1. Introduction
This article examines the role of religiosity and religious coping (RC) when adjusting to traumatic events, both in attenuation of symptoms and favouring positive effects of growth. We will discuss the relationship between positive and negative RC with social support and its role both in symptoms of trauma and posttraumatic growth. Reviewed studies suggest the potential role of RC as a moderator between adjustment and others forms of coping like social support and also suggest that RC is different from other forms of coping—like coping by seeking social support.
There is evidence indicating that religiosity helps to cope with highly stressful or potentially traumatic events. For example, religious beliefs can help in re-evaluating stressful situations such as a mild threat or a challenge [
1], or help in attributing meaning to them [
2]. Stressful or traumatic experiences can, in turn, lead to a deepening of religiosity [
1].
One of the probable positive consequences after living through an extreme event is posttraumatic growth (PTG), defined as the perception of positive changes in self and in relations with others, as a result of the struggle needed to deal with the consequences of a highly stressful or traumatic event [
3]. Meta-analyses by Helgeson, Reynolds and Tomich [
4] and by Prati and Pietrantoni [
5] identify religiosity as one of the factors associated to the development of PTG. For example, a positive relationship has been found between RC and PTG in patients with cancer [
6] and in survivors of a natural disaster [
7,
8,
9]. However, Pargament, Feuille and Burdzy [
10] warn that RC can also lead to harmful results. For this reason, the investigation must recognize ‘the bitter’ as much ‘the sweet’ in religious attitudes. In the same vein, Pargament, Smith, Koenig and Perez [
11] differentiate between positive and negative RC. The former leads to psychological and spiritual satisfaction, based on spiritual support, religious purification, looking for help from priests or church members and religious forgiveness. The latter refers to a punitive religious appreciation, spiritual unrest and interpersonal religious unrest. Studies show a different relationship between positive and negative RC with the psychological effects that occur after a stressful traumatic event. In one of the first studies regarding this field, Koenig, Pargament and Nielsen [
12] observed that those who had a negative religious view showed low physical health and higher levels of depression. Conversely, a positive religious view was linked to a more positive mental health. Other longitudinal investigations have shown that an increased spiritual questioning at the onset of a negative experience is a predictor of a significant increase in the indexes of psychological disorders over time [
13,
14]. The study by Pargament et al. [
14] also shows us that positive RC is associated to improvements in health, and negative RC is associated with the decrease of health over time. In the study by Harris et al. [
15], negative RC showed a significant positive relationship with posttraumatic symptoms (PTS) both immediately after and a year later. On the other hand, positive RC did not show a relationship with PTS in any of the two instances. While PTS have a direct relationship with negative RC [
16,
17,
18,
19], positive RC is associated to an increase of PTG as time passes [
14]. Other studies have shown that PTG has a direct relationship with positive RC [
1,
8,
20]. For example, in the study performed by Ai, Hall, Pargament and Tice [
21] with heart patients, it was observed that positive pre-operation RC predicts PTG thirty months after operation.
Prominent among the non-religious psychosocial factors and coping strategies associated to psychological responses after a stressful event are the perceived level and seeking of social support or asking and receiving emotional, instrumental and informative help from others to deal with stress. Social support is defined as the perceived or actual group of instrumental and expressive dispositions, which are emitted by various sources [
22]. Social support decreases the cognitive impact of stressful events, it allows a better regulation of negative emotions, it favours the control of dysfunctional conducts, reinforces distraction and gratification activities, and it helps to better solve practical problems, which jointly contributes to an increase in PTG—both social support and coping by seeking social support were associated to PTG in a meta-analysis [
5]. It has also been postulated that an increase in social support could be one of the processes by which religious coping and religiosity are positively associated with adjusting to stress and experiencing less symptomatology [
23]. Two studies have confirmed this association by showing that the more negative RC, the less social support [
24], and that the higher RC, the higher social support [
8]. The studies of Avilés, Cova, Bustos and García [
25] and the authors [
8] have suggested that social support is not the only mechanism by which RC has a positive effect such as PTG. These studies showed that positive RC is associated to PTG even after controlling for social support. This evidence showed that religiosity helps growth beyond its function as a provider of social networks that are supportive in the spiritual area, as other studies have suggested [
21]. Both studies also showed that positive RC was a stronger predictor of PTG than social support.
