Significant Correlation Between Grip Strength and m2bpgi in Patients with Chronic Liver Diseases

Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Statistical Considerations
3. Results
3.1. Baseline Characteristics
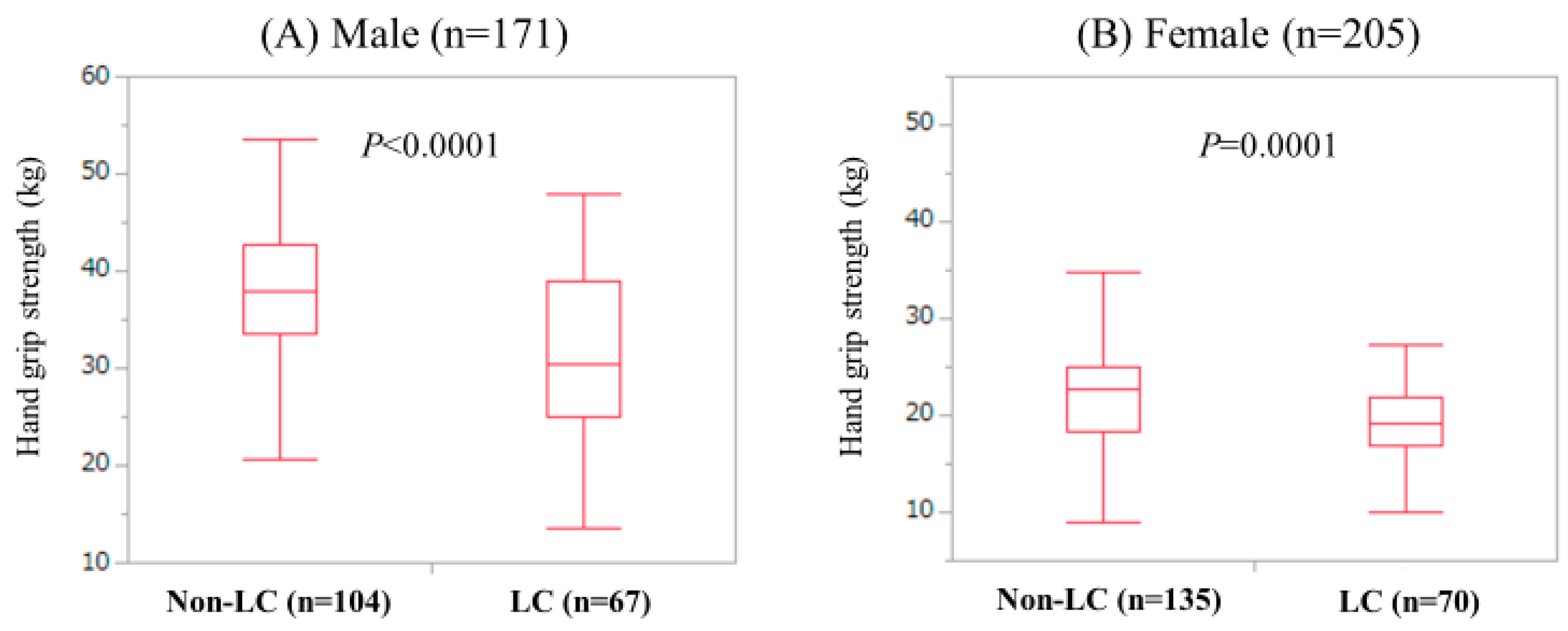
3.2. Gs According to the LC Status in Male and Female
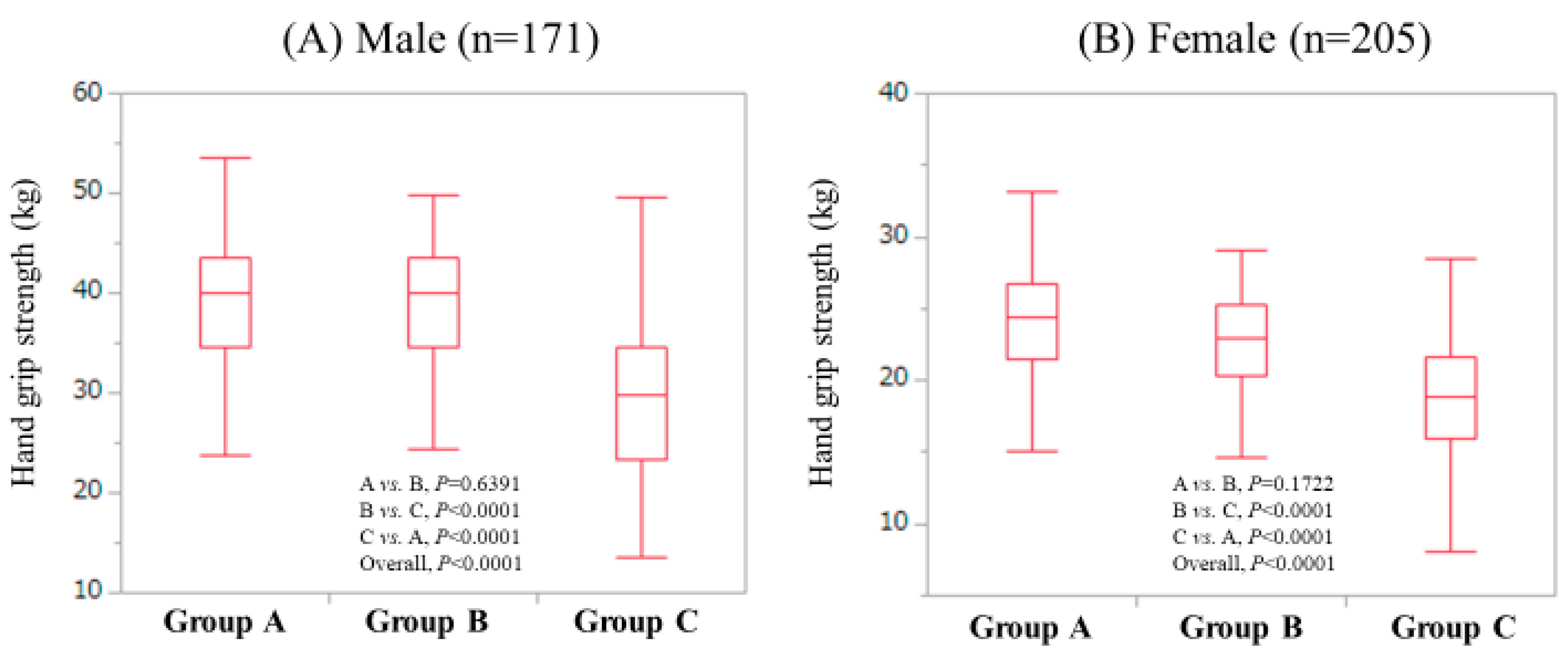
3.3. GS According to Age in Male and Female
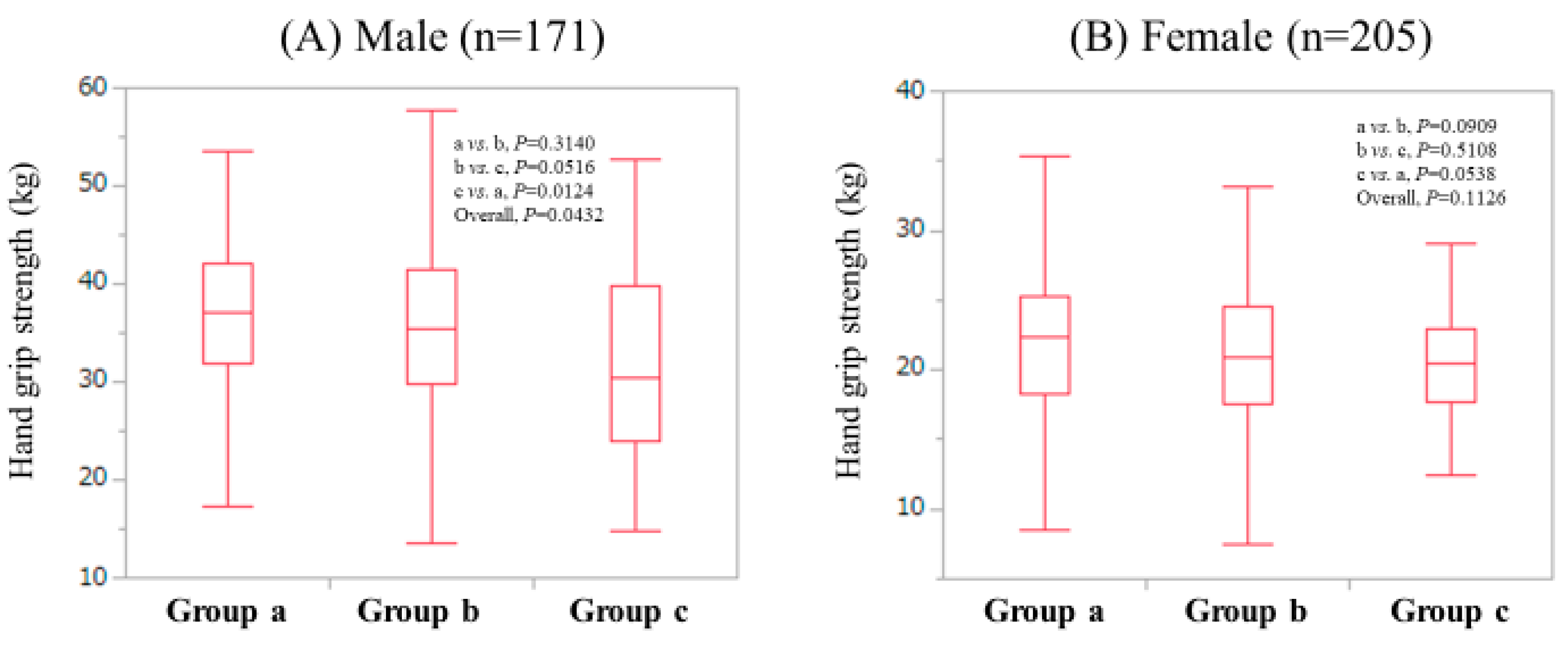
3.4. GS According to Body Mass Index (BMI) in Male and Female
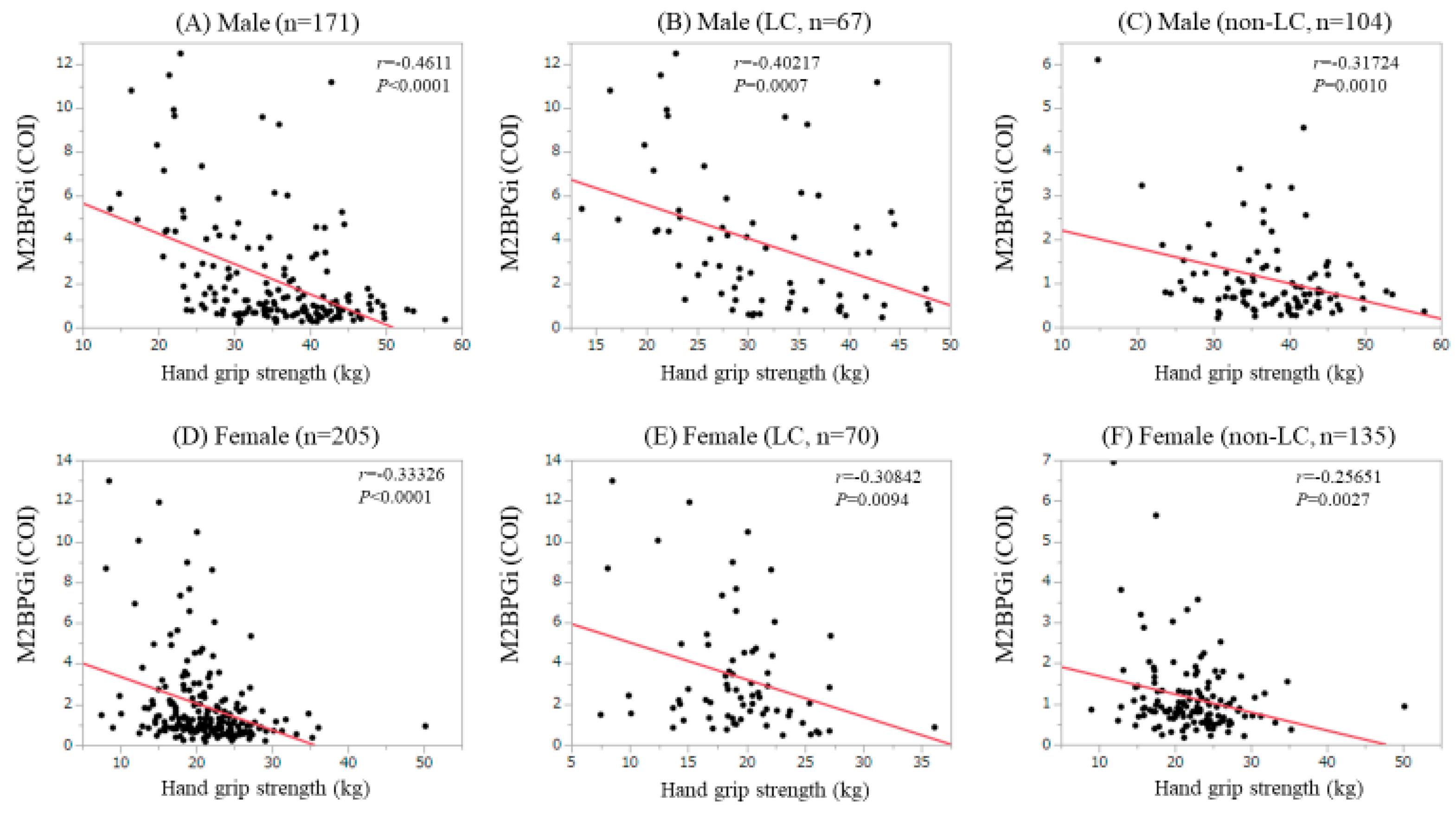
3.5. Correlation Between GS and m2bpgi in Male and Female
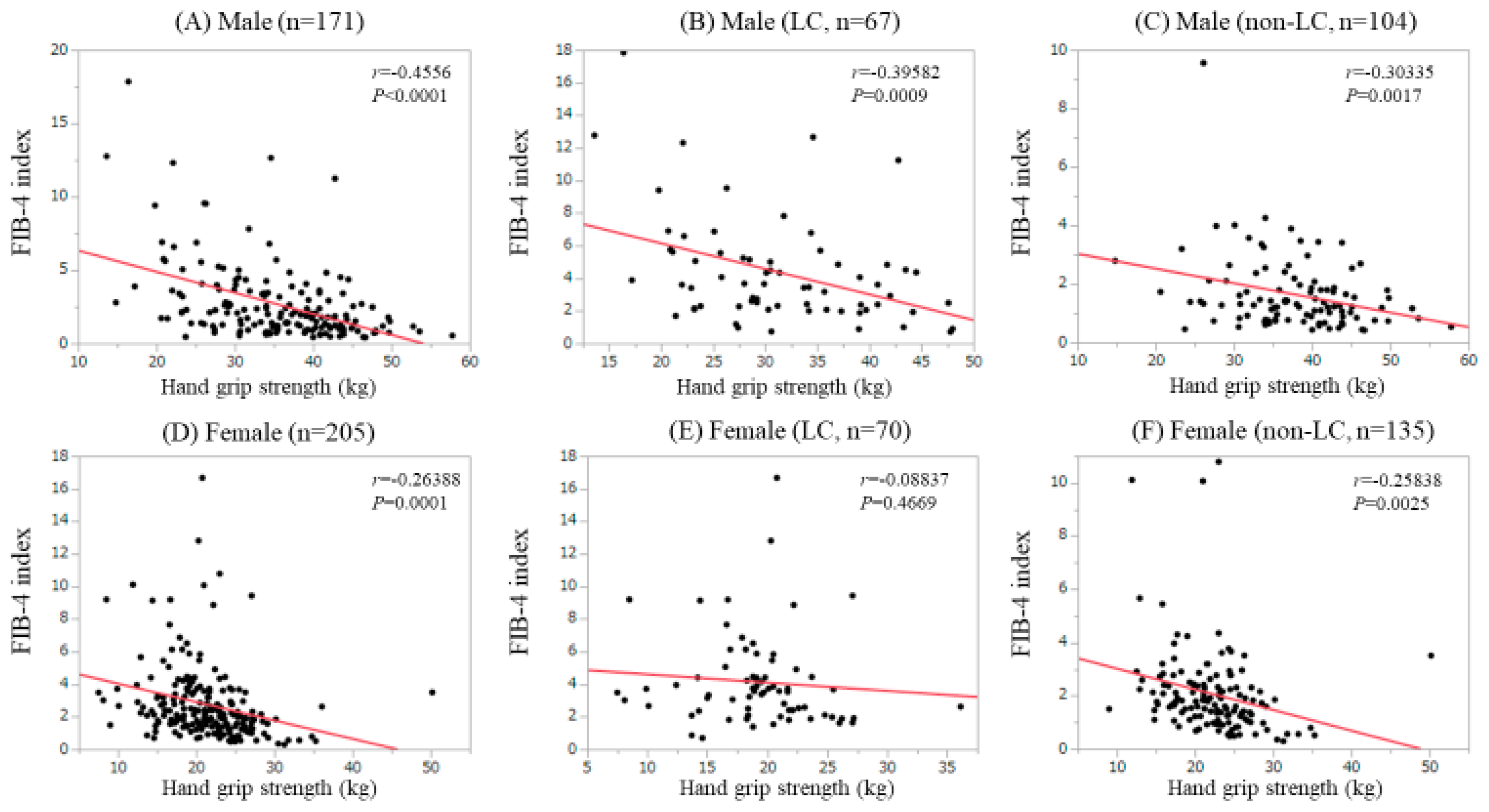
3.6. Correlation Between GS and Fib-4 Index in Male and Female
3.7. Uni- and Multivariate Analyses of Factors Linked to Low GS in Male Patients
3.8. Uni- and Multivariate Analyses of Factors Lnked to Low GS in Female Patients
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ekerfors, U.; Sunnerhagen, K.S.; Westin, J.; Jakobsson, U.E.; Marschall, H.U.; Josefsson, A.; Simrén, M. Muscle performance and fatigue in compensated chronic liver disease. Scand. J. Gastroenterol. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nagamatsu, A.; Kawaguchi, T.; Hirota, K.; Koya, S.; Tomita, M.; Hashida, R.; Kita, Y.; Narao, H.; Manako, Y.; Tanaka, D.; et al. Slow Walking Speed Overlapped with Low Hand Grip Strength in Chronic Liver Disease Patients with Hepatocellular Carcinoma. Hepatol. Res. 2019, 4. [Google Scholar] [CrossRef]
- Kulkarni, S.; Chen, H.; Josbeno, D.; Schmotzer, A.; Hughes, C.; Humar, A.; Sood, P.; Rachakonda, V.; Dunn, M.; Tevar, A. Gait Speed and Grip Strength Are Associated With Dropping Out of the Liver Transplant Waiting List. Transplant. Proc. 2019, 51, 794–797. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Health-Related Quality of Life in Chronic Liver Diseases: A Strong Impact of Hand Grip Strength. J. Clin. Med. 2018, 7, 553. [Google Scholar] [CrossRef]
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Effect of Sarcopenia on Sleep Disturbance in Patients with Chronic Liver Diseases. J. Clin. Med. 2018, 8, 16. [Google Scholar] [CrossRef]
