Effect of Baricitinib and Adalimumab in Reducing Pain and Improving Function in Patients with Rheumatoid Arthritis in Low Disease Activity: Exploratory Analyses from RA-BEAM

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. RA-BEAM Study Design
2.2. Outcomes Relevant to the Post-Hoc Analyses
2.3. Statistical Analysis
3. Results
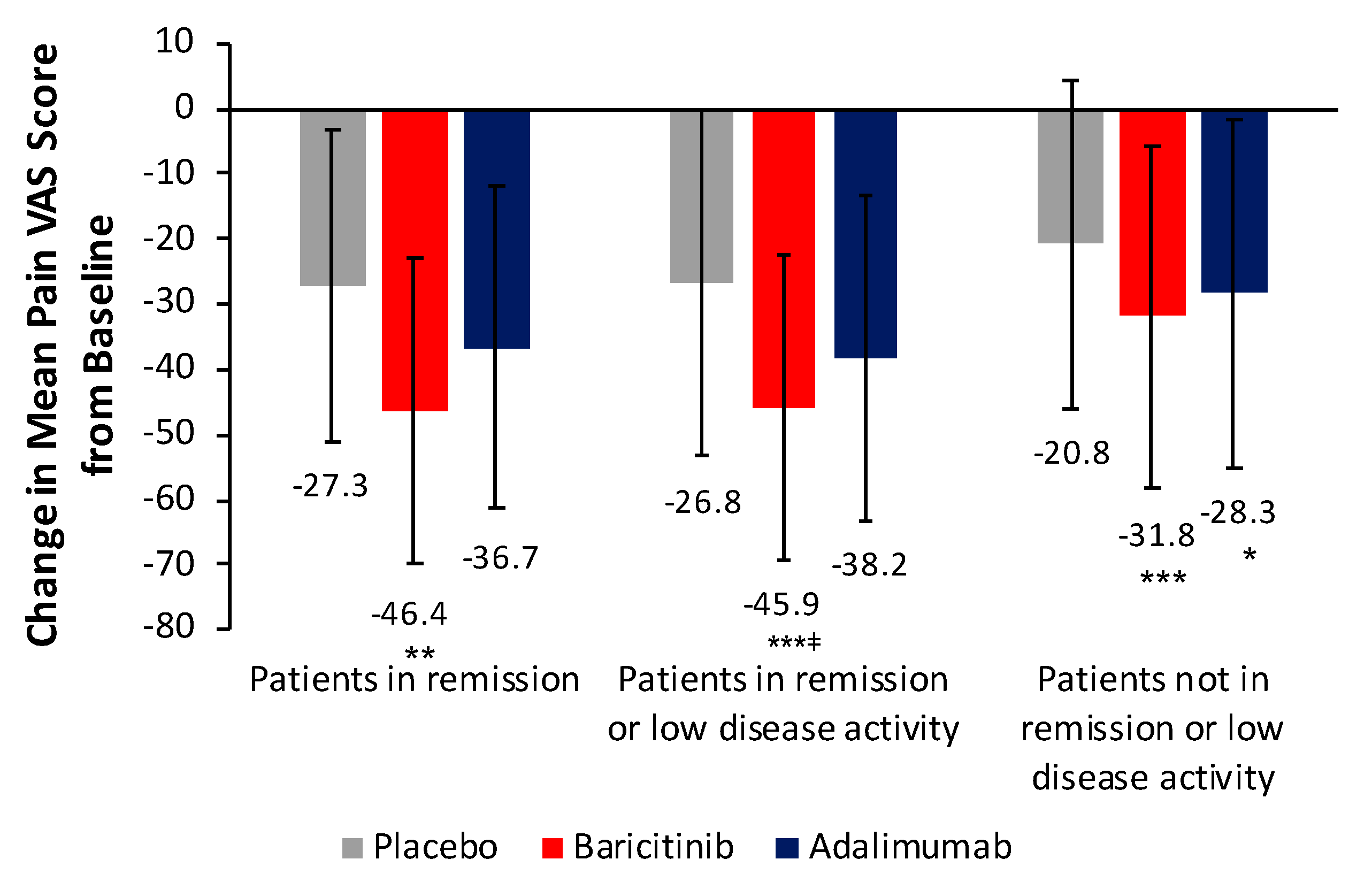
3.1. Change in Pain VAS Scores
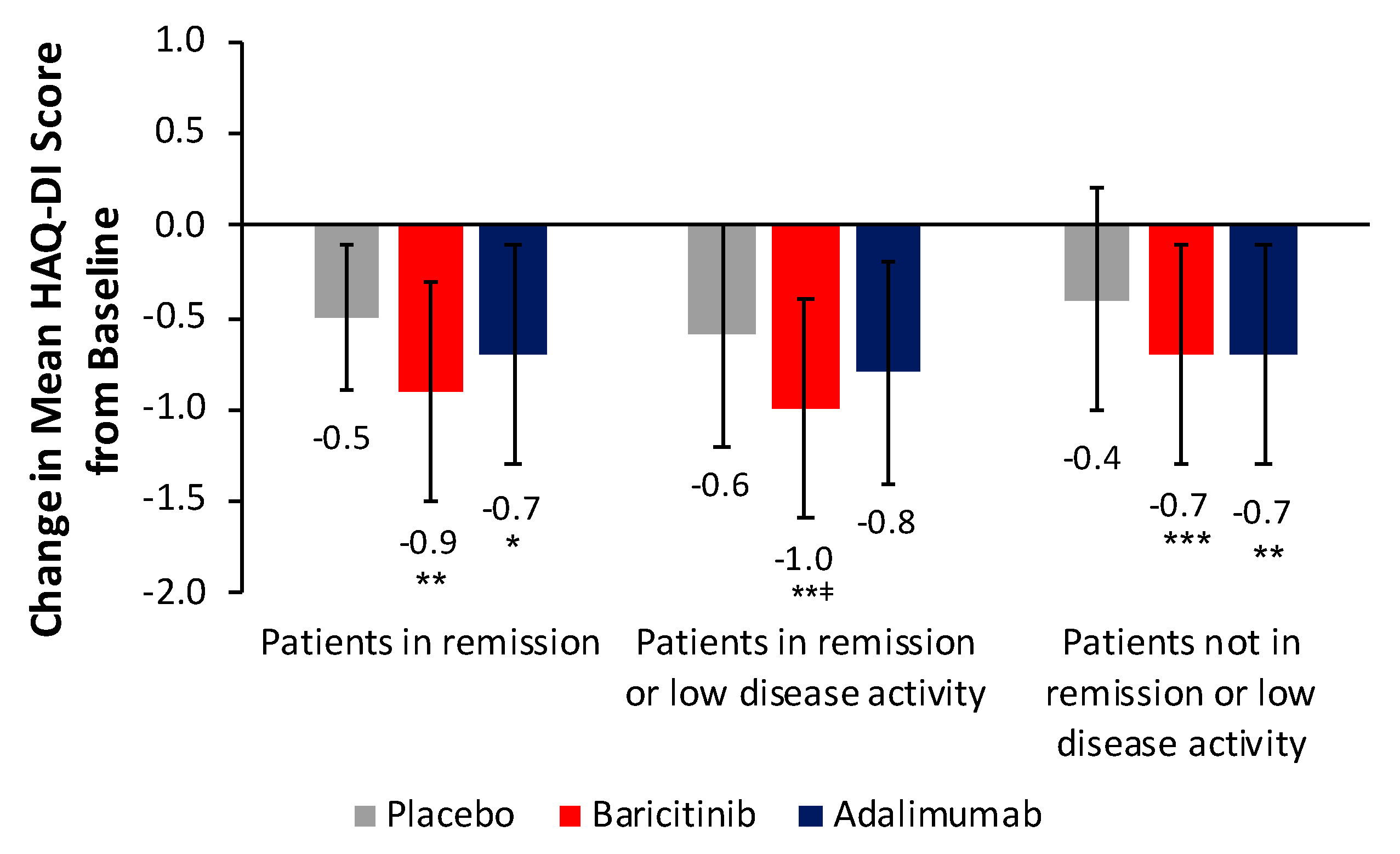
3.2. Change in HAQ-DI Scores
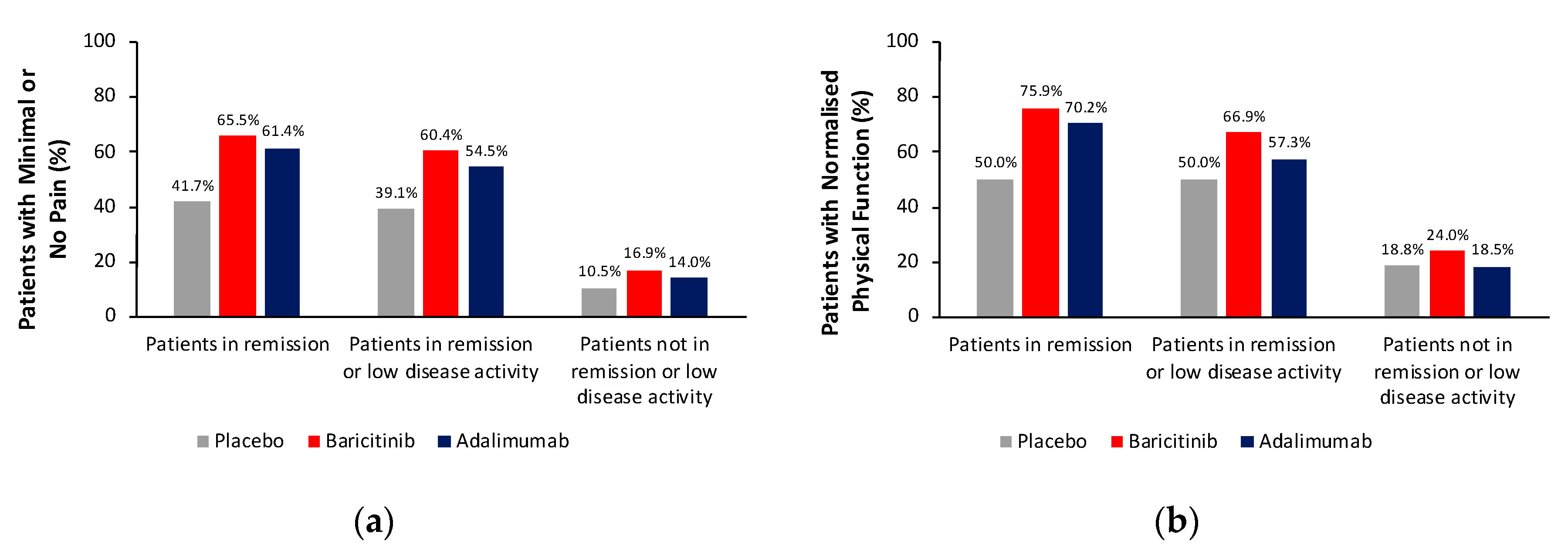
3.3. Proportion of Patients Achieving Minimal or No Pain and Proportion Achieving Normalisation of Physical Function
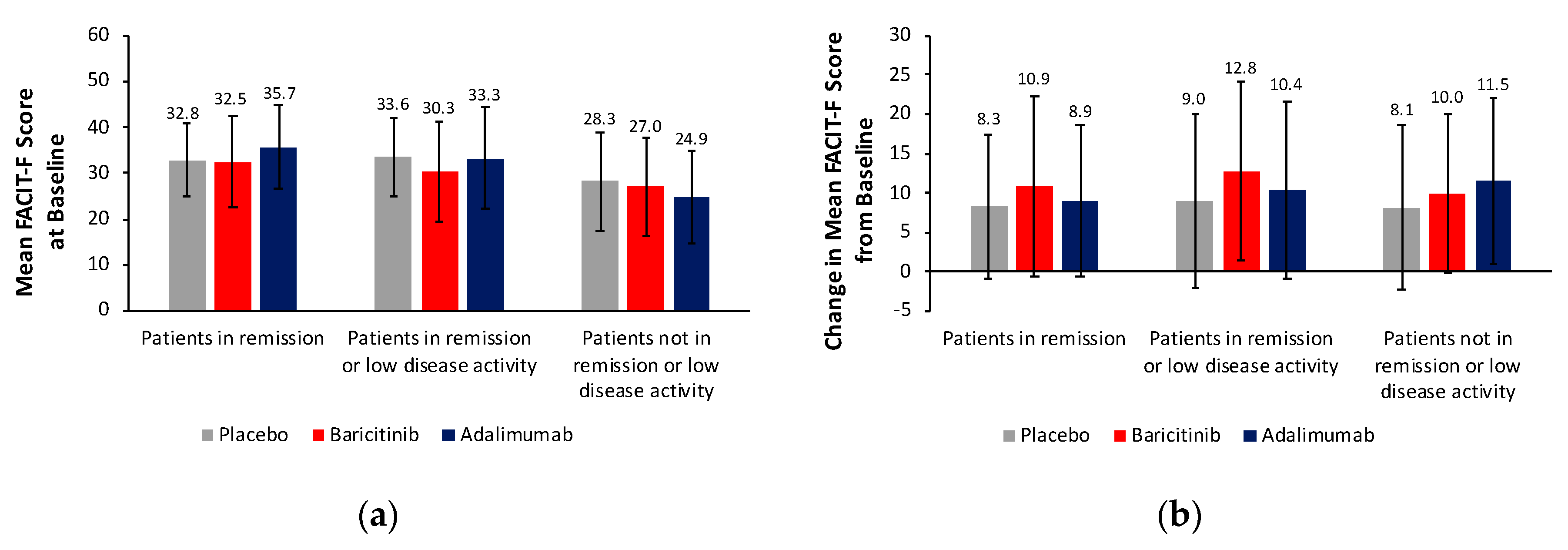
3.4. Changes in Other Patient-Reported Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Singh, J.A.; Saag, K.G.; Bridges, S.L., Jr.; Akl, E.A.; Bannuru, R.R.; Sullivan, M.C.; Vaysbrot, E.; McNaughton, C.; Osani, M.; Shmerling, R.H.; et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016, 68, 1–26. