Synovial Cytokines Significantly Correlate with Osteoarthritis-Related Knee Pain and Disability: Inflammatory Mediators of Potential Clinical Relevance
 ,
, 
 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Population
2.2. Clinical Assessment
2.3. Sample Collection and Multiplex Cytokine Analysis
2.4. Statistical Analyses
3. Results
3.1. Description of the Study Population
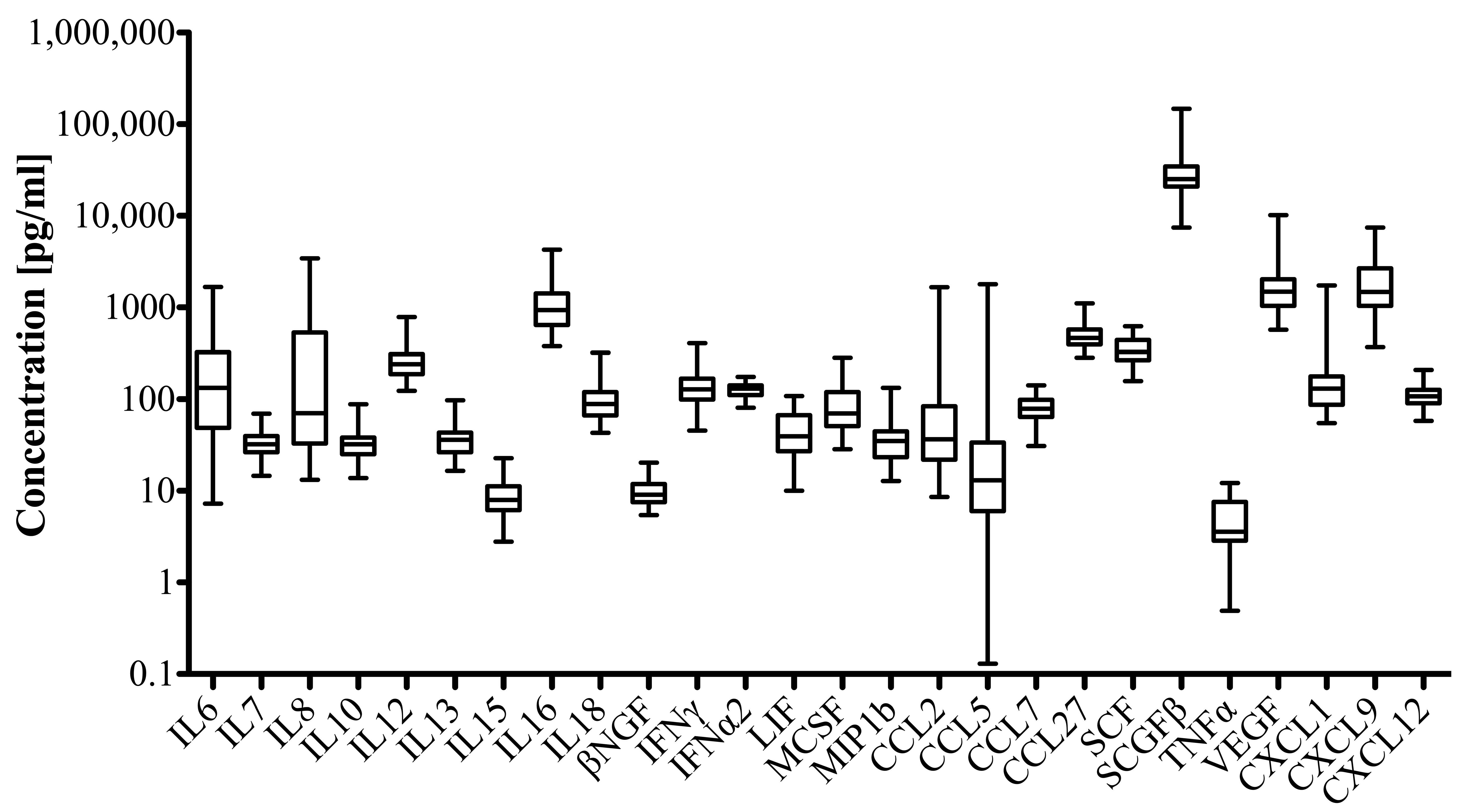
3.2. Profile of Inflammatory Mediators in OA-Related Knee Pain
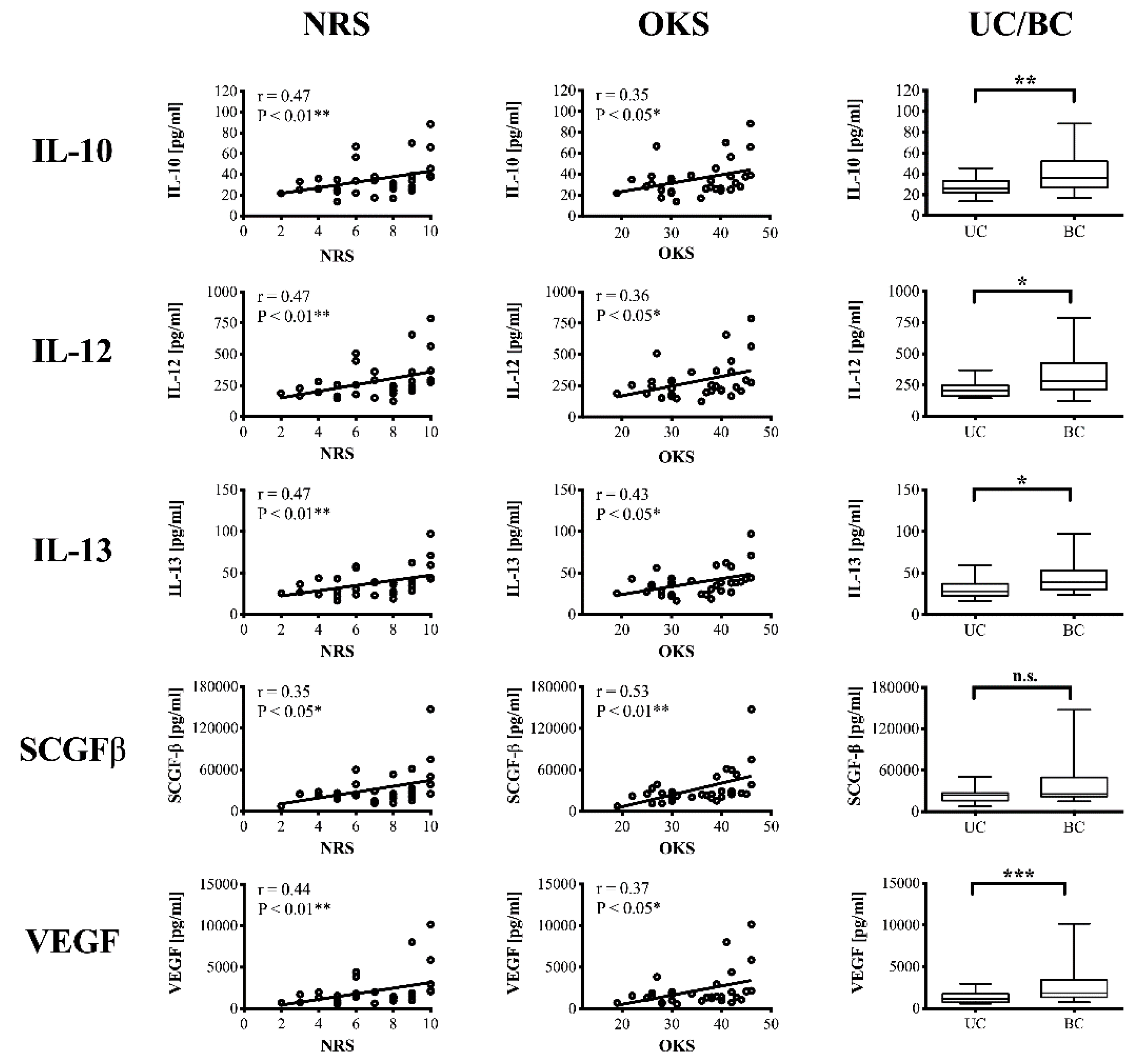
3.3. Correlation of Inflammatory Mediators and Clinical Parameters
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hay, S.I.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1260–1344. [Google Scholar] [CrossRef]
- Roemer, F.W.; Guermazi, A.; Felson, D.T.; Niu, J.; Nevitt, M.C.; Crema, M.D.; Lynch, J.A.; Lewis, C.E.; Torner, J.; Zhang, Y. Presence of MRI-detected joint effusion and synovitis increases the risk of cartilage loss in knees without osteoarthritis at 30-month follow-up: The MOST study. Ann. Rheum. Dis. 2011, 70, 1804–1809. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Rozelle, A.L.; Lepus, C.M.; Scanzello, C.R.; Song, J.J.; Larsen, D.M.; Crish, J.F.; Bebek, G.; Ritter, S.Y.; Lindstrom, T.M.; et al. Identification of a central role for complement in osteoarthritis. Nat. med. 2011, 17, 1674–1679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bondeson, J.; Blom, A.B.; Wainwright, S.; Hughes, C.; Caterson, B.; van den Berg, W.B. The role of synovial macrophages and macrophage-produced mediators in driving inflammatory and destructive responses in osteoarthritis. Arthritis Rheum. 2010, 62, 647–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moradi, B.; Rosshirt, N.; Tripel, E.; Kirsch, J.; Barie, A.; Zeifang, F.; Gotterbarm, T.; Hagmann, S. Unicompartmental and bicompartmental knee osteoarthritis show different patterns of mononuclear cell infiltration and cytokine release in the affected joints. Clin. Exp. Immunol. 2015, 180, 143–154. [Google Scholar] [CrossRef] [Green Version]
- Moradi, B.; Schnatzer, P.; Hagmann, S.; Rosshirt, N.; Gotterbarm, T.; Kretzer, J.P.; Thomsen, M.; Lorenz, H.M.; Zeifang, F.; Tretter, T. CD4+ CD25+/high CD127 low/-regulatory T cells are enriched in rheumatoid arthritis and osteoarthritis joints—Analysis of frequency and phenotype in synovial membrane, synovial fluid and peripheral blood. Arthritis Res. Ther. 2014, 16, R97. [Google Scholar] [CrossRef]
