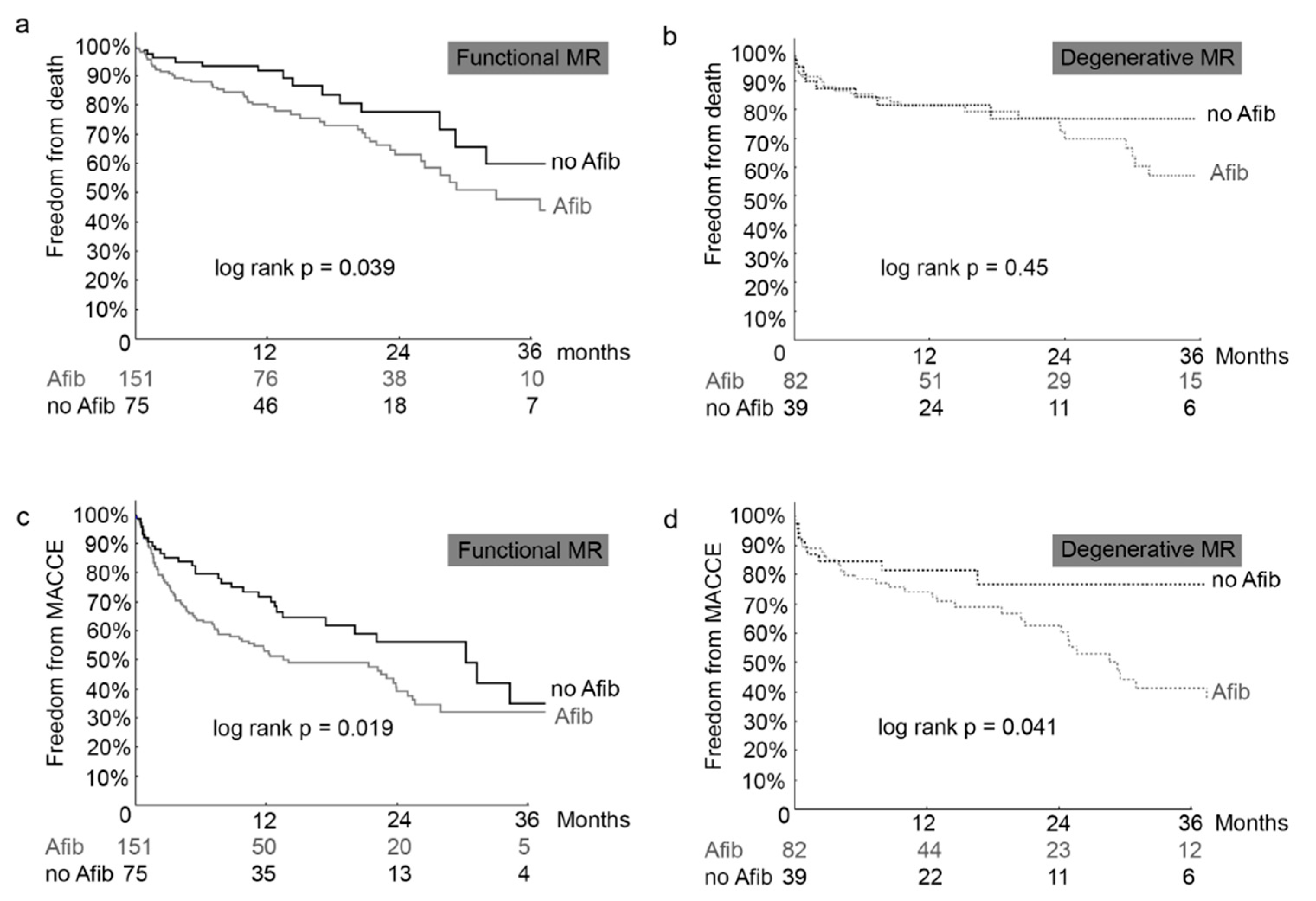
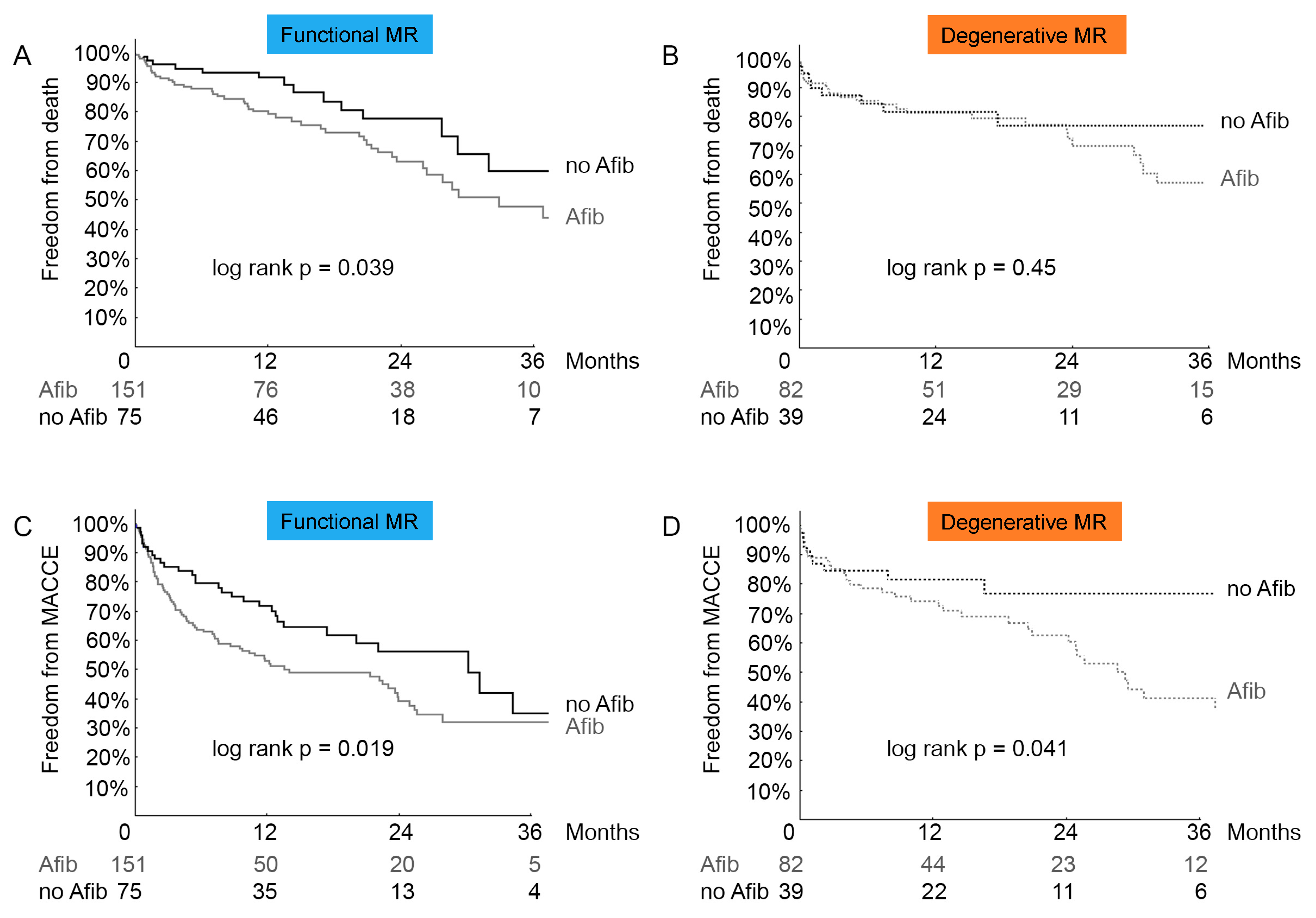
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Inderbitzin, D.T.; Taramasso, M.; Nietlispach, F.; Maisano, F. Percutaneous Mitral Valve Repair with MitraClip: Patient and Valve Selection for Optimal Outcome. Curr. Cardiol. Rep. 2016, 18, 129. [Google Scholar] [CrossRef] [PubMed]
- Feldman, T.; Kar, S.; Elmariah, S.; Smart, S.C.; Trento, A.; Siegel, R.J.; Apruzzese, P.; Fail, P.; Rinaldi, M.J.; Smalling, R.W.; et al. Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation: 5-Year Results of EVEREST II. J. Am. Coll. Cardiol. 2015, 66, 2844–2854. [Google Scholar] [CrossRef] [PubMed]
- Feldman, T.; Kar, S.; Rinaldi, M.; Fail, P.; Hermiller, J.; Smalling, R.; Whitlow, P.L.; Gray, W.; Low, R.; Herrmann, H.C.; et al. Percutaneous mitral repair with the MitraClip system: Safety and midterm durability in the initial EVEREST (Endovascular Valve Edge-to-Edge REpair Study) cohort. J. Am. Coll. Cardiol. 2009, 54, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puls, M.; Lubos, E.; Boekstegers, P.; von Bardeleben, R.S.; Ouarrak, T.; Butter, C.; Zuern, C.S.; Bekeredjian, R.; Sievert, H.; Nickenig, G.; et al. One-year outcomes and predictors of mortality after MitraClip therapy in contemporary clinical practice: Results from the German transcatheter mitral valve interventions registry. Eur. Heart J. 2016, 37, 703–712. [Google Scholar] [CrossRef] [PubMed]
- Maisano, F.; Franzen, O.; Baldus, S.; Schafer, U.; Hausleiter, J.; Butter, C.; Ussia, G.P.; Sievert, H.; Richardt, G.; Widder, J.D.; et al. Percutaneous mitral valve interventions in the real world: Early and 1-year results from the ACCESS-EU, a prospective, multicenter, nonrandomized post-approval study of the MitraClip therapy in Europe. J. Am. Coll. Cardiol. 2013, 62, 1052–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nickenig, G.; Estevez-Loureiro, R.; Franzen, O.; Tamburino, C.; Vanderheyden, M.; Luscher, T.F.; Moat, N.; Price, S.; Dall’Ara, G.; Winter, R.; et al. Percutaneous mitral valve edge-to-edge repair: In-hospital results and 1-year follow-up of 628 patients of the 2011-2012 Pilot European Sentinel Registry. J. Am. Coll. Cardiol. 