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewé, R.; Bijlsma, J.; Burmester, G.; Chatzidionysiou, K.; Dougados, M.; Nam, J.; Ramiro, S.; Voshaar, M.; Van Vollenhoven, R.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann. Rheum. Dis. 2017, 76, 960–977. [Google Scholar] [CrossRef]
- Nieuwenhuis, W.P.; De Wit, M.P.; Boonen, A.; Van Der Helm-Van Mil, A.H. Changes in the clinical presentation of patients with rheumatoid arthritis from the early 1990s to the years 2010: Earlier identification but more severe patient reported outcomes. Ann. Rheum. Dis. 2016, 75, 2054–2056. [Google Scholar] [CrossRef]
- Ishiguro, N.; Dougados, M.; Cai, Z.; Zhu, B.; Ishida, M.; Sato, M.; Gaich, C.; Quebe, A.; Stoykov, I.; Tanaka, Y. Relationship between disease activity and patient-reported outcomes in rheumatoid arthritis: Post hoc analyses of overall and Japanese results from two phase 3 clinical trials. Mod. Rheumatol. 2018, 28, 950–959. [Google Scholar] [CrossRef]
- Taylor, P.C.; Moore, A.; Vasilescu, R.; Alvir, J.; Tarallo, M. A structured literature review of the burden of illness and unmet needs in patients with rheumatoid arthritis: A current perspective. Rheumatol. Int. 2016, 36, 685–695. [Google Scholar] [CrossRef]
