Topical Sunscreen Application Preventing Skin Cancer: Systematic Review

Department of Drug Science, University of Pavia, via Taramelli 12, 27100 Pavia, Italy
*
Author to whom correspondence should be addressed.
Cosmetics 2019, 6(3), 42; https://doi.org/10.3390/cosmetics6030042
Submission received: 1 June 2019
/
Revised: 6 July 2019
/
Accepted: 10 July 2019
/
Published: 11 July 2019
(This article belongs to the Special Issue Cosmetic Safety and Risk Assessment)
Abstract
:Background: Avoiding extended exposure to direct sunlight and the topical application of sunscreen when exposed are the main techniques used to protect the skin form sunburn, photoaging, and skin cancer risk (melanoma and non-melanoma skin cancer). Preventive strategies could lead to a significant reduction of the excessive health system cost for the treatment of these conditions. Sunscreen employment and efficacy stay controversial despite decades of humane use with health benefits closely related. At the present, few studies still found a connection between the use of sunscreen and not significant long-term benefits from UV induced damages. Objectives: To assess the effects of sunscreens for preventing melanoma, non-melanoma skin cancer (basal or squamous carcinoma and melanoma) and precancerous skin lesions. Method: Published literature (1993–2017) was reviewed and eligible studies that reported the impact of sunscreen use in the prevention of melanoma, non-melanoma skin cancer, or precancerous skin lesion were selected. Result: Starting from 532 sources, a total of seven articles met the inclusion criteria and they have been subjected to a systematic review. All of the included studies suggest that sunscreen use is associated with a reduction in melanoma, squamous cell carcinoma, and precancerous skin lesions; however, the difficulties in evaluating the efficiency of sunscreen were pointed out. Conclusion: The review of the experimental evidence supports the topical application of sunscreen as an effective effort in preventing skin cancer and precancerous skin lesions.
1. Introduction
Skin cancer represents the most common type of malignant neoplasms in Caucasian population, with over a million cases diagnosed each year [1]. Nearly 15,000 deaths and 76,380 new cases were estimated in the United States (US) in 2016 [2]. Intrinsic and extrinsic factors regulate the skin cancer development. ~10–30% of lifetime risk to cancer development is represented by DNA replication random errors followed a genetic mutation, but the extrinsic factor as prolonged and unprotected UV exposure is accepted as the biggest cause of melanoma (MM) and non-melanoma skin cancer (NMSC), such as basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) [3]. The origin of the melanoma cells is not fully agreed, and it has been suggested that the MM cells may have originated from either from dedifferentiated melanocytes or from melanocyte progenitors. BCC and SCC originates from malignant transformation of keratinocytes and the suppression of the cutaneous inflammatory response [4]. BCC and SCC show precursor lesions, such as Actinic Keratoses (AK), which are considerate premalignant lesions, with 1–20% of rate progression in invasive carcinoma and the risk is appreciably higher in subjects with five or more AK; it is a reliable marker in identifying those most predisposed to the development of NMSC [5].
Studies show that the timing, pattern and amount of UV exposure seems to be relevant in their development, MM is related to intermittent, infrequent UV exposure and episodes of severe sunburns, BCC to intermittent, infrequent, and intense UV exposure, and SCC is connected to frequent moderate exposure episodes, and, usually, presents keratinizing lesions, such as actinic keratoses (AKs) [6]. Even if the origin of MM and NMSC seems to be different, studies showed that MM and NMSC incidence is higher for: (i) specific phenotypic category: fair-skinned phenotype presents low levels of melanin (skin pigment able to absorb UV radiation), resulting in less protection against UV radiation, usually they are very sensitive to the solar radiation, tending to burn, (ii) history of sunburn (in particular during the childhood), (iii) personal behavior (e.g., indoor tanning, intentional sun exposure), (iv) sun protective attitude (e.g., sunscreen, sun avoiding), and (v) latitude during UV exposure.
The prevention of MM and NMSC is an essential factor; the measures are divided in sunscreen and physical barriers (special clothes). Sunscreen agents are able to absorb or reflect the UV radiation preventing the skin damages. They are made in a wide range of SPFs, which informs on the time that is needed to produce sunburn when the sunscreen is applied to the skin as compared to the unprotected skin. The efficacy of a sunscreen depends on such specific characteristics, such as: ingredients, general formulation (e.g., water-resistance), broad-spectrum, application patterns, sunscreen amount applied, exposure time, etc. [7].
“Sunscreen product” means any preparation (such as creams, oils, gels, sprays) that is intended to be placed in contact with the human skin with a view exclusively or mainly to protecting it from UV radiation by absorbing, scattering, or reflecting radiation [8].
Acute response of human skin to UVB irradiation includes erythema, edema, and pigment darkening, followed by delayed tanning, thickening of the epidermis and dermis, and synthesis of vitamin D; chronic UVB effects are photoaging, immunosuppression, and photocarcinogenesis [9,10].
The sun emits non-ionizing electromagnetic radiation (EMR) that is composed of UV (100–400 nm), visible (400–780 nm), and infrared (780–5000 nm) radiation. With regard to human health, UVR is the most relevant and concerning form of EMR (4–6). Ultraviolet radiation is composed of wavelengths between 100 and 400 nm that are further divided into UVC (100–290 nm), UVB (290–320 nm), and UVA (320–400 nm). Wavelengths that are below 290 nm are absorbed by atmospheric ozone and they do not reach the earth’s surface [11].
Ideal sunscreens provide uniform protection against ultraviolet A and B light, having anyway aesthetically pleasing compositions that enhance the user’s compliance.
Sunscreen vehicles often determine product efficacy. A sunscreen vehicle must minimize interaction of inert and active ingredients to maintain the photoprotective properties and photostability of its UV filters. Vehicle type also determines sunscreen durability and water resistance [12].
