Add-on Immunoadsorption Shortly-after Optimal Medical Treatment Further Significantly and Persistently Improves Cardiac Function and Symptoms in Recent-Onset Heart Failure—A Single Center Experience


Abstract
:1. Introduction
2. Methods
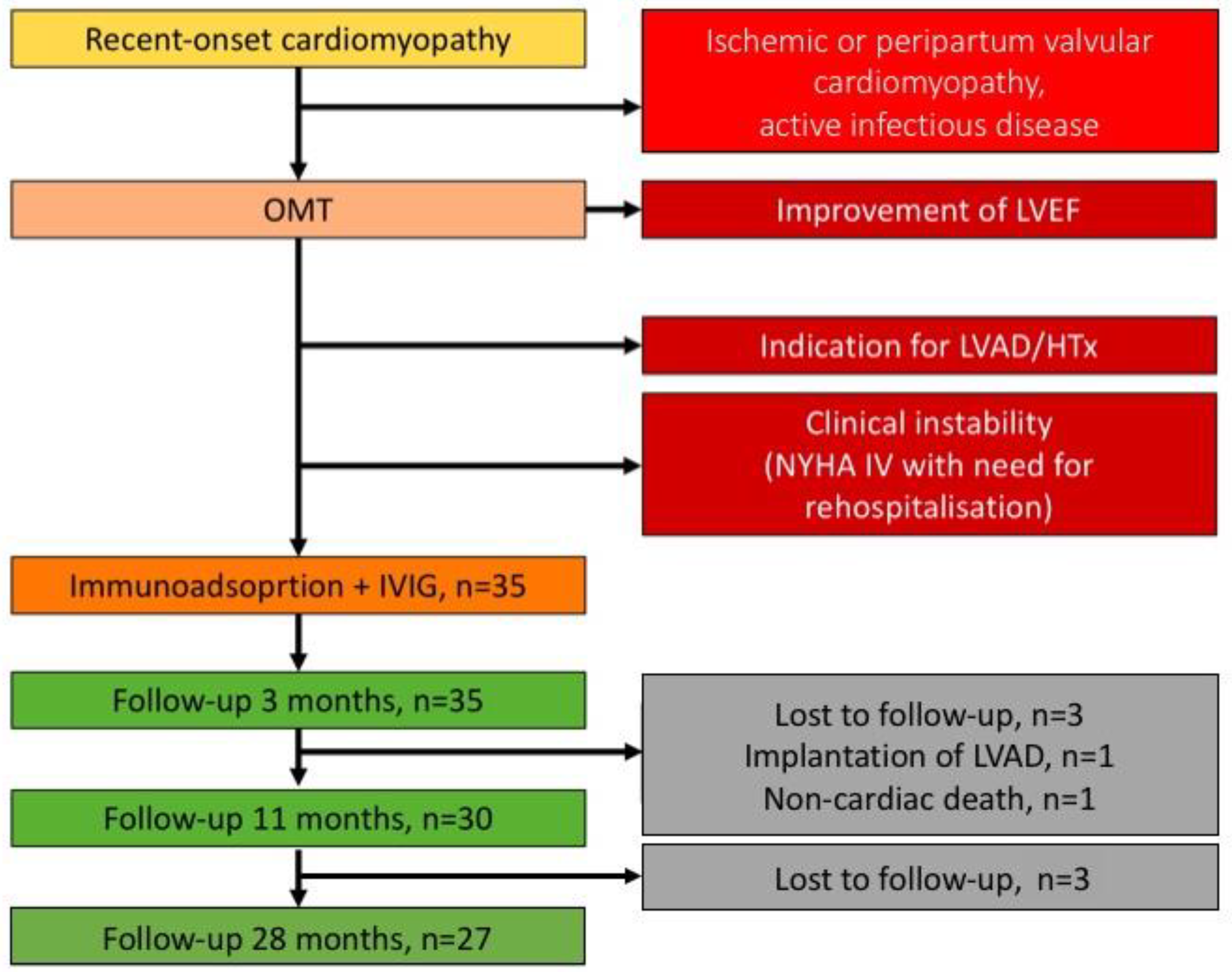
2.1. Study Population
2.2. Pharmacological Treatment of HF
2.3. Diagnostic Approaches at Initial Diagnosis and during Follow-Up Visits
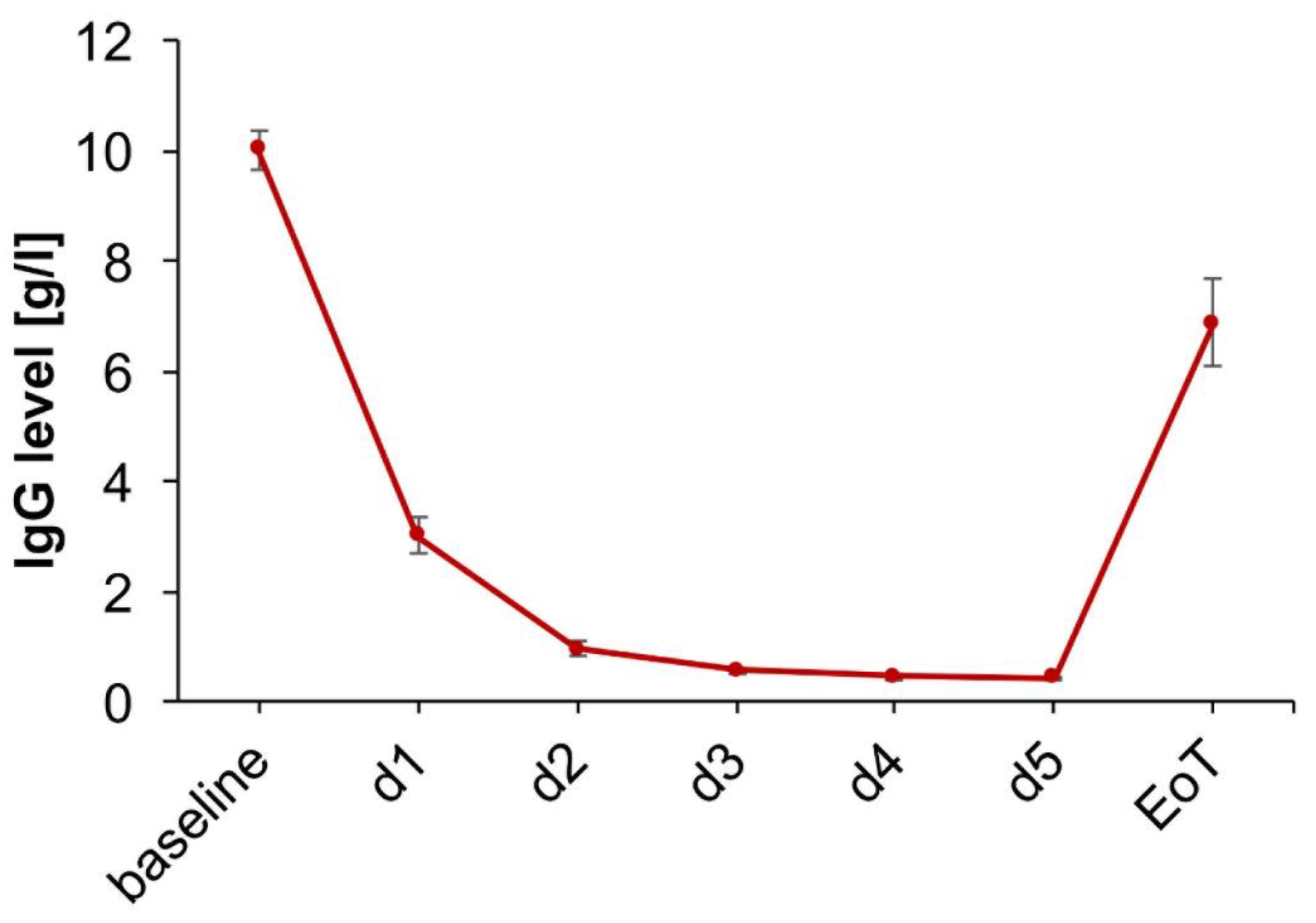
2.4. Extracorporal Immunoglobulin Adsorption and Subsequent IVIG Administration
2.5. Quality of Life (QoL) Assessment Using the Minnesota Living with HF Questionnaire (MLHFQ)
2.6. Evaluation of Responsiveness to Treatment
2.7. Statistical Analysis
2.8. Ethics
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Optimal Medical HF Treatment Improved NYHA Functional Class without Affecting LVEF
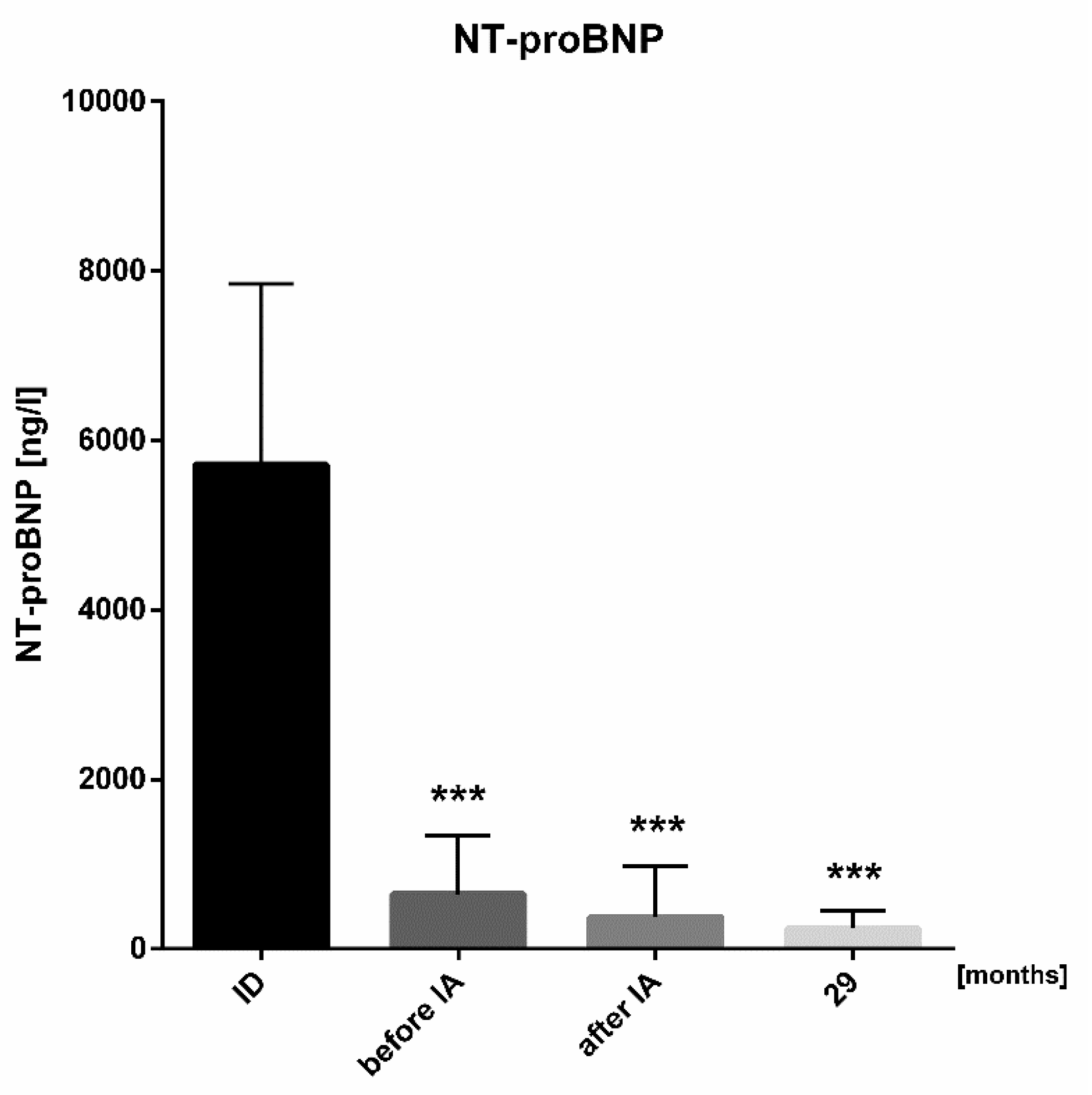
3.3. Add-On Immunoadsorption with Subsequent IVIG Administration Improved NYHA Functional Class, LVEF and NT-proBNP during Short-Term and Long-Term Follow-Up
3.4. High Response Rate to Immunoadsorption Treatment Regarding Cardiac Function and Clinical Parameters
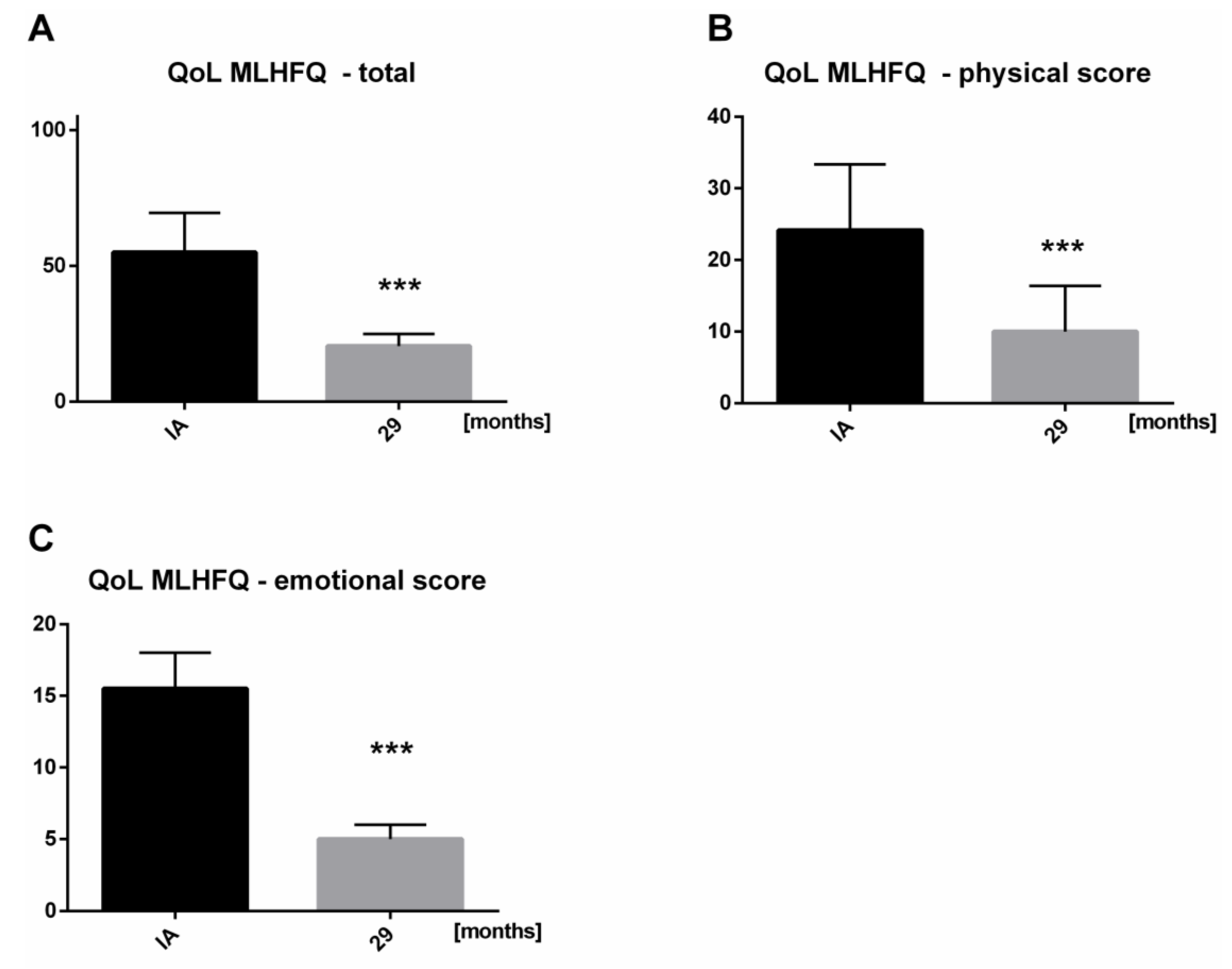
3.5. Significant Improvement in QoL during Long-Term Follow-Up
4. Discussion
4.1. Benefits of Immunoadsorption and Subsequent IVIG in Patients with Limited HF Therapy
4.2. Immunoadsorption and Subsequent IVIG Administration in Recent-Onset Cardiomyopathy vs. End-Stage Heart Failure
4.3. Predictors for Responsiveness to Immunoadsorption