- Gossec, L.; Dougados, M.; Rincheval, N.; Balanescu, A.; Boumpas, D.T.; Canadelo, S.; Carmona, L.; Daurès, J.P.; de Wit, M.; Dijkmans, B.A.; et al. Elaboration of the preliminary Rheumatoid Arthritis Impact of Disease (RAID) score: A EULAR initiative. Ann. Rheum. Dis. 2009, 68, 1680–1685. [Google Scholar] [CrossRef]
- Khan, N.A.; Spencer, H.J.; Abda, E.; Aggarwal, A.; Alten, R.; Ancuta, C.; Andersone, D.; Bergman, M.; Craig-Muller, J.; Detert, J.; et al. Determinants of discordance in patients’ and physicians’ rating of rheumatoid arthritis disease activity. Arthritis Care Res. 2012, 64, 206–214. [Google Scholar] [CrossRef]
- Wen, H.; Ralph Schumacher, H.; Li, X.; Gu, J.; Ma, L.; Wei, H.; Yokogawa, N.; Shiroto, K.; Baker, J.F.; Dinnella, J.; et al. Comparison of expectations of physicians and patients with rheumatoid arthritis for rheumatology clinic visits: A pilot, multicenter, international study. Int. J. Rheum. Dis. 2012, 15, 380–389. [Google Scholar] [CrossRef]