The heart of any sunscreen product is the ultraviolet absorber; ultraviolet filters are classified according to their action’s mechanism, physical filters (mineral filters), which act like glasses reflecting the light, and chemical filters (organic filters), which absorb the radiation’s energy, since they contain a suitable cromophore that has conjugated π-electron systems. Increasing the number of conjugated double bonds in the molecule the absorption maximum shifts to longer wavelengths and also gives rise to a larger absorption cross section and, therefore, stronger absorption [13].
All countries have a positive list of UV filters, including the maximum concentration allowed in sunscreens. In most countries, including Europe and Japan, UV absorbers are regulated as cosmetics, in the United States and Canada as OTC (Over The Counter) drugs, while in Australia as therapeutic drugs. The number of available UV filters differs from region to region; the US sunscreen monograph lists the least number of UV filters.
Regarding the EU legislation, Annex VI indicates 28 authorized substances, of which 26 are organic filters (e.g., Benzophenone-3, Butyl Methoxydibenzoylmethane, Ethylhexyl Methoxycinnamate, Ethylhexyl Triazone, Octocrylene, etc…) and just two are inorganic filters, which are Titanium Dioxide and Zinc Oxide [8].
UV filters can be broadly classified into two types: UV absorbers (chemical filters) and inorganic particulates (physical filters) [14].
The required feature of inorganic sunscreen filters is to screen/block UV light over the whole UVA/UVB range (290–400 nm) through scattering and reflection properties that, in turn, are determined by the intrinsic refractive index, the size of particles, dispersion in the emulsion base, and by film thickness. This kind of filters absorb considerable UV radiation.
On the other side, chemical organic filters are classified into either UVA (benzophenones, anthranilates, and dibenzoylmethanes) or UVB filters (PABA derivates, salycilates, cinnamates, and camphor derivates). These filters are almost always used in combination, because no single active agent, used at levels that are currently allowed by Regulations of different countries, provides high enough SPF (Sun Protection Factor) protection or broad-spectrum absorption.
This systematic review aims to provide a complete, exhaustive summary of current literature that is relevant to assessing the effects of sunscreens for preventing melanoma, non-melanoma skin cancer (basal or squamous carcinoma and melanoma), and precancerous skin lesions.
2. Materials and Methods
2.1. Criteria for Considering Studies for this Review. The Specification of Types of Studies, of Participants, of Interventions (and Comparisons), and the Types of Outcomes that Are of Interest Were Considered the Basis of the Pre-Specified Eligibility Criteria for this Work
- Types of studies
The following process was applied in order to select studies to be included into the review:
- Merge search results using reference management software, and remove duplicate records of the same report.
- Examine titles and abstracts to remove obviously irrelevant reports
- Examine full-text reports for compliance of studies with eligibility criteria.
- Make final decisions on study inclusion and proceed to data collection.
Any randomized controlled trial, case control, population-based cohort study that assessed incidence rate of MM, NMSC, and precancerous skin lesion (such as actinic keratosis, AK) was included.
- Types of participants
General population, including children and special population, was included in the following systematic review.
- Types of interventions
- Experimental studied measuring UVR induced damages in humane skin using sunscreen with Sun Protection Factor (SPF) at least 15 or more versus placebo or other interventions were considered in this review. The Sun Protection Factor refers to the product’s ability to screen or block out the UVB sun’s rays. Following the European guidelines, the sunscreen products must assure also at least 1/3 of protection against UVA in relation to the UVB protection. Thus, values lower than 15 were not considered, because they cannot guarantee a minimum of UVA protection.
- Type of outcomes measures
- -
- Primary outcomes: melanoma confirmed clinically or histopathologically at any follow-up, basal-cell carcinomas (BCC) confirmed clinically or histopathologically at any follow-up, squamous-cell carcinomas (SCC) confirmed clinically or histopathologically at any follow-up.
- -
- Secondary outcomes: actinic keratoses (AK) clinically or histopathologically confirmed at any follow-up. Studies that were conducted on animals, animal models, and cell lines were excluded.
2.2. Search Strategy for Identification of Studies
A comprehensive search strategy was developed, on-line searches, electronic searches, and searches in clinical trial registers were made. The relevant papers were searched while using following key words, or a combination of them, to identify the relevant papers: skin cancer, cutaneous tumor, melanoma, non-melanoma skin cancer (NMSC), basal cell carcinoma (BCC), squamous cell carcinoma (SCC), actinic keratoses (AK), sun-protection, sunscreen, UV filters, clinical trials, incidence, epidemiology, skin group. No restrictions on language were imposed during the search strategy. An investigator (C.A.C.) independently reviewed the titles, abstract, text, and abstracted data from the identified studies. On-line searchers: Google Scholar and Medline; electronic searches: the Cochrane database browse and the Cochrane Central Register of Controlled Trial (CENTRAL); clinical trial register: Australian New Zealand Clinical Trials Registry, WHO International Clinical Trials Registry Platform, and the EU Clinical Trial Register.
2.3. Extraction and Unification Data
An extraction form was developed to collect the relevant information from included papers:
- -
- General data: author and year of publication, study design, and characteristic of selected population.
- -
- Treatment strategy, in term of application of sunscreen alone or with oral supplementation.
- -
- Sunscreen information: SPF, brand, UV filters and their percentage, spectrum, and type of formulation.
- -
- Additional information: phototype, intentional exposure, sunscreen amount, latitude, reapplication.
- -
- Statistical information: statistical method used, adjusting for factors.