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ameling, S.; Bhardwaj, G.; Hammer, E.; Beug, D.; Steil, L.; Reinke, Y.; Weitmann, K.; Grube, M.; Trimpert, C.; Klingel, K.; et al. Changes of myocardial gene expression and protein composition in patients with dilated cardiomyopathy after immunoadsorption with subsequent immunoglobulin substitution. Basic Res. Cardiol. 2016, 111, 53. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.; Mahon, N.J.; McKenna, W.J. Cardiac autoantibodies to myosin and other heart-specific autoantigens in myocarditis and dilated cardiomyopathy. Autoimmunity 2001, 34, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Kaya, Z.; Katus, H.A.; Rose, N.R. Cardiac troponins and autoimmunity: Their role in the pathogenesis of myocarditis and of heart failure. Clin. Immunol. 2010, 134, 80–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujinami, R.S.; von Herrath, M.G.; Christen, U.; Whitton, J.L. Molecular mimicry, bystander activation, or viral persistence: Infections and autoimmune disease. Clin. Microbiol. Rev. 2006, 19, 80–94. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, M.W. T cell mimicry in inflammatory heart disease. Mol. Immunol. 2004, 40, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.W.; O’Connell, J.B.; Herskowitz, A.; Rose, N.R.; McManus, B.M.; Billingham, M.E.; Moon, T.E. A clinical trial of immunosuppressive therapy for myocarditis. The Myocarditis Treatment Trial Investigators. N. Engl. J. Med. 1995, 333, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Costanzo-Nordin, M.R.; Reap, E.A.; O’Connell, J.B.; Robinson, J.A.; Scanlon, P.J. A nonsteroid anti-inflammatory drug exacerbates Coxsackie B3 murine myocarditis. J. Am. Coll. Cardiol. 1985, 6, 1078–1082. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef] [PubMed]
