Adverse Outcome Prediction of Iron Deficiency in Patients with Acute Coronary Syndrome

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Laboratory Methods
2.4. Statistical Methods
3. Results
4. Discussion
4.1. Pathophysiological Implications and Clinical Impact
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Anderson, G.J.; Vulpe, C.D. Mammalian iron transport. Cell. Mol. Life Sci. 2009, 66, 3241–3261. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.C. Disorders of iron metabolism. N. Engl. J. Med. 1999, 341, 1986–1995. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, E.A.; von Haehling, S.; Anker, S.D.; Macdougall, I.C.; Ponikowski, P. Iron deficiency and heart failure: Diagnostic dilemmas and therapeutic perspectives. Eur. Heart J. 2013, 34, 816–829. [Google Scholar] [CrossRef] [PubMed]
- Zeller, T.; Altay, A.; Waldeyer, C.; Appelbaum, S.; Ojeda, F.; Ruhe, J.; Schnabel, R.B.; Lackner, K.J.; Blankenberg, S.; Karakas, M. Prognostic Value of Iron-Homeostasis Regulating Peptide Hepcidin in Coronary Heart Disease—Evidence from the Large AtheroGene Study. Biomolecules 2018, 8, 43. [Google Scholar] [CrossRef] [PubMed]
- Traghella, I.; Mastorci, F.; Alessia, P.; Pingitore, A.; Vassalle, C. Nontraditional Cardiovascular Biomarkers and Risk Factors: Rationale and Future Perspectives. Biomolecules 2018, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Wish, J.B. Assessing iron status: Beyond serum ferritin and transferrin saturation. Clin. J. Am. Soc. Nephrol. 2006, 1, S4–S8. [Google Scholar] [CrossRef] [PubMed]
- Goodnough, L.T.; Nemeth, E.; Ganz, T. Detection, evaluation, and management of iron-restricted erythropoiesis. Blood 2010, 116, 4754–4761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasricha, S.R.; Flecknoe-Brown, S.C.; Allen, K.J.; Gibson, P.R.; McMahon, L.P.; Olynyk, J.K.; Roger, S.D.; Savoia, H.F.; Tampi, R.; Thomson, A.R.; et al. Diagnosis and management of iron deficiency anaemia: A clinical update. Med. J. Aust. 2010, 193, 525–532. [Google Scholar] [PubMed]