2014, 64, 875–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L.; Scientific Document Committee of the European Association of Cardiovascular Imaging. Recommendations for the echocardiographic assessment of native valvular regurgitation: An executive summary from the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef] [PubMed]
- Barbash, I.M.; Minha, S.; Ben-Dor, I.; Dvir, D.; Torguson, R.; Aly, M.; Bond, E.; Satler, L.F.; Pichard, A.D.; Waksman, R. Predictors and clinical implications of atrial fibrillation in patients with severe aortic stenosis undergoing transcatheter aortic valve implantation. Catheter. Cardiovasc. Interv. 2015, 85, 468–477. [Google Scholar] [CrossRef] [PubMed]
- Maan, A.; Heist, E.K.; Passeri, J.; Inglessis, I.; Baker, J.; Ptaszek, L.; Vlahakes, G.; Ruskin, J.N.; Palacios, I.; Sundt, T.; et al. Impact of atrial fibrillation on outcomes in patients who underwent transcatheter aortic valve replacement. Am. J. Cardiol. 2015, 115, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Ngaage, D.L.; Schaff, H.V.; Mullany, C.J.; Barnes, S.; Dearani, J.A.; Daly, R.C.; Orszulak, T.A.; Sundt, T.M., 3rd. Influence of preoperative atrial fibrillation on late results of mitral repair: Is concomitant ablation justified? Ann. Thoracic. Surg. 2007, 84, 434–442; discussion 442–443. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, K.; Ohtaki, E.; Matsumura, T.; Tanaka, K.; Tohbaru, T.; Iguchi, N.; Misu, K.; Asano, R.; Nagayama, M.; Sumiyoshi, T.; et al. Pre-operative atrial fibrillation as the key determinant of outcome of mitral valve repair for degenerative mitral regurgitation. Eur. Heart J. 2005, 26, 1866–1872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kammerlander, A.A.; Marzluf, B.A.; Graf, A.; Bachmann, A.; Kocher, A.; Bonderman, D.; Mascherbauer, J. Right ventricular dysfunction, but not tricuspid regurgitation, is associated with outcome late after left heart valve procedure. J. Am. Coll. Cardiol. 2014, 64, 2633–2642. [Google Scholar] [CrossRef] [PubMed]