- Renders, L.; Wen, M.; Küchle, C.J.D.N. Plasmapherese und Immunadsorption. Nephrologe 2014, 9, 284–292. [Google Scholar] [CrossRef]
- Rector, T.S.; Cohn, J.N. Assessment of patient outcome with the Minnesota Living with Heart Failure questionnaire: Reliability and validity during a randomized, double-blind, placebo-controlled trial of pimobendan. Pimobendan Multicenter Research Group. Am. Heart J. 1992, 124, 1017–1025. [Google Scholar] [CrossRef]
- Rector, T.S.; Kubo, S.H.; Cohn, J.N. Validity of the Minnesota Living with Heart Failure questionnaire as a measure of therapeutic response to enalapril or placebo. Am. J. Cardiol. 1993, 71, 1106–1107. [Google Scholar] [CrossRef]
- Ohlow, M.A.; Brunelli, M.; Schreiber, M.; Lauer, B. Therapeutic effect of immunoadsorption and subsequent immunoglobulin substitution in patients with dilated cardiomyopathy: Results from the observational prospective Bad Berka Registry. J. Cardiol. 2017, 69, 409–416. [Google Scholar] [CrossRef] [PubMed]
- The treatment of heart failure. Task Force of the Working Group on Heart Failure of the European Society of Cardiology. Eur. Heart J. 1997, 18, 736–753. [CrossRef]
- Felix, S.B.; Staudt, A.; Dorffel, W.V.; Stangl, V.; Merkel, K.; Pohl, M.; Docke, W.D.; Morgera, S.; Neumayer, H.H.; Wernecke, K.D.; et al. Hemodynamic effects of immunoadsorption and subsequent immunoglobulin substitution in dilated cardiomyopathy: Three-month results from a randomized study. J. Am. Coll. Cardiol. 2000, 35, 1590–1598. [Google Scholar] [CrossRef]