- Scanzello, C.R. Chemokines and inflammation in osteoarthritis: Insights from patients and animal models. J. Orthop. Res. 2017, 35, 735–739. [Google Scholar] [CrossRef]
- Bondeson, J.; Wainwright, S.D.; Lauder, S.; Amos, N.; Hughes, C.E. The role of synovial macrophages and macrophage-produced cytokines in driving aggrecanases, matrix metalloproteinases, and other destructive and inflammatory responses in osteoarthritis. Arthritis Res. Ther. 2006, 8, R187. [Google Scholar] [CrossRef]
- Richter, F.; Natura, G.; Loser, S.; Schmidt, K.; Viisanen, H.; Schaible, H.G. Tumor necrosis factor causes persistent sensitization of joint nociceptors to mechanical stimuli in rats. Arthritis Rheum. 2010, 62, 3806–3814. [Google Scholar] [CrossRef]
- Brenn, D.; Richter, F.; Schaible, H.G. Sensitization of unmyelinated sensory fibers of the joint nerve to mechanical stimuli by interleukin-6 in the rat: An inflammatory mechanism of joint pain. Arthritis Rheum. 2007, 56, 351–359. [Google Scholar] [CrossRef]
- Miotla Zarebska, J.; Chanalaris, A.; Driscoll, C.; Burleigh, A.; Miller, R.E.; Malfait, A.M.; Stott, B.; Vincent, T.L. CCL2 and CCR2 regulate pain-related behaviour and early gene expression in post-traumatic murine osteoarthritis but contribute little to chondropathy. Osteoarthr. Cartil. 2017, 25, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Thakur, M.; Dickenson, A.H.; Baron, R. Osteoarthritis pain: Nociceptive or neuropathic? Nat. Rev. Rheumatol. 2014, 10, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Walsh, D.A.; McWilliams, D.F.; Turley, M.J.; Dixon, M.R.; Franses, R.E.; Mapp, P.I.; Wilson, D. Angiogenesis and nerve growth factor at the osteochondral junction in rheumatoid arthritis and osteoarthritis. Rheumatology (Oxf., Engl.) 2010, 49, 1852–1861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lane, N.E.; Schnitzer, T.J.; Birbara, C.A.; Mokhtarani, M.; Shelton, D.L.; Smith, M.D.; Brown, M.T. Tanezumab for the treatment of pain from osteoarthritis of the knee. N. Engl. J. Med. 2010, 363, 1521–1531. [Google Scholar] [CrossRef] [PubMed]
- Das, V.; Kc, R.; Li, X.; O-Sullivan, I.; van Wijnen, A.J.; Kroin, J.S.; Pytowski, B.; Applegate, D.T.; Votta-Velis, G.; Ripper, R.L.; et al. Blockade of Vascular Endothelial Growth Factor Receptor-1 (Flt-1), Reveals a Novel Analgesic For Osteoarthritis-Induced Joint Pain. Gene Rep. 2018, 11, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Ren, G.; Lutz, I.; Railton, P.; Wiley, J.P.; McAllister, J.; Powell, J.; Krawetz, R.J. Serum and synovial fluid cytokine profiling in hip osteoarthritis: Distinct from knee osteoarthritis and correlated with pain. BMC Musculoskelet. Disord. 2018, 19, 39. [Google Scholar] [CrossRef] [PubMed]