- Kim, B.-J.; Ahn, S.H.; Lee, S.H.; Hong, S.; Hamrick, M.W.; Isales, C.M.; Koh, J.-M. Lower hand grip strength in older adults with non-alcoholic fatty liver disease: A nationwide population-based study. Aging 2019, 11, 4547–4560. [Google Scholar] [CrossRef]
- Gan, D.; Wang, L.; Jia, M.; Ru, Y.; Ma, Y.; Zheng, W.; Zhao, X.; Yang, F.; Wang, T.; Mu, Y.; et al. Low muscle mass and low muscle strength associate with nonalcoholic fatty liver disease. Clin. Nutr. 2019, 25, pii: S0261-5614(19)30199-2. [Google Scholar] [CrossRef]
- Lee, I.; Cho, J.; Park, J.; Kang, H. Association of hand-grip strength and non-alcoholic fatty liver disease index in older adults. J. Exerc. Nutr. Biochem. 2018, 22, 62–68. [Google Scholar] [CrossRef]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar]
- Fujiyoshi, M.; The Hepatitis Glyco-biomarker Study Group; Kuno, A.; Gotoh, M.; Fukai, M.; Yokoo, H.; Kamachi, H.; Kamiyama, T.; Korenaga, M.; Mizokami, M.; et al. Clinicopathological characteristics and diagnostic performance of Wisteria floribunda agglutinin positive Mac-2-binding protein as a preoperative serum marker of liver fibrosis in hepatocellular carcinoma. J. Gastroenterol. 2015, 50, 1134–1144. [Google Scholar]
- Toshima, T.; Shirabe, K.; Ikegami, T.; Yoshizumi, T.; Kuno, A.; Togayachi, A.; Gotoh, M.; Narimatsu, H.; Korenaga, M.; Mizokami, M.; et al. A novel serum marker, glycosylated Wisteria floribunda agglutinin-positive Mac-2 binding protein (WFA(+)-M2BP), for assessing liver fibrosis. J. Gastroenterol. 2015, 50, 76–84. [Google Scholar] [CrossRef]
- Yamasaki, K.; Tateyama, M.; Abiru, S.; Komori, A.; Nagaoka, S.; Saeki, A.; Hashimoto, S.; Sasaki, R.; Bekki, S.; Kugiyama, Y.; et al. Elevated serum levels of Wisteria floribunda agglutinin-positive human Mac-2 binding protein predict the development of hepatocellular carcinoma in hepatitis C patients. Hepatology 2014, 60, 1563–1570. [Google Scholar] [CrossRef] [PubMed]