- Lauer, B.; Schannwell, M.; Kuhl, U.; Strauer, B.E.; Schultheiss, H.P. Antimyosin autoantibodies are associated with deterioration of systolic and diastolic left ventricular function in patients with chronic myocarditis. J. Am. Coll. Cardiol. 2000, 35, 11–18. [Google Scholar] [CrossRef]
- Muller, J.; Wallukat, G.; Dandel, M.; Bieda, H.; Brandes, K.; Spiegelsberger, S.; Nissen, E.; Kunze, R.; Hetzer, R. Immunoglobulin adsorption in patients with idiopathic dilated cardiomyopathy. Circulation 2000, 101, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Jessup, M.; Marwick, T.H.; Ponikowski, P.; Voors, A.A.; Yancy, C.W. 2016 ESC and ACC/AHA/HFSA heart failure guideline update—What is new and why is it important? Nat. Rev. Cardiol. 2016, 13, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Staudt, A.; Hummel, A.; Ruppert, J.; Dorr, M.; Trimpert, C.; Birkenmeier, K.; Krieg, T.; Staudt, Y.; Felix, S.B. Immunoadsorption in dilated cardiomyopathy: 6-month results from a randomized study. Am. Heart J. 2006, 152, 712.e1–712.e6. [Google Scholar] [CrossRef] [PubMed]
- Staudt, A.; Bohm, M.; Knebel, F.; Grosse, Y.; Bischoff, C.; Hummel, A.; Dahm, J.B.; Borges, A.; Jochmann, N.; Wernecke, K.D.; et al. Potential role of autoantibodies belonging to the immunoglobulin G-3 subclass in cardiac dysfunction among patients with dilated cardiomyopathy. Circulation 2002, 106, 2448–2453. [Google Scholar] [CrossRef] [PubMed]