- Schaefer, S.; Zeller, T.; Waldeyer, C.; Ojeda, F.; Schnabel, R.; Atay, A.; Lackner, K.; Anker, S.; Westermann, D.; Blankenberg, S.; et al. 5759 Iron deficiency independently and strongly predicts adverse outcome in patients with acute coronary syndrome—First report on the prospective relevance of iron deficiency. Eur. Heart J. 2017, 38. [Google Scholar] [CrossRef]
- Anker, S.D.; Comin Colet, J.; Filippatos, G.; Willenheimer, R.; Dickstein, K.; Drexler, H.; Lüscher, T.F.; Bart, B.; Banasiak, W.; Niegowska, J.; et al. Ferric carboxymaltose in patients with heart failure and iron deficiency. N. Engl. J. Med. 2009, 361, 2436–2448. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; van Veldhuisen, D.J.; Comin-Colet, J.; Ertl, G.; Komajda, M.; Mareev, V.; McDonagh, T.; Parkhomenko, A.; Tavazzi, L.; Mori, V.L.C.; et al. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency. Eur. Heart J. 2015, 36, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, E.A.; Tkaczyszyn, M.; Suchocki, T.; Drozd, M.; von Haehling, S.; Doehner, W.; Banasiak, W.; Filippatos, G.; Anker, S.D.; Ponikowski, P.; et al. Effects of intravenous iron therapy in iron-deficient patients with systolic heart failure: A meta-analysis of randomized controlled trials. Eur. J. Heart Fail. 2016. [Google Scholar] [CrossRef] [PubMed]
- Blankenberg, S.; Rupprecht, H.J.; Bickel, C.; Torzewski, M.; Hafner, G.; Tiret, L.; Smieja, M.; Cambien, F.; Meyer, J.; Lackner, K.J.; et al. Glutathione peroxidase 1 activity and cardiovascular events in patients with coronary artery disease. N. Engl. J. Med. 2003, 349, 1605–1613. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, R.; Messow, C.M.; Lubos, E.; Espinola-Klein, C.; Rupprecht, H.J.; Bickel, C.; Sinning, C.; Tzikas, S.; Keller, T.; Blankenberg, S.; et al. Association of adiponectin with adverse outcome in coronary artery disease patients: Results from the AtheroGene study. Eur. Heart J. 2008, 29, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Calvin, J.E.; Klein, L.W.; Vandenberg, B.J.; Meyer, P.; Condon, J.V.; Snell, R.J.; Ramirez-Morgen, L.M.; Parrillo, J.E. Risk stratification in unstable angina: Prospective validation of the Braunwald classification. J. Am. Med. Assoc. 1995, 273, 136–141. [Google Scholar] [CrossRef]