Perceiving an event as severe also has an important influence in the psychological responses to stressful events. An association has been observed between severity and PTS [
26,
27]. A similar association has also been observed between subjectively perceived severity and PTG in a meta-analysis [
5] and in two studies with survivors of an earthquake [
8,
28]. This is a population in which Shakespeare-Finch and Lurie-Beck [
29] have found positive relationships between PTS and PTG without finding the same association when exposed to other types of events. The influence of the severity of event on psychological responses also appears to be mediated [
8] or moderated [
30] by RC.
Thus, it seems especially interesting to evaluate the role of religiosity as a mediator or moderator between predicting variables and psychological responses. It has been observed that negative RC acts as a process that explains the increase of symptoms and hinders growth. For example, it mediated between the experience of childhood abuse and PTS [
31], it dampened the relationship between direct traumatic events and PTG [
32], and it strengthened the relationship between stress and depression [
33]. Positive RC also acts as a mediator or an explanatory process, but in an opposite way, because it partially mediated the relationship between gender and PTG [
16], or it totally mediated the relationship between subject severity and PTG [
8].
With this background, we hypothesize that severity of event will be associated with PTS and PTG, positive RC and perceived social support will be associated to PTG, while RC and low social support will be associated to PTS. We also expect that positive RC will moderate the relationship between social support and the change in PTG level and that the negative RC will moderate the relationship between subjective severity and the change in PTS levels.
3. Results
Regarding the stressful events, 22.7% mentioned the death of a loved one, 13.7% mentioned a natural disaster, 11.4% was affected by the serious disease of a loved one, 10.4% was affected by a breakup and 41.8% was affected by other stressful events such as a serious illness, an accident at home, a workplace accident, a car accident, violence from the state, violence at home or criminal violence, among others.
The results of the descriptive statistics of the variables (see
Table 1) showed asymmetry coefficients and curtosis lower than ±2.0, which indicates similarity with the normal curve [
45]. The internal consistency of the scales, established by Cronbach alpha coefficient, ranged between 0.82 (social support) and 0.95 (positive RC).
A Student t-test was performed for independent samples to observe if there were differences due to gender in the change of PTG and PTS. We did not observe differences, which is why gender was excluded as a control variable in hierarchical regressions.
Then, we explored the associations between subjective severity of event, positive and negative RC, social support, PTG, PTS. We also looked at how severity of event, RC and social support in Time 1 predict changes in PTG and PTS or differences between Time 1 and Time 2 PTG and PTS. The results are observed on
Table 2.
The table shows that subjective severity was unrelated with PTG in any case (T1, T2 and with changes scores), but severity had a significant relationship with PTS in general—at T1, T2 and with changes scores. In turn, positive RC shows a significant relationship with PTG at T1 and T2 and also positive RC at Time 1 was associated to the increase of PTG at T2. Positive RC does not show a significant relationship with PTS in any case. On the other hand, negative RC shows a significant relationship with PTS at T1 and T2, and predicts the increase in PTS. Negative RC does not have a significant relationship with PTG in any of the measurements. Coping by seeking social support shows positive and significant relationships with PTG in all cases. Globally, positive RC and social support were associated to PTG and unrelated to PTS. Conversely, negative RC was associated to PTS and unrelated to PTG.
Then, regressions were performed to predict the change (increase or decrease) of PTG and PTS. First, it was evaluated if RC influenced change in PTG, controlling for social support coping. For this reason, social support coping was included in the first step and positive and negative RC were incorporated in the second step. To evaluate a possible moderation, the interaction between social support and RC was included in a third step. The results show a significant model for the three steps, the third with a value F(4206) = 6.378,
p < 0.001; with an R
2 = 0.11 and a significant increase in explained variance of five percent—but in any case, effect of predictors or explained variance is not so strong. The results are shown on
Table 3. When RC was included in the second step, the positive association of coping by social support with the increase of PTG was no longer significant, while the negative RC decreases PTG, the positive RC increases PTG. In the third step, the three variables predict the change in PTG.