3. Result
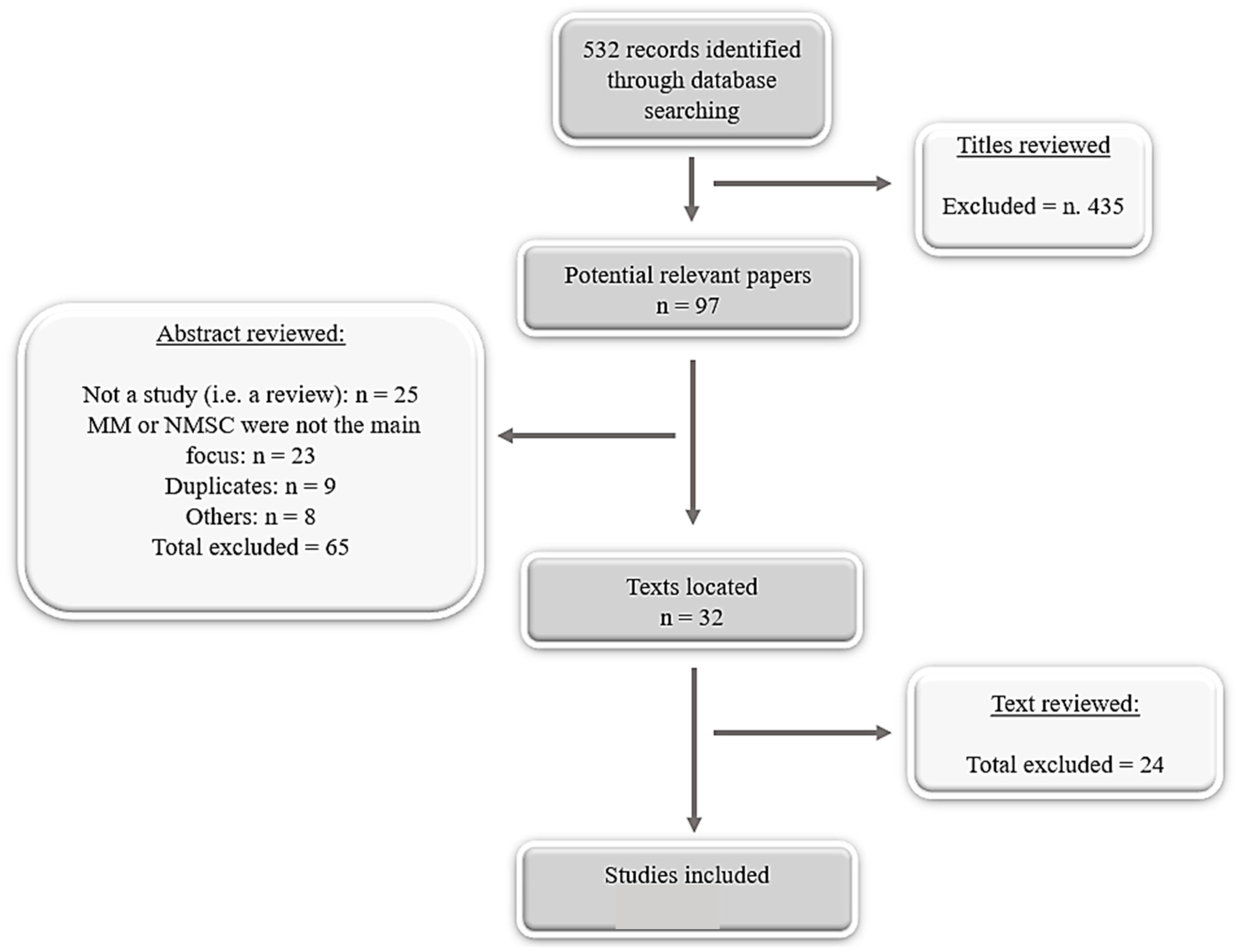
With the search strategy being defined, 532 publications were identified, with 97 being potentially eligible for inclusion based on title, after abstract reviewing 23 papers were excluded, because they did not exclusively focus on MM/NMSC or the application of sunscreen SPF 15 or more as prevention tool. 10 papers were duplicates. We included seven studies: two for MM, two for NMSC, and three for AK (Figure 1). The papers included in this systematic review provide data on four different countries over the period 1993–2017. For included studies were based on Australian population, one Norwegian population, one German population, and one Canadian population. In all of the papers, the population ages were evaluated in a range of 20–77. Data acquired form the experimental studies considered, were heterogeneous in terms of: (i) sunscreen SPF, (ii) UV filters actives, (iii) sunscreen brand, (iv) sunscreen application directive, and (v) additional info. Outcomes for melanoma, BCC/SCC, and precancerous skin lesions were separately analyzed.
3.1. Included Studies Description
3.1.1. Melanoma (MM)
Only two papers claimed a potential reduction of melanoma incidence after using sunscreen SPF > 15+. One study used a randomized controlled trial (RCT) and the other one the population-based cohort study (P-BCS). Both enrolled the general population from Australia or Norway.
Green A.C. in 2011 made a randomized controlled trial (RCT) follow-up, suggesting that melanoma may be preventable by regular sunscreen use in adults. A general population of 1,339 residents (~50% female and ~50% male, age between 20 and 69) from Nambour (Australia, latitude 26 °S) was selected and independently randomly assigned to four groups: (1) daily application of sunscreen broad-spectrum SPF 16 plus 30 mg betacarotene, (2) daily application of sunscreen broad-spectrum SPF 16 plus placebo tables, (3) betacarotente only, and (4) placebo only. Placebo sunscreen was considered unethical and was avoided. In the first group, free and unlimited supply of broad-spectrum sunscreen containing 8% of Octinoxate and 2% of Avobenzone was given. The participants not assigned to daily application of sunscreen were asked to continue the application of sunscreen at their usual discretionary rate, which for most was recreational use. Information regarding the risk factors for skin cancers, such as skin color (fair, medium, olive/brown), outdoor behavior (mainly outdoors, indoors and outdoors, mainly outdoors), and sunburn history (none, once, 2–5, >5), was obtained at baseline. Self-application of a layer to all the exposed sites every morning was requested, and reapplication was suggested for heavy sweating or after long exposure. The amount of sunscreen applied during exposure was estimated by weighting sunscreen returned battels. No information about relative latitude during the sun exposure was recorded [15].