- Shirabe, K.; Bekki, Y.; Gantumur, D.; Araki, K.; Ishii, N.; Kuno, A.; Narimatsu, H.; Mizokami, M. Mac-2 binding protein glycan isomer (M2BPGi) is a new serum biomarker for assessing liver fibrosis: more than a biomarker of liver fibrosis. J. Gastroenterol. 2018, 53, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Narimatsu, H.; Sato, T. Wisteria floribunda agglutinin positive glycobiomarkers: a unique lectin as a serum biomarker probe in various diseases. Expert. Rev. Proteomics. 2018, 15, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, H.; Tada, T.; Yasuda, S.; Mizuno, K.; Ito, T.; Kumada, T. Dynamic Evaluation of Liver Fibrosis to Assess the Risk of Hepatocellular Carcinoma in Patients with Chronic Hepatitis C Who Achieved Sustained Virologic Response. Clin. Infect. Dis. 2019, 6, pii: ciz359. [Google Scholar] [CrossRef]
- Seko, Y.; Moriguchi, M.; Hara, T.; Kataoka, S.; Okuda, K.; Furuta, M.; Takemura, M.; Taketani, H.; Umemura, A.; Nishikawa, T.; et al. Presence of varices in patients after hepatitis C virus eradication predicts deterioration in the FIB-4 index. Hepatol. Res. 2019, 49, 473–478. [Google Scholar] [CrossRef]
- Cheng, P.-N.; Chiu, H.-C.; Chiu, Y.-C.; Chen, S.-C.; Chen, Y. Comparison of FIB-4 and transient elastography in evaluating liver fibrosis of chronic hepatitis C subjects in community. PLoS ONE 2018, 13, e0206947. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, N.; Higuchi, M.; Kurosaki, M.; Kirino, S.; Osawa, L.; Watakabe, K.; Wang, W.; Okada, M.; Shimizu, T.; Takaura, K.; et al. Wisteria floribunda agglutinin-positive mac-2 binding protein as an age-independent fibrosis marker in nonalcoholic fatty liver disease. Sci. Rep. 2019, 9, 10109. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Beste, L.A.; Green, P.K.; Singal, A.G.; Tapper, E.B.; Waljee, A.K.; Sterling, R.K.; Feld, J.J.; Kaplan, D.E.; Taddei, T.H.; et al. Increased Risk for Hepatocellular Carcinoma Persists Up to 10 Years After HCV Eradication in Patients with Baseline Cirrhosis or High FIB-4 Scores. Gastroenterology 2019, pii: S0016-5085(19)41130-X, [Epub ahead of print]. [Google Scholar] [CrossRef]
- Vilar-Gomez, E.; Chalasani, N. Non-invasive assessment of non-alcoholic fatty liver disease: Clinical prediction rules and blood-based biomarkers. J. Hepatol. 2018, 68, 305–315. [Google Scholar] [CrossRef]