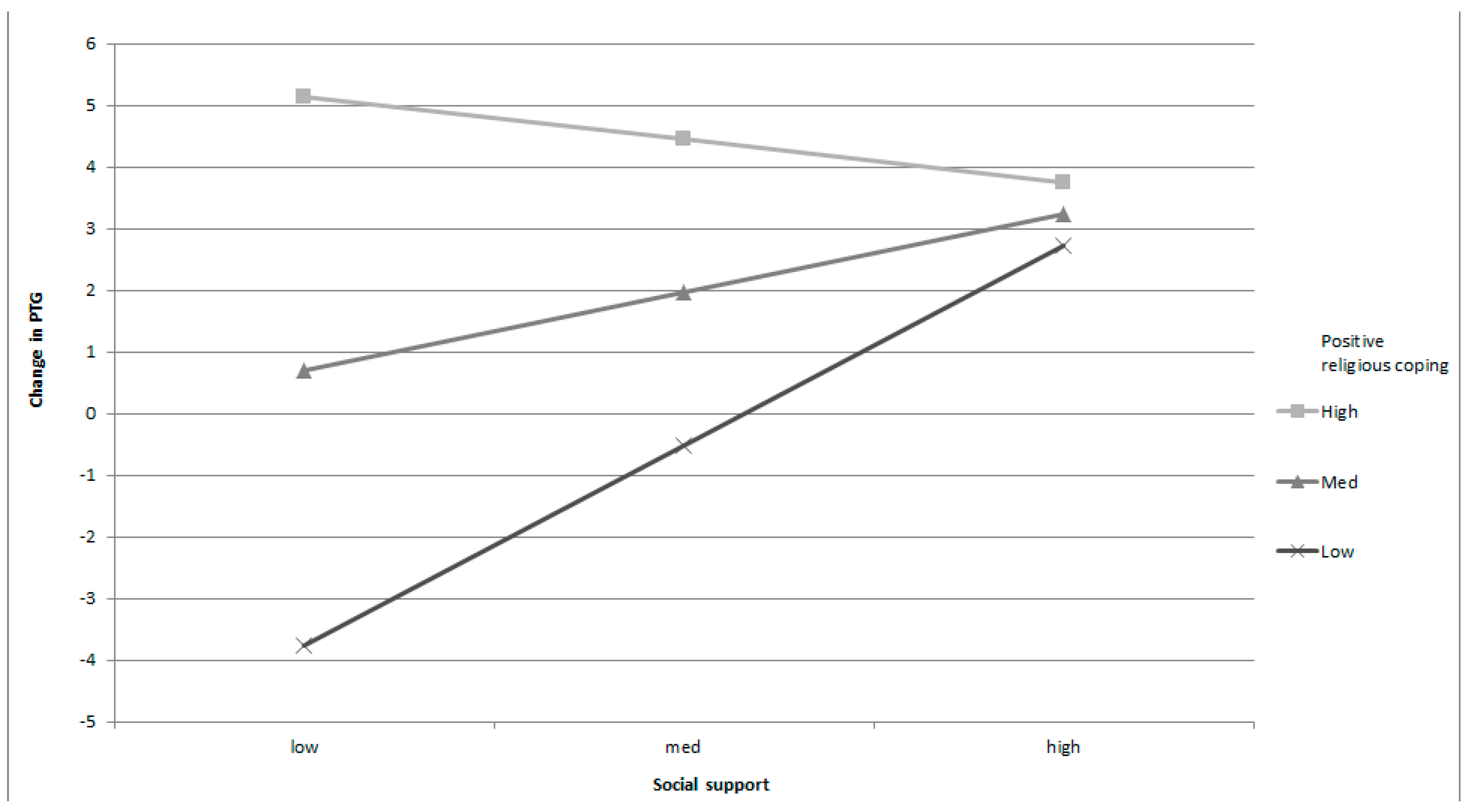
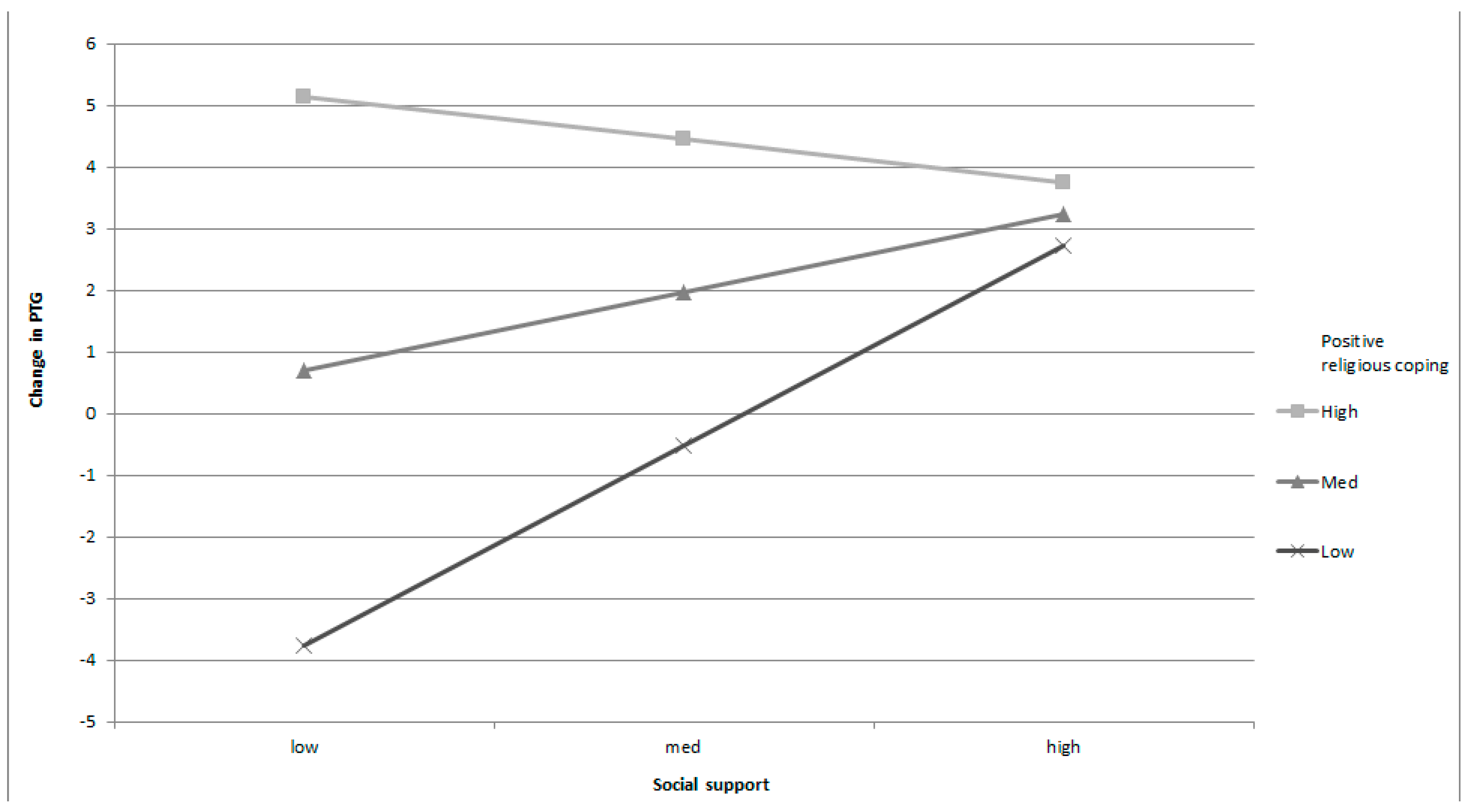
The significant interaction of positive RC and social support implies a moderation effect of positive RC on the relation between social support and change in PTG. Regarding these moderation effects in
Table 4, a low level of positive RC is associated to a significant and positive association of social support with an incremental change in PTG, while at a high level of positive RC level social support was not associated to change in PTG (see
Figure 1). When positive RC is low, social support was strongly associated to the increase of PTG; when positive RC is moderate, the relationship between support and change is positive but weaker; when positive RC is high, there is no relationship between social support level and PTG changes. In other words, social support has a strong influence on the change in PTG when positive RC is low.
A second hierarchical regression evaluated the influence of RC on the change in PTS, controlling for subjective severity of event. Consequently, subjective severity was included in the first step, and positive and negative RC were incorporated in the second step. To evaluate a possible moderation, the interaction between subject severity and negative RC was included in a third step. The results show a significant model for the first and third steps, the third with a value F(4206) = 3.384,
p < 0.01; with an R
2 = 0.06 , that is a limited amount of explained variance controlling severity, the influence of RC in the increase of PTS was not significant in step 2. In step three, only interaction has significance. The results are observed in
Table 5.