In the second paper, Ghiasvand R. in 2016 with a P-BCS enrolled Norwegian general population with age between 30 and 75 years. 171,725 subjects were enrolled. Specific information about the time spent under the sun and the relative latitude were asked. The sunscreen brand and SPF were selected by the single participant, but precise information regarding the occasion of use of sunscreen were asked in order to know which sunscreen was used in high or low latitude condition. Based on the fact that sunscreen SPF 15 is considered to be sufficient to prevent sunburn if properly applied, the population was divided in three groups: (1) sunscreen non-users, when they did not indicate sunscreen use or they indicate SPF 0; (2) sunscreen users SPF < 15; and, (3) sunscreen users SPF ≥ 15. The phenotype of participantes were recorded by a color scale that was graded from 1 (very fair) to 10 (very dark brown) in relation to their skin color. Participants getting a score from 8 to 10 were excluded from the study. Other phenotype characteristics were recorded as: hair color, freckles, and nevi. History of indoor tanning were reported. Skin reactions before, during, and after sun exposure were recorded. The study excluded participants who had been given a diagnosis of melanoma. The study evaluated the patterns and intensity of the sun exposure for European people who receive intense UV exposure mainly during summer vacation [16].
3.1.2. Non-Melanoma Skin Cancer (NMSC)
Three studies claimed a potential reduction of BCC and SCC incidence after using of sunscreen. A RCT and its follow up seven years late with randomly selected population form Australia and a case-control (C-C) with 120 immunocompromised organ transplant form Berlin. Green A.C. et al. [17] and in Van Der Pols J.C. et al. [18] conducted a RCT in 1999 and its follow-up in 2006 with the specific outcomes, which were previously reported in the study made from Green A.C. et al. in 2011 [17].
Ulrich C. et al. randomly selected 120 patients in 2009 immunocompromised, with age between 40 to 77, form Charite’ University Hospital in Berlin, Germany. The population was divided in relation to the Fitzpatrick’s skin type and it was considered only in patients with type II and III avoiding population with very fair or very dark skin. In order to make 2 groups comparable, the type of immunosuppression was evaluated and equally distributed. Specific information about sunscreen formulation used: water-resistant cream Daylong actinica, Spirig Pharma Ltd. (Egerkingen, Switzerland) with several UV filters (bemotrizinol, octyl Triazone, isoamyl p-methoxycinnamate, ethylhexyl methoxycinnamate, methylene bis-benzotriazolyl tetramethylbutylphenol, avobenzone) rated as sunscreen SPF > 60 for UV-B, according to the EU commission recommendation (26/9/2006), and the product also delivers high UV-A protection, according to the Australian Standards (AS/NZS 2604–1997). The population was divided in sunscreen and control groups. In both groups, information regarding sun intense unprotected UV exposure risks and sun protection behaviors, in the specific the use of sunscreen were given. Specifically, all of the patients were awarded to apply at least 2 mg/cm2 on the exposed areas 20–30 min. before UV exposure [19].
3.1.3. Precancerous Skin Lesions (PSL)
Three studies focusing on the prevention PSL using sunscreen were identified. Two RTC and one prospective, double-blind, controlled trial (PCT).
Thompson SC. enrolled 588 subjects living in Maryborough (Australia) in 1993 and randomly assigned to the sunscreen or base-cream groups. The sunscreen composition was specified as broad-spectrum sunscreen cream containing 8% of Octinoxate and 2% of Avobenzone with SPF 17 (according to Australian Standard 2604 1986). The instructions were to apply 1.5 mL of sunscreen on the exposed spots of the skin every day and reapplying it was suggested if necessary. The number of new lesions appeared, and the remission of existing ones were evaluated [20].
In 1995, Naylor M.F. set up a PCT from 1987 to 1990. 90 participants with clinical evidence of AKS or NMSC were divided in treatment group or placebo group. The treatment received sunscreen SPF 29 contained methoxycinnamate, benzophenone-3, and octyl salicylate (UVB protection). Information regarding the negative side of sun overexposure were given, but no information about the sunscreen amount or reapplication was allowed; the participants were encouraged to use their usual routines. The amount of sunscreen used was approximately estimated counting the bottle request during the trial (max 2 battle 120 mL per month) [21].
3.2. General Data Results and Statistical Evaluation
Table 1 shows the seven datasets that were included with a total of 177,104 subjects. In six cases, the population was randomly enrolled collecting general population, one consists of high risk population and the last one focused on immunocompromised population. Most of the selected articles concerned a randomized controlled trial, population-based cohort, and prospective double-blind controlled trial. The studies were performed in Australia, Norway, Germany, and Canada. The ages of the subjects were in the range of 20 to 77 years old; sunlight susceptibility was determined following Fitzpatrick classification or authors suitable protocol. Data, such as hair color, freckling, nevi, etc., were examined and recorded by the authors. The findings were reported as hazard ration 95% confidence intervals [15,16] in two studies, relative risk 95% confidence in three studies [17,18,22], and in mean differences 95% confidence intervals in one study [20].
In the study that was conducted by Green A.C. et al. in 2011, 11 new primary melanomas were identified in the daily application sunscreen versus 22 new primary melanomas that were detected in the control group and a substantial reduction of invasive melanoma (three versus 11 in the control group) was observed. Invasive melanoma was reduced by 73% in the daily sunscreen group, the diagnosticated melanoma average thickness was 1.2 mm in the control group and 0.5 mm in the intervention group. In the control group, 38% of the subjects did not use sunscreen or applied it maximally twice a week (35%), in the intervention group 75% of the subjects claimed to use sunscreen. Time that was spent under the sun was close for both groups during the trial, 79% for intervention group, and 77% for control group, spent less than 50% of weekend time outdoors. Around 60% of both groups used sunscreen-alternative sun protection actions (shade avoiding, hat, etc.) [15].