- Van Tuyl, L.H.; Sadlonova, M.; Hewlett, S.; Davis, B.; Flurey, C.; Goel, N.; Gossec, L.; Brahe, C.H.; Hill, C.L.; Hoogland, W.; et al. The patient perspective on absence of disease activity in rheumatoid arthritis: A survey to identify key domains of patient-perceived remission. Ann. Rheum. Dis. 2017, 76, 855–861. [Google Scholar] [CrossRef]
- Fautrel, B.; Alten, R.; Kirkham, B.; De La Torre, I.; Durand, F.; Barry, J.; Holzkaemper, T.; Fakhouri WTaylor, P.C. Call for action: How to improve use of patient-reported outcomes to guide clinical decision making in rheumatoid arthritis. Rheumatol. Int. 2018, 38, 935–947. [Google Scholar] [CrossRef]
- Fridman, J.S.; Scherle, P.A.; Collins, R.; Burn, T.C.; Li, Y.; Li, J.; Covington, M.B.; Thomas, B.; Collier, P.; Favata, M.F.; et al. Selective inhibition of JAK1 and JAK2 is efficacious in rodent models of arthritis: Preclinical characterization of INCB028050. J. Immunol. 2010, 184, 5298–5307. [Google Scholar] [CrossRef]
- O’Shea, J.J.; Kontzias, A.; Yamaoka, K.; Tanaka, Y.; Laurence, A. Janus kinase inhibitors in autoimmune diseases. Ann. Rheum. Dis. 2013, 72, ii111–ii115. [Google Scholar] [CrossRef]
- Choy, E.H.S.; Miceli-Richard, C.; González-Gay, M.A.; Sinigaglia, L.; Schlichting, D.E.; Meszaros, G.; de la Torre, I.; Schulze-Koops, H. The effect of JAK/JAK2 inhibition in rheumatoid arthritis: Efficacy and safety of baricitinib. RMD Open 2019, 5, e000798. [Google Scholar] [CrossRef]
- European Medicines Agency. Olumiant 2 mg and 4 mg Film-Coated Tablets. Summary of Product Characteristics. 2018. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/004085/WC500223723.pdf (accessed on 11 April 2018).
- Food and Drug Administration. Olumiant (Baricitinib) Tablets, for Oral Use. Prescribing Information; 2018. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/207924s000lbl.pdf (accessed on 21 June 2018).
- Pharmaceutical and Medical Devices Agency. Report on the Deliberation Results. Olumiant Tablets 2 mg, Olumiant Tablets 4 mg. 2017. Available online: http://www.pmda.go.jp/files/000226301.pdf (accessed on 21 June 2018).