- Boerlage-vanDijk, K.; Wiegerinck, E.M.; Araki, M.; Meregalli, P.G.; Bindraban, N.R.; Koch, K.T.; Vis, M.M.; Piek, J.J.; Tijssen, J.G.; Bouma, B.J.; et al. Predictors of outcome in patients undergoing MitraClip implantation: An aid to improve patient selection. Int. J. Cardiol. 2015, 189, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Triantafyllis, A.S.; Kortlandt, F.; Bakker, A.L.; Swaans, M.J.; Eefting, F.D.; van der Heyden, J.A.; Post, M.C.; Rensing, B.W. Long-term survival and preprocedural predictors of mortality in high surgical risk patients undergoing percutaneous mitral valve repair. Catheter. Cardiovasc. Interv. 2016, 87, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Patton, K.K.; Ellinor, P.T.; Heckbert, S.R.; Christenson, R.H.; DeFilippi, C.; Gottdiener, J.S.; Kronmal, R.A. N-terminal pro-B-type natriuretic peptide is a major predictor of the development of atrial fibrillation: The Cardiovascular Health Study. Circulation 2009, 120, 1768–1774. [Google Scholar] [CrossRef] [PubMed]
- Wohrle, J.; Karakas, M.; Trepte, U.; Seeger, J.; Gonska, B.; Koenig, W.; Rottbauer, W. Midregional-proAtrial Natriuretic Peptide and High Sensitive Troponin T Strongly Predict Adverse Outcome in Patients Undergoing Percutaneous Repair of Mitral Valve Regurgitation. PLoS ONE 2015, 10, e0137464. [Google Scholar] [CrossRef] [PubMed]
- Yasue, H.; Yoshimura, M.; Sumida, H.; Kikuta, K.; Kugiyama, K.; Jougasaki, M.; Ogawa, H.; Okumura, K.; Mukoyama, M.; Nakao, K. Localization and mechanism of secretion of B-type natriuretic peptide in comparison with those of A-type natriuretic peptide in normal subjects and patients with heart failure. Circulation 1994, 90, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Naruse, M.; Takeyama, Y.; Tanabe, A.; Hiroshige, J.; Naruse, K.; Yoshimoto, T.; Tanaka, M.; Katagiri, T.; Demura, H. Atrial and brain natriuretic peptides in cardiovascular diseases. Hypertension 1994, 23, I231–I234. [Google Scholar] [CrossRef] [PubMed]