Ghiasvand R. in 2016 concluded that the use of sunscreen with SPF 15+ or more could potentially reduce the melanoma incidence by 18%. Significative differences were observed between the sunscreen group and the control group; sunscreen users were mainly the youngest part of the selected population, living in the areas with higher ambient UV radiation, higher education, and closer to phenotype I/II. Skin reaction, such as sunburn, were correlated to a higher risk of melanoma, even in the sunscreen group, sunscreen users with no history of sunburn tended to have lower incidence of melanoma. In 10.7 years follow-up, 722 new cases of melanoma were diagnosticated, the most common areas were: limb, trunk, head, and neck with 56% of spreading melanoma and 15% of nodular melanoma [16].
In 1999, Green A.C. et al. detected a prevention action for daily application of sunscreen for SCC, but not for BCC, because lower incidence for SCC (1508 versus 1146 per 100,000) was shown in the daily sunscreen group when compared to the control group, but no significative difference was detected in BCC incidence. Until 1996, the new skin cancer cases were 1343 in 441 subjects, 67% were histologically confirmed or reviewed on medical records (33%). SCC incidence was significatly lower in intervention groups when compared with control group; instead, BCC incidence did not show any difference between the intervention group and control group [17]. Some years later, during the follow-up in 2006, previous findings were confirmed. No significant decrease (25%) in BCC incidence was observed in the sunscreen users group as compared with the control group, but the SCC incidence rates presented a significant value (38%) in sunscreen users group when compared to the control one [18].
Ulrich C. also found that the daily application of sunscreen could prevent the development of AK and invasive SCC, but the same positive result was confirmed for BCC. In 24 months study, significantly less lesions were detected in the sunscreen group when compared to the control group (89 vs. 273; P < 0.01), with a good tolerance for the sunscreen formulation. Additionally, the vitamin D levels were monitored, showing a lower level of vitamin in the sunscreen group when compared to the control group (53 ng/mL1 vs. 60 ng mL). During the 24 months trial, 19 new invasive NMSC were histologically confirmed in 22 subjects, eight new SCC, and two new BCC cases were identified in the control group versus, respectively, 0 and 3 new cases in the intervention group [19].
Three studies reported a positive result regarding the action of sunscreen on the progression of AK. In the RCT that was conducted by Thompson SC., a mean increase of 1.0 ± 0.3 in AK count for control group as compared to sunscreen group (0.6 ± 0.3). The control group had 508 new lesions and 18% of lesion remission when compared to the 333 new lesions and 25% remission detected in sunscreen group, hence the sunscreen use prevents the development if AK and promoted the regression of the existing ones. The amount of cream during the study used was similar in both the intervention and control group, and only a difference between the two sexes was observed: the man used more cream than woman. The incidence of new lesions was correlated to the amount of sunscreen used, 23% of the new lesions were found in the subject using less than 500 g of sunscreen, and the percentage is reduced at 12% in the subject using more than 1000 g [20]. In its study, Naylor M.F reported less appearance rate of AK in the sunscreen group when compared to the control group. The control group showed an average of 27.9 AK per year as compared to the intervention group, where the average was 13.6 AK per year [21]. Darlington S. concludes that there is a decrease in the ratio of AK counts for the sunscreen group when compared with the control group (24%) [22].
4. Discussion
Comments on Included Studies
Few observations regarding the exanimated studies can be made (Table 2). This systematic review wants to evaluate the effectiveness of sunscreen in preventing melanoma, non-melanoma skin cancer (basal or squamous carcinoma and melanoma), and precancerous skin lesions. The effectiveness of a sunscreen is regulated by multifactorial model. It depends not only on its SPF, UV spectral absorption, or sunscreen actives, but also the amount applied, type of sunscreen formulation, coverage of sun-exposed parts, reapplication, sun elevation, etc.
A sunscreen is defined “broad-spectrum” when it is able to protect against both UVA and UVB offering a full covered protection. In five studies [15,17,18,20,22], were given specific information regarding sunscreen, such as SPF rating, sunscreen brand, type of sunscreen formulation, and UV filters percentage. For those studies, the formulation was the same and it was identified as a water-resistant sunscreen SPF 16 broad-spectrum (Auscreen Ultrablock Lotion SPF 15-plus, Ross Cosmetics, Melbourne, Australia), with 8% octinoxate and 2% avobenzone. In one study [19] was specified the sunscreen UV filters, but the percentages were not available and it was used a sunscreen protection with SPF 60+ for UVB and a “high” UVA protection, according to the Australian Standards (AS ⁄NZS 2604–1997). In the study n. 14, it has been used a sunscreen SPF 29 only absorbing in the UVB range and the sunscreen brand, the type of formulation, and the percentage of UV filters were not specified, and the sunscreen choice was made following the usual participants sunscreen routine in the study n. 9.
The guidelines from the FDA [23] and the international Organization for Standardization [24] agreed that the amount of sunscreen applied for testing SPF should be 2 mg/cm2. This is the amount of sunscreen that is necessary to achieve the labeled SPF rating. Additionally, applying the recommended quantity of sunscreen is not a guarantee for proper protection against UV radiation. The sunscreen application and the relative body coverage after application are the premises for a full activated protection. The sunscreen should stay stable during UV exposure on the superficial part of the skin in order to create a protective film. In the included studies, only in one case [19], in the sunscreen group, were the participants trained to apply 2 mg/cm2 on the exposed areas, 20–30 min. before leaving the shade. In all the other studies followed a self-application of a layer to all exposed sites every morning or following the participants usual routine, and the sunscreen application was only a suggestion in almost all the studies. The reapplication of the sunscreen every two hours or after working, swimming, playing, or exercising outdoors is mandatory in guaranteeing the complete protection over all the exposure time.