- Jankowska, E.A.; Wojtas, K.; Kasztura, M.; Mazur, G.; Butrym, A.; Kalicinska, E.; Rybinska, I.; Skiba, J.; von Haehling, S.; Doehner, W.; et al. Bone marrow iron depletion is common in patients with coronary artery disease. Int. J. Cardiol. 2015, 182, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, E.A.; Rozentryt, P.; Witkowska, A.; Nowak, J.; Hartmann, O.; Ponikowska, B.; Borodulin-Nadzieja, L.; Banasiak, W.; Polonski, L.; Anker, S.D.; et al. Iron deficiency: An ominous sign in patients with systolic chronic heart failure. Eur. Heart J. 2010, 31, 1872–1880. [Google Scholar] [CrossRef] [PubMed]
- Von Haehling, S.; Jankowska, E.A.; van Veldhuisen, D.J.; Ponikowski, P.; Anker, S.D. Iron deficiency and cardiovascular disease. Nat. Rev. Cardiol. 2015, 12, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Grammer, T.B.; Kleber, M.E.; Silbernagel, G.; Pilz, S.; Scharnagl, H.; Tomaschitz, A.; König, W.; März, W. Hemoglobin, iron metabolism and angiographic coronary artery disease (The Ludwigshafen Risk and Cardiovascular Health Study). Atherosclerosis 2014, 236, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Dziegala, M.; Kasztura, M.; Kobak, K.; Bania, J.; Banasiak, W.; Ponikowski, P.; Jankowska, E.A. Influence of the availability of iron during hypoxia on the genes associated with apoptotic activity and local iron metabolism in rat H9C2 cardiomyocytes and L6G8C5 skeletal myocytes. Mol. Med. Rep. 2016, 14, 3969–3977. [Google Scholar] [CrossRef] [PubMed]
- Isoda, M.; Hanawa, H.; Watanabe, R.; Yoshida, T.; Toba, K.; Yoshida, K.; Kojima, M.; Otaki, K.; Hao, K.; Ding, L.; et al. Expression of the peptide hormone hepcidin increases in cardiomyocytes under myocarditis and myocardial infarction. J. Nutr. Biochem. 2010, 21, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Merle, U.; Fein, E.; Gehrke, S.G.; Stremmel, W.; Kulaksiz, H. The iron regulatory peptide hepcidin is expressed in the heart and regulated by hypoxia and inflammation. Endocrinology 2007, 148, 2663–2668. [Google Scholar] [CrossRef] [PubMed]