- Houot, M.; Ngo, Y.; Munteanu, M.; Marque, S.; Poynard, T. Systematic review with meta-analysis: direct comparisons of biomarkers for the diagnosis of fibrosis in chronic hepatitis C and B. Aliment. Pharmacol. Ther. 2016, 43, 16–29. [Google Scholar] [CrossRef]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology guidelines for sarcopenia in liver disease: Recommendation from the working group for creation of sarcopenia assessment criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef]
- Fukui, H.; Saito, H.; Ueno, Y.; Uto, H.; Obara, K.; Sakaida, I.; Shibuya, A.; Seike, M.; Nagoshi, S.; Segawa, M.; et al. Evidence-based clinical practice guidelines for liver cirrhosis 2015. J. Gastroenterol. 2016, 51, 629–650. [Google Scholar] [CrossRef]
- Kudo, M.; Zheng, R.Q.; Kim, S.R.; Okabe, Y.; Osaki, Y.; Iijima, H.; Itani, T.; Kasugai, H.; Kanematsu, M.; Ito, K.; et al. Diagnostic Accuracy of Imaging for Liver Cirrhosis Compared to Histologically Proven Liver Cirrhosis. Intervirology 2008, 51, 17–26. [Google Scholar] [CrossRef]
- Zarski, J.P.; Sturm, N.; Guechot, J.; Paris, A.; Zafrani, E.S.; Asselah, T.; Boisson, R.C.; Bosson, J.L.; Guyader, D.; Renversez, J.C.; et al. Comparison of nine blood tests and transient elastography for liver fibrosis in chronic hepatitis C: the ANRS HCEP-23 study. J. Hepatol. 2012, 56, 55–62. [Google Scholar] [CrossRef]
- Tsochatzis, E.; Gurusamy, K.; Ntaoula, S.; Cholongitas, E.; Davidson, B.; Burroughs, A.; Tsochatzis, E.; Gurusamy, K. Elastography for the diagnosis of severity of fibrosis in chronic liver disease: A meta-analysis of diagnostic accuracy. J. Hepatol. 2011, 54, 650–659. [Google Scholar] [CrossRef]
- Kudo, M.; Izumi, N.; Kokudo, N.; Matsui, O.; Sakamoto, M.; Nakashima, O.; Kojiro, M.; Makuuchi, M.; HCC Expert Panel of Japan Society of Hepatology. IN Management of hepatocellular carcinoma in Japan: Consensus-Based Clinical Practice Guidelines proposed by the Japan Society of Hepatology (JSH) 2010 updated version. Dig. Dis. 2011, 29, 339–364. [Google Scholar] [CrossRef]