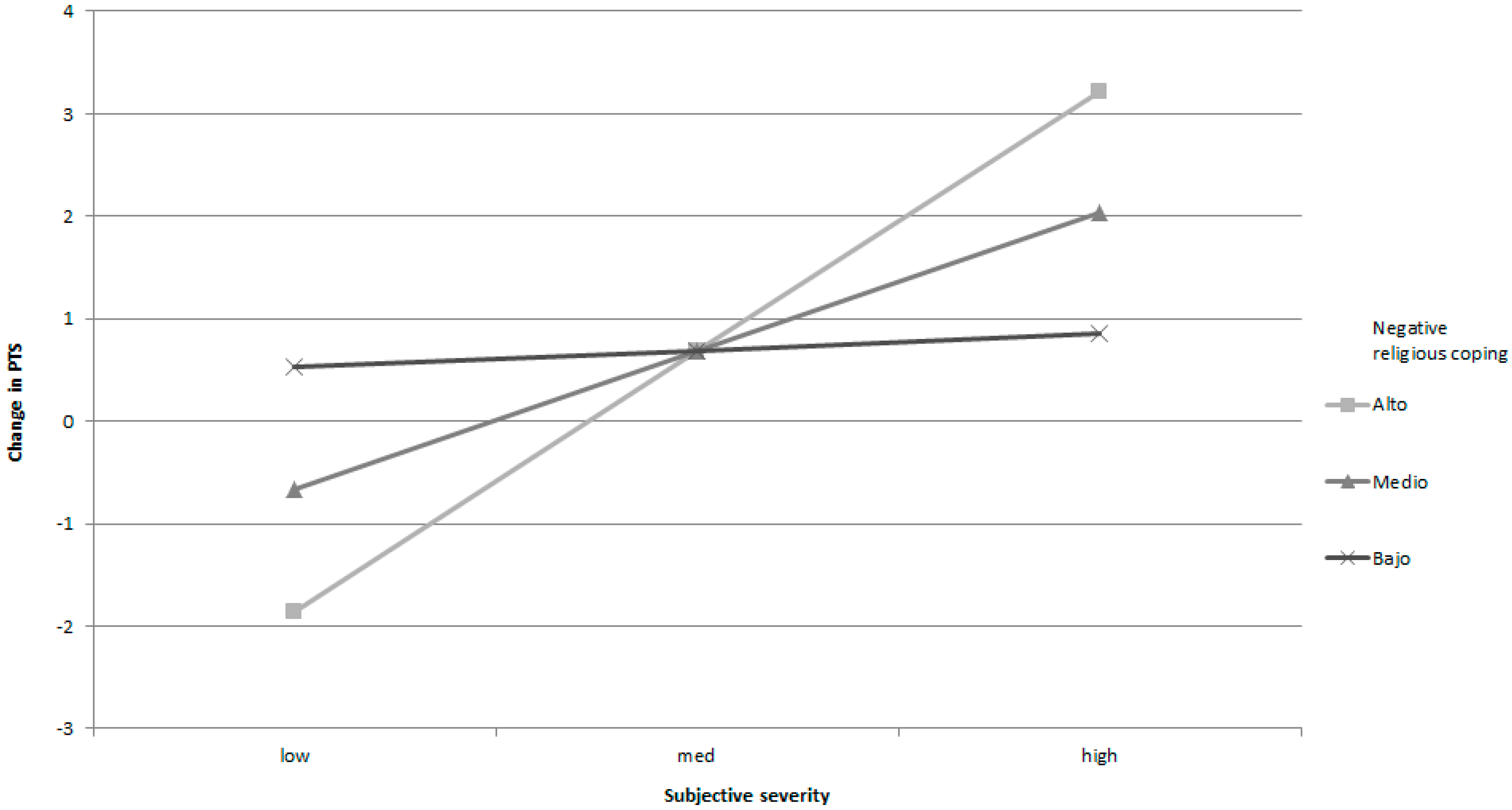
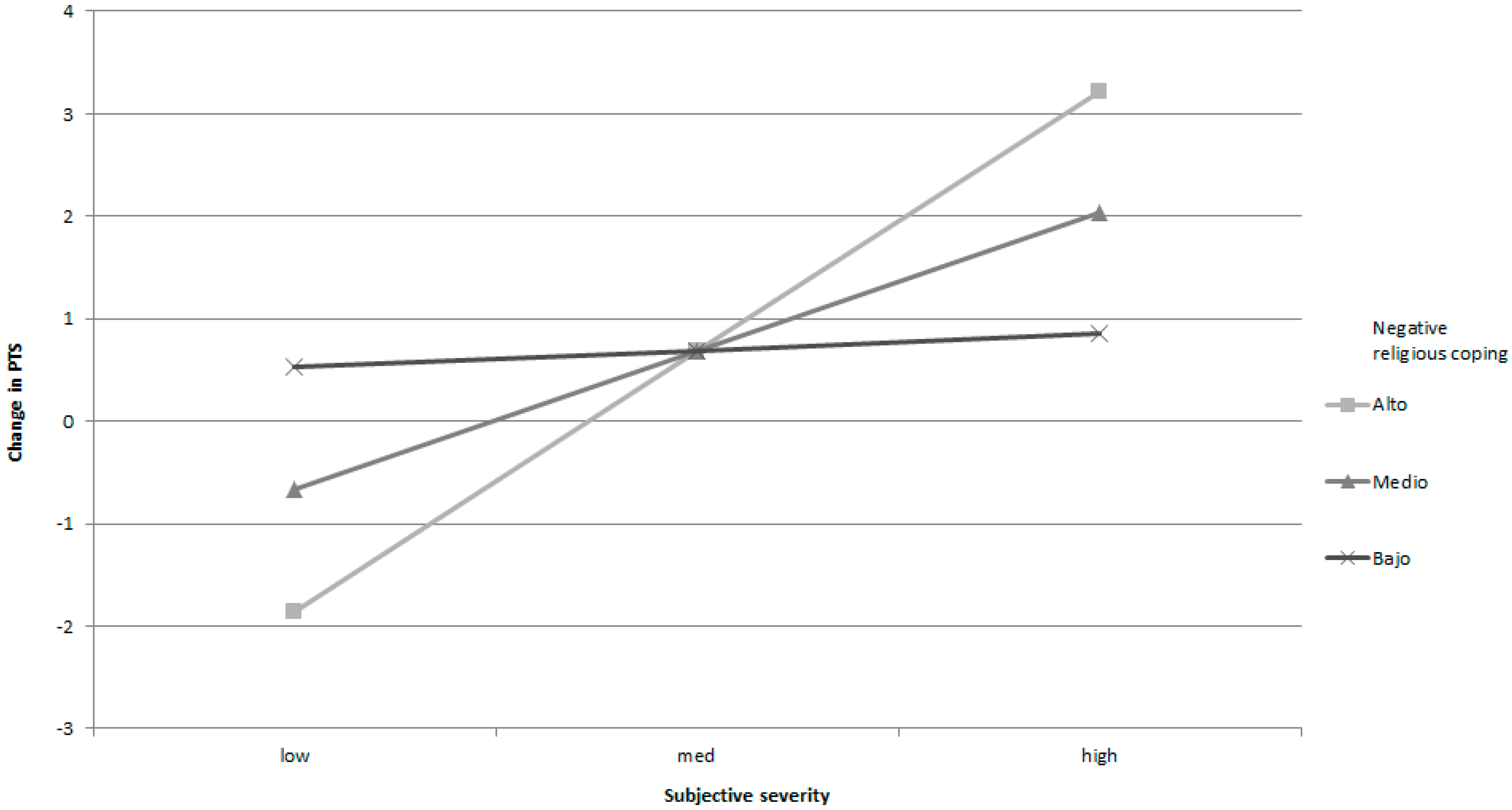
The significant interaction of negative RC and subjective severity implied the possibility of an effect of negative RC moderating the relationship between subjective severity and change in PTS. Regarding conditional effects in
Table 6, the middle and high values of negative RC generated an increase of PTS for high values of subjective severity, while this does not occur when negative RC is low (see
Figure 2). When negative RC is high or moderate, the severity of PTS is higher.
We also performed regressions to evaluate PTG and PTS predictors at T2, controlling the influence of PTG and PTS at T1, finding similar results but with a lower effect size (data not shown).
4. Discussion
Results globally confirm the hypothesized associations between variables: subjective severity and negative RC affect changes to PTS more frequently, and in turn, social support and positive RC affect the changes in PTG. The positive relationship between subject severity of event and PTS had been observed in other studies [
27]. While subjective severity and PTS have shown a direct relationship in studies about natural disasters [
29], in this study they were not related, probably because of the more heterogeneous character of the traumatic events included.