In literature, studies showed that there is a close relation between the incidence rate of MM and NMSC and the ambient solar latitude gradient. The skin cancer incidence increases with a decreasing of the latitude, where there is the greater UV energy to which they are exposed [25]. Additionally, ambient factor as ozone layer depletion plays a role. The ozone layer is a region of the Earth’s stratosphere that it is able to absorb some of sun UVR radiation; its depletion leads to region overexposed to UVR [26]. Ozone depletion is most evident in polar regions, studies have related close correlation between an increase of the skin cancer incidence in Caucasians living near those regions [27]. There was specific information regarding where the participants used sunscreen within Norway or other location, during vacation, in low or high latitude, and which sunscreen they used in that occasion in only in one study [16]. We should consider that the trial conduced in subtropical areas consists of mainly unintentional sun exposure, because the population is well aware about the hazard risk about exposure. Instead, Europeans and North Americans occasionally expose themselves to UV light, mainly during the summer. Accordingly, we considered that the intentional exposure to the sunlight is not related to the time spent outside, but it has to be connected with the intention of the single person. Two different type of sun exposure patterns came up: non-intentional sun exposure (NISE) and intentional sun exposure (ISE). The NISE type does not have interest in acquiring a tan, the exposure is related to the daily life activities or occasional exposure enjoying the time spent outside in the sun, but avoiding uncovered long and intense exposure. The ISE type stays under the sun a big number of hours per day with uncovered skin with the porpoise to acquire [28].
The sun-protective behaviors and sunscreen application patterns are fundamental and they should be not left outside of a study. All of the factors pointed out above should be considerate in order to have a result that expresses the real effect of sunscreen action and not just the expression of intrinsic risks.
5. Conclusions
In the current socio-economic scenario, there is a significant increase in skin cancer cases per year, followed by constant pressure to reduce the costs related to medical treatments (direct costs), extra-medical expenses, and humane intangible costs. In the health system, the assessment of these costs is essential in concentrating the resources. Pharmacoeconomic evaluation models are able to identify the value (convenience) and the economic impact of a specific intervention providing the better facility at minimum cost. This systematic review intended to be a scientific tool that uses a reproducible and transparent approach to evaluate the results of individual studies making them available to the health care decision makers. Sunscreen use as strategy for sun protection has been criticized for its long-term activity, such as protection against MM and NMSC development. The studies that were included in this systematic review support the beneficial effects of the sunscreen as a tool to prevent the harmful effect of UV radiation; however, several comments regarding sunscreen selection and application were made. Sunscreen spectrum, its modality of application, and the amount applied should be considered essential factors for sunscreen activity. Studies conducted with a standardized protocol to evaluate the real efficacy of a sunscreen and not just the variation of sunscreen intrinsic factors are needed.
Author Contributions
P.P., A.C.C. and G.L.C. designed the study. A.C.C. and M.B. performed the review of literature. All authors wrote the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rogers, H.W.; Weinstock, M.A.; Harris, A.R.; Hinckley, M.R.; Feldman, S.R.; Fleischer, A.B.; Coldiron, B.M. Incidence estimate of nonmelanoma skin cancer in the United States 2006. Arch. Dermatol. 2010, 146, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Apalla, Z.; Lallas, A.; Sotiriou, E.; Lazaridou, E.; Ioannides, D. Epidemiological trends in skin cancer. Dermatol. Pract. Concept. 2017, 7, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scherer, D.; Kumar, R. Genetics of pigmentation in skin cancer—A review. Mutat. Res. 2010, 705, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Erb, P.; Jingmin, J.; Kump, E.; Mielgo, A.; Wernli, M. Apoptosis and pathogenesis of melanoma and non-melanoma skin cancer. Adv. Exp. Med. Biol. 2008, 624, 283–295. [Google Scholar] [PubMed]
- Salasche, S.J. Epidemiology of actinic keratoses and squamous cell carcinoma. J. Am. Acad. Dermatol. 2000, 42, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Madan, V.; Lear, J.T.; Szeimies, R.M. Non-melanoma skin cancer. Lancet 2010, 375, 673–685. [Google Scholar] [CrossRef] [Green Version]
- Schalka, S.; Manoel, V.; Dos Reis, S., II. Sun protection factor: Meaning and controversies. An. Bras. Dermatol. 2011, 86, 507–515. [Google Scholar] [CrossRef]
- European Union. Regulation (EC) No 1223/2009 of the European Parliament and of the Council of the on Cosmetic Products. Off. J. Eur. Union L 2009, 342, 1. [Google Scholar]
- Kullavanijaya, P.; Lim, H.W. Photoprotection. J. Am. Acad. Dermatol. 2005, 52, 937–958. [Google Scholar] [CrossRef]
- Gil, E.M.; Kim, T.H. UV-induced immune suppression and sunscreen. Photodermatol. Photoimmunol. Photomed. 2000, 16, 101–110. [Google Scholar] [CrossRef]
- Stiefel, C.; Schwack, W. Photoprotection in changing times UV filter efficacy and safety, sensitization processes and regulatory aspects. Int. J. Cosmet. Sci. 2015, 37, 2–30. [Google Scholar] [CrossRef]
- Sambandan, D.R.; Ratner, D. Sunscreens: An overview and update. J. Am. Acad. Dermatol. 2011, 64, 748–758. [Google Scholar] [CrossRef] [PubMed]