- Genovese, M.C.; Kremer, J.; Zamani, O.; Ludivico, C.; Krogulec, M.; Xie, L.; Beattie, S.D.; Koch, A.E.; Cardillo, T.E.; Rooney, T.P.; et al. Baricitinib in patients with refractory rheumatoid arthritis. N. Engl. J. Med. 2016, 374, 1243–1252. [Google Scholar] [CrossRef]
- Dougados, M.; van der Heijde, D.; Chen, Y.C.; Greenwald, M.; Drescher, E.; Liu, J.; Beattie, S.; Witt, S.; de la Torre, I.; Gaich CRooney, T. Baricitinib in patients with inadequate response or intolerance to conventional synthetic DMARDs: Results from the RA-BUILD study. Ann. Rheum. Dis. 2017, 76, 88–95. [Google Scholar] [CrossRef]
- Fleischmann, R.; Schiff, M.; van der Heijde, D.; Ramos-Remus, C.; Spindler, A.; Stanislav, M.; Zerbini, C.A.; Gurbuz, S.; Dickson, C.; de Bono, S.; et al. Baricitinib, methotrexate, or combination in patients with rheumatoid arthritis and no or limited prior disease-modifying antirheumatic drug treatment. Arthritis Rheumatol. 2017, 69, 506–517. [Google Scholar] [CrossRef]
- Taylor, P.C.; Keystone, E.C.; van der Heijde, D.; Weinblatt, M.E.; del Carmen Morales, L.; Reyes Gonzaga, J.; Yakushin, S.; Ishii, T.; Emoto, K.; Beattie, S.; et al. Baricitinib versus placebo or adalimumab in rheumatoid arthritis. N. Engl. J. Med. 2017, 376, 652–662. [Google Scholar] [CrossRef]
- Fries, J.F.; Spitz, P.W.; Young, D.Y. The dimensions of health outcomes: The health assessment questionnaire, disability and pain scales. J. Rheumatol. 1982, 9, 789–793. [Google Scholar]
- Cella, D.; Yount, S.; Sorensen, M.; Chartash, E.; Sengupta, N.; Grober, J. Validation of the Functional Assessment of Chronic Illness Therapy Fatigue Scale relative to other instrumentation in patients with rheumatoid arthritis. J. Rheumatol. 2005, 32, 811–819. [Google Scholar]
- Reilly, M.C.; Zbrozek, A.S.; Dukes, E.M. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics 1993, 4, 353–365. [Google Scholar] [CrossRef]
- Ishida, M.; Kuroiwa, Y.; Yoshida, E.; Sato, M.; Krupa, D.; Henry, N.; Ikeda, K.; Kaneko, Y. Residual symptoms and disease burden among patients with rheumatoid arthritis in remission or low disease activity: A systematic literature review. Mod. Rheumatol. 2018, 28, 789–799. [Google Scholar] [CrossRef]
- Taylor, P.; Manger, B.; Alvaro-Gracia, J.; Johnstone, R.; Gomez-Reino, J.; Eberhardt, E.; Wolfe, F.; Schwartzman, S.; Furfaro, N.; Kavanaugh, A. Patient perceptions concerning pain management in the treatment of rheumatoid arthritis. J. Int. Med. Res. 2010, 38, 1213–1224. [Google Scholar] [CrossRef]
- Walsh, D.A.; Mcwilliams, D.F. Mechanisms, impact and management of pain in rheumatoid arthritis. Nat. Rev. Rheumatol. 2014, 10, 581–592. [Google Scholar] [CrossRef]
- Boyden, S.D.; Hossain, I.N.; Wohlfahrt, A.; Lee, Y.C. Non-inflammatory causes of pain in patients with rheumatoid arthritis. Curr. Rheumatol. Rep. 2016, 18, 30. [Google Scholar] [CrossRef]
- Taylor, P.C.; Lee, Y.C.; Fleischmann, R.; Takeuchi, T.; Perkins, E.L.; Fautrel, B.; Zhu, B.; Quebe, A.K.; Gaich, C.L.; Zhang, X.; et al. Achieving pain control in rheumatoid arthritis with baricitinib or adalimumab plus methotrexate: Results from the RA-BEAM trial. J. Clin. Med. 2019, 8, 831. [Google Scholar] [CrossRef]