- Radojcic, M.R.; Thudium, C.S.; Henriksen, K.; Tan, K.; Karlsten, R.; Dudley, A.; Chessell, I.; Karsdal, M.A.; Bay-Jensen, A.C.; Crema, M.D.; et al. Biomarker of extracellular matrix remodelling C1M and proinflammatory cytokine interleukin 6 are related to synovitis and pain in end-stage knee osteoarthritis patients. Pain 2017, 158, 1254–1263. [Google Scholar] [CrossRef] [Green Version]
- Orita, S.; Koshi, T.; Mitsuka, T.; Miyagi, M.; Inoue, G.; Arai, G.; Ishikawa, T.; Hanaoka, E.; Yamashita, K.; Yamashita, M.; et al. Associations between proinflammatory cytokines in the synovial fluid and radiographic grading and pain-related scores in 47 consecutive patients with osteoarthritis of the knee. BMC Musculoskelet. Disord. 2011, 12, 144. [Google Scholar] [CrossRef]
- Leung, Y.Y.; Huebner, J.L.; Haaland, B.; Wong, S.B.S.; Kraus, V.B. Synovial fluid pro-inflammatory profile differs according to the characteristics of knee pain. Osteoarthr. Cartil. 2017, 25, 1420–1427. [Google Scholar] [CrossRef] [Green Version]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef]
- Naal, F.D.; Impellizzeri, F.M.; Sieverding, M.; Loibl, M.; von Knoch, F.; Mannion, A.F.; Leunig, M.; Munzinger, U. The 12-item Oxford Knee Score: Cross-cultural adaptation into German and assessment of its psychometric properties in patients with osteoarthritis of the knee. Osteoarthr. Cartil. 2009, 17, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Schaible, H.G. Mechanisms of chronic pain in osteoarthritis. Curr. Rheumatol. Rep. 2012, 14, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Wojdasiewicz, P.; Poniatowski, Ł.A.; Szukiewicz, D. The Role of Inflammatory and Anti-Inflammatory Cytokines in the Pathogenesis of Osteoarthritis. Mediat. Inflamm. 2014, 2014, 19. [Google Scholar] [CrossRef]
- Schaible, H.G.; von Banchet, G.S.; Boettger, M.K.; Brauer, R.; Gajda, M.; Richter, F.; Hensellek, S.; Brenn, D.; Natura, G. The role of proinflammatory cytokines in the generation and maintenance of joint pain. Ann. N. Y. Acad. Sci. 2010, 1193, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Schaible, H.G. Nociceptive neurons detect cytokines in arthritis. Arthritis Res. Ther. 2014, 16, 470. [Google Scholar] [CrossRef] [PubMed]