- Murashita, T.; Okada, Y.; Kanemitsu, H.; Fukunaga, N.; Konishi, Y.; Nakamura, K.; Koyama, T. Long-term outcomes after mitral valve repair for degenerative mitral regurgitation with persistent atrial fibrillation. Thoracic. Cardiov. Surg. 2015, 63, 243–249. [Google Scholar] [CrossRef]
- Coutinho, G.F.; Garcia, A.L.; Correia, P.M.; Branco, C.; Antunes, M.J. Negative impact of atrial fibrillation and pulmonary hypertension after mitral valve surgery in asymptomatic patients with severe mitral regurgitation: A 20-year follow-up. Eur. J. Cardio-Thorac. Surg. 2015, 48, 548–555; discussion 555–556. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.; Barlow, C.W.; Hosseinpour, A.R.; Wisbey, C.; Wilson, K.; Pidgeon, W.; Charman, S.; Barlow, J.B.; Wells, F.C. Influence of atrial fibrillation on outcome following mitral valve repair. Circulation 2001, 104, I59–I63. [Google Scholar] [CrossRef] [PubMed]
- Chua, Y.L.; Schaff, H.V.; Orszulak, T.A.; Morris, J.J. Outcome of mitral valve repair in patients with preoperative atrial fibrillation. Should the maze procedure be combined with mitral valvuloplasty? J. Thorac. Cardiovasc. Surg. 1994, 107, 408–415. [Google Scholar] [PubMed]
- Ohno, Y.; Attizzani, G.F.; Capodanno, D.; Cannata, S.; Dipasqua, F.; Imme, S.; Barbanti, M.; Ministeri, M.; Caggegi, A.; Pistritto, A.M.; et al. Association of tricuspid regurgitation with clinical and echocardiographic outcomes after percutaneous mitral valve repair with the MitraClip System: 30-day and 12-month follow-up from the GRASP Registry. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 1246–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jabs, A.; von Bardeleben, R.S.; Boekstegers, P.; Puls, M.; Lubos, E.; Bekeredjian, R.; Ouarrak, T.; Plicht, B.; Eggebrecht, H.; Nickenig, G.; et al. Effects of atrial fibrillation and heart rate on percutaneous mitral valve repair with MitraClip: Results from the TRAnscatheter Mitral valve Interventions (TRAMI) registry. EuroIntervention 2017, 12, 1697–1705. [Google Scholar] [CrossRef] [PubMed]