- Cook, A.D.; Pobjoy, J.; Steidl, S.; Dürr, M.; Braine, E.L.; Turner, A.L.; Lacey, D.C.; Hamilton, J.A. Granulocyte-macrophage colony-stimulating factor is a key mediator in experimental osteoarthritis pain and disease development. Arthritis Res. Ther. 2012, 14, R199. [Google Scholar] [CrossRef]
- Dominguez, E.; Rivat, C.; Pommier, B.; Mauborgne, A.; Pohl, M. JAK/STAT3 pathway is activated in spinal cord microglia after peripheral nerve injury and contributes to neuropathic pain development in rat. J. Neurochem. 2008, 107, 50–60. [Google Scholar] [CrossRef]
- Capron, J.; De Leonardis, F.; Fakhouri, W.; Burke, T.; Rose, A.; Jacob, I. The impact of rheumatoid arthritis (RA) on a patient’s ability to stay in work and level of pain experienced. Value Health 2017, 20, A531–A532. [Google Scholar] [CrossRef]
- Malm, K.; Bergman, S.; Andersson, M.; Bremander, A.; BARFOT Study Group. Predictors of severe self-reported disability in RA in a long-term follow-up study. Disabil. Rehabil. 2015, 37, 686–691. [Google Scholar] [CrossRef]
- Hodkinson, B.; Musenge, E.; Ally, M.; Meyer, P.W.; Anderson, R.; Tikly, M. Functional disability and health-related quality of life in South Africans with early rheumatoid arthritis. Scand. J. Rheumatol. 2012, 41, 366–374. [Google Scholar] [CrossRef]
- Manders, S.H.; Kievit, W.; Braakman-Jansen, A.L.; Brus, H.L.; Hendriks, L.; Fransen, J.; van de Laar, M.A.; van Riel, P.L. Determinants associated with work participation in patients with established rheumatoid arthritis taking tumor necrosis factor inhibitors. J. Rheumatol. 2014, 41, 1263–1269. [Google Scholar] [CrossRef]
- Kobelt, G.; Woronoff, A.S.; Richard, B.; Peeters, P.; Sany, J. Disease status, costs and quality of life of patients with rheumatoid arthritis in France: The ECO-PR study. Jt. Bone Spine 2008, 75, 408–415. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment ¥ | BARI 4 mg | ADA 40 mg Q2W | Placebo |
|---|---|---|---|
| n | 487 | 330 | 488 |
| Remission rates (%) | |||
| DAS28-ESR <2.6 | 18 *** | 18 *** | 5 |
| DAS28-hsCRP <2.6 | 34 *** | 32 *** | 8 |
| SDAI ≤3.3 | 16 *** | 14 *** | 3 |
| CDAI ≤2.8 | 16 *** | 12 *** | 4 |
| Remission or low disease activity rates (%) | |||
| DAS28-ESR ≤3.2 | 32 *** | 34 *** | 10 |
| DAS28-hsCRP ≤3.2 | 52 *** | 48 *** | 19 |
| DAS28-ESR ≥2.6 and ≤3.2 | 14 | 16 | 5 |
| DAS28-hsCRP ≥2.6 and ≤3.2 | 18 | 16 | 11 |
| SDAI >3.3 and ≤11 | 35 | 34 | 17 |
| CDAI >2.8 and ≤10 | 34 | 36 | 16 |
| Characteristic | All Randomised and Treated Patients (N = 1305) | Patients in Remission at Week 24 (N = 168) | ||||
|---|---|---|---|---|---|---|
| Placebo (N = 488) | Baricitinib 4 mg (N = 487) | Adalimumab (N = 330) | Placebo (N = 24) | Baricitinib 4 mg (N = 87) | Adalimumab (N = 57) | |
| Age (years) | 53 ± 12 | 54 ± 12 | 53 ± 12 | 52 ± 12 | 52 ± 13 | 53 ± 13 |
| Female | 382 (78) | 375 (77) | 251 (76) | 15 (63) | 62 (71) | 41 (72) |
| Time from symptom onset (years) | 10.4 ± 9 | 10.3 ± 9 | 9.6 ± 9 | 9.1 ± 6 | 8.9 ± 9 | 8.1 ± 8 |