- Simonis, G.; Mueller, K.; Schwarz, P.; Wiedemann, S.; Adler, G.; Strasser, R.H.; Kulaksiz, H.; et al. The iron-regulatory peptide hepcidin is upregulated in the ischemic and in the remote myocardium after myocardial infarction. Peptides 2010, 31, 1786–1790. [Google Scholar] [CrossRef] [PubMed]
- Makrecka-Kuka, M.; Krumschnabel, G.; Gnaiger, E. High-Resolution Respirometry for Simultaneous Measurement of Oxygen and Hydrogen Peroxide Fluxes in Permeabilized Cells, Tissue Homogenate and Isolated Mitochondria. Biomolecules 2015, 5, 1319–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alayash, A.I. Hemoglobin-Based Blood Substitutes and the Treatment of Sickle Cell Disease: More Harm than Help? Biomolecules 2017, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Florian, A.; Ludwig, A.; Rösch, S.; Yildiz, H.; Klumpp, S.; Sechtem, U.; Yilmaz, A. Positive effect of intravenous iron-oxide administration on left ventricular remodelling in patients with acute ST-elevation myocardial infarction—A cardiovascular magnetic resonance (CMR) study. Int. J. Cardiol. 2014, 173, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Haddad, S.; Wang, Y.; Galy, B.; Korf-Klingebiel, M.; Hirsch, V.; Baru, A.M.; Rostami, F.; Reboll, M.R.; Heineke, J.; Groos, U.F.S.; et al. Iron-regulatory proteins secure iron availability in cardiomyocytes to prevent heart failure. Eur. Heart J. 2016. [Google Scholar] [CrossRef] [PubMed]
- Siglienti, I.; Bendszus, M.; Kleinschmitz, C.; Stoll, G. Cytokine profile of iron-laden macrophages: Implications for cellular magnetic resonance imaging. J. Neuroimmunol. 2006, 173, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; et al. Executive Summary: Heart Disease and Stroke Statistics-2016 Update: A report from the American Heart Association. Circulation 2016, 133, 447–454. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n | 836 |
|---|---|
| Age (years) * | 63 (54, 70) |
| Male sex (%) | 76.0 |
| BMI (kg/m²) * | 27.2 (24.9, 29.7) |
| Smoker (%) | 27.5 |
| Diabetes (%) | 20.0 |
| Hypertension (%) | 68.2 |
| Hyperlipidemia (%) | 63.4 |
| History of MI (%) | 37.0 |
| Total cholesterol (mg/dL) * | 202.0 (176.0, 233.3) |