- John, J.; Prue, F.J.; Hart, H. Photoprotection: Sunscreens and the immunomodulatory effects of UV irradiation. Mutat. Res. 1998, 422, 155–159. [Google Scholar]
- Nadim, A. Shaath, Ultraviolet filters. Photochem. Photobiol. Sci. 2010, 9, 464–469. [Google Scholar]
- Green, A.C.; Gail, W.M.; Logan, V.; Strutton, G.M. Reduced Melanoma after Regular Sunscreen Use: Randomized Trial Follow-Up. J. Clin. Oncol. 2011, 29, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Ghiasvand, R.; Weiderpass, E.; Green, A.C.; Lund, E.; Veierød, M.B. Sunscreen Use and Subsequent Melanoma Risk: A Population-Based Cohort Study. J. Clin. Oncol. 2016, 34, 3976–3982. [Google Scholar] [CrossRef] [PubMed]
- Green, A.C.; Gail, W.M.; Neale, R.; Hart, V.; Leslie, D.; Parsons, P.; Marks, G.; Gaffney, P.; Battistuta, D.; Frost, C.; et al. Daily sunscreen application and betacarotene supplementation in prevention of basal-cell and squamous-cell carcinomas of the skin: A randomized controlled trial. Lancet 1999, 354, 723–729. [Google Scholar] [CrossRef]
- Van Der Pols, J.C.; Williams, G.M.; Pandeya, N.; Logan, V.; Green, A.C. Prolonged Prevention of Squamous Cell Carcinoma of the Skin by Regular Sunscreen Use. Cancer Epidemiol. Biomark. Prev. 2006, 15, 2546–2548. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, C.; Jurgensen, J.S.; Degen, A.; Hackethal, M.; Ulrich, M.; Patel, M.J.; Eberle, J.; Terhorst, D.; Sterry, W.; Stockfleth, E. Prevention of non-melanoma skin cancer in organ transplant patients by regular use of a sunscreen: A 24 month, prospective, case-control study. Br. J. Dermatol. 2009, 161, 78–84. [Google Scholar] [CrossRef]
- Thompson, S.C. Reduction of solar keratoses by regular sunscreen use. N. Engl. J. Med. 1993, 329, 1147–1151. [Google Scholar] [CrossRef]
- Naylor, M.F.; Boyd, A.; Smith, D.W.; Cameron, G.S.; Hubbard, D.; Neldner, K.H. High Sun Protection Factor Sunscreens in the Suppression of Actinic Neoplasia. Arch. Dermatol. 1995, 131, 170–175. [Google Scholar] [CrossRef]
- Darlington, S.; Williams, G.; Neale, R.; Frost, C.; Green, A. A randomized controlled trial to assess sunscreen application and betacarotene supplementation in the prevent solar keratosis. Arch. Dermatol. 2003, 139, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Labelling and effectiveness testing; sunscreen drug products for over-the-counter human use. Fed. Regist. 2010, 76, 35620–35665. [Google Scholar]
- Standardization, T.I. Cosmetics—Sun Protection Test Methods—In Vivo Determination of the Sun Protection Factor (SPF) 2010; ISO; European Committee for Standardization (CEN): Brussels, Belgium, 2010; p. 4444. [Google Scholar]
- Scotto, J.; Fears, T.R.; Fraumeni, J.F. Incidence of Nonmelanoma Skin Cancer in the United States; US Department of Health and Human Services, NIH Publication: Rockville Pike, Bethesda, Maryland, April 1983; No. 83-2433.
- De Fabo, E.C. Artic stratospheric ozone depletion and increased UVB radiation: Potential impacts to human health. Int J. Circumpolar Health 2005, 64, 509–522. [Google Scholar] [CrossRef] [PubMed]
- Schaart, F.; Garbe, C.; Orfanos, C. Disappearance of the ozone layer and skin cancer: Attempt at risk assessment. Hautarzt 1993, 44, 63–68. [Google Scholar] [PubMed]
- Autier, P.; Boniol, M.; Doré, J.F. Sunscreen use and increased duration of intentional sun exposure: Still a burning issue. Int. J. Cancer 2007, 121, 1–5. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study flow diagram.


{kind=link}
Table 1.
Study’s findings. RTC: randomized controlled trial, P-BCS: population-based cohort study, C-C: case-control, CT: controlled trial, CI: confidence interval, HR: hazard ratio, RR: relative risk, MD: mean difference, PCT: prospective controlled trial.
Table 1.
Study’s findings. RTC: randomized controlled trial, P-BCS: population-based cohort study, C-C: case-control, CT: controlled trial, CI: confidence interval, HR: hazard ratio, RR: relative risk, MD: mean difference, PCT: prospective controlled trial.
| Study, Year | Population | Findings |
|---|---|---|
| MELANOMA | ||
| [15] Green A.C., 2011, RTC | Australia (Nambour, Queensland), n. 1339, general population, age 20–69 | Risk of melanoma reduced in daily sunscreen application compared with discretionary use, HR 0.50; 95% CI, 0.24 to 1.02. Invasive melanoma was reduced by 73% in the daily sunscreen group HR 0.27; 95% CI, 0.08 to 0.97 |
| [16] Ghiasvand R., 2016, P-BCS | Norway, n. 171,725, general population, age 30–75 | Risk of melanoma reduced in sunscreen SPF > 15 group compared with sunscreen SPF < 15, HR 0.67; 95% CI, 0.53 to 0.83 |
| NMSC | ||
| [17] Green A.C., 1999, RTC [18] Van Der Pols J.C., RTC follow-up 2006 | Australia (Nambour, Queensland), n. 1621, general population, age 20–69 | The incidence of SCC reduces in sunscreen group compared with control group, RR 0·61, 95% IC, 0·46–0·81. |
| [19] Ulrich C., 2009, C-C | Berlin, n. 120, immunocompromised organ transplant, age 40–77 | 8 new cases of SCC were developed in control group compared 0 diagnosticated in the intervention group (P < 0.01) and 2 new BCC cases in intervention groups compared to 3 cases in control group (n.s.). 11 BCC (2 vs. 9; ns). |
| AK | ||
| [20] Thompson SC., 1993, RCT | Australia, n. 588, general population, age over 40 | The incidence of AK reduces in sunscreen group compared with placebo group, MD 1.53, 95% CI, 0.8 to 2.25 |
| [21] Naylor M.F., 1995, PCT | USA, n. 90, high-risk population, age 39–70 | Reduction of 51% in appearance rate of AK in intervention group compared to the control group |
| [22] Darlington S., 2003, RTC | Australia (Nambour, Queensland), n. 1621, general population, age 20–69 | The AK incidence decreases in sunscreen group compared to no-sunscreen-group, 1992–1994: RR 0.78, 95% CI, 0.64–0.96; 1994–1996: RR 0.94, 95% CI, 0.75–1.19 |
Table 2.