- Staudt, A.; Herda, L.R.; Trimpert, C.; Lubenow, L.; Landsberger, M.; Dorr, M.; Hummel, A.; Eckerle, L.G.; Beug, D.; Muller, C.; et al. Fcgamma-receptor IIa polymorphism and the role of immunoadsorption in cardiac dysfunction in patients with dilated cardiomyopathy. Clin. Pharmacol. Ther. 2010, 87, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Hall, S.A.; Cigarroa, C.G.; Marcoux, L.; Risser, R.C.; Grayburn, P.A.; Eichhorn, E.J. Time course of improvement in left ventricular function, mass and geometry in patients with congestive heart failure treated with beta-adrenergic blockade. J. Am. Coll. Cardiol. 1995, 25, 1154–1161. [Google Scholar] [CrossRef]
- Tsutamoto, T.; Wada, A.; Maeda, K.; Mabuchi, N.; Hayashi, M.; Tsutsui, T.; Ohnishi, M.; Sawaki, M.; Fujii, M.; Matsumoto, T.; et al. Effect of spironolactone on plasma brain natriuretic peptide and left ventricular remodeling in patients with congestive heart failure. J. Am. Coll. Cardiol. 2001, 37, 1228–1233. [Google Scholar] [CrossRef]
- Eriksson, S.; Hellman, J.; Pettersson, K. Autoantibodies against cardiac troponins. N. Engl. J. Med. 2005, 352, 98–100. [Google Scholar] [CrossRef] [PubMed]
- Ameling, S.; Herda, L.R.; Hammer, E.; Steil, L.; Teumer, A.; Trimpert, C.; Dorr, M.; Kroemer, H.K.; Klingel, K.; Kandolf, R.; et al. Myocardial gene expression profiles and cardiodepressant autoantibodies predict response of patients with dilated cardiomyopathy to immunoadsorption therapy. Eur. Heart J. 2013, 34, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Dandel, M.; Wallukat, G.; Englert, A.; Lehmkuhl, H.B.; Knosalla, C.; Hetzer, R. Long-term benefits of immunoadsorption in beta(1)-adrenoceptor autoantibody-positive transplant candidates with dilated cardiomyopathy. Eur. J. Heart Fail. 2012, 14, 1374–1388. [Google Scholar] [CrossRef] [PubMed]