- Velu, J.F.; Kortlandt, F.A.; Hendriks, T.; Schurer, R.A.J.; van Boven, A.J.; Koch, K.T.; Vis, M.M.; Henriques, J.P.; Piek, J.J.; Van den Branden, B.J.L.; et al. Comparison of Outcome After Percutaneous Mitral Valve Repair With the MitraClip in Patients With Versus Without Atrial Fibrillation. Am. J. Cardiol. 2017. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Afib | No Afib | p-Value | |
|---|---|---|---|
| Number of patients | 239 | 116 | |
| Age (years) | 77.6 ± 7.6 | 75.5 ± 9.8 | 0.024 |
| Female gender | 90 (37.7%) | 49 (42.2%) | 0.41 |
| BMI (kg/m2) | 25.9 ± 4.3 | 25.4 ± 4.5 | 0.29 |
| Diabetes mellitus | 66 (27.6%) | 38 (32.8%) | 0.54 |
| Creatinine (µmol/L) | 131.9 ± 61.8 | 128.1 ± 79.8 | 0.63 |
| Glomerular filtration rate (mL/min) | 42.2 ± 15.8 | 46.3 ± 18.7 | 0.06 |
| Hemoglobin (g/dL) | 12.3 ± 1.8 | 12.2 ± 1.9 | 0.67 |
| Troponin T (ng/L) | 42.9 ± 43.9 | 76.9 ± 254.5 | 0.09 |
| NT-pro-BNP (pg/mL) | 6517.5 ± 7308.0 | 4153.8 ± 4682.5 | 0.010 |
| Coronary artery disease | 169 (71.1%) | 89 (77.4%) | 0.29 |
| History of MI | 52 (21.8%) | 29 (25.0%) | 0.33 |
| History of cardiac bypass graft | 37 (15.5%) | 25 (21.6%) | 0.16 |
| Peripheral or cerebral vascular disease | 63 (26.5%) | 37 (32.5%) | 0.25 |
| History of stroke or intracerebral bleeding | 25 (10.5%) | 11 (9.7%) | 0.80 |
| Chronic obstructive pulmonary disease | 34 (14.2%) | 14 (12.1%) | 0.57 |
| ICD (pre-existing) | 40 (16.7%) | 24 (20.7%) | 0.37 |
| CRT (pre-existing) | 19 (8.0%) | 15 (12.9%) | 0.14 |
| NYHA class | 3.2 ± 0.7 | 3.0 ± 0.8 | 0.16 |
| EuroScore II | 8.6 ± 7.7 | 8.9 ± 8.6 | 0.79 |
| STS for mortality | 4.2 ± 4.9 | 3.8 ± 4.1 | 0.37 |
| Afib | No Afib | p-Value | |
|---|---|---|---|
| Number of patients | 239 | 116 | |
| Transthoracic echocardiography | |||
| Degenerative etiology of MR | 82 (35.0%) | 39 (34.2%) | 0.50 |
| MR grade (0–4) | 3.5 ± 0.6 | 3.5 ± 0.5 | 0.36 |
| LVEDD (mm) | 60.5 ± 11.3 | 63.4 ± 11.5 | 0.06 |