- Hasegawa, K.; Takata, R.; Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Nakano, C.; et al. Impact of Wisteria floribunda Agglutinin-Positive Mac-2-Binding Protein in Patients with Hepatitis C Virus-Related Compensated Liver Cirrhosis. Int. J. Mol. Sci. 2016, 17, 1500. [Google Scholar] [CrossRef]
- Nishikawa, H.; Nishijima, N.; Enomoto, H.; Sakamoto, A.; Nasu, A.; Komekado, H.; Nishimura, T.; Kita, R.; Kimura, T.; Iijima, H.; et al. Comparison of FIB-4 index and aspartate aminotransferase to platelet ratio index on carcinogenesis in chronic hepatitis B treated with entecavir. J. Cancer 2017, 8, 152–161. [Google Scholar] [CrossRef]
- Nishikawa, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Yuri, Y.; Takata, R.; Hasegawa, K.; Nakano, C.; Nishimura, T.; Kazunori, Y.; et al. Development of a simple predictive model for decreased skeletal muscle mass in patients with compensated chronic liver disease. Hepatol. Res. 2017, 47, 1223–1234. [Google Scholar] [CrossRef]
- Arai, H.; Akishita, M.; Chen, L.-K. Growing research on sarcopenia in Asia. Geriatr. Gerontol. Int. 2014, 14, 1–7. [Google Scholar] [CrossRef]
- Sinclair, M.; Gow, P.J.; Grossmann, M.; Angus, P.W. Review article: Sarcopenia in cirrhosis - aetiology, implications and potential therapeutic interventions. Aliment. Pharmacol. Ther. 2016, 43, 765–777. [Google Scholar] [CrossRef]
- Lai, J.C.; Covinsky, K.E.; McCulloch, C.E.; Feng, S. The Liver Frailty Index Improves Mortality Prediction of the Subjective Clinician Assessment in Patients With Cirrhosis. Am. J. Gastroenterol. 2018, 113, 235–242. [Google Scholar] [CrossRef]
- Ortega, F.B.; Silventoinen, K.; Tynelius, P.; Rasmussen, F. Muscular strength in male adolescents and premature death: cohort study of one million participants. BMJ 2012, 345, e7279. [Google Scholar] [CrossRef]
- López-Jaramillo, P.; Cohen, D.D.; Gomez-Arbelaez, D.; Bosch, J.; Dyal, L.; Yusuf, S.; Gerstein, H.C. Association of handgrip strength to cardiovascular mortality in pre-diabetic and diabetic patients: A subanalysis of the ORIGIN trial. Int. J. Cardiol. 2014, 174, 458–461. [Google Scholar] [CrossRef]
- Sasaki, H.; Kasagi, F.; Yamada, M.; Fujita, S. Grip Strength Predicts Cause-Specific Mortality in Middle-Aged and Elderly Persons. Am. J. Med. 2007, 120, 337–342. [Google Scholar] [CrossRef]