- Trimpert, C.; Herda, L.R.; Eckerle, L.G.; Pohle, S.; Muller, C.; Landsberger, M.; Felix, S.B.; Staudt, A. Immunoadsorption in dilated cardiomyopathy: Long-term reduction of cardiodepressant antibodies. Eur. J. Clin. Investig. 2010, 40, 685–691. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients, n | 35 |
| Age, y | 47.1 (35.1–53.8) |
| Sex, n | |
| Male | 24 |
| Female | 11 |
| Medical history | |
| History of preceding infectious disease | 26 (74.3%) |
| Duration between infectious disease and HF, months | 1.4 (0.6–2.9) |
| Lab values | |
| Troponin T, ng/L | 22 (13–34) |
| NT-proBNP, ng/L | 5720 (1850–7294) |
| White blood cell count, 109/L | 8.4 (6.9–9.9) |
| C-reactive protein, mg/L | 4.8 (3.0–14.8) |
| Coronary artery disease (CAD) | |
| no CAD | 23 (65.7%) |
| 1-vessel CAD | 8 (22.9%) |
| 2-vessel CAD | 4 (11.4%) |
| 3-vessel CAD | 0 |
| Endomyocardial biopsy, n | 27 |
| Virus positive | 13 (48.1%) |
| Cardiac magnetic resonance imaging (MRI), n | 18 |
| Diagnostic criteria for myocardial inflammation | 13 (72.2%) |
| Initial Diagnosis | Immunoadsorption | p-Value | |
|---|---|---|---|
| Patients, n | 35 | 35 | |
| NYHA classification | 3.0 (2.5–3.3) | 2.0 (1.3–2.8) | <0.001 |
| NYHA classification, n (%) | |||
| I | 0 (0.0) | 9 (25.7) | |
| II | 5 (14.3) | 13 (37.1) | |
| III | 21 (60.0) | 12 (34.3) | |
| IV | 9 (25.7) | 1 (2.9) | |
| LVEF, % | 27.0 (24.3–30.0) | 27.0 (23.0–31.0) | 0.80 |
| LVDd, mm | 67.0 (63.0–70.0) | 65.5 (61.0–68.5) | 0.31 |