| LVESD (mm) | 45.5 ± 14.0 | 49.2 ± 13.7 | 0.07 |
| LA diameter (mm) | 56.9 ± 10.1 | 51.6 ± 7.0 | 0.00002 |
| Transvalvular mitral gradient (mmHg) | 2.1 ± 2.1 | 1.8 ± 1.3 | 0.22 |
| Left ventricular ejection fraction (%) | 44.2 ± 18.0 | 42.3 ± 17.0 | 0.43 |
| Tricuspid regurgitation grade III/IV | 118 (56.2%) | 31 (33.0%) | 0.0002 |
| Cardiac catheterization | |||
| Cardiac output (L/min), Fick method | 3.8 ± 1.2 | 3.7 ± 1.1 | 0.44 |
| Cardiac index (L/min/m2) | 2.0 ± 0.6 | 2.1 ± 0.5 | 0.77 |
| Systolic pulmonary artery pressure (mmHg) | 51.6 ± 15.9 | 47.8 ± 16.0 | 0.11 |
| Mean pulmonary artery pressure (mmHg) | 33.2 ± 10.6 | 31.3 ± 11.3 | 0.25 |
| Pulmonary capillary wedge pressure (mmHg) | 23.0 ± 9.1 | 20.2 ± 9.2 | 0.05 |
| Pulmonary vascular resistance (dynxsxcm−5) | 311 ± 270 | 285 ± 233 | 0.55 |
| Afib | No Afib | p-Value | |
|---|---|---|---|
| Number of patients | 239 | 116 | |
| Implantation details | |||
| Procedural success | 236 (98.7%) | 112 (96.6%) | 0.18 |
| Number of clips | 1.3 ± 0.5 | 1.3 ± 0.5 | 0.86 |
| Clip detachment | 5 (2.1%) | 3 (2.5%) | 0.78 |
| Echocardiography post-procedural | |||
| MR grade (0–4) | 1.6 ± 0.6 | 1.6 ± 0.7 | 0.50 |
| Transvalvular mitral gradient (mmHg) | 4.0 ± 2.7 | 4.2 ± 2.2 | 0.70 |
| In-hospital outcome | |||
| ICU stay after procedure | 1.3 ± 3.7 | 1.0 ± 1.6 | 0.80 |
| Hospital stay after procedure | 7.7 ± 5.7 | 7.2 ± 4.9 | 0.80 |
| In-hospital death | 7 (2.9%) | 4 (3.5%) | 0.79 |
| Post-procedural myocardial infarction | 0 | 0 | n.a. |
| Cardiogenic shock | 5 (2.1%) | 1 (0.9%) | 0.37 |
| Need for CPR | 4 (1.7%) | 3 (2.6%) | 0.57 |
| Need for Inotropes | 32 (13.5%) | 13 (11.2%) | 0.55 |
| Stroke | 4 (1.7%) | 2 (1.7%) | 0.97 |
| Post-procedural bleeding MVARC ≥ 2 | 6 (2.5%) | 2 (1.7%) | 0.63 |
| Infection (any) | 9 (3.8%) | 7 (6.0%) | 0.34 |
| Baseline | 3 Months | 12 Months | 3 Years | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Afib | No Afib | p-Value | Afib | No Afib | p-Value | Afib | No Afib | p-Value | Afib | No Afib | p-Value | |