- Yoshida, D.; Suzuki, T.; Shimada, H.; Park, H.; Makizako, H.; Doi, T.; Anan, Y.; Tsutsumimoto, K.; Uemura, K.; Ito, T.; et al. Using two different algorithms to determine the prevalence of sarcopenia. Geriatr. Gerontol. Int. 2014, 14, 46–51. [Google Scholar] [CrossRef]
- Sung, J.H.; Uojima, H.; Hidaka, H.; Tanaka, Y.; Wada, N.; Kubota, K.; Nakazawa, T.; Shibuya, A.; Fujikawa, T.; Yamanoue, H.; et al. Risk factors for loss of skeletal muscle mass in patients with cirrhosis. Hepatol. Res. 2019, 49, 550–558. [Google Scholar] [CrossRef]
- Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Hasegawa, K.; Nakano, C.; Nishimura, T.; et al. Elevated serum myostatin level is associated with worse survival in patients with liver cirrhosis. J. Cachex- Sarcopenia Muscle 2017, 8, 915–925. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Number or |
|---|---|
| Median Value (IQR) | |
| Age (years) | 64 (52, 71) |
| Gender, male/female | 171/205 |
| HCV/HBV/HCV and HBV/NBNC | 208/55/4/109 |
| Body mass index (kg/m2) | 22.7 (20.7, 25.6) |
| Hand grip strength (kg, male) | 35.5 (29.2, 41.5) |
| Hand grip strength (kg, female) | 21.1 (17.9, 24.4) |
| Presence of HCC, yes/no | 9/367 |
| Presence of LC, yes/no | 137/239 |
| Child-Pugh, A/B/C | 345/25/6 |
| Total bilirubin (mg/dL) | 0.8 (0.6, 1.0) |
| Serum albumin (g/dL) | 4.3 (4.0, 4.5) |
| Prothrombin time (%) | 92.4 (83.825, 101.95) |
| Platelet count (× 104/mm3) | 18.0 (12.9, 22.475) |
| M2BPGi (cutoff index) | 1.11 (0.70, 2.34) |
| FIB4-index | 2.069 (1.2515, 3.451) |
| SMI (kg/m2, male) | 7.61 (7.07, 8.12) |
| SMI (kg/m2, female) | 5.94 (5.505, 6.48) |
| AST (IU/L) | 24 (19, 32) |
| ALT (IU/L) | 49 (14, 30) |
| HbA1c (NGSP) | 5.7 (5.4, 6.0) |
| eGFR (ml/min/1.73m2) | 81 (68, 99) |
| Serum ammonia (μg/dl) | 39 (30, 49.5) |
| Variables | GS ≥ 26 kg (n = 146) | GS < 26 kg (n = 25) | P Value |
|---|---|---|---|
| Age (years) | 58.5 (48, 68) | 73 (68, 76.5) | < 0.0001 |
| HBV/HCV/HBV and HCV/NBNC | 31/76/2/37 | 4/14/0/7 | 0.8614 |
| Body mass index (kg/m2) | 23.8 (21.8, 26) | 21.5 (19.85, 24.75) | 0.0357 |