- Vuolteenaho, K.; Koskinen-Kolasa, A.; Laavola, M.; Nieminen, R.; Moilanen, T.; Moilanen, E. High synovial fluid interleukin-6 levels are associated with increased matrix metalloproteinase levels and severe radiographic changes in osteoarthritis patients. Osteoarthr. Cartil. 2017, 25, S92–S93. [Google Scholar] [CrossRef]
- Livshits, G.; Zhai, G.; Hart, D.J.; Kato, B.S.; Wang, H.; Williams, F.M.; Spector, T.D. Interleukin-6 is a significant predictor of radiographic knee osteoarthritis: The Chingford Study. Arthritis Rheum. 2009, 60, 2037–2045. [Google Scholar] [CrossRef] [PubMed]
- Imamura, M.; Ezquerro, F.; Marcon Alfieri, F.; Vilas Boas, L.; Tozetto-Mendoza, T.R.; Chen, J.; Ozcakar, L.; Arendt-Nielsen, L.; Rizzo Battistella, L. Serum levels of proinflammatory cytokines in painful knee osteoarthritis and sensitization. Int. J. Inflam. 2015, 2015, 1–8. [Google Scholar] [CrossRef]
- Verbruggen, G.; Wittoek, R.; Vander Cruyssen, B.; Elewaut, D. Tumour necrosis factor blockade for the treatment of erosive osteoarthritis of the interphalangeal finger joints: A double blind, randomised trial on structure modification. Ann. Rheum. Dis. 2012, 71, 891–898. [Google Scholar] [CrossRef]
- Chevalier, X.; Ravaud, P.; Maheu, E.; Baron, G.; Rialland, A.; Vergnaud, P.; Roux, C.; Maugars, Y.; Mulleman, D.; Lukas, C.; et al. Adalimumab in patients with hand osteoarthritis refractory to analgesics and NSAIDs: A randomised, multicentre, double-blind, placebo-controlled trial. Ann. Rheum. Dis. 2015, 74, 1697–1705. [Google Scholar] [CrossRef]
- Barker, T.; Rogers, V.E.; Henriksen, V.T.; Aguirre, D.; Trawick, R.H.; Rasmussen, G.L.; Momberger, N.G. Serum cytokines are increased and circulating micronutrients are not altered in subjects with early compared to advanced knee osteoarthritis. Cytokine 2014, 68, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Marks, P.H.; Donaldson, M.L.C. Inflammatory cytokine profiles associated with chondral damage in the anterior cruciate ligament-deficient knee. Arthroscopy 2005, 21, 1342–1347. [Google Scholar] [CrossRef] [PubMed]
- Borzi, R.M.; Mazzetti, I.; Magagnoli, G.; Paoletti, S.; Uguccioni, M.; Gatti, R.; Orlandini, G.; Cattini, L.; Facchini, A. Growth-related oncogene alpha induction of apoptosis in osteoarthritis chondrocytes. Arthritis Rheum. 2002, 46, 3201–3211. [Google Scholar] [CrossRef] [PubMed]