| Beta-blocker | 92.8 | 91.2 | 0.60 | 92.6 | 87.5 | 0.23 | 90.0 | 89.6 | 0.93 | 79.3 | 93.3 | 0.20 |
| ACE-I or ARB | 78.9 | 85.7 | 0.12 | 75.0 | 80.3 | 0.39 | 70.5 | 79.2 | 0.11 | 62.1 | 86.7 | 0.08 |
| MRA | 41.0 | 46.4 | 0.34 | 46.3 | 50.7 | 0.55 | 39.2 | 40.3 | 0.88 | 44.8 | 46.7 | 0.91 |
| ARNI | 3.2 | 0 | 0.14 | 4.3 | 5.0 | >0.89 | 5.4 | 4.3 | 0.77 | n.a. | n.a. | |
| 12 Months | 24 Months | 36 Months | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Afib | No Afib | Afib | No Afib | Afib | No Afib | ||
| Mortality | (47) 21.1% | (13) 11.8% | (62) 34.0% | (19) 22.3% | (74) 50.3% | (22) 32.2% | 0.032 |
| Cardiovascular mortality | (29) 14.1% | (8) 7.5% | (37) 21.5% | (11) 13.0% | (45) 35.1% | (14) 24.2% | 0.10 |
| MACCE | (94) 41.5% | (31) 28.5% | (112) 57.6% | (36) 36.3% | (120) 66.7% | (39) 46.7% | 0.003 |
| Rehospitalization due to heart failure | (44) 21.9% | (21) 20.5% | (54) 31.0% | (24) 25.0% | (56) 34.6% | (25) 28.4% | 0.50 |
| Beta | Hazard Ratio | 95% Confidence Interval | p-Value | |
|---|---|---|---|---|
| Atrial fibrillation | 0.872 | 2.39 | 1.06–5.41 | 0.036 |
| NT-pro-BNP | 0 | 1.0 | 1.0–1.0 | 0.072 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keßler, M.; Pott, A.; Mammadova, E.; Seeger, J.; Wöhrle, J.; Rottbauer, W.; Markovic, S. Atrial Fibrillation Predicts Long-Term Outcome after Transcatheter Edge-to-Edge Mitral Valve Repair by MitraClip Implantation. Biomolecules 2018, 8, 152. https://doi.org/10.3390/biom8040152
Keßler M, Pott A, Mammadova E, Seeger J, Wöhrle J, Rottbauer W, Markovic S. Atrial Fibrillation Predicts Long-Term Outcome after Transcatheter Edge-to-Edge Mitral Valve Repair by MitraClip Implantation. Biomolecules. 2018; 8(4):152. https://doi.org/10.3390/biom8040152
Chicago/Turabian StyleKeßler, Mirjam, Alexander Pott, Elnura Mammadova, Julia Seeger, Jochen Wöhrle, Wolfgang Rottbauer, and Sinisa Markovic. 2018. "Atrial Fibrillation Predicts Long-Term Outcome after Transcatheter Edge-to-Edge Mitral Valve Repair by MitraClip Implantation" Biomolecules 8, no. 4: 152. https://doi.org/10.3390/biom8040152