| Presence of LC, yes/no | 48/98 | 19/6 | < 0.0001 |
| Total bilirubin (mg/dl) | 0.8 (0.6, 1.1) | 0.8 (0.6, 1.45) | 0.3377 |
| Serum albumin (g/dl) | 4.4 (4.1, 4.6) | 3.7 (3.05, 4.05) | < 0.0001 |
| Prothrombin time (%) | 92.45 (84.2, 99.65) | 80.4 (54.8, 93.1) | 0.0013 |
| Platelet count (× 104/mm3) | 18.55 (12.9, 22.225) | 13.4 (8.1, 18.0) | 0.0025 |
| M2BPGi | 0.9 (0.61, 1.7825) | 4.93 (2.615, 7.85) | < 0.0001 |
| FIB-4 index | 1.73 (0.97, 2.83) | 3.89 (2.13, 6.74) | < 0.0001 |
| eGFR (ml/min/1.73m2) | 84 (71, 100.25) | 75 (53, 84) | 0.0249 |
| HbA1c (NGSP) | 5.6 (5.3, 6.0) | 6.0 (5.35, 7.1) | 0.0608 |
| Serum ammonia (μg/dl) | 43 (33, 54) | 49 (33, 74) | 0.3551 |
| SMI (kg/m2) | 7.70 (7.1575, 8.22) | 7.12 (6.565, 7.665) | 0.0028 |
| Multivariate Analysis | |||
|---|---|---|---|
| Hazard Ratio | 95% CI | P Value | |
| Age (per one year) | 1.015 | 0.933−1.104 | 0.7270 |
| BMI (per one kg/m2) | 0.905 | 0.688−1.190 | 0.4754 |
| Presence of LC | 2.522 | 0.448−14.185 | 0.2940 |
| Serum albumin (per one g/dl) | 0.327 | 0.071−1.502 | 0.1508 |
| Prothrombin time (per one%) | 1.005 | 0.962−1.050 | 0.8128 |
| Platelet count (per one × 104/mm3) | 1.117 | 0.951−1.311 | 0.1747 |
| eGFR (per one ml/min/1.73m2) | 0.990 | 0.962−1.018 | 0.4725 |
| M2BPGi (per one COI) | 1.740 | 1.228−2.467 | 0.0003 |
| FIB−4 index (per one) | 1.160 | 0.797−1.688 | 0.4344 |
| Skeletal muscle index (per one) | 0.124 | 0.032−0.482 | 0.0007 |
| Variables | GS ≥ 18 kg (n = 153) | GS < 18 kg (n = 52) | P Value |
|---|---|---|---|
| Age (years) | 63 (54, 69) | 71 (66.25, 75) | <0.0001 |
| HBV/HCV/HBV and HCV/NBNC | 17/87/2/47 | 3/31/0/18 | 0.5617 |
| Body mass index (kg/m2) | 22.3 (20.35, 25.45) | 21.8 (20.35, 25.25) | 0.5834 |
| Presence of LC, yes/no | 49/104 | 21/31 | 0.3109 |
| Total bilirubin (mg/dl) | 0.7 (0.6, 1.0) | 0.7 (0.6, 0.9) | 0.4856 |
| Serum albumin (g/dl) | 4.3 (4.1, 4.5) | 4.1 (3.8, 4.4) | 0.0209 |
| Prothrombin time (%) | 94.5 (86.9, 103.1) | 88.6 (82.375, 98.525) | 0.0283 |
| Platelet count (×104/mm3) | 18.9 (13.8, 23.5) | 16.25 (10.825, 20.175) | 0.0255 |
| M2BPGi (cutoff index) | 1.01 (0.685, 1.805) | 1.53 (0.8875, 2.845) | 0.0017 |