- Beekhuizen, M.; Gierman, L.M.; van Spil, W.E.; Van Osch, G.J.; Huizinga, T.W.; Saris, D.B.; Creemers, L.B.; Zuurmond, A.M. An explorative study comparing levels of soluble mediators in control and osteoarthritic synovial fluid. Osteoarthr. Cartil. 2013, 21, 918–922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heard, B.J.; Fritzler, M.J.; Wiley, J.P.; McAllister, J.; Martin, L.; El-Gabalawy, H.; Hart, D.A.; Frank, C.B.; Krawetz, R. Intraarticular and systemic inflammatory profiles may identify patients with osteoarthritis. J. Rheumatol. 2013, 40, 1379–1387. [Google Scholar] [CrossRef] [PubMed]
- Scanzello, C.R.; Umoh, E.; Pessler, F.; Diaz-Torne, C.; Miles, T.; Dicarlo, E.; Potter, H.G.; Mandl, L.; Marx, R.; Rodeo, S.; et al. Local cytokine profiles in knee osteoarthritis: Elevated synovial fluid interleukin-15 differentiates early from end-stage disease. Osteoarthr. Cartil. 2009, 17, 1040–1048. [Google Scholar] [CrossRef] [PubMed]
- Iannone, F.; De Bari, C.; Dell’Accio, F.; Covelli, M.; Cantatore, F.P.; Patella, V.; Lo Bianco, G.; Lapadula, G. Interleukin-10 and interleukin-10 receptor in human osteoarthritic and healthy chondrocytes. Clin. Exp. Immunol. Rheumatol. 2001, 19, 139–145. [Google Scholar]
- Wang, Y.; Lou, S. Direct protective effect of interleukin-10 on articular chondrocytes in vitro. Chin. Med. J. 2001, 114, 723–725. [Google Scholar] [PubMed]
- John, T.; Muller, R.D.; Oberholzer, A.; Zreiqat, H.; Kohl, B.; Ertel, W.; Hostmann, A.; Tschoeke, S.K.; Schulze-Tanzil, G. Interleukin-10 modulates pro-apoptotic effects of TNF-alpha in human articular chondrocytes in vitro. Cytokine 2007, 40, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Eijkelkamp, N.; Steen-Louws, C.; Hartgring, S.A.; Willemen, H.L.; Prado, J.; Lafeber, F.P.; Heijnen, C.J.; Hack, C.E.; van Roon, J.A.; Kavelaars, A. IL4-10 Fusion Protein Is a Novel Drug to Treat Persistent Inflammatory Pain. J. Neurosci. 2016, 36, 7353–7363. [Google Scholar] [CrossRef]
- Nagao, M.; Hamilton, J.L.; Kc, R.; Berendsen, A.D.; Duan, X.; Cheong, C.W.; Li, X.; Im, H.J.; Olsen, B.R. Vascular Endothelial Growth Factor in Cartilage Development and Osteoarthritis. Sci. Rep. 2017, 7, 13027. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Murata, Y.; Liu, Y.; Nicolae, C.; Olsen, B.R.; Berendsen, A.D. Vegfa regulates perichondrial vascularity and osteoblast differentiation in bone development. Development (Camb. Engl.) 2015, 142, 1984–1991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zelzer, E.; Mamluk, R.; Ferrara, N.; Johnson, R.S.; Schipani, E.; Olsen, B.R. VEGFA is necessary for chondrocyte survival during bone development. Development (Camb. Engl.) 2004, 131, 2161–2171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Fontenla, C.; Calaza, M.; Evangelou, E.; Valdes, A.M.; Arden, N.; Blanco, F.J.; Carr, A.; Chapman, K.; Deloukas, P.; Doherty, M.; et al. Assessment of osteoarthritis candidate genes in a meta-analysis of nine genome-wide association studies. Arthritis Rheumatol. 2014, 66, 940–949. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, J.L.; Nagao, M.; Levine, B.R.; Chen, D.; Olsen, B.R.; Im, H.J. Targeting VEGF and Its Receptors for the Treatment of Osteoarthritis and Associated Pain. J. Bone Miner. Res. 2016, 31, 911–924. [Google Scholar] [CrossRef] [PubMed]
- Ludin, A.; Sela, J.J.; Schroeder, A.; Samuni, Y.; Nitzan, D.W.; Amir, G. Injection of vascular endothelial growth factor into knee joints induces osteoarthritis in mice. Osteoarthr. Cartil. 2013, 21, 491–497. [Google Scholar] [CrossRef] [Green Version]
- Selvaraj, D.; Gangadharan, V.; Michalski, C.W.; Kurejova, M.; Stosser, S.; Srivastava, K.; Schweizerhof, M.; Waltenberger, J.; Ferrara, N.; Heppenstall, P.; et al. A Functional Role for VEGFR1 Expressed in Peripheral Sensory Neurons in Cancer Pain. Cancer cell 2015, 27, 780–796. [Google Scholar] [CrossRef] [Green Version]
- Hiraoka, A.; Sugimura, A.; Seki, T.; Nagasawa, T.; Ohta, N.; Shimonishi, M.; Hagiya, M.; Shimizu, S. Cloning, expression, and characterization of a cDNA encoding a novel human growth factor for primitive hematopoietic progenitor cells. Proc. Natl. Acad. Sci. USA 1997, 94, 7577–7582. [Google Scholar] [CrossRef] [Green Version]
- Hiraoka, A.; Yano Ki, K.; Kagami, N.; Takeshige, K.; Mio, H.; Anazawa, H.; Sugimoto, S. Stem cell growth factor: In situ hybridization analysis on the gene expression, molecular characterization and in vitro proliferative activity of a recombinant preparation on primitive hematopoietic progenitor cells. Hematol. J. 2001, 2, 307–315. [Google Scholar] [CrossRef]
- Sukowati, C.H.C.; Patti, R.; Pascut, D.; Ladju, R.B.; Tarchi, P.; Zanotta, N.; Comar, M.; Tiribelli, C.; Croce, L.S. Serum Stem Cell Growth Factor Beta for the Prediction of Therapy Response in Hepatocellular Carcinoma. Biomed Res. Int. 2018, 2018, 6435482. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total Study Population | UC OA | BC OA | |