| ACPA positive | 424 (87) | 427 (88) | 295 (89) | 22 (92) | 75 (86) | 52 (91) |
| RF positive | 451 (92) | 439 (90) | 301 (91) | 22 (92) | 76 (87) | 49 (86) |
| ≥3 erosions | 371 (76) | 371 (76) | 245 (75) | 17 (71) | 66 (77) | 41 (75) |
| mTSS total score | 45 ± 50 | 43 ± 50 | 44 ± 51 | 36 ± 41 | 39 ± 43 | 37 ± 42 |
| Erosion score | 26.8 ± 29 | 25.1 ± 28 | 26.4 ± 29 | 22.5 ± 24 | 24.4 ± 26 | 22.7 ± 23 |
| Joint space narrowing score | 18.2 ± 23 | 17.3 ± 23 | 18.0 ± 24 | 13.1 ± 18 | 14.6 ± 19 | 14.7 ± 20 |
| Concomitant corticosteroid use | 290 (59) | 275 (56) | 201 (61) | 13 (54) | 50 (58) | 39 (68) |
| Type of csDMARD currently used | ||||||
| MTX only | 398 (82) | 413 (85) | 277 (84) | 20 (83) | 71 (82) | 49 (86) |
| MTX + other csDMARD | 89 (18) | 74 (15) | 53 (16) | 4 (17) | 16 (18) | 8 (14) |
| MTX weekly dose in mg | 15 ± 5 | 15 ± 5 | 15 ± 4 | 15 ± 4 | 14 ± 5 | 14 ± 5 |
| DAS28-hsCRP | 5.7 ± 1.0 | 5.8 ± 0.9 | 5.8 ± 0.9 | 5.0 ± 0.8 | 5.3 ± 1.0 | 5.2 ± 0.9 |
| DAS28-ESR | 6.4 ± 1.0 | 6.5 ± 0.9 | 6.4 ± 1.0 | 5.4 ± 0.8 | 5.9 ± 1.0 | 5.8 ± 0.9 |
| CDAI score | 38 ± 13 | 38 ± 12 | 38 ± 13 | 30 ± 10 | 33 ± 12 | 32 ± 12 |
| Pain VAS score (0–100 mm) ¥ | 60 ± 23 | 62 ± 22 | 61 ± 23 | 44 ± 21 | 57 ± 23 | 48 ± 23 |
| HAQ-DI ¶ | 1.6 ± 0.7 | 1.6 ± 0.7 | 1.6 ± 0.7 | 1.1 ± 0.5 | 1.3 ± 0.6 | 1.1 ± 0.7 |
| FACIT-F $ | 28.6 ± 10.7 | 28.1 ± 10.7 | 27.6 ± 11.4 | 32.8 ± 7.9 | 32.5 ± 10.0 | 35.7 ± 9.1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fautrel, B.; Kirkham, B.; Pope, J.E.; Takeuchi, T.; Gaich, C.; Quebe, A.; Zhu, B.; de la Torre, I.; De Leonardis, F.; Taylor, P.C. Effect of Baricitinib and Adalimumab in Reducing Pain and Improving Function in Patients with Rheumatoid Arthritis in Low Disease Activity: Exploratory Analyses from RA-BEAM. J. Clin. Med. 2019, 8, 1394. https://doi.org/10.3390/jcm8091394
Fautrel B, Kirkham B, Pope JE, Takeuchi T, Gaich C, Quebe A, Zhu B, de la Torre I, De Leonardis F, Taylor PC. Effect of Baricitinib and Adalimumab in Reducing Pain and Improving Function in Patients with Rheumatoid Arthritis in Low Disease Activity: Exploratory Analyses from RA-BEAM. Journal of Clinical Medicine. 2019; 8(9):1394. https://doi.org/10.3390/jcm8091394
Chicago/Turabian StyleFautrel, Bruno, Bruce Kirkham, Janet E. Pope, Tsutomu Takeuchi, Carol Gaich, Amanda Quebe, Baojin Zhu, Inmaculada de la Torre, Francesco De Leonardis, and Peter C. Taylor. 2019. "Effect of Baricitinib and Adalimumab in Reducing Pain and Improving Function in Patients with Rheumatoid Arthritis in Low Disease Activity: Exploratory Analyses from RA-BEAM" Journal of Clinical Medicine 8, no. 9: 1394. https://doi.org/10.3390/jcm8091394
APA StyleFautrel, B., Kirkham, B., Pope, J. E., Takeuchi, T., Gaich, C., Quebe, A., Zhu, B., de la Torre, I., De Leonardis, F., & Taylor, P. C. (2019). Effect of Baricitinib and Adalimumab in Reducing Pain and Improving Function in Patients with Rheumatoid Arthritis in Low Disease Activity: Exploratory Analyses from RA-BEAM. Journal of Clinical Medicine, 8(9), 1394. https://doi.org/10.3390/jcm8091394