| FIB-4 index | 1.983 (1.321, 3.2165) | 2.6945 (1.76725, 3.9655) | 0.0328 |
| eGFR (ml/min/1.73m2) | 83 (69, 99) | 73 (65.5, 92.5) | 0.0759 |
| HbA1c (NGSP) | 5.7 (5.4, 6.0) | 5.8 (5.4, 6.0) | 0.6959 |
| Serum ammonia (μg/dl) | 36 (27.75, 42) | 33 (21, 45) | 0.7235 |
| SMI (kg/m2) | 6.02 (5.65, 6.53) | 5.58 (5.27, 6.33) | 0.0036 |
| Multivariate Analysis | |||
|---|---|---|---|
| Hazard Ratio | 95% CI | P Value | |
| Age (per one year) | 1.085 | 1.039–1.133 | <0.0001 |
| Serum albumin (per one g/dl) | 0.363 | 0.132–0.998 | 0.0484 |
| Prothrombin time (per one%) | 0.988 | 0.957–1.020 | 0.4450 |
| Platelet count (per one × 104/mm3) | 0.987 | 0.915–1.064 | 0.7210 |
| M2BPGi (per one COI) | 1.100 | 0.902–1.343 | 0.3502 |
| FIB-4 index (per one) | 1.129 | 0.881–1.446 | 0.3100 |
| Skeletal muscle index (per one) | 0.657 | 0.384–1.125 | 0.1181 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Significant Correlation Between Grip Strength and m2bpgi in Patients with Chronic Liver Diseases. J. Clin. Med. 2019, 8, 1359. https://doi.org/10.3390/jcm8091359
Nishikawa H, Enomoto H, Yoh K, Iwata Y, Sakai Y, Kishino K, Ikeda N, Takashima T, Aizawa N, Takata R, et al. Significant Correlation Between Grip Strength and m2bpgi in Patients with Chronic Liver Diseases. Journal of Clinical Medicine. 2019; 8(9):1359. https://doi.org/10.3390/jcm8091359
Chicago/Turabian StyleNishikawa, Hiroki, Hirayuki Enomoto, Kazunori Yoh, Yoshinori Iwata, Yoshiyuki Sakai, Kyohei Kishino, Naoto Ikeda, Tomoyuki Takashima, Nobuhiro Aizawa, Ryo Takata, and et al. 2019. "Significant Correlation Between Grip Strength and m2bpgi in Patients with Chronic Liver Diseases" Journal of Clinical Medicine 8, no. 9: 1359. https://doi.org/10.3390/jcm8091359
APA StyleNishikawa, H., Enomoto, H., Yoh, K., Iwata, Y., Sakai, Y., Kishino, K., Ikeda, N., Takashima, T., Aizawa, N., Takata, R., Hasegawa, K., Ishii, N., Yuri, Y., Nishimura, T., Iijima, H., & Nishiguchi, S. (2019). Significant Correlation Between Grip Strength and m2bpgi in Patients with Chronic Liver Diseases. Journal of Clinical Medicine, 8(9), 1359. https://doi.org/10.3390/jcm8091359