The association of coping by social support on the increase in PTG can be explained because support networks provide conditions that favour attributing positive results to the experience [
5]. On the other hand, positive religious coping can be conceived of as a form of transcendent support, or the equivalent, having the support not of a human confident but of a suprahuman one or God. One of the aspects of PTG is to value receiving and giving social support; consequently, this form of support would nurture this aspect. We can also suppose that receiving support helps in discovering new opportunities, changing priorities and discovering personal strengths, another three facets of PTG [
3]. It is important to remark that analysis showed that high social support and positive RC, and also low negative RC, predicted PTG increase. These results are very important, because they offer longitudinal evidence about the effect of RC, which showed a specific influence controlling the coping from social support. This evidence supports the idea that religiosity helps growth beyond its function as a provider of social support networks [
21]. Also, correlations and regressions showed that positive RC was a stronger predictor of change in PTG than social support—although the role in undermining the increase of PTG by negative RC was even lower. The direct relationship and influence of positive RC with positive change in PTG corroborates the result of other studies [
8] and implies that positive RC would help to find a sense in life, providing a framework of meaning that helps to understand and accept the nature of stressing events and their consequences [
1]. This has led to RC being considered as a healthy psychological adaptation to stress [
46], providing additional benefits to other non-religious means of coping [
10].
The effect of negative RC on the increase of PTS indicates that seeing god or religion as punishing or distant [
31], questioning the goodness of god [
24], or having doubts about the existence of a god that protects good people from bad events [
47] also contributes to the increase of negative feelings associated with PTS. The predictive coefficient of RC was the lower of the three variables and its influence disappeared when severity was controlled.
Regarding the moderator role of positive RC in the relationship between social support and change in PTG, a low level of positive RC makes the relationship between social support and increase in PTG stronger. On the other hand, when positive RC is high, this relationship weakens. We must point out that a low level of positive RC is not the same as negative RC, but an absence of religiosity, possibly present in people of low spirituality or non-believers. In that sense, we can assume that the lack of religious coping strengthens the effect that high coping by social support gives to the increase on PTG. This result supplements the previous one and suggests that an aspect of religious coping implies obtaining social support [
23]. As previously discussed, positive religious coping can be conceived of a form of transcendence support and at high level erodes the importance of secular social support.
The moderating role of negative RC in the relationship between subjective severity and change in the PTS also was significant. In this case, we observed that subjective severity influenced the increase of PTS only when negative RC is medium or high. These results show that religiosity does serve a moderating role between predictive variables and psychological responses after stressing events, which has been found in other studies [
30,
32,
33], strengthening the negative impact of subjective severity when it is high. However, as Harris et al. [
15] suggested, severity and Time 1 PTS could predict negative RC and this form of coping could act as a mediational path between baseline traumatic reactions and Time 2 PTS. In fact, they found that a proxy of severity or distress and negative RC (religious strain or conflict over faith) predicted poorer mental health after stressful life events over time. In other terms, high severity and high PTS symptoms at the base line can increase negative religious coping and by this token reinforces indirectly traumatic symptoms and decreases mental health over time. This model process is not at odds with our results, and is valid as a complementary explanation.
This study has some limitations that need to be mentioned. Firstly, the possible presence of stressful events (or other type of events that could have emerged during the period between measures) could have caused an effect over PTS and PTG that was not controlled. Secondly, the heterogeneous nature of the events to which these people were exposed is also a limitation and low degrees of freedom preclude an analysis by type of event. However, heterogeneity could also be a strength, because it represents the diversity of stressful events in the general population. On the other hand, we suppose that these results could vary in more specific samples, and we recommend continuing investigating these relationships in people exposed to more delimited stressful events. Thirdly, we do not inquire about the identification or participation of people towards a specific religious belief or whether they are agnostic or other spiritual beliefs, which prevented us from doing an analysis controlling this variable. Fourthly, participants reported events experienced up until four years ago, but probably a more precise baseline and follow up are needed to obtain more valid conclusions. Finally, this is a longitudinal study with only two measures, so more measures are necessary to establish the course of changes in PTS and PTG which could be non-linear and could suffer changes through time.



{kind=link}
{kind=link}