| LVDs, mm | 57.0 (49.0–60.0) | 51.0 (51.0–51.0) | 0.50 |
| Patients, n | 35 |
| Heart rate (HR), bpm | 70 (62.0–74.5) |
| ARB, n | 9 |
| % of dose equivalent | 25.0 (25.0–50.0) |
| ACE-inhibitor, n | 26 |
| % of dose equivalent | 50.0 (44.4–100.0) |
| Beta-adrenergic blocking agent, n | 35 |
| % of dose equivalent | 50.0 (25.0–75.0) |
| Aldosterone-antagonist, n | 34 |
| % of dose equivalent | 50.0 (50.0–50.0) |
| Loop diuretics, n | 29 |
| Digitalis, n | 2 |
| Cardiac resynchronization therapy, n | 2 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weinmann, K.; Werner, J.; Koenig, W.; Rottbauer, W.; Walcher, D.; Keßler, M. Add-on Immunoadsorption Shortly-after Optimal Medical Treatment Further Significantly and Persistently Improves Cardiac Function and Symptoms in Recent-Onset Heart Failure—A Single Center Experience. Biomolecules 2018, 8, 133. https://doi.org/10.3390/biom8040133
Weinmann K, Werner J, Koenig W, Rottbauer W, Walcher D, Keßler M. Add-on Immunoadsorption Shortly-after Optimal Medical Treatment Further Significantly and Persistently Improves Cardiac Function and Symptoms in Recent-Onset Heart Failure—A Single Center Experience. Biomolecules. 2018; 8(4):133. https://doi.org/10.3390/biom8040133
Chicago/Turabian StyleWeinmann, Karolina, Jakob Werner, Wolfgang Koenig, Wolfgang Rottbauer, Daniel Walcher, and Mirjam Keßler. 2018. "Add-on Immunoadsorption Shortly-after Optimal Medical Treatment Further Significantly and Persistently Improves Cardiac Function and Symptoms in Recent-Onset Heart Failure—A Single Center Experience" Biomolecules 8, no. 4: 133. https://doi.org/10.3390/biom8040133