| HDL-C (mg/dL) * | 46.0 (40.0, 56.0) |
| LDL-C (mg/dL) * | 128.0 (104.0, 155.0) |
| Troponin I (ng/mL) * | 0.1 (0, 2.0) |
| NT-proBNP (pg/mL) * | 429.0 (158.7, 1288.3) |
| CRP (mg/dL) *,# | 6.3 (2.5, 20.2) |
| Ferritin (µg/L) * | 236.2 (117.3, 387.2) |
| TSAT (%) * | 25.5 (13.5, 48.0) |
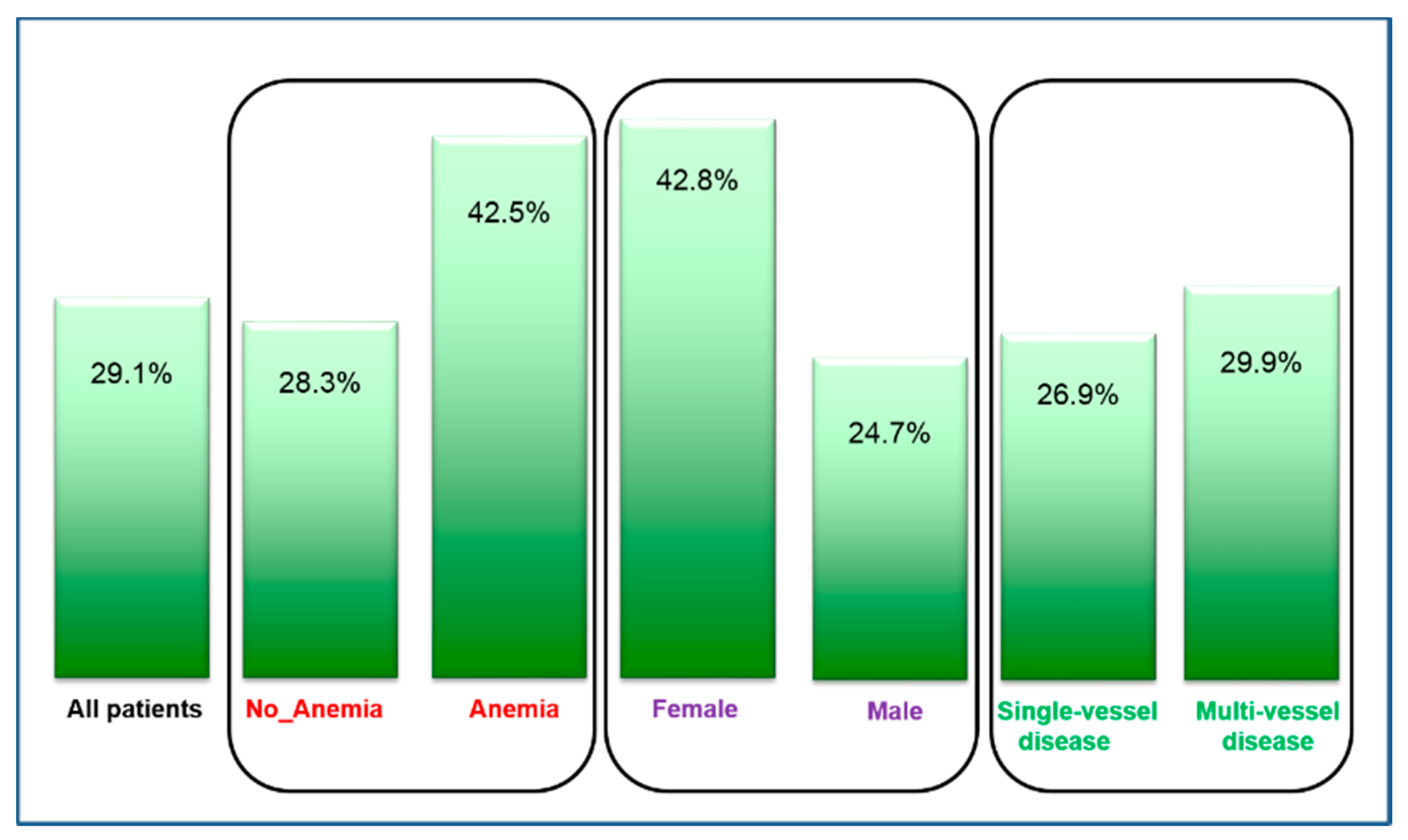
| Iron deficiency (%) | 29.1 |
| Hemoglobin (g/dL) * | 14.1 (13.1, 15.0) |
| Ferritin (p-Value) | TSAT (p-Value) | |
|---|---|---|
| Male gender | 0.26 (<0.001) | −0.13 (<0.001) |
| Age | −0.04 (0.20) | −0.04 (0.27) |
| Smoking status | −0.02 (0.59) | 0.06 (0.12) |
| Diabetes | 0.05 (0.12) | −0.05 (0.16) |
| Hypertension | −0.01 (0.71) | <0.01 (0.98) |
| History of MI | −0.05 (0.18) | 0.05 (0.16) |
| Hyperlipidemia | −0.09 (0.007) | 0.14 (<0.001) |
| BMI | 0.08 (0.030) | −0.05 (0.18) |
| Troponin I | 0.14 (<0.001) | −0.31 (<0.001) |
| NT-proBNP | 0.05 (0.22) | −0.24 (<0.001) |
| Hemoglobin | 0.09 (0.012) | 0.08 (0.038) |
| HR | 95% CI | p-Value | |
|---|---|---|---|
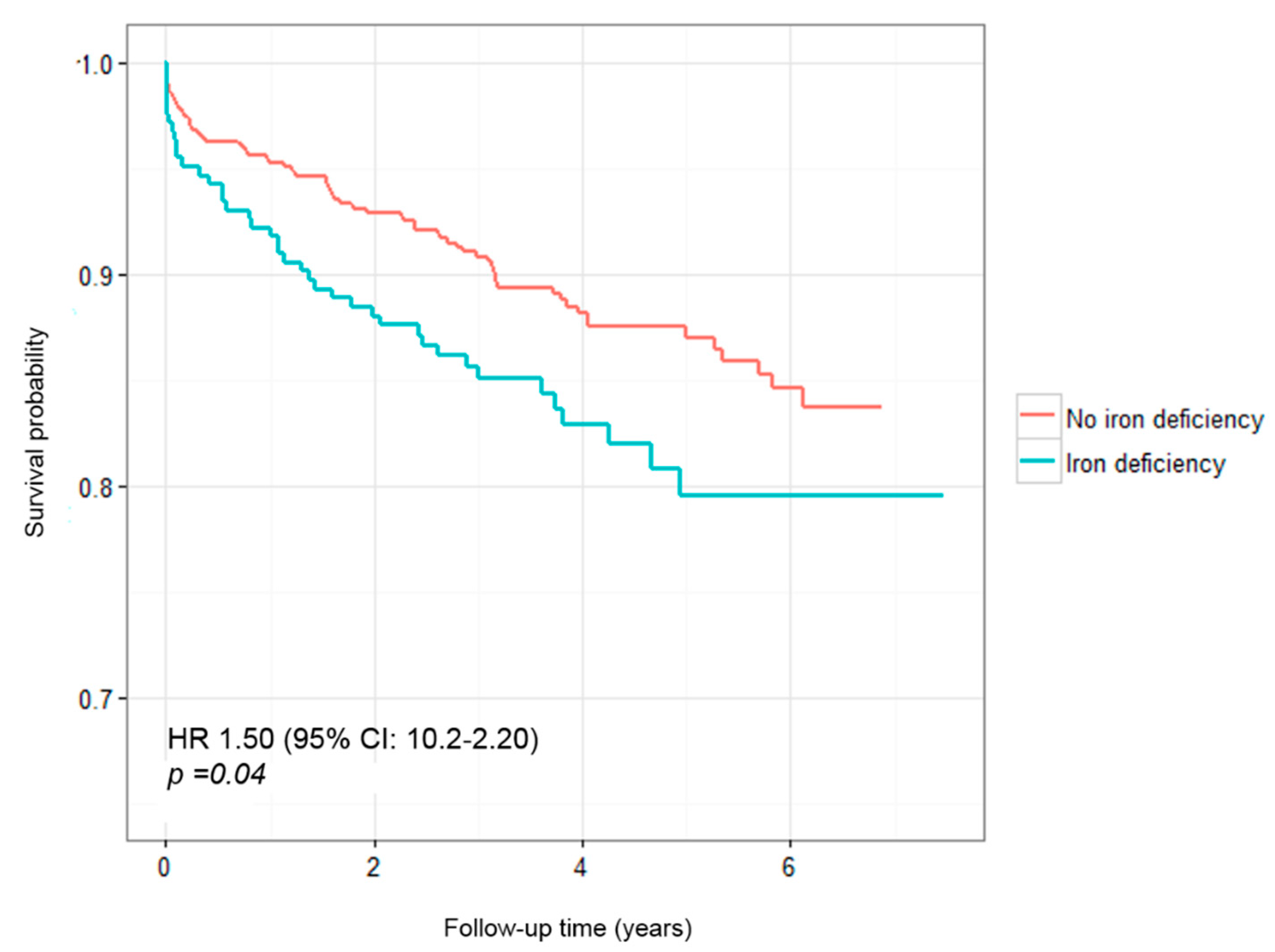
| Model 1 | 1.52 | 1.03–2.26 | 0.037 |
| Model 2 | 1.73 | 1.07–2.81 | 0.026 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeller, T.; Waldeyer, C.; Ojeda, F.; Schnabel, R.B.; Schäfer, S.; Altay, A.; Lackner, K.J.; Anker, S.D.; Westermann, D.; Blankenberg, S.; et al. Adverse Outcome Prediction of Iron Deficiency in Patients with Acute Coronary Syndrome. Biomolecules 2018, 8, 60. https://doi.org/10.3390/biom8030060
Zeller T, Waldeyer C, Ojeda F, Schnabel RB, Schäfer S, Altay A, Lackner KJ, Anker SD, Westermann D, Blankenberg S, et al. Adverse Outcome Prediction of Iron Deficiency in Patients with Acute Coronary Syndrome. Biomolecules. 2018; 8(3):60. https://doi.org/10.3390/biom8030060
Chicago/Turabian StyleZeller, Tanja, Christoph Waldeyer, Francisco Ojeda, Renate B. Schnabel, Sarina Schäfer, Alev Altay, Karl J. Lackner, Stefan D. Anker, Dirk Westermann, Stefan Blankenberg, and et al. 2018. "Adverse Outcome Prediction of Iron Deficiency in Patients with Acute Coronary Syndrome" Biomolecules 8, no. 3: 60. https://doi.org/10.3390/biom8030060