|---|---|---|---|
| Number of patients, n | 34 | 14 | 20 |
| Gender, n (%) | |||
| Male | 14 (41.2%) | 9 (64.3%) | 5 (25.0%) |
| Female | 20 (58.8%) | 5 (35.7%) | 15 (75.0%) |
| Age, years | 67.38 ± 10.48 (40–89) | 66.71 ± 10.23 (50–89) | 67.85 ± 10.89 (40–83) |
| BMI (kg/m²) | 30.74 ± 5.78 (21.00–43.00) | 29.43 ± 5.36 (22.00–40.00) | 31.65 ± 6.02 (21.00–43.00) |
| K&L score, n (%) | |||
| 2 | 5 (15.1%) | 2 (14.3%) | 3 (15.8%) |
| 3 | 13 (39.4%) | 9 (64.3%) | 4 (21.0%) |
| 4 | 15 (45.5%) | 3 (21.4%) | 12 (63.2%) |
| Knee pain, NRS (0–10) | 7.12 ± 2.29 (2.00–10.00) | 6.21 ± 2.39 (2.00–10.00) | 7.75 ± 2.05 (3.00–10.00) |
| OKS-12 (Pt. 12–60) | 35.15 ± 7.68 (19.00–46.00) | 32.21 ± 6.69 (19.00–44.00) | 37.32 ± 7.80 (22.00–46.00) |
| Mediator | Concentration in SF [pg/mL] | K&L Score | Knee Pain, NRS (0–10) | OKS, (Pt. 12–60) | |||
|---|---|---|---|---|---|---|---|
| Mean ± SD (Range) | r | p | r | p | r | p | |
| IL-6 | 277.4 ± 368.7 (7.2–1666.4) | 0.37 | 0.035 * | 0.23 | 0.18 | 0.41 | 0.017 * |
| IL-7 | 35.3 ± 13.1 (14.5–69.7) | 0.26 | 0.14 | 0.39 | 0.023 * | 0.21 | 0.23 |
| IL-8 | 405.1 ± 694.9 (13.2–3419.8) | 0.47 | 0.006 ** | −0.04 | 0.81 | 0.10 | 0.59 |
| IL-10 | 35.4 ± 16.5 (13.7–88.3) | 0.22 | 0.21 | 0.47 | 0.005 ** | 0.35 | 0.047 * |
| IL-12 | 284.1 ± 150.5 (123.8–786.8) | 0.22 | 0.22 | 0.47 | 0.005 ** | 0.36 | 0.037 * |
| IL-13 | 38.2 ± 16.6 (16.5–97.1) | 0.20 | 0.28 | 0.47 | 0.005 ** | 0.43 | 0.012 * |
| IL-15 | 9.1 ± 4.2 (2.8–22.7) | 0.14 | 0.45 | −0.20 | 0.26 | 0.17 | 0.36 |
| IL-16 | 1122.4 ± 757.4 (378.2–4256.3) | 0.28 | 0.11 | −0.16 | 0.38 | 0.29 | 0.10 |
| IL-18 | 100.8 ± 53.6 (43–321.6) | 0.14 | 0.45 | −0.10 | 0.58 | 0.36 | 0.043 * |
| βNGF | 9.6 ± 2.9 (5.4–20.3) | 0.10 | 0.60 | 0.05 | 0.79 | 0.40 | 0.021 * |
| IFNγ | 142.7 ± 73.3 (45.5–406.9) | 0.35 | 0.049 * | 0.35 | 0.044 * | 0.34 | 0.05 |
| IFNα2 | 126.4 ± 21.40 (80.92–175.7) | 0.20 | 0.26 | −0.12 | 0.49 | 0.27 | 0.13 |
| LIF | 47.2 ± 25.2 (10.1–108.6) | 0.25 | 0.16 | −0.29 | 0.10 | 0.22 | 0.22 |
| M-CSF | 85.80 ± 51.90 (28.42–283.8) | 0.22 | 0.23 | −0.08 | 0.63 | 0.20 | 0.27 |
| MIP-1β | 40 ± 24.1 (12.8–133.1) | −0.06 | 0.76 | −0.10 | 0.59 | 0.07 | 0.70 |
| CCL2 | 114.6 ± 293.2 (8.6–1655.8) | 0.02 | 0.93 | 0.14 | 0.43 | 0.24 | 0.18 |
| CCL5 | 115.8 ± 329.5 (0.1–1791.1) | 0.12 | 0.49 | −0.01 | 0.97 | 0.34 | 0.05 |
| CCL7 | 82.92 ± 26.4 (30.80–141.4) | 0.001 | 0.99 | −0.08 | 0.65 | 0.18 | 0.30 |