Studies characteristic.
| Study, Year | Approaches | Sunscreen | Application | Additional Info | ||||
|---|---|---|---|---|---|---|---|---|
| Phototype | Intentional Exposure | Sunscreen Amount | Latitude | Re-application | ||||
| MM | ||||||||
| [15] Green A.C., 2011 | (1) sunscreen SPF 16 plus 30mg betacarotene (2) sunscreen SPF 16 plus placebo tables (3) betacarotente only (4) placebo only | SPF: 16, Sunscreen brand: Auscreen Ultrablock Lotion SPF 15-plus, Ross Cosmetics, Melbourne, Australia, Type of formulation: lotion water-resistant, UV filters percentage: 8% Octinoxate and 2% Avobenzone, Spectrum: broad-spectrum rated according to Australian Standard 2604.1. | Daily group: Self-application of a layer to all exposed sites every morning (suggestion: reapplication for heavy sweating or long sun exposure), Discretional group: continue application of sunscreen at their usual discretionary rate | Measured weights of returned bottles | Suggestion | |||
| [16] Ghiasvand R., 2016 | (1) sunscreen SPF < 15 (2) sunscreen SPF > 15 | Participants usual routine | Participants usual routine | Excluded: Very dark skin | High or low latitude | |||
| NMSC | ||||||||
| [17] Green A.C., 1999 [18] Van Der Pols J.C., 2006 | (1) sunscreen SPF 16 plus 30mg betacarotene (2) sunscreen SPF 16 plus placebo tables (3) betacarotente only (4) placebo only | SPF: 16, Sunscreen brand: Auscreen Ultrablock Lotion SPF 15-plus, Ross Cosmetics, Melbourne, Australia, Type of formulation: lotion water-resistant, UV filters percentage: 8% Octinoxate and 2% Avobenzone, Spectrum: broad-spectrum rated according to Australian Standard 2604.1. | Daily group: Self-application of a layer to all exposed sites every morning (suggestion: reapplication for heavy sweating or long sun exposure), discretional group: continue application of sunscreen at their usual discretionary rate | Measured weights of returned bottles | Suggestion | |||
| [19] Ulrich C., 2009 | (1) sunscreen SPF 50 plus education (2) sunscreen SPF 50 self-responsible application | SPF: 60+, Sunscreen brand: Daylong actinica; Spirig Pharma Ltd. Switzerland, Type of formulation: water-resistant cream lotion, UV filters: Bis-ethylhexyloxyphenol methoxyphenyl triazine, ethylhexyl triazone, isoamyl p-tetramethylbutylphenol, butyl methoxydibenzoylmethanemethoxycinnamate, ethylhexyl methoxycinnamate and methylene bis-benzotriazolyl, Spectrum: SPF over 60 for UVB, good UVA protection according to the Australian Standards. | Both groups: Written and oral information on sun protection, Sunscreen group: trained 2 mg cm2 to the head, neck, forearms, and hands. | Included: only phenotype II and III | 2mg/cm2 | |||
| AK | ||||||||
| [20] Thmpson SC., 1993 | (1) sunscreen SPF 17, (2) placebo. | SPF: 16, Sunscreen brand: Auscreen Ultrablock Lotion SPF 15-plus, Ross Cosmetics, Melbourne, Australia, Type of formulation: lotion water-resistant, UV filters percentage: 8% Octinoxate and 2% Avobenzone, Spectrum: broad-spectrum rated according to Australian Standard 2604.1. | apply 1.5 mL of sunscreen on exposed spots of the skin every day and it was suggest reapplying it if necessary. | 1.5 mL per day | Suggestion | |||
| [21] Naylor M.F., 1995 | (1) sunscreen SPF 29, (2) placebo. | SPF: 29, Sunscreen brand: n.d., Type of formulation: n.d., UV filters presented: methoxycinnamate, benzophenone-3 and octyl salicylate, Spectrum absorption 280–320 nm (UVB). | participants usual routine. | Estimation n. battles ordered per month | Participants usual routine | |||
| [22] Darlington S., 2003 | (1) sunscreen broad-spectrum SPF 16 plus 30 mg betacarotene, (2) sunscreen broad-spectrum SPF 16 plus placebo tables, (3) betacarotente only, (4) placebo only. | SPF: 16, Sunscreen brand: Auscreen Ultrablock Lotion SPF 15-plus, Ross Cosmetics, Melbourne, Australia, Type of formulation: lotion water-resistant, UV filters percentage: 8% Octinoxate and 2% Avobenzone, Spectrum: broad-spectrum rated according to Australian Standard 2604.1. | Daily group: Self-application of a layer to all exposed sites every morning (suggestion: reapplication for heavy sweating or long sun exposure), discretional group: continue application of sunscreen at their usual discretionary rate. | Measured weights of returned bottles | Suggestion | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Perugini, P.; Bonetti, M.; Cozzi, A.C.; Colombo, G.L. Topical Sunscreen Application Preventing Skin Cancer: Systematic Review. Cosmetics 2019, 6, 42. https://doi.org/10.3390/cosmetics6030042
AMA Style
Perugini P, Bonetti M, Cozzi AC, Colombo GL. Topical Sunscreen Application Preventing Skin Cancer: Systematic Review. Cosmetics. 2019; 6(3):42. https://doi.org/10.3390/cosmetics6030042
Chicago/Turabian StylePerugini, Paola, Margherita Bonetti, Arianna Cecilia Cozzi, and Giorgio Lorenzo Colombo. 2019. "Topical Sunscreen Application Preventing Skin Cancer: Systematic Review" Cosmetics 6, no. 3: 42. https://doi.org/10.3390/cosmetics6030042
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.