| CCL27 | 500.0 ± 155.3 (284.0–1104) | 0.03 | 0.88 | −0.12 | 0.50 | 0.03 | 0.86 |
| SCF | 346.7 ± 102.9 (157.2–623.2) | 0.09 | 0.61 | −0.33 | 0.06 | 0.10 | 0.58 |
| SCGF-β | 32337.5 ± 25341.6 (7435–147588) | 0.43 | 0.013 * | 0.35 | 0.040 * | 0.53 | 0.002 ** |
| TNF-a | 5 ± 3.1 (0.5–12.2) | 0.34 | 0.053 | 0.27 | 0.12 | 0.32 | 0.07 |
| VEGF | 2180.3 ± 2087.7 (569.4–10159.9) | 0.39 | 0.025 * | 0.44 | 0.009 ** | 0.37 | 0.034 * |
| CXCL1 | 232.4 ± 316.7 (54.76–1733) | 0.49 | 0.004 ** | 0.08 | 0.64 | 0.30 | 0.09 |
| CXCL9 | 1972 ± 1378 (368.5–7445) | 0.15 | 0.42 | 0.06 | 0.73 | 0.38 | 0.028 * |
| CXCL12 | 110.7 ± 31.41 (58.17–208,7) | 0.19 | 0.30 | −0.22 | 0.21 | 0.02 | 0.89 |
| Mediator | UC OA Median (IQR) | BC OA Median (IQR) | p-Value |
|---|---|---|---|
| IL-7 | 29.04 (23.79, 34.56) | 34.64 (29.34, 48.40) | 0.0321 * |
| IL-8 | 38.96 (27.36, 86.69) | 208.2 (44.45, 615.5) | 0.0390 * |
| IL-10 | 26.29 (21.95, 33.19) | 36.21 (26.77, 52.14) | 0.0047 ** |
| IL-12 | 207.8 (160.7, 248.8) | 279.5 (213.0, 425.9) | 0.0200 * |
| IL-13 | 28.20 (22.55, 37.07) | 38.54 (29.99, 53.11) | 0.0264 * |
| IFN-γ | 112.7 (85.34, 138.6) | 138.6 (103.0, 187.0) | 0.0439 * |
| VEGF | 1178 (747.1, 1762) | 1855 (1358, 3428) | 0.0108 * |
| CXCL1 | 95.69 (73.09, 134.1) | 171.1 (119.0, 258.4) | 0.0097 ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nees, T.A.; Rosshirt, N.; Zhang, J.A.; Reiner, T.; Sorbi, R.; Tripel, E.; Walker, T.; Schiltenwolf, M.; Hagmann, S.; Moradi, B. Synovial Cytokines Significantly Correlate with Osteoarthritis-Related Knee Pain and Disability: Inflammatory Mediators of Potential Clinical Relevance. J. Clin. Med. 2019, 8, 1343. https://doi.org/10.3390/jcm8091343
Nees TA, Rosshirt N, Zhang JA, Reiner T, Sorbi R, Tripel E, Walker T, Schiltenwolf M, Hagmann S, Moradi B. Synovial Cytokines Significantly Correlate with Osteoarthritis-Related Knee Pain and Disability: Inflammatory Mediators of Potential Clinical Relevance. Journal of Clinical Medicine. 2019; 8(9):1343. https://doi.org/10.3390/jcm8091343
Chicago/Turabian StyleNees, Timo A., Nils Rosshirt, Jiji A. Zhang, Tobias Reiner, Reza Sorbi, Elena Tripel, Tilman Walker, Marcus Schiltenwolf, Sébastien Hagmann, and Babak Moradi. 2019. "Synovial Cytokines Significantly Correlate with Osteoarthritis-Related Knee Pain and Disability: Inflammatory Mediators of Potential Clinical Relevance" Journal of Clinical Medicine 8, no. 9: 1343. https://doi.org/10.3